
Abstract
Context
In sporadic acromegaly, overall AIPmut prevalence is reported as 3, 4.1 and 16 % in studies carried out across Europe. However, it is not known whether the prevalence shows any changes across different ethnicities. The aim of the study was to identify prevalence of AIPmut in a series of Turkish acromegalic patients.
Patients and methods
Direct sequencing of AIP gene was performed in 92 sporadic acromegalic patients.
Results
One patient was found to have a new mutation in exon 6: g67.258,286 (G/A) heterozygote; (GGC/GAC; gly/asp). Apart from this new mutation, previously defined synonymous mutations in AIP gene were detected in seven patients (Exon 4; rs2276020; (GAC/GAT; asp/asp) and six patients were found to have five different intronic mutations in AIP gene which were not previously defined. The patient with pathogenic AIPmut presented at a young age and had an aggressive and treatment resistant tumour. The prevalence of AIPmut in Turkish patients was found to be 1 % in sporadic acromegaly in the present study. In addition, one synonymous mutation which was previously defined and six new intronic mutations have been described in Turkish acromegalic patients. All acromegalic patients with synonymous AIPmut presented with macroadenoma and majority of them had invasive tumour.
Conclusion
The prevalence of AIPmut in Turkish patients was found to be 1 % in sporadic acromegaly in the present study. This ratio increases when younger age groups are taken into account 6 % among patients <30 years of age at the time of diagnosis of acromegaly. The clinical features of acromegaly, such as having large and invasive tumours, may be affected by the presence of synonymous AIPmut.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acromegaly is a rare clinical entity caused in at least 95 % of cases by a growth hormone (GH)-secreting pituitary adenoma. Although benign, excessive production of GH is associated with diabetes mellitus, hypertension and cardiovascular diseases hence increased mortality if left untreated.
Majority of these tumors are sporadic, but a minority of them may present as a part of multiple endocrine neoplasia type 1 and type 4 (MEN1 and MEN4), Carney complex, McCune Albright syndrome or familial isolated pituitary adenoma (FIPA). If two or more cases of acromegaly or gigantism are present in a single family without other features of these syndromes, it is called isolated familial somatotropinomas (IFS). IFS account for 18–30 % of familial isolated pituitary adenoma (FIPAs) [1, 2].
Germline aryl hydrocarbon receptor interacting protein (AIP) mutations (AIPmut) can be found in about 20 % of FIPA and 40 % of IFS families [3–5]. However AIPmut is rare in sporadic pituitary adenomas, except in young patients with GH-secreting adenomas [6–8]. The genetic causes of acromegaly in young patients with pituitary adenomas are AIP and MEN1, but very recently the new Xq26.3 microduplications were also found to be related to GH secreting pituitary adenomas in very young patients, too [9] It has been suggested that molecular genetic testing for AIPmut should be considered in (1) patients fulfilling the criteria for FIPA, (2) patients with any pituitary adenoma diagnosed before age of 18, (3) patients with a pituitary macroadenoma diagnosed before age of 30 [5].
In sporadic acromegaly, overall AIPmut prevalence is reported as 3, 4.1 and 16 % in studies carried out in Italy, France and Finland [10–12]. However, it is not known whether the prevalence shows any changes across different ethnicities. In order to answer this question, we analyzed apparently sporadic acromegalic Turkish patients for the presence of AIP mutation. We have also investigated the frequency of synonymous and intronic mutations in AIP gene and their importancy in terms of clinical presentation.
Materials and methods
The study was approved by Local Ethics Committee and all patients were gave their written informed consent. Clinical trial Gov. Number: NCT01902420.
Study population
Ninety-two patients with sporadic acromegaly (based on the absence of family history of GH secreting or other types of pituitary adenomas) who were followed up in Erciyes University Medical School were enrolled into the study. Clinical data of the patients were obtained retrospectively from medical records. The current age and age at diagnosis of the patients, disease duration, features of adenoma at the time of diagnosis were recorded. Tumours with extrasellar extension, tumours invading cavernous sinus and surrounding brain structures radiologically were classified as invasive tumours. The treatments received and treatment responses of the patients were evaluated. ‘Complete response’ was defined as having normal IGF-1 levels according to age and sex and suppressed GH ≤ 1 μg/L after OGTT or having a safe basal GH level ≤ 2.5 μg/L for the patients receiving somatostatin analog (SSA) therapy. ‘Partial response’ was defined as having a reduced, but still elevated, IGF-1 of <50 % of the baseline level and suppressed GH ≤ 1 μg/L after OGTT or having a safe basal GH level. All other cases were defined as ‘treatment failure’ [13–15]. The tumoral response was also assessed according to last pituitary imaging studies. Presence of residual tumour, increment or decrement in the size of the tumour were evaluated on pituitary MRI. Twenty healthy individuals without a history of another disease, who did not carry the clinical features of acromegaly or other pituitary adenomas were selected as the control group.
AIP genetic analysis
Genomic DNA was isolated from blood samples from acromegaly patients. The primers used for the analysis of the AIP exonic and flanking intronic sequences are as reported by Rowlands et al. [16]. The following sequences obtained from GenBank were used as reference sequences of AIP NT_167190.1 (genomic), NM_003977.2 (mRNA). Each AIP exon from each DNA sample was amplified by PCR (SensQuest Labcycler, Qiagen) and PCR reactions were performed by ExPrime Taq premix (Genet Bio, Korea). AIP gene PCR primers for six exons are listed in suppl Table 1 (Synthesized at Metabion, Germany). Amplification program was in 30 cycles of: 30 s at 95 °C; 20 s at 60 °C and 30 s at 72 °C. The PCR products were electrophoresised in a 1.5 % agarose gel stained with ethidium bromide Each PCR reaction was purified using OMEGA bio-tek kit (OMEGA, Norcross, GA). Mutation analysis of purified PCR products was performed by direct sequencing of genomic DNA using Beckman CEQ8000 DNA sequencer (Beckman Coulter, USA). The whole coding region of AIP gene was sequenced, as well as flanking intronic sequences and 5′ and 3′ untranslated regions.
Results
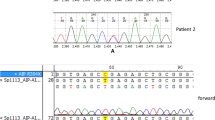
AIP gene sequence analyses were carried out succesfully in all patients. One patient was found to have a new mutation in exon 6: g67.258,286 (G/A) heterozygote; (GGC/GAC; gly/asp) (Fig. 1). This AIPmut was not previously defined in the literature or found in the control group.

Pathogenic new mutation (patient initials: FD): Exon-6 g67.258.286(G/A) heterozygote (GGC/GAC; gly/asp, G272A, c.815G > A) mutation
The patient with pathogenic AIPmut was 50 years old at the time of evaluation. She was diagnosed with acromegaly at the age of 21. The patient had a pituitary adenoma which was 3.5 cm in its largest diameter on MRI. She was operated on and received radiotherapy following operation in another center. The patient had 2nd and 3rd surgeries in the 15th and 20th years of diagnosis since she had hormonally active recurrent adenoma. Gamma-knife radiosurgery was applied in 2003 due to partial resistance to SSA and dopamine agonist (DA) combination therapy. Hormonal control was achieved after the addition of pegvisomant to her treatment when the drug was available in Turkey. The patient was also treated with hydrocortisone and levothyroxine for hypopituitarism.
This patient did not have any relatives with acromegaly or pituitary adenoma. AIP mutation could be studied in DNA samples of her sister and her daughter. Her sister was found to be normal in terms of AIP gene, but the patient’s daughter was found to have similar mutation with the patient. The daughter is 25 years old. She does not have any acromegaloid features, but since the daughter was 8 weeks pregnant when she was called for laboratory evaluation, the evaluation was postponed to postpartum period.
The prevalence of AIPmut was found to be 1 % among Turkish patients with sporadic acromegaly. The prevalence was 6 % when patients <30 years of age at the time of diagnosis and sporadic acromegaly (n = 16) were considered. The prevalence of AIPmut was calculated as 9 % among patients <30 years of age with a macroadenoma (n = 11).
Apart from this new mutation, previously defined synonymous mutations in AIP gene were detected in seven patients (Exon 4; rs2276020; (GAC/GAT; asp/asp) and six patients were found to have five different intronic mutations in AIP gene which were not previously defined. The clinical data and treatment responses of patients according to the presence of AIPmut are presented in Table 1. All patients with a synonymous mutation had a macroadenoma at presentation and five of them had an invasive tumour. The largest tumour diameter was higher in these patients than in patients without a mutation (Table 1). The clinical features of patients with intronic mutations in AIP gene were not different from the ones without an intronic AIPmut.
Discussion
In this study, a new AIPmut was found in exon 6: g.67.258,286 (G/A) heterozygote; (GGC/GAC; gly/asp, G272A, c.815G > A). To date 53 different AIPmut was identified. All these mutations are germline mutations including different types such as nonsense, missense, splice site, insertion, deletion, frameshift and promoter region mutations or heterozygous deletion of most or entire AIP gene. Nonsense or frameshifts leading to truncation of AIP protein structure compromise half of the reported AIPmut [17]. The G272A change has not been previously reported in the clinical setting. This mutation leads to conversion of glycine to aspartic acid in exon 6 of AIP gene. It is generally believed that the AIP protein acts as a tumor suppressor gene and that the product of a single normal allele is sufficient to prevent tumorigenesis. A second somatic mutation (‘second hit’) is necessary to loose the expression of the normal allele and to cause disease. When AIP activity is lost, it has been shown recently that the mechanism of tumorigenesis is related to the loss of inhibition of cAMP synthesis due to alteration in the function of inhibitory G-protein Gai2 [18, 19].
The human AIP gene encodes a 37-kDa protein composed of 330 amino acids that has an N-terminal immunophilin like domain and C-terminal tetratricopeptide repeat (TPR) domains [20, 21]. Approximately 75 % of AIP mutations completely disrupt the C-terminal TPR domain and/or the Cα 7 h [17, 22], suggesting that these domains have an important role in the function of AIP as a tumor suppressor. However, the exact mechanisms of tumor suppression by AIP are poorly understood. The present study reinforces the importance of the C-terminal region of AIP for pituitary tumorigenesis.
This patient with a new AIPmut was diagnosed with acromegaly at a young age with a large tumour. She was operated on for three times, received conventional and gamma-knife radiotherapies at different times. The patient was resistant to DA and SSA and hormonal control could be achieved only after pegvisomant addition. AIPmut in acromegalic patients was found to be associated with male sex, gigantism or PRL cosecretion more frequently besides higher GH levels than in patients without a mutation [4]. Acromegalic patients who carry an AIPmut were shown to require reoperation and/or radiotherapy more frequently [4, 23, 24] and both hormonal and tumoral response to SSA was found to be less in these patients [4]. Oriola et al. [24] investigated 50 acromegalic patients who were resistant to SSA and found mutations or variance of unknown significance in AIP gene in 8 % of the patients. So when presentation features and treatment responses of this patient were considered, the risk of this patient to carry an AIP mutation was increased.
Only two relatives of the patient could be studied for the presence of AIPmut. The sister of the patient was found to be normal, but the daughter revealed similar mutation in the AIP gene with the patient. Although the daughter could not be evaluated by hormonal analysis or pituitary MRI since she was pregnant when she was called for evaluation, she did not have any acromegaloid features. Due to the low penetrance of the disease, the probability of being only a carrier for the AIPmut is expected to be high for her daughter [25]. In sporadic acromegaly, overall AIP mutation prevalence was reported as 3.1–16 % [10–12, 26]. In selected acromegalic populations such as patients diagnosed with a macroadenoma before the age of 30, the ratio is reported as 2.3 or 13.3 % in different studies [18, 27] or patients diagnosed before the age 40 as 4 % [28] or patients with resistance to SSA as 4 % [24]. These studies were carried out in patients from different regions of Europe. The prevalence of AIPmut in Turkish patients was found to be 1 % in sporadic acromegaly in the present study.
The necessity of screening for the presence of AIPmut in FIPA is already known. However, studies carried out in the last years led to a suggestion of screening for the presence of AIPmut in patients with a pituitary adenoma diagnosed before the age of 18 or a pituitary macroadenoma diagnosed before the age of 30 [5]. The risks of carrying AIPmut in these groups of patients are 20 and 11 % respectively [4, 18, 23, 29]. There were no patients diagnosed before age 18 years in the present study, but in patients who were diagnosed at an age <30 years (n = 16), the prevalence of AIPmut was found to be 6 % and in patients who were diagnosed at an age <30 years with a macroadenoma (n = 11), the prevalence was found to be 9 %. Although the number of patients in these selected groups is very limited to derive a direct conclusion, the findings support the importance of young age and tumour size for the risk of carrying an AIPmut.
Previously defined synonymous mutations in AIP gene were detected in seven patients (Exon 4; rs2276020; (GAC/GAT; asp/asp). This polymorphism did not change the amino acid residue (asp) but it may be clinically significant. However, all patients with synonymous mutations had a macroadenoma at presentation and five of them had an invasive tumour. The tumour diameter on pituitary MRI was higher in these patients. Synonymous mutations may lead to sequential changes on mRNA. These changes on mRNA have been reported result in degradation or functional loss of mRNA by modifying its folding pattern [30]. So the presence of synonymous AIPmut may also have clinical importance in terms of tumour size and local invasion. Synonymous codon changes were previously thought to have no functional consequence. Although this concept has been overturned in recent years, there is no unique mechanism by which these changes exert biological effects [31]. Igreja et al. showed that synonymous c.807C > T mutation reduces expression of AIP gene in their study. They had identified synonymous mutations at the beginning of exon 6 in a family with two somatotrophinomas [32]. Synonymous SNPs are the most polymorphic ones, indicating that most such mutations may be functionally neutral. However, this does not mean that every synonymous site is non-functional or neutral. Studies in E. coli, yeast, and Drosophila support translation selection for major codons, and there is a strong correlation between bias in synonymous codon (SC) usage and the gene expression level. An effect of synonymous codon usage on gene expression is supported by the detection of epistatic interactions between nucleotides that are important in maintaining pre-mRNA/mRNA secondary structures [33–36]. In addition, some synonymous changes in humans have been shown to cause genetic disorders by exon skipping [37, 38]. As a result, synonymous mutations are thought to lead to decreased mRNA translation and decreased mRNA stability [39].
Six patients were found to have five different intronic mutations in AIP gene which were not previously defined. Although the number of patients was low, the clinical features of them were not different from the ones without intronic AIPmut. Normally intronic region of DNA is not associated with protein synthesis. So they are not expected to cause functional or structural changes in the protein. In order to understand to full effects of these mutations, functional analysis is necessary.
Although we called the other changes in AIP gene namely exonic synonymous and intronic mutations, they were not included in the prevalence of AIPmut in this series. In a review by Beckers et al. [17], intronic/splicing mutations were suggested to be labeled as variance of unknown significance until data regarding clear deleterious effects of genetic variants are present.
In conclusion, the prevalence of AIPmut in Turkish patients was found to be 1 % in sporadic acromegaly in the present study. The prevalence was found to be 6 % among patients <30 years of age at the time of diagnosis and 9 % among patients <30 years of age with a macroadenoma. All acromegalic patients with synonymous AIPmut presented with macroadenoma and majority of them had invasive tumour. This may suggest that the clinical features of acromegaly may be affected by the presence of synonymous AIPmut although the mutation does not change protein structure. Further studies concentrating on the effects of synonymous and intronic AIPmut would be helpful to understand their clinical effects.
References
Beckers A, Daly AF (2007) The clinical, pathological, and genetic features of familial isolated pituitary adenomas. Eur J Endocrinol 157(4):371–382
Daly AF, Tichomirowa MA, Beckers A (2009) Genetic, molecular and clinical features of familial isolated pituitary adenomas. Horm Res 71(Suppl 2):116–122
Daly AF, Vanbellinghen JF, Khoo SK, Jaffrain-Rea ML, Naves LA, Guitelman MA, Murat A, Emy P, Gimenez-Roqueplo AP, Tamburrano G, Raverot G, Barlier A, De HW, Penfornis A, Ciccarelli E, Estour B, Lecomte P, Gatta B, Chabre O, Sabate MI, Bertagna X, Garcia BN, Stalldecker G, Colao A, Ferolla P, Wemeau JL, Caron P, Sadoul JL, Oneto A, Archambeaud F, Calender A, Sinilnikova O, Montanana CF, Cavagnini F, Hana V, Solano A, Delettieres D, Luccio-Camelo DC, Basso A, Rohmer V, Brue T, Bours V, Teh BT, Beckers A (2007) Aryl hydrocarbon receptor-interacting protein gene mutations in familial isolated pituitary adenomas: analysis in 73 families. J Clin Endocrinol Metab 92(5):1891–1896
Daly AF, Tichomirowa MA, Petrossians P, Heliovaara E, Jaffrain-Rea ML, Barlier A, Naves LA, Ebeling T, Karhu A, Raappana A, Cazabat L, De ME, Montanana CF, Raverot G, Weil RJ, Sane T, Maiter D, Neggers S, Yaneva M, Tabarin A, Verrua E, Eloranta E, Murat A, Vierimaa O, Salmela PI, Emy P, Toledo RA, Sabate MI, Villa C, Popelier M, Salvatori R, Jennings J, Longas AF, Labarta Aizpun JI, Georgitsi M, Paschke R, Ronchi C, Valimaki M, Saloranta C, De HW, Cozzi R, Guitelman M, Magri F, Lagonigro MS, Halaby G, Corman V, Hagelstein MT, Vanbellinghen JF, Barra GB, Gimenez-Roqueplo AP, Cameron FJ, Borson-Chazot F, Holdaway I, Toledo SP, Stalla GK, Spada A, Zacharieva S, Bertherat J, Brue T, Bours V, Chanson P, Aaltonen LA, Beckers A (2010) Clinical characteristics and therapeutic responses in patients with germ-line AIP mutations and pituitary adenomas: an international collaborative study. J Clin Endocrinol Metab 95(11):E373–E383
Korbonits M, Storr H, Kumar AV (2012) Familial pituitary adenomas: who should be tested for AIP mutations? Clin Endocrinol (Oxf) 77(3):351–356
Barlier A, Vanbellinghen JF, Daly AF, Silvy M, Jaffrain-Rea ML, Trouillas J, Tamagno G, Cazabat L, Bours V, Brue T, Enjalbert A, Beckers A (2007) Mutations in the aryl hydrocarbon receptor interacting protein gene are not highly prevalent among subjects with sporadic pituitary adenomas. J Clin Endocrinol Metab 92(5):1952–1955
Cazabat L, Libe R, Perlemoine K, Rene-Corail F, Burnichon N, Gimenez-Roqueplo AP, Dupasquier-Fediaevsky L, Bertagna X, Clauser E, Chanson P, Bertherat J, Raffin-Sanson ML (2007) Germline inactivating mutations of the aryl hydrocarbon receptor-interacting protein gene in a large cohort of sporadic acromegaly: mutations are found in a subset of young patients with macroadenomas. Eur J Endocrinol 157(1):1–8
Georgitsi M, Raitila A, Karhu A, Tuppurainen K, Makinen MJ, Vierimaa O, Paschke R, Saeger W, van der Luijt RB, Sane T, Robledo M, De ME, Weil RJ, Wasik A, Zielinski G, Lucewicz O, Lubinski J, Launonen V, Vahteristo P, Aaltonen LA (2007) Molecular diagnosis of pituitary adenoma predisposition caused by aryl hydrocarbon receptor-interacting protein gene mutations. Proc Natl Acad Sci USA 104(10):4101–4105
Trivellin G, Daly AF, Faucz FR, Yuan B, Rostomyan L, Larco DO, Schernthaner-Reiter MH, Szarek E, Leal LF, Caberg JH, Castermans E, Villa C, Dimopoulos A, Chittiboina P, Xekouki P, Shah N, Metzger D, Lysy PA, Ferrante E, Strebkova N, Mazerkina N, Zatelli MC, Lodish M, Horvath A, de Alexandre RB, Manning AD, Levy I, Keil MF, Sierra ML, Palmeira L, Coppieters W, Georges M, Naves LA, Jamar M, Bours V, Wu TJ, Choong CS, Bertherat J, Chanson P, Kamenicky P, Farrell WE, Barlier A, Quezado M, Bjelobaba I, Stojilkovic SS, Wess J, Costanzi S, Liu P, Lupski JR, Beckers A, Stratakis CA (2014) Gigantism and acromegaly due to Xq26 microduplications and GPR101 mutation. N Engl J Med 371(25):2363–2374
Cazabat L, Bouligand J, Salenave S, Bernier M, Gaillard S, Parker F, Young J, Guiochon-Mantel A, Chanson P (2012) Germline AIP mutations in apparently sporadic pituitary adenomas: prevalence in a prospective single-center cohort of 443 patients. J Clin Endocrinol Metab 97(4):E663–E670
Occhi G, Trivellin G, Ceccato F, De LP, Giorgi G, Dematte S, Grimaldi F, Castello R, Davi MV, Arnaldi G, Salviati L, Opocher G, Mantero F, Scaroni C (2010) Prevalence of AIP mutations in a large series of sporadic Italian acromegalic patients and evaluation of CDKN1B status in acromegalic patients with multiple endocrine neoplasia. Eur J Endocrinol 163(3):369–376
Vierimaa O, Georgitsi M, Lehtonen R, Vahteristo P, Kokko A, Raitila A, Tuppurainen K, Ebeling TM, Salmela PI, Paschke R, Gundogdu S, De ME, Makinen MJ, Launonen V, Karhu A, Aaltonen LA (2006) Pituitary adenoma predisposition caused by germline mutations in the AIP gene. Science 312(5777):1228–1230
Colao A, Cappabianca P, Caron P, De ME, Farrall AJ, Gadelha MR, Hmissi A, Rees A, Reincke M, Safari M, T’Sjoen G, Bouterfa H, Cuneo RC (2009) Octreotide LAR vs. surgery in newly diagnosed patients with acromegaly: a randomized, open-label, multicentre study. Clin Endocrinol (Oxf) 70(5):757–768
Giustina A, Barkan A, Chanson P, Grossman A, Hoffman A, Ghigo E, Casanueva F, Colao A, Lamberts S, Sheppard M, Melmed S (2008) Guidelines for the treatment of growth hormone excess and growth hormone deficiency in adults. J Endocrinol Investig 31(9):820–838
Melmed S, Colao A, Barkan A, Molitch M, Grossman AB, Kleinberg D, Clemmons D, Chanson P, Laws E, Schlechte J, Vance ML, Ho K, Giustina A (2009) Guidelines for acromegaly management: an update. J Clin Endocrinol Metab 94(5):1509–1517
Rowlands JC, Urban JD, Wikoff DS, Budinsky RA (2011) An evaluation of single nucleotide polymorphisms in the human aryl hydrocarbon receptor-interacting protein (AIP) gene. Drug Metab Pharmacokinet 26(4):431–439
Beckers A, Aaltonen LA, Daly AF, Karhu A (2013) Familial isolated pituitary adenomas (FIPA) and the pituitary adenoma predisposition due to mutations in the aryl hydrocarbon receptor interacting protein (AIP) gene. Endocr Rev 34(2):239–277
Tichomirowa MA, Barlier A, Daly AF, Jaffrain-Rea ML, Ronchi C, Yaneva M, Urban JD, Petrossians P, Elenkova A, Tabarin A, Desailloud R, Maiter D, Schurmeyer T, Cozzi R, Theodoropoulou M, Sievers C, Bernabeu I, Naves LA, Chabre O, Montanana CF, Hana V, Halaby G, Delemer B, Aizpun JI, Sonnet E, Longas AF, Hagelstein MT, Caron P, Stalla GK, Bours V, Zacharieva S, Spada A, Brue T, Beckers A (2011) High prevalence of AIP gene mutations following focused screening in young patients with sporadic pituitary macroadenomas. Eur J Endocrinol 165(4):509–515
Tuominen I, Heliovaara E, Raitila A, Rautiainen MR, Mehine M, Katainen R, Donner I, Aittomaki V, Lehtonen HJ, Ahlsten M, Kivipelto L, Schalin-Jantti C, Arola J, Hautaniemi S, Karhu A (2015) AIP inactivation leads to pituitary tumorigenesis through defective Galpha-cAMP signaling. Oncogene 34(9):1174–1184
Linnert M, Haupt K, Lin YJ, Kissing S, Paschke AK, Fischer G, Weiwad M, Lucke C (2012) NMR assignments of the FKBP-type PPIase domain of the human aryl-hydrocarbon receptor-interacting protein (AIP). Biomol NMR Assign 6(2):209–212
Ma Q, Whitlock JP Jr (1997) A novel cytoplasmic protein that interacts with the Ah receptor, contains tetratricopeptide repeat motifs, and augments the transcriptional response to 2,3,7,8-tetrachlorodibenzo-p-dioxin. J Biol Chem 272(14):8878–8884
Martucci F, Trivellin G, Korbonits M (2012) Familial isolated pituitary adenomas: an emerging clinical entity. J Endocrinol Invest 35(11):1003–1014
Chahal HS, Stals K, Unterlander M, Balding DJ, Thomas MG, Kumar AV, Besser GM, Atkinson AB, Morrison PJ, Howlett TA, Levy MJ, Orme SM, Akker SA, Abel RL, Grossman AB, Burger J, Ellard S, Korbonits M (2011) AIP mutation in pituitary adenomas in the 18th century and today. N Engl J Med 364(1):43–50
Oriola J, Lucas T, Halperin I, Mora M, Perales MJ, Alvarez-Escola C, de Paz MN, Diaz SG, Salinas I, Julian MT, Olaizola I, Bernabeu I, Marazuela M, Puig-Domingo M (2013) Germline mutations of AIP gene in somatotropinomas resistant to somatostatin analogues. Eur J Endocrinol 168(1):9–13
Cazabat L, Guillaud-Bataille M, Bertherat J, Raffin-Sanson ML (2009) Mutations of the gene for the aryl hydrocarbon receptor-interacting protein in pituitary adenomas. Horm Res 71(3):132–141
Cazabat L, Bouligand J, Chanson P (2011) AIP mutation in pituitary adenomas. N Engl J Med 364(20):1973–1974
Schofl C, Honegger J, Droste M, Grussendorf M, Finke R, Plockinger U, Berg C, Willenberg HS, Lammert A, Klingmuller D, Jaursch-Hancke C, Tonjes A, Schneidewind S, Flitsch J, Bullmann C, Dimopoulou C, Stalla G, Mayr B, Hoeppner W, Schopohl J (2014) Frequency of AIP gene mutations in young patients with acromegaly: a registry-based study. J Clin Endocrinol Metab 99(12):E2789–E2793. doi:10.1210/jc.2014-2094
Preda V, Korbonits M, Cudlip S, Karavitaki N, Grossman AB (2014) Low rate of germline AIP mutations in patients with apparently sporadic pituitary adenomas before the age of 40: a single-centre adult cohort. Eur J Endocrinol 171(5):659–666
Stratakis CA, Tichomirowa MA, Boikos S, Azevedo MF, Lodish M, Martari M, Verma S, Daly AF, Raygada M, Keil MF, Papademetriou J, Drori-Herishanu L, Horvath A, Tsang KM, Nesterova M, Franklin S, Vanbellinghen JF, Bours V, Salvatori R, Beckers A (2010) The role of germline AIP, MEN1, PRKAR1A, CDKN1B and CDKN2C mutations in causing pituitary adenomas in a large cohort of children, adolescents, and patients with genetic syndromes. Clin Genet 78(5):457–463
Chamary JV, Hurst LD (2005) Evidence for selection on synonymous mutations affecting stability of mRNA secondary structure in mammals. Genome Biol 6(9):R75
Hunt RC, Simhadri VL, Iandoli M, Sauna ZE, Kimchi-Sarfaty C (2014) Exposing synonymous mutations. Trends Genet 30(7):308–321
Igreja S, Chahal HS, King P, Bolger GB, Srirangalingam U, Guasti L, Chapple JP, Trivellin G, Gueorguiev M, Guegan K, Stals K, Khoo B, Kumar AV, Ellard S, Grossman AB, Korbonits M (2010) Characterization of aryl hydrocarbon receptor interacting protein (AIP) mutations in familial isolated pituitary adenoma families. Hum Mutat 31(8):950–960
Akashi H (2001) Gene expression and molecular evolution. Curr Opin Genet Dev 11(6):660–666
Carlini DB, Chen Y, Stephan W (2001) The relationship between third-codon position nucleotide content, codon bias, mRNA secondary structure and gene expression in the drosophilid alcohol dehydrogenase genes Adh and Adhr. Genetics 159(2):623–633
Chen Y, Carlini DB, Baines JF, Parsch J, Braverman JM, Tanda S, Stephan W (1999) RNA secondary structure and compensatory evolution. Genes Genet Syst 74(6):271–286
Parsch J, Tanda S, Stephan W (1997) Site-directed mutations reveal long-range compensatory interactions in the Adh gene of Drosophila melanogaster. Proc Natl Acad Sci USA 94(3):928–933
Jin Y, Dietz HC, Montgomery RA, Bell WR, McIntosh I, Coller B, Bray PF (1996) Glanzmann thrombasthenia. Cooperation between sequence variants in cis during splice site selection. J Clin Invest 98(8):1745–1754
Liu H, Fu XA, Yu YX, Yu GQ, Yan XX, Liu HX, Tian HQ, Zhang FR (2011) Identification of two novel splice mutations of the ADAR1 gene in two Chinese families with dyschromatosis symmetrica hereditaria. Clin Exp Dermatol 36(7):797–799
Duan J, Antezana MA (2003) Mammalian mutation pressure, synonymous codon choice, and mRNA degradation. J Mol Evol 57(6):694–701
Acknowledgments
This Project was supported by Turkish Council of Scientific and Technological Research. (Project Number: 113S432)
Conflict of interest
The authors have nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Karaca, Z., Taheri, S., Tanriverdi, F. et al. Prevalence of AIP mutations in a series of Turkish acromegalic patients: are synonymous AIP mutations relevant?. Pituitary 18, 831–837 (2015). https://doi.org/10.1007/s11102-015-0659-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-015-0659-0