
Abstract
In this paper, Weibull unobserved heterogeneity (frailty) survival models are utilized to analyze the determinants of infant and child mortality in Kenya. The results of these models are compared to those of standard Weibull survival models. The study particularly examines the extent to which child survival risks continue to vary net of observed factors and the extent to which nonfrailty models are biased due to the violation of the statistical assumption of independence. The data came from the 1998 Kenya Demographic and Health Survey. The results of the standard Weibull survival models clearly show that biodemographic factors are more important in explaining infant mortality, while socioeconomic, sociocultural and hygienic factors are more important in explaining child mortality. Frailty effects are substantial and highly significant both in infancy and in childhood, but the conclusions remain the same as in the nonfrailty models.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Like most developing countries, Kenya started experiencing declines in early life mortality in the late 1940s (Hill 1992); the declines continued through most of the 1970s and 1980s (Brass 1993). Infant and child mortality rates currently standing at 77 and 41 per 1,000 live births, respectively, are still high even by sub-Saharan Africa standards (Central Bureau of Statistics, Ministry of Health & ORC Macro 2004). However, the reasons for this high mortality remain largely unknown as there are no systematic analyses of the determinants of infant and child mortality in the country. This study examines in particular the socioeconomic, sociocultural, biodemographic, and household environmental factors associated with mortality among children in Kenya, and the extent to which the survival outcomes of siblings are associated net of the observed factors. This association of child survival outcomes even after accounting for different known determinants of mortality has been attributed to unobserved heterogeneity or frailty (Sastry 1997a; Madise and Diamond 1995; Curtis et al. 1993). This analysis is conducted separately for infancy (0–11 months) and childhood (12–59 months) because the effect of factors associated with mortality among children varies by the age of the child (Manda 1999; Sastry 1997a).
The association of siblings’ survival outcomes net of observed factors arises in the context of clustered data. Studies of childhood mortality in developing countries have largely utilized women’s retrospective birth histories data from World Fertility Surveys (WFS) and Demographic and Health Surveys (DHS). This suggests that the lifetimes of a woman’s children are dependent and therefore their risks of death are correlated. The clustering of siblings’ survival experiences has methodological and substantive implications. Methodologically, models that ignore the clustering in siblings’ survival experiences could be biased as they violate the statistical assumption of independence. In this respect frailty models are important because they allow for the correlation in siblings’ survival experiences and hence yield accurate estimates of mortality determinants. Frailty models are also substantively important as they allow for the estimation of the effect of unmeasured and unmeasurable factors on the risk of death. In this paper, we control for correlation between siblings’ survival risks at the family level, which also captures the effect of unobserved factors on the risk of child death.
Frailty: some theoretical perspectives
The major assumption of the hazard models and other standard statistical techniques is that the observations are independent. However, in DHS the information on children is collected from mothers in sampled households, hence children are not independent observations. In the presence of correlated observations, the information provided on siblings is less than would have been the case if the same number of children were from different households. This leads to small standard errors and hence falsely significant estimates, while in the case of hazard models it yields small parameter estimates that are inconsistent and biased (Guo and Zhao 2000; Trussell and Rodríguez 1990). Adjusting for the correlation structure in the data corrects for the biases in parameter estimates and provides correct standard errors and hence correct confidence intervals and significance tests.
Besides the methodological issue of correlated mortality risks of siblings, there are also substantive considerations associated with frailty. Generally, frailty in mortality studies is an unmeasured effect and serves to represent the idea that individuals in the population are heterogeneous due to factors that remain unobserved (Cleves et al. 2004; Sastry 1997b). Accounting for all relevant determinants of mortality would cause frailty in any group of families to disappear; it is only of importance if it points to factors that have not yet been considered for analysis (Das Gupta 1997). Frailty effects reflect a diversity of factors that can be broadly classified as genetic, behavioral and environmental factors, occurring at individual-, family- and community-level (Sastry 1997b). The discussion here is limited to the first two levels; Sastry (1997b) provides a detailed discussion on the effect of unobserved community factors.
Unless one is conducting a biological survey, genetic factors are unobserved in social surveys such as DHS. They are therefore important in the understanding of frailty effects particularly at the family level among children born to the same mother (Vaupel 1989). Unlike in the developed countries where most of the causes of death are congenital, in the less developed countries most child deaths are due to infectious diseases. Although the role of genetic factors is likely to be stronger for congenital causes of death, genetic variation underlies differentials in susceptibility to infections and there is therefore a genetic component to all illnesses (Sastry 1997b). However, the role of genetic factors in mortality differences between families is limited. This is because genetic factors inimical to child survival are kept low by natural selection, which ensures that those who die young have no chance of passing on their unfavorable genes (Guo 1993).
Genetic factors are largely unmeasurable, but surveys rarely include all theoretically relevant and measurable covariates. For instance, in demographic and health surveys, health seeking behavior during pregnancy and after child delivery is collected only for children born in the last 3–5 years preceding the survey. Consequently, information on the use of antenatal care, immunization, delivery care, and breastfeeding is unavailable for a majority of the children and it forms part of the unobserved behavioral factors at the family level. The behavior on utilization of antenatal and postnatal care is correlated between siblings (Magadi et al. 2001; Pebley et al. 1996) and is therefore important in the interpretation of shared unobserved behavioral factors at the family level (Sastry 1997b). Other behavior that could be unobserved includes beliefs about the causes of illnesses and the manner of their treatment.
Children belonging to the same family are clearly exposed to the same household environmental conditions (Sastry 1996; Curtis et al. 1993). Demographic and health surveys collect information on sanitation facilities and sources of drinking water, which serve as proxies for hygiene behavior including waste disposal, body cleanliness, and food preparation and storage. However, the type of toilet facility and source of water may not adequately capture the complexity associated with household environmental conditions and patterns of hygiene behavior, which suggests that the conditions and behaviors will comprise part of the family frailty effects.
An often recurring issue in studies of correlated mortality risks is the role of maternal competence in child care, which is independent of maternal education. For instance, Das Gupta (1990) demonstrated that women who experienced multiple child deaths were often less resourceful and less organized in caring for their surviving children and running the household even when compared with other women in households with similar socioeconomic conditions. In general, most mothers are resourceful and skillful in childrearing and the proportion in a population that is lacking in these skills is likely to be small, thus pointing to an innate inability that is not directly measurable. Childcare could also be differentiated by the gender of the child, with girl children being at a greater disadvantage in terms of feeding and receiving healthcare when sick (Das Gupta 1997). Preferential childcare by sex is unobserved because parents would not readily admit that they practice gender discrimination among their children.
The mother is used in this study as a measure of the family, and it is assumed that even though the woman is in a polygamous union, she is the de facto head of the household. We first estimate models that assume that siblings’ mortality risks are uncorrelated and then compare the results of these models with those of models that explicitly control for the correlation of siblings’ survival experiences and unobserved heterogeneity. The presence of frailty indicates the amount of variation across families and suggests that deaths are likely to be clustered in certain families. The major problem associated with the interpretation of frailty effects is that, being unmeasured, it is difficult to uniquely identify what these effects comprise and the exact mechanisms through which they affect the risk of death. The best one can do is to include as many factors as is theoretically possible to reduce the effect of frailty. However, even when all theoretically relevant factors are accounted for, the effect of unmeasured factors is never completely muted.
Data and methods
Data
This study utilizes data from the 1998 DHS for Kenya undertaken by National Council for Population and Development and Macro International of USA within the broader framework of demographic and health survey programs for developing countries. The 2003 DHS for Kenya became available at the end of 2004. However, the 1998 DHS was the first to clearly show that mortality conditions were on an upward trend. Naturally, it is important to first analyze these data as the basis for understanding contemporary mortality conditions and trends. Birth history information was collected from 7,881 women of reproductive age, 15–49 years. This analysis excludes children born in the month of interview because their survival experience is unknown. Of the 7,881 women, 5,716 reported a total of 23,348 births; 2,165 women were nulliparous. A detailed description of the survey including the sampling procedure, quality of the data, and the descriptive information on child mortality, fertility, and family planning among others is available in the country report (National Council for Population & Development [NCPD], Central Bureau of Statistics [CBS] & Macro International [MI] 1999).
A fundamental criterion in survival analysis is that the covariates correspond to the time the event occurred. The socioeconomic, sociocultural and hygienic factors considered in this analysis likely refer to conditions at the time of the survey. But it is possible that the factors have changed over the course of a woman’s childrearing and childbearing history. However, migration status refers to lifetime residential shift and hence it is invariant. Similarly, in Kenya as in most of the developing world, female schooling ceases with the start of childbearing and rarely resumes thereafter. Also, because it is not known whether household socioeconomic status has changed over time, it is assumed that it has remained unchanged. The biodemographic factors that are included are specific to each child and therefore correspond to the conditions under which the child was at risk of death. The inclusion of the biodemographic factors, especially the survival status of elder siblings and preceding birth interval, necessitate that we consider the entire birth history of the woman. Previous studies left-truncate the sample to minimize recall errors, which are assumed to be larger the farther back in time one moves. Despite the identified problem of age heaping (Marckwardt and Rutstein 1996) it seems unlikely that mothers ever forget the age at death of their children or that they experienced a child’s death. Also, in situations where the risks of immediate pairs of siblings are correlated, truncating the sample at certain birth orders or at certain years before the survey would mean that the entire risk profile for children in the same family would not be captured.
Analytical method
The dependent variable is the risk of death in infancy or childhood measured as the duration of survival since birth in months. Consequently, survival analysis procedures initially proposed by Cox (1972) are used to examine the effect of various factors on the risk of death. The main advantage of survival or hazard models is that they account for the problem of censoring in data from reproductive histories. A fundamental discriminating criterion between various survival models is the distribution that the timing function is assumed to follow (Cleves et al. 2004). Based on preliminary results documented in Omariba (2004), we utilize the Weibull proportional hazards model of the form:
where h i (t/x i ) is the hazard of child death at time t; γ is an ancillary shape parameter estimated from the data, x i is a vector of covariates with associated vector of fixed parameters β; while the scale parameter is parameterized as λ exp(β′x i ). The choice of the Weibull model is made on the basis of well-established knowledge on the distribution of deaths in human populations. Mortality is generally high in the first year of life; it declines in other ages of childhood and through most of the teenage years, increasing slowly in adult ages and especially in old age. The Weibull distribution is also appropriate for hazards that are either monotonically decreasing or rising (Blossfeld and Rowher 2002). The model is estimated by the Stata software (StataCorp 2003), which constructs the likelihood function of the study’s observations, maximizing the resulting function with respect to the unknown parameters, β, λ, and γ.
The hazard model with frailty assumes that the individual risk of death is a function of measured factors (Eq. 1) and a random perturbation on the baseline hazard due to the unobserved family effect. The model is of the form:
for data consisting of n groups with jth group comprised of n i observations. The index j denotes the group (j = 1,...,n), while i denotes the observation within group, (i = 1,...,n i ). In this study, the indexes i and j correspond to children and mothers, respectively. The frailty, α j , is a random positive quantity shared within the families, which for purposes of model identifiability is assumed to have a mean of one and variance, θ. Being unobserved, frailty is captured by its variance, θ, and is assumed to follow a gamma distribution (Sastry 1996; Oakes 1982). It is estimated from the data and measures the variability of frailty across families. A variance estimate that is significantly different from zero will indicate that unmeasured and unmeasurable factors shared by siblings affect the risk of death and that their survival risks are correlated. If the variance estimate is zero, it means that all families have the same risk of death, that is, mortality does not differ between families. Unlike the nonfrailty models, frailty models do not estimate a unique risk of death for children with particular characteristics. The risk of death in frailty models depends on both the measured factors and the unmeasured family effect. Their resulting hazard ratios are therefore family-specific and measure the effect of a particular variable on the risk of death within a particular family (Cleves et al. 2004).
Control variables
This paper aims to assess the extent to which shared familial factors, but which are unmeasured, affect child survival net of observed factors. The selection of the observed factors is based on the Mosley and Chen (1984) conceptual framework and existing literature on child mortality (see, for example, Rutstein 2000; Manda 1999; Sastry 1997c; Kuate-Defo 1996). In the Mosley and Chen framework all socioeconomic and sociocultural determinants of child mortality operate through a common set of five proximate determinants (maternal factors, household environmental contamination, nutrient deficiency, injury, and personal illness control) to affect child health. The socioeconomic factors included in this study are maternal education, migration status, household socioeconomic status, and year of child’s birth, while the sociocultural factors are ethnicity, marital status and type of marriage, and religion. The proximate factors include survival status of the preceding sibling, preceding birth interval, maternal age at birth of child, source of water, and type of toilet facility.
Table 1 presents the distribution of the variables selected for this analysis by number of births and deaths. Except for migration status and household socioeconomic status, the other variables are self-explanatory. Migration status was constructed using maternal current and childhood place of residence. Nonmigrants comprise women whose current and childhood place of residence is the same, while migrants are women for whom either of the places of residence is different. Ownership of household items, itself a proxy of amount of disposable income, is used as a measure of household socioeconomic status. The items used to construct this variable are ownership of radio, television, refrigerator, bicycle, motorcycle, and car. Households in the “low” socioeconomic status category do not own any of the items; those in the “medium” category own either a radio or bicycle, while households in the “high” category own a television, refrigerator, motorcycle, or car.
There were very few observations with missing information on the selected variables. The numbers ranged from 31 (maternal childhood place of residence) to 155 (whether household has a refrigerator). In this case, the observations were retained and assigned the mean value for the particular variable or the value for the “other” category as appropriate. However, since the numbers of children with missing information relative to the overall sample are very small the recoding will have minimal impact on the results reported here.
Results
Descriptive analysis
In order to undertake an analysis controlling for frailty it is first necessary to examine the distribution of births and deaths to determine the potential correlation of children born to the same mother. The distribution of births and child deaths from the 1998 DHS for Kenya, are presented in Tables 2 and 3, respectively. Table 2 shows that over 80% of the families contribute two or more births to the sample. Only 38% of the families have five or more children, and yet these children make up about two-thirds of total children.
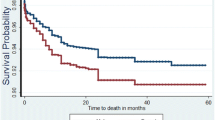
The results in Table 3 show that 2,325 of the children had died either in infancy or childhood, suggesting that one in ten children do not live to see their fifth birthday. Further description of the mortality in the population is provided by Fig. 1, which shows the survival functions of all children in the data set. The results show that 70 per 1,000 children had died by age one, 85 per 1,000 had died by age two, while 104 per 1,000 children had died by age five. Table 3 also provides evidence of substantial clustering of child deaths in certain families. The 2,325 deaths occurred to 1,483 families; 4,233 families had never experienced a child death. About 33% of the deaths occurred to 4% of the families with three or more child deaths. Slightly over 1% of the families contribute four or more deaths; together they account for about 18% of the deaths. There is therefore a need to explicitly account for the correlation between siblings and to assess the contribution of unobserved factors to the risk of child death.

Child survival plot for all children in Kenya, DHS 1998
Weibull hazard models results
For both infant and child mortality we estimate two models that assume that siblings’ survival risks are uncorrelated, and two additional models that control for frailty. The first model in each case includes socioeconomic and sociocultural factors, while the second adds household environmental conditions and biodemographic factors. This analytic strategy allows us to examine how the effects of background variables that are assumed to be distant from the event of death change as proximate determinants are added to the model. The separation of the analysis into infant and child mortality enables us to determine the relative contribution of the selected factors on the risk of death both in infancy and in childhood. This is important in identifying factors that could be targeted in the design of intervention programs at different age periods in childhood.
Infant mortality
Table 4 presents the results from fitting the four hazard models for infant mortality. The results show that a total of 1,620 children died in infancy, with 403 of these being firstborns. Hazard ratios greater than unity signify an increased risk of death, while those less than unity signify a decreased risk. The interpretation of the hazard ratios is either in terms of the percentage change in the risk of death or the number of times the risk changes. The γ parameters at the bottom of the table indicate that the hazard is declining in all the models, which affirms the choice of the Weibull distribution. For all the models, the chi-squared statistics and log likelihood ratios describing the goodness of fit of the models are significant.
The estimated variance parameters associated with the frailty effect, θ, in the Weibull model are 0.83 and 0.45 in Model I and Model II, respectively. These parameters are highly significant and indicate that survival risks in infancy continue to vary due to unobserved factors shared by siblings. The frailty parameter has direct interpretation in terms of hazard ratio (Guo 1993). The frailty estimate in Model II means that each infant death in a family increases the risk of the death for the index child in infancy by 45% relative to what it would be if the child were alive. The standard errors associated with the hazard ratios of the covariates are consistently higher in the frailty models than in standard Weibull models, hence the wider confidence intervals. Nonetheless, the appreciation is generally small and does not change the significance of any of the parameter estimates. Similarly, the magnitude of effect of the covariates is largely unchanged in the presence of frailty, suggesting that the substantive conclusions from the Weibull standard models are robust to the failure of the statistical assumption of independence. However, in the subsequent pages we report the results of the Weibull frailty models because they are more precise and efficient.
The results in Model I show that all the socioeconomic and sociocultural covariates, controlling for each other, are significantly associated with infant survival. The effect of the variables is also consistent with theoretical expectations and previous research on mortality among children. Model II, which includes controls for household environmental conditions and biodemographic factors, is limited to second and higher order births because information on the survival status of previous child and preceding birth interval does not apply to first births. The model shows significant improvements over Model I as indicated by the higher likelihood ratio and model’s chi-squared statistics. As in childhood also, the change in magnitude of effect and variance of frailty between Models I and II could possibly be due to the reduction in sample size. To test whether this is the case, Model II with a category for firstborns for the preceding birth interval and preceding child survival status was estimated. The results (not shown) indicated that the change in the magnitude of effects was minimal and the direction of the effects of the variables did not change. The conclusions of the models reported here are therefore retained.
Model II exhibits substantial changes in the effects of the covariates from the preceding model. Overall, the magnitude of effect of the distant factors (including maternal education, ethnicity, and religion) is depressed, while that of year of birth is increased. Unlike in Model I, however, household socioeconomic status and migration status are not significantly associated with the risk of death in infancy. Children of mothers with secondary education are about 20% less likely to die compared to those of mothers with primary education. This suggests about 9% of the effect of secondary or higher education operates through the biodemographic factors and household environmental conditions. Children born in the period 1990–1994 are 66%, while those born in the period 1995–1998 are 85% more likely to die compared to those born before 1980. The increase in coefficients associated with the period of birth means that its relationship is better revealed in the presence of biodemographic factors and household environmental conditions. It also possible that there are other factors that are not controlled for that may be associated with the period of birth.
The large disparity between the Luo and the Kikuyu substantially decreases in the model including biodemographic factors and household environmental conditions. Compared to Model I, where children of Luo mothers are about five times more likely to die than those of the Kikuyu, they are now three and half times more likely to die. The hazard ratios for the other ethnic groups also decline substantially in the presence of biodemographic factors and household environmental conditions. A large proportion of the effects of ethnicity therefore operate through observed proximate determinants, including type of toilet facility, birth spacing, survival status of preceding child, and maternal age.
Regarding religion, children of Muslim mothers are about 75% while those of Catholic mothers are 14% more likely to die in infancy compared to children of Protestant mothers. Relative to children of mothers in monogamous unions, children of mothers in polygynous unions are 21% more likely to die in infancy, while those of single mothers are 16% more likely to die, but the relationship is not significant.
Among household environmental conditions indicators, only the type of toilet facility is significantly associated with infant mortality. Living in a household with no toilet facility increases the risk of child death by 20% compared to living in a household with a pit latrine. Although its effect is expected to be stronger in childhood, the results show that the risk of death in infancy is not any less for children living in unhygienic household conditions.
There is a large reduction in the magnitude of the random term between Model I and Model II, which attests to the importance of the biodemographic factors for survival in infancy. The results demonstrate the negative effects of short birth intervals and young and old maternal age at birth on the risk of child death. For example, children born less than 19 months after their preceding siblings are 48% more likely to die compared to those born 19–35 months after preceding siblings. Similarly, children born when their mothers were aged below 20 are 22%, while those born when their mothers were aged 35 and over are 37% more likely to die compared to children born when their mothers were aged 20–24 years.
A comparison in the effect of the death of the preceding child between the standard and frailty models is particularly noteworthy. Its effect reduces from 2.45 in the standard model to 2.05 in the frailty model, a 16% reduction. The result suggests that the death of the previous child is acting as a proxy for unmeasured family factors and is also an indicator of correlated mortality risks among siblings (Omariba 2004; Sastry 1997b; Zenger 1993).
Child mortality
The results regarding relationships between child mortality and different factors are presented in Table 5. The data show that a total of 705 children died between 12 and 59 months, with 158 of these being firstborns. The respective negative log likelihood and chi-squared statistics indicate that the overall models are significant. Further, the γ parameter indicates that for all models the hazard is declining. The frailty effects are substantial and significant (0.93 and 0.98) for child mortality also; the risks of child death between families continue to differ even after controlling for a number of known determinants of mortality. The latter estimate indicates that one child death in a family is associated with a 98% increase in the risk of the index child dying relative to what it would be if the child were alive. These results suggest that, unlike in infant mortality, there is great variation between families in the risk of child mortality that is not accounted by the measured factors. The magnitude of effects of the covariates is smaller and the standard errors are slightly inflated in the frailty models compared to the standard models. Again, since the direction of the effect of the covariates is unchanged the substantive conclusions from the Weibull standard models remain.
The results of the parameter estimates are largely in line with theoretical expectations and patterns observed for infant mortality. However, it is clearly evident that the relative effect of the covariates on child mortality is larger than that observed for infant mortality.
Since we described the results relating to infant mortality, in this section we provide an overview of the patterns shown in the table, comparing them with those of infant mortality where appropriate.
Whereas in infancy, children of mothers with no education face an increased risk of death of 16%, in childhood the increase is one-third. In infancy, the reduction in the risk of death among children of mothers with secondary education is 30%, but in childhood the risk is reduced by about 50%. This pattern is also maintained in the full model including biodemographic factors and household environmental conditions. The estimated effects of maternal education on child mortality in Kenya therefore correspond closely to findings from elsewhere in the less developed world (Rutstein 2000; Desai and Alva 1998).
The effect of household socioeconomic status is stronger for child mortality than for infant mortality. Living in a low socioeconomic household increases the risk of death by over one-fifth, but living in a high socioeconomic one reduces the risk of death by one third. Children born in the 1990–1994 period are about twice as likely, while those born in the 1995–1998 period are over one and half times more likely to die compared to children born before 1980. Unlike infant mortality, however, children born in the 1985–1989 period are more likely to die in childhood, an increase of 34% in the risk of death.
Although children of Luo mothers are the most disadvantaged, being about ten times more likely to die, the differences between children of other ethnic groups and those of the Kikuyu are larger and starker than in infancy. For example, whereas in infancy children of Luhya mothers are only twice as likely to die compared to those of the Kikuyu, they are seven times more likely to die in childhood.
As indicated by the log likelihood and chi-squared statistics, Model II of the Weibull frailty models significantly improves on Model I. However, the effect of household socioeconomic status is not significant while marital status is weakly associated with child survival. The direction of the effect of education, year of birth, and ethnicity is similar to that in Model I, attesting to the robustness of these factors in explaining death in childhood. However, whereas the magnitude of effects of education remains largely unchanged, that of ethnicity is substantially depressed. The attenuation of the parameters suggests that some of their effects operate through household environmental conditions and biodemographic factors. As in infancy, mortality differences by year of birth are more prominently revealed in the presence of biodemographic factors and household environmental conditions.
Just as in infancy, only the type of toilet facility is significantly associated with child death among household environmental conditions factors. Living in households without toilet facilities increased the risk of child death by about one-fifth. These results are congruent with previous research showing that the type of toilet facility is a more important determinant of child survival than water supply (Esrey 1996; Gubhaju et al. 1991).
The magnitude of the effects of biodemographic factors clearly demonstrates that they are less important in childhood relative to infancy. For instance, whereas in infancy a birth interval of less than 19 months is associated with an almost 50% increase in the risk of death, in childhood the increase is only about one-third relative to an interval of 19–35 months. Similarly, an interval of 36 or more months reduces the risk of death by about 32% in infancy, but by 25% in childhood. Only young maternal age (below 20) is significantly associated with the risk of death. This sharply contrasts with infancy, where young and old maternal ages at birth were positively associated with heightened risk of death. The main surprising finding relates to the survival status of the preceding child; unlike in the model without frailty, the death of the preceding child becomes insignificant in the presence of frailty.
Discussion and conclusion
In this paper, we have analyzed the relationships between socioeconomic, sociocultural, and biodemographic factors and household environmental conditions on the risk of child death in Kenya and at the same time controlled for the correlation between mortality risks of siblings using shared frailty hazard models. The largely unchanged frailty effect in the final child mortality models suggests that biodemographic factors are not as important in childhood as in infancy. The effect of the survival status of the preceding child attenuates in infancy, but it remains substantial and significant. However, controlling for frailty effects, the death of the previous child is not significantly associated with the risk of death after infancy. The effects of death of the previous child on the risk of death of the subsequent one, especially the depletion of maternal physiological resources due to shortened birth interval, are well known (Gyimah and Rajulton 2004; Palloni and Rafalimanana 1999; Zenger 1993). However, an obvious but less known hypothesis in demographic literature is maternal depression. Psychiatrists have long identified major loss events as important markers of depression. Maternal depression due to child loss could therefore undermine the health of the subsequent one both before and after birth. A depressed woman may not adhere to proper dietary habits during pregnancy, may suffer sleep loss, and her general ability to care for the child could be less than optimal. Depression is also associated with negative pregnancy outcomes including preterm delivery, low birth weight, and small-for-gestational-age babies, all of which are significant risk factors especially for infant mortality (Steer et al. 1992). Although it is difficult to determine precisely what mechanism is operating in a given situation, the exercise is important for selecting between policy options. If its effect reflects the birth spacing mechanism, improving availability and use of contraception would reduce the risk of child death associated with the death of the older child. However, policy options responding to the depression and replacement mechanisms are less certain. The stronger effect of the death of the preceding child in infancy suggests that the birth interval mechanisms are more important in Kenya.
Maternal depletion effects should be weaker when the preceding child is dead because the physiological demands of lactation are no longer present (Zenger 1993). In Kenya, the cessation of breastfeeding due to a child’s death is, however, likely to lead to earlier subsequent conception because only about 32% of married women use modern contraception (NCPD et al. 1999). Besides the maternal depletion syndrome, short birth intervals increase the number of children of comparable ages in the household. Consequently, this heightens susceptibility of children to infectious diseases due to their physical proximity (Alam 1995) and leads to siblings’ competition for household resources including individualized maternal care (Gribble 1993). However, the difference in the magnitude of effects suggests that the physiological effects of birth intervals are stronger in infancy, while those of competition for household resources are stronger in childhood.
Family planning could also mitigate the negative effects of young and old maternal age at birth on child survival. The effects of maternal age at birth are both physiological and sociopsychological. The immature reproductive systems of young mothers and primaparity and the depleted physiological system of older mothers due to repeated pregnancies makes them susceptible to pregnancy complications and bearing low birthweight babies (Miller 1993) both of which are associated with a higher risk of child death (see Solis et al. 2000). By delaying the next birth, family planning ensures that the mother’s body has sufficient time to recover in readiness for the next birth and also it reduces the number of children women eventually bear, even if they are using it just for spacing. The sociopsychological hypothesis holds that younger mothers are also not yet ready to take parental responsibilities, may not have decision-making authority in the household, and lack financial resources to seek medical care for their children (Alam 2000).
An important mechanism for improving women’s autonomy and decision-making in the household is education (see O’Toole and Wright 1991; Caldwell 1986). Mortality is also lower among children of educated mothers due to higher socioeconomic status and improvement in domestic management of child illness, preventive care strategies, and effective use of modern health services (Das Gupta 1997; Caldwell 1979, 1994). Nonetheless, at higher levels of education it is difficult to measure the effect on child health that is actually attributable to education. Highly educated mothers are not only likely to be working in occupations that afford them the means to improve the household standard of living, but they may also marry men who are more educated and have higher income (see Ware 1984).
Besides socioeconomic factors such as education, the other group of distant factors that were analyzed are sociocultural variables. These factors shape and modify the economic choices and health-related practices of individuals according to the cultural traditions and norms of the society (Mosley and Chen 1984). Cultural traditions and norms influence power relationships in the household, value of children, food preferences, and beliefs about disease causation. Ethnicity and religion are directly related to cultural traditions and norms that affect child survival. On the other hand, type of marriage is more related to household power relations, especially allocation of resources for childcare (see Strassman 1997).
Ethnic mortality differentials are largely attributed to differential levels of socioeconomic development between areas inhabited by the various groups (see Brockerhoff and Hewett 2000). However, in Kenya, cultural differences in childcare practices and beliefs on disease causation and patterns of diseases could be more important. For example, although they both inhabit Nyanza province, the risk of child death in all models was consistently higher among the Luo than the Kisii. The high mortality among children of Luo mothers could be attributed to the high incidence of HIV/AIDS in this group (Kenya Ministry of Health 2001) due to the prevalence of levirate marriage and the belief that HIV/AIDS is caused by witchcraft and/or breaking of certain traditional taboos (Ocholla-Ayayo 1991). Nonetheless, further research especially examining ethnocultural differences in childcare and health related behavior to better understand ethnic mortality differentials is needed.
The results, especially the higher risk of death for children born in the 1990s, support research pointing to the potential effects of HIV/AIDS (Hill et al. 2001; Nyambedha et al. 2001). In particular, controlling for other factors strengthened the year of birth effects and the effect of unmeasured factors is substantial. The effects of HIV/AIDS on child survival are both direct and indirect. The direct effect operates through mother-to-child infection during pregnancy or at delivery, while the indirect effects are manifested through death of parents. Orphans face diverse problems including lack of food and abuse from relatives while some are forced into child labor (Yamano and Jayne 2004; Nyambedha et al. 2003). The effects of AIDS are likely to persist given that there is no cure and because of the slow pace and logistical problems associated with availing retroviral medicines to the infected. Generally, however, the examination of the direct relationship between HIV/AIDS and the risk of child death is hampered by lack of data.
An important issue raised by this analysis is that of the reliability of the data used to make mortality estimates. The large differences between ethnic groups in particular could be an indication of differential willingness to recall child deaths across ethnic groups or that deaths farther back in time were more subject to recall errors. Hill et al. (2001) examined whether mortality trends were an artifact of the survey by including a dummy variable for the round of survey, estimated for overlapping time periods in their models. The variable did not have an effect on the odds ratios of the time periods. However, understanding differential cultural approaches to death and to the remembering of dead children would require ethnographic data.
The type of toilet facility and source of water reflect the level of environmental contamination, which determines the transmission of infectious agents to children (Mosley and Chen 1984). These factors also serve as a proxy for information unavailable from the survey including household hygiene, standards of cleanliness, and food preparation and storage practices. Although the results on type of toilet facility were consistent with the theoretical expectations and previous research, the effect of source of water was statistically insignificant. The result is surprising because only about 20% of children live in households using piped water (Table 1). Since the majority of the population relies on unsafe water sources, conditions of use, including manner of storage and whether families treat the water before using it, would be more important.
Comparable results from adjusting for correlated survival experiences of siblings have been observed elsewhere and under different cultural settings (Guo 1993; Curtis et al. 1993). This creates the impression that adjusting for correlated observations does not bring any benefit to the analysis of mortality determinants, more so because the substantive conclusions remain unchanged. Beyond correcting for biased standard errors, models with frailty are also of substantive interest. The fact that the risk of child death is not completely captured by the analyzed factors is important in the sense that it points to unmeasured factors. This analysis did not include breastfeeding and healthcare factors because the information was collected only for children born in the 3 years preceding the survey. One way to assess whether these are important is to restrict the analysis to children born 3 years before the survey. The exclusion of these important determinants of child survival therefore inflates the magnitude of the frailty effect. The substantial frailty estimate also corroborates the descriptive findings (Table 2) and suggests that deaths are likely to cluster in families due to unmeasured factors. In Kenya, one such factor, HIV/AIDS, has already been suggested. Although HIV/AIDS is differentially distributed in the population, programs to mitigate its effect such as aggressive provision of retroviral medicine, counseling, and information and education campaigns targeting behavior change will benefit everyone.
Although this study has demonstrated that child mortality risks vary due to unobserved factors at the family level, unobserved heterogeneity at the community level is also important. Children in the same community live under similar climatic, environmental, socioeconomic, and cultural conditions and are exposed to the same illness and diseases prevalent in the community (Sastry 1997b). The results of our frailty models suggest that the effects of unmeasured environmental factors and community factors such as availability of hospitals and economic resources are likely to be important for child mortality. Consequently, the frailty magnitude in the current study could be inflated by the unobserved community effects. However, a major limitation of the DHS data is that it does not collect community information. Future studies should therefore endeavor to include community factors where they are available.
References
Alam, N. (1995). Birth spacing and infant and early childhood mortality in a high fertility area of Bangladesh: Age-dependent and interactive effects. Journal of Biosocial Science, 27(3), 393–404.
Alam, N. (2000). Teenage motherhood and infant mortality in Bangladesh: Maternal age-dependent effect of parity one. Journal of Biosocial Science, 32(2), 229–236.
Blossfeld, H.-P., & Rowher, G. (2002). Techniques of event history modelling: New approaches to causal analysis. London, England: Lawrence Erlbaum Associates.
Brass, W. (1993). Child mortality improvement and the initiation of fertility falls in Kenya. In International Union for the Scientific Study of Population [IUSSP] (Eds.), International population conference, Montreal, 1993, Vol. I (pp. 73–80). Liège, Belgium: IUSSP.
Brockerhoff, M., & Hewitt, P. (2000). Inequality of child mortality among ethnic groups in sub-Saharan Africa. Bulletin of the World Health Organization, 78(1), 30–41.
Caldwell, J. C. (1979). Education as a factor in mortality decline: An examination of Nigerian data. Population Studies, 3, 395–414.
Caldwell, J. C. (1986). Routes to low mortality in poor countries. Population and Development Review, 12(2), 171–219.
Caldwell, J. C. (1994). How is greater maternal education translated into lower child mortality? Health Transition Review, 4, 224–229.
Central Bureau of Statistics [Kenya] Ministry of Health [Kenya] & ORC Macro. (2004). Kenya demographic and health survey 2003. Calverton MD: CBS, MOH & ORC Macro.
Cleves, M. A., Gould, W. W., & Gutierrez, R. G. (2004). An introduction to survival analysis using Stata. College Station, TX: Stata Corporation.
Cox, D. R. (1972). Regression models and life tables (with discussion). Journal of the Royal Statistical Society Series B, 34, 187–220.
Curtis, S. L., Diamond, I., & McDonald, J. W. (1993). Birth interval and family effects on postneonatal and mortality in Brazil. Demography, 30(1), 33–43.
Das Gupta, M. (1990). Death clustering, mothers’ education and the determinants of child mortality in rural Punjab, India. Population Studies, 44, 489–505.
Das Gupta, M. (1997). Socioeconomic status and clustering of child deaths in rural Punjab. Population Studies, 51, 191–202.
Desai, S., & Alva, S. (1998). Maternal education and child health: Is there a strong causal relationship? Demography, 35(1), 71–81.
Esrey, S. (1996). Water, waste and well-being: A multicountry study. American Journal of Epidemiology, 143(6), 608–623.
Gribble, J. N. (1993). Birth intervals, gestational age, and low birth weight: Are the relationships confounded? Population Studies, 47, 133–146.
Gubhaju, B. B., Streatfield, K., & Majumder, A. K. (1991). Socioeconomic, demographic and environmental determinants of infant mortality in Nepal. Journal of Biosocial Science, 23, 425–436.
Guo, G. (1993). Use of sibling data to estimate family mortality effects in Guatemala. Demography, 30(1), 15–32.
Guo, G., & Zhao, H. (2000). Multilevel modelling for binary data. Annual Review Sociology, 26, 441–462.
Gyimah, S. O., & Rajulton, F. (2004). Intentional replacement of dead children in sub-Saharan Africa: Evidence from Ghana and Kenya. Canadian Studies in Population, 31(1), 33–53.
Hill, A. (1992). Trends in childhood mortality in sub-Saharan mainland Africa. In E. van de Walle, P. Gilles, & M. Sala-Diakanda (Eds.), Mortality and society in sub-Saharan Africa (pp. 10–31). Oxford, England: Clarendon Press.
Hill, K., Bicego, G., & Mahy, M. (2001). Childhood mortality in Kenya: An examination of trends and determinants in the late 1980s to mid 1990s. Working paper 01-01. John Hopkins University, Hopkins Population Center.
Kenya Ministry of Health. (2001). AIDS in Kenya: Background, projections, interventions and policy (6th ed.). Nairobi, Kenya: National AIDS and STD Control.
Kuate-Defo, B. (1996). Areal and socioeconomic differentials in infant and child mortality in Cameroon. Social Science and Medicine, 42(3), 399–420.
Madise, N., & Diamond, I. (1995). Determinants of infant mortality in Malawi: An analysis to control for death clustering within families. Journal of Biosocial Science, 27(1), 95–106.
Magadi, M. A., Diamond, I., & Rodrigues, R. N. (2001). The determinants of delivery care in Kenya. Social Biology, 47(3–4), 164–188.
Manda, S. O. M. (1999). Birth intervals, breastfeeding and determinants of childhood mortality in Malawi. Social Science and Medicine, 48, 301–312.
Marckwardt, A. M., & Rutstein, S. O. (1996). Accuracy of DHS-II demographic data: Gains and losses in comparison with earlier surveys. DHS Working papers 19. Macro International Inc.
Miller, J. E. (1993). Birth outcomes by mother’s age at first birth in the Philippines. International Family Planning Perspectives, 19, 98–102.
Mosley, W. H., & Chen, L. C. (1984). An analytical framework for the study of child survival in developing countries. Population and Development Review, 10(Suppl.), 25–45.
National Council for Population & Development [NCPD], Central Bureau of Statistics [CBS], & Macro International [MI]. (1999). Kenya demographic and health survey 1998. Calverton MD: NCPD, CBS, and MI.
Nyambedha, E. O., Wandibba S., & Aagaard-Hansen, J. (2001). Policy implications of the inadequate support systems for orphans in Western Kenya. Health Policy, 58, 83–96.
Nyambedha, E. O., Wandibba, S., & Aagaard-Hansen, J. (2003). Changing patterns of orphan care due to the HIV epidemic in western Kenya. Social Science and Medicine, 57, 301–311.
Oakes, D. (1982). A model for association in bivariate survival data. Journal of Royal Statistical Society Series B, 44(3), 414–422.
Ocholla-Ayayo, A. B. C. (1991). The spirit of a nation. Nairobi, Kenya: Shirikon Publishers.
Omariba, D. W. R. (2004). Levels, trends and correlates of child mortality in Kenya: An exploration into the phenomenon of death clustering. Ph.D. Dissertation, Faculty of Graduate Studies, The University of Western Ontario, London, Canada.
O’Toole, J. O., & Wright, R. E. (1991). Parental education and child mortality in Burundi. Journal of Biosocial Science, 23, 255–262.
Palloni, A., & Rafalimanana, H. (1999). The effects of infant mortality on fertility revisited: New evidence from Latin America. Demography, 36(1), 41–58.
Pebley, A. R., Goldman, N., & Rodriguez, G. (1996). Prenatal and delivery care and childhood immunization in Guatemala: Do family and community matter? Demography 33(2), 231–247.
Rutstein, S. O. (2000). Factors associated with trends in infant and child mortality in developing countries during the 1990s. Bulletin of the World Health Organization, 78, 1256–1270.
Sastry, N. (1996). Community characteristics, individual and household attributes, and child survival in Brazil. Demography, 33(2), 211–229.
Sastry, N. (1997a). A nested frailty model for survival data, with an application of child survival in Northeast Brazil. Journal of the American Statistical Association, 92(438), 426–435.
Sastry, N. (1997b). Family-level clustering of childhood mortality risk in northeast Brazil. Population Studies, 51, 245–261.
Sastry, N. (1997c). What explains rural–urban differentials in child mortality in Brazil? Social Science & Medicine, 44(7), 899–1002.
Solis, P., Pullum, S. G., & Frisbie, W. P. (2000). Demographic models of birth outcomes and infant mortality: An alternative approach. Demography, 37(4), 489–498.
Stata Corp. (2003). Stata statistical software: Release 8.0. College Station, TX: Stata Corporation.
Steer, R. A., Scholl, T. O., Hediger, M. L., & Fischer, R. L. (1992). Self-reported depression and negative pregnancy outcomes. Journal of Clinical Epidemiology, 45(10), 1093–1099.
Strassman, B. I. (1997). Polygyny as a risk factor for child mortality among the Dogon. Current Anthropology, 38(4), 688–695.
Trussell, J., & Rodríguez, G. (1990). Heterogeneity in demographic research. In J. Adams, D. A. Lam, A. I. Hermalin, & P. E. Smouse (Eds.), Convergent issues in genetics and demography (pp. 112–132). London, England: Oxford University Press.
Vaupel, J. W. (1989). Kindred lifetimes: Frailty models in population genetics. In J. Adams, D. A. Lam, A. I. Hermalin, & P. E. Smouse (Eds.), Convergent issues in genetics and demography (pp. 155–170). New York: Oxford University Press.
Ware, H. (1984). Effects of maternal education, women’s roles, and child care on child mortality. Population and Development Review, 10(Suppl.), 191–214.
Yamano, T., & Jayne, T. S. (2004). Measuring the impacts of working-age adult mortality on small-scale farm households in Kenya. World Development, 32(1), 91–119.
Zenger, E. (1993). Siblings’ neonatal morality risks and birth spacing in Bangladesh. Demography, 30(3), 477–488.
Acknowledgments
The authors are grateful for very helpful comments provided by Stephen Gyimah and two anonymous reviewers on earlier versions of this paper. This study was completed while D. Walter Rasugu Omariba was a postdoctoral fellow at the Offord Centre for Child Studies, McMaster University with funding from the Institute of Population and Public Health of the Canadian Institutes of Health Research (CIHR).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Omariba, D.W.R., Beaujot, R. & Rajulton, F. Determinants of infant and child mortality in Kenya: an analysis controlling for frailty effects. Popul Res Policy Rev 26, 299–321 (2007). https://doi.org/10.1007/s11113-007-9031-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11113-007-9031-z