
Abstract
Background Acromegaly is a chronic disease impacting on morbidity and mortality. Increased mortality is reverted after the achievement of hormonal targets. The relative role of treatment options is still matter of debate. Methods A retrospective chart review was performed on all the acromegalic patients attending our center along the last 20 years. Results Data about 159 patients (83 F) were retrieved and analyzed: 18% had been lost to follow-up, while follow-up was >5 years in 79%. Growth hormone (GH) at diagnosis was 24 μg/L (median, range 3–239). Pituitary MRI showed a macro-, micro-adenoma or no lesion in 73.6, 22.9, and 3.5%, respectively. Hyperprolactinemia (hyperPRL) was present in 20.8%. Ninety-six and 29 patients had been treated by neurosurgery (NS) and irradiated (RT), respectively. Drugs had been employed in 149 patients (in 58 as the only treatment). At the last evaluation, 22% of patients were cured (hypopituitarism and GH deficiency in 6.3%), 37.1% were controlled by ongoing pharmacological treatment, 22.6% had discordant GH and Insulin-like growth factor I (IGF-I) values, and 18.2% had still active disease (median follow-up in this last group was 9 months). By evaluating the outcome with a multimodal approach, safe GH and normal IGF-I had been achieved in 78 and 63.5% of the whole series, 80.5 and 59.7% in patients submitted to NS (and adjuvantly treated with drugs), 95.8 and 91.7% in those submitted to NS + RT (and drugs as well), 70.2 and 55.2% in those treated only with drugs (increased to 82.2 and 60.9% if considering only patients treated with modern long-acting drugs). Hypopituitarism had occurred in 25, 66.6, and 13.8% in the three groups, respectively. At multivariate analysis, previous RT and NS were significant positive predictors of cure, whereas previous NS, follow-up, and year of diagnosis were significant positive predictors of control. Diabetes was a negative predictor both of cure and control. Sex, age, baseline GH levels, hyperPRL, tumor size, extrasellar extension, and invasiveness were not independent predictors of either cure or control. Conclusion This series seems to indicate that a multimodal approach can achieve control of disease in most patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acromegaly is an insidious chronic disease due to unrestrained hypersecretion of growth hormone (GH) and insulin-like growth factor I (IGF-I) [1]. It is associated with reduced expectancy and quality of life, symptoms and signs due to local expansion, and increased morbidity (arthropathy, cardiovascular and respiratory disease, metabolic derangement, likely increased oncological risk) [2, 3]. At present, there is consensus about the targets that establish the remission of the disease, i.e., GH levels below 1 μg/L after glucose load, and normal age-matched IGF-I levels [4]. In addition, epidemiological studies have shown that the increased mortality associated with active acromegaly is reverted to that of the normal population after decreasing GH to below 2–2.5 μg/L and restoring IGF-I levels to normal levels for sex- and age-matched controls, regardless of the treatments employed [5–10]. Accordingly, these targets are commonly used to assess good disease control.
At present three therapeutic options are available, neurosurgery (NS), radiotherapy (RT), and pharmacotherapy, whose relative role is still subject of active debate.
Aim of this study was to retrospectively review the outcome of different treatments in a large series of acromegalic patients attending a single center over a large time span.
Patients and methods
Methodology of data extraction and evaluation
A retrospective chart review was performed on all the acromegalic patients attending our center since 1986 till the end of 2006. Each patient diagnosed with acromegaly in our hospital was identified and its history was retrospectively retrieved from archive materials.
Demographic data about population of our district were collected at National Institute of Statistics (updated up to January 1st 2005).
Diagnosis had been performed on the basis of clinical picture, elevated GH levels not suppressible after an oral glucose load (OGTT, with cut-off evolving through the years according to literature data), and high IGF-I levels (that were expressed as mass units and age-adjusted since 1994). A few patients were included regardless of inadequate baseline assessment (missing baseline GH-values or neuroradiological evaluation in 18 and 14 patients, respectively), because long-term follow-up confirmed the diagnosis. In two cases acromegaly was diagnosed after NS.
Diagnostic delay had been estimated, whenever possible, as the years elapsed between the onset of typical symptoms and diagnosis of the disease, or after the observation of serial pictures of the patient.
Patients were followed-up as in- or outpatients with serial monitoring of clinics, hormonal values (at least yearly) and imaging (at 2–3-year intervals). Patients were regarded as lost to follow-up if more than 2 years had elapsed since the last available control.
Hyperprolactinemia (hyperPRL) was arbitrarily defined as the occurrence of serum prolactin (PRL) levels higher than 30 μg/L regardless of gender.
Imaging had been performed by magnetic resonance equipment (MR) since available, except when absolute contraindications occurred. Due to different equipments and operators involved throughout the years, as well as poor availability of original images for revision, only data at diagnosis were considered, whereas possible drug- or radiation-induced tumor shrinkage could not be evaluated. If a discrete lesion had been identified within the pituitary, it was arbitrarily classified as micro-adenoma or macro-adenoma, according to size less or greater than 10 mm, respectively, otherwise imaging was classified as negative. If an adenoma had been shown, it was arbitrarily defined as intrasellar, extrasellar or invasive, if fully included within the pituitary fossa, expanding outside it regardless of the direction, or invading cavernous or sphenoid sinus, respectively.
Visual disturbance was considered if objectively evaluated by visual perimetry (by techniques evolving throughout the years) or evoked potentials.
Arterial hypertension was defined as the use of anti-hypertensive drugs or, in the last 3 years, when pathological results were obtained by the routinely performed ambulatory blood pressure monitoring. Cardiopathy was defined as the occurrence of any lesion (hypertrophy, or dyskinesia, or valve alteration) at echocardiography that was routinely performed at 1–2-year-intervals in all patients, or when any documentation of hospital admission for cardiac failure, or coronary heart disease, or arrhythmia was retrieved. Diabetes was defined as any treatment with antidiabetic drugs or as the occurrence at least twice of fasting glucose levels higher than 140 mg/dL. Impaired glucose tolerance was defined as the occurrence of glucose levels ranging 115–140 mg/dL when fasting and/or 140–200 mg/dL at 120 min after OGTT. Dyslipidemias were defined as the occurrence at least twice of cholesterol (total or subfractions) or triglycerides levels out of reference limits. Neuropathy was defined when any documentation of previous surgery for carpal tunnel syndrome was retrieved or as the occurrence of alterations at electromyography. Goiter was defined as thyroid enlargement or multiple nodules at ultrasound examination routinely performed in all patients. Neoplasm was defined as any occurrence (previous or ongoing) of tumors in whatever part of the body. Sleepiness and snoring had not been routinely evaluated until the last 3 years and thus were not considered.
The outcome of NS was evaluated after at least 3, and 6–12 months as for hormonal values and visual disturbances, and imaging, respectively. Presurgical treatment was defined as the administration of any drug aimed at suppressing GH hypersecretion for any time before NS.
The outcome of RT was considered if patients were off GH-suppressive treatment for an appropriate interval, i.e., 1, 4, and 12 weeks for short-acting somatostatin analogs (SA), dopamine agonists (DA) and Pegvisomant, and long-acting SA, respectively.
Before starting pharmacological treatment, many patients had been submitted as inpatients to the acute administration of bromocriptine (2.5 mg orally) and/or octreotide (50 μg subcutaneously) to select the drug to be employed thereafter. During both tests blood samples for GH assay had been collected at h 7.00 and then hourly, up to h 20.00, and the test drug had been administered at h 8.00. In each case the lowest GH-value obtained after the drug administration had been identified and expressed as percent change versus baseline value. Patients had been then administered SA or DA if GH suppression had been more pronounced or prolonged after octreotide or bromocriptine, respectively, or both drugs if the response had been poor.
Data obtained in each patient during pharmacological treatment, were divided, when appropriate, between those achieved during primary pharmacologic treatments and those obtained as adjuvant after previous ablative treatments (NS and/or RT). The evaluation of results was considered when samples had been collected just before the next injection of long-acting drugs. Only the most recent data obtained while on each treatment were considered for the evaluation of drug efficacy, without any consideration of the eventual progression of results during follow-up. Compliance to pharmacological treatments could not be objectively evaluated.
The most recent data obtained in each patient were considered for cure/control. Patients were judged as cured if IGF-I levels were within normal age-adjusted range and GH levels were suppressed below 1 μg/L after OGTT, without any GH-suppressing drug. Patients were considered controlled if IGF-I levels were within normal age-adjusted range and GH levels (as the mean of at least 5 hourly samples after an overnight fast and rest, while supine and awake, with an indwelling needle inserted in an antecubital vein and kept patent by slow infusion of saline) were below 2.5 μg/L while on treatment with drugs aimed at suppressing GH/IGF-I hypersecretion.
Hypopituitarism was defined as the need for substitutive adrenal or thyroid treatment, evaluated on a clinical basis, as well as after the finding of morning cortisol and free-thyroxine (assayed by validated standard methods, commonly employed in our hospital, but changed throughout the years) below reference limits. For the evaluation of adrenal function, the low-dose adrenocorticotropin (ACTH) test (1 μg iv) was employed since 2 years in patients whose morning cortisol was between 3 and 12 μg/dL (setting at 18 μg/dL the cut-off for normal cortisol response) [11]. During the preceding years ovine corticotropin-releasing hormone test (100 μg iv) had been employed (setting at 15 μg/dL the cut-off for normal cortisol response) [12] in the context of the combined administration of multiple hypothalamic releasing hormones, whose results are not shown here. Males were classified as hypogonadal if testosterone levels were below reference limits at least twice. Females were considered eugonadal if normally cycling. Gonadotropins were not routinely assayed in post-menopausal women. Worsening hypopituitarism was defined as the need for a new replacement therapy, without any consideration to dosage or schedule changes.
Growth hormone deficiency was diagnosed, after full and stable replacement of other pituitary deficiencies (except estrogens in post-menopausal women), if low GH levels did not increase above 9 μg/L after the administration of GHRH + Arginine (100 μg + 0.5 g/kg iv) [13].
Laboratory
Growth hormone had been assayed by different methods throughout the years. In the last 2 years GH had been assayed by chemiluminescence (DPC Immulite 2000, Los Angeles, CA, USA), with standard calibrated against 1st IRP 80/505 (1 ng = 2.6 μIU), and a detection limit of 0.01 μg/L.
Insulin-like growth factor I had been assayed by different methods throughout the years always involving a preliminary acid-ethanol extraction. In the last year IGF-I had been assayed by chemiluminescence (DPC Immulite 2000), with standard calibrated against WHO NIBSC 1st IRR 87/518, and a detection limit of 20 μg/L. Normal values (5th–95th percentiles) provided by the manufacturer for IGF-I are 116–358, 117–329, 115–307, 109–284, 101–267, 94–252, 87–238, 81–225, 75–212, 69–200, 64–188, 59–177, 55–166 μg/L in patients 21–25, 26–30, 31–35, 36–40, 41–45, 46–50, 51–55, 56–60, 61–65, 66–70, 71–75, 76–80, 81–85 years old, respectively.
Statistics
Values are expressed as mean and standard deviation, or proportions, unless otherwise stated.
Continuous data were analyzed by t-test for paired or unpaired data, and Pearson correlation test.
Categorical data were analyzed by odds ratio, Chi-square test or Fisher exact test, as appropriate.
Multivariate analysis was performed by logistic regression, setting as dependent variable the achievement of cure or control and as independent: sex, age at diagnosis, year of diagnosis, hyperPRL, basal GH levels, neuroradiological features (micro, macro or negative), extrasellar extension of the adenoma, invasiveness, diabetes mellitus, NS, RT, follow-up. Stepwise forward analysis was employed to establish rank of predictors.
All statistical tests (performed by Statwiew for Windows 4.53, Abacus Concept Inc., Berkeley, CA, USA) were two-tailed and values of p < 0.05 were considered significant.
Estimated post-test Bayesian probability after acute tests was calculated as:
where postodd was estimated post-test odd.
Postodd was calculated as:
where LR was likelihood ratio and preodd estimated pre-test odd.
LR was calculated as:
where TP were true positives (responders to both the test and the treatment), FN false negatives (responders to treatment but not to the test), FP false positives (responders to the test but not to treatment), and TN true negatives (not responders to both).
Pre-odd was calculated as the percentage of estimated prevalence of response to chronic administration of the drug.
Assuming 20% as the prevalence of positive response to chronic treatment with DA, an arbitrary cut-off of 50% decrease during acute bromocriptine test was compared with an arbitrary chosen 50% decrease of GH values during chronic DA treatment versus baseline. Assuming 50% as the prevalence of positive response to chronic treatment with SA, an arbitrary cut-off of 75% decrease during acute octreotide test versus baseline was compared with the achievement of safe GH-values during chronic SA treatment. Only acute tests performed at baseline (without considering those performed after NS) and only results of primary treatment were included in this calculation, irrespective of the duration of treatments.
Results
Demographic and clinical data
Data about 159 patients were retrieved, 83 females and 76 males. Age at diagnosis was 16–77 years (median 44); males were younger than females (data not shown).
Diagnostic delay, estimated in 54 patients (34%), was 1–34 years (median 4), without any difference between genders, or between patients diagnosed in recent years as compared to older diagnosis (data not shown).
Patients had been followed-up for 12 ± 7.9 years (median 11, range 0.5–35) for a total of 1,794 patient-years.
Twenty-nine patients (18%) had been lost to follow-up, eight (5%) were dead and the others (77%) were still on active follow-up. The cause of death was known in five patients: cardiac failure in one (aged 72), neoplastic disease in two (at 62 and 79 years), advanced age in two (at 83 and 90 years). A 37 year-old patient died for unknown reasons 1 week after NS (post-mortem examination had not disclosed any apparent cause).
Patients attending our center come from different regions of our country. After discarding those coming from other districts, as well as the deceased subjects and those lost to follow-up, there are 82 patients living in our district and actively followed-up. Since whole population is 1,022,428 inhabitants, the prevalence of the disease is 80.2 per million.
GH at diagnosis was 24 μg/L (median, range 3–239) without any gender difference, but with higher values in younger patients (data not shown).
Pituitary MRI showed a macro-adenoma in 73.6%, a micro-adenoma in 22.9%, and was negative in 3.5%. In all these patients an extensive work-up had been performed, including Octreoscan but not GHRH assay, without finding the origin of GH/IGF-I hypersecretion (notwithstanding a follow-up lasting 6–30 years). Tumor had extrasellar expansion in 51% and was regarded as invasive in 31.5%.
Visual disturbances were present at diagnosis in 13.2% of patients.
Hyperprolactinemia occurred in 20.8% of patients, without any gender difference.
Hypopituitarism was present at diagnosis in 18.2% of patients, involving one or more axes (data not shown).
Hypertension, cardiopathy, glucose metabolism abnormalities, dyslipidemias, neuropathy, goiter, and tumors were present in 42, 30, 57, 16, 37, 21 and 11% of patients, respectively. Among the 18 patients affected by tumors, neoplasm involved colon, breast, skin, kidney, thyroid, lung, prostate, bladder, and larynx in 6 (four carcinomas and two polyps), 3, 2, 2, 2, 2, 1, 1, 1, respectively. In one patient three different neoplasms were subsequently diagnosed (kidney, colon, and lung).
Results of neurosurgery
Ninety-six patients (60.4% of the whole series) had undergone NS for a total of 106 operations (eight patients had been operated on twice and one three times). NS had been performed via the transsphenoidal or trans-cranial approach in 96 and 8 cases, respectively (in two cases this information was not available). The endoscopic technique for transsphenoidal surgery had been employed only once. The neurosurgeon could not be identified in 29 interventions, whereas operation had been performed by a single operator in our two main reference centers in 16 and 49 cases, respectively, and in nine different centers of our country in the other 15 cases.
The success rate in the whole series was 33.3% as for disappearance of visual disturbances, and 18.9% as for the achievement of target hormonal levels pointing to cure as defined in the methods section. If only first interventions via transsphenoidal approach were considered (n = 89), success rate was 21.3%. Table 1 shows the impact of different parameters on surgical success rate.
Cure was never achieved by NS performed via the transcranial approach, whereas it was achieved in only one of ten reoperations.
Surgical success rate was not different in past versus more recent years (data not shown).
Surgical cure had been achieved in 29% versus 9% of patients operated on with or without medical pretreatment, respectively (p = 0.03), but at multivariate analysis basal GH level was the best (negative) predictor of surgical success rate among all the above mentioned.
Among those treated with GH-suppressive treatment both before and after non-curative NS, we identified a small subset of 13 patients treated with the same drug and the same follow-up. In these patients the second cycle of pharmacologic treatment obtained safe GH and normal IGF-I in 69 and 54%, respectively (vs. 7% and nil after the first cycle).
Post-operative complications occurred in 25.5% of interventions: hypopituitarism in 18%, water metabolism disorders in 6.6%, cerebrospinal fluid leak in 3.8%, bleeding requiring reoperation in one patient, and unexplained death on day 7 in one patient.
After a confirmed cure, relapse occurred in three patients, after 6, 10, 10 years.
Results of radiotherapy
Among the 29 patients treated by RT (18.2% of the whole series, administered as primary treatment in five patients), 22 had been submitted to conventional three-field fractionated RT (46 Gy median, range 35–50), four to gamma-knife radio-surgery (GK)(25 Gy margin dose), and three to interstitial radiotherapy by implantation of radioactive seeds loaded with 90Y.
The cumulative follow-up was 408 patient-years, but the mean follow-up of the three techniques was very different, being 15, 3, and 29 years, respectively.
Safe GH had been achieved in 50, 50, and 100%, respectively, of the patients irradiated (RT) by the different techniques, whereas the respective figures for IGF-I normalization were 50, 33, and 66%.
Safe GH levels were achieved in 60 and 56.5% of patients RT as primary or adjuvant treatment, respectively (p = NS), whereas the respective figures for IGF-I normalization were 40 and 56.5% (p = NS). Time to safe GH was 27 years (median, range 11–28) and 3.5 years (0–27), respectively.
Hypopituitarism (occurrence or worsening) had developed in 27.6% of patients (up to GH deficiency in 20.7%).
The information about withdrawal of GH-suppressive treatment during the period of irradiation was available only for patients submitted to GK, in whom it was routinely performed.
Results of pharmacological treatment
One hundred forty-nine patients (93.7% of the whole series) had been treated with drugs aimed at suppressing GH/IGF-I hypersecretion for a cumulative follow-up of 1,084 patient-years. Pharmacotherapy had been the only treatment in 58 patients (36.5% of the whole series) with a cumulative follow-up of 596 patient-years.
Dopamine agonist drugs
During 32 different and subsequent cycles DA had been employed in 28 patients (11 females), as primary or adjuvant treatment in 17 and 9 patients, respectively (in two both as primary and adjuvant treatment), for a cumulative follow-up of 91.8 patient-years. Employed molecules had been bromocriptine, both in the oral (up to 30 mg/day for 3–360 months) and long-acting injectable (up to 100 mg/month for 1–60 months) formulations, quinagolide (at 0.15 mg/day for 1 month), and cabergoline (at 0.5 mg/week–0.25 mg/day for 2–48 months) in 15, 11, 1, and 4 patients, respectively.
Even though DA had obtained a significant decrease in GH and IGF-I levels (from 10.9 μg/L median, 3–178 range, to 6.2 (0.5–52) μg/L, p = 0.019, and from 673 ± 219 to 514 ± 248 μg/L, p = 0.032, respectively), safe GH had been achieved only in 9/32 cycles (3/19 as primary treatment) and normal IGF-I in only one adjuvant treatment. Neither hyperPRL nor the response to the acute administration of bromocriptine were predictive of the response to chronic DA administration (data not shown).
Somatostatin analogs
During 234 different and subsequent cycles SA had been employed in 128 patients (68 females), as primary or adjuvant treatment in 71 and 37 patients, respectively (in 20 both as primary and adjuvant treatment), for a cumulative follow-up of 750.3 patient-years. Employed molecules were octreotide, both in the short acting sc (in 72 patients, 50 as primary treatment and 28 as adjuvant treatment, up to 500 μg tid for 1–146 months) and in the long-acting im (in 72 patients, 48 as primary treatment and 30 as adjuvant treatment, up to 30 mg/28 day for 1–162 months) formulations, and lanreotide SR, in the different formulations of 30 mg (in 38 patients, 25 as primary treatment and 13 as adjuvant treatment, injected q 7–21 days for 3–60 months), 60 mg (in 22 patients, 14 as primary treatment and ten as adjuvant treatment, injected q 28 days for 1–84 months), autogel (in 15 patients, 9 as primary treatment and 7 as adjuvant treatment, 90–120 mg injected q 28–56 days for 3–48 months). During SA treatment GH declined from 7.8 (2–239) to 2.1 (0.1–51) μg/L (p < 0.0001), reaching safe values in 52%, and IGF-I from 592 ± 264 to 351 ± 197 μg/L (p < 0.0001), reaching normal values in 35.5%. Table 2 shows results obtained by SA. The horizontal reading of table (by lines) shows that primary and adjuvant treatment achieved the same results, on considering both the whole group and each single molecule. On the other hand, the vertical reading (by columns) shows that long-acting drugs obtained better results than sc octreotide (p = 0.0001, 0.0007, and 0.0004 for safe GH, normal IGF-I and both results, respectively).
The acute octreotide test was not predictive of response to chronic treatment: positive predictive value, accuracy and estimated post-test probability of a 75% decrease in GH-value versus baseline after the acute octreotide administration were 50, 55, and 38.4%, respectively, in the whole SA series. Results were not improved if only octreotide treatment was considered (data not shown).
Combined DA and SA
During 118 different and subsequent cycles combined DA and SA had been employed in 61 patients (29 females), as primary or adjuvant treatment in 25 and 14 patients, respectively (in 22 both as primary and adjuvant treatment) for a cumulative follow-up of 240 patient-years. Table 3 shows the efficacy of the different combinations.
Combined treatment obtained better results than SA alone in 12 of 39 patients in whom a meaningful comparison could be performed (30.8%), whereas the opposite was true in 6 and no difference was observed in the remaining 21.
Pegvisomant
Pegvisomant had been used in three patients for 4, 6, 15 months at 10 mg/day, obtaining a striking suppression of IGF-I levels (47, 54, 67% versus baseline), but achieving normal levels in one patient only.
Results of multimodal therapy
In summary, 72 (45.3%), 24 (15.1%), 5 (3.1%), and 58 (36.5%) patients had been treated by NS, NS + RT, RT, and drugs alone, respectively. Drugs had been employed as adjuvant treatment in patients submitted to NS and/or RT, if needed. At the last evaluation (Fig. 1), 35 patients were cured (22%) (hypopituitarism and GH deficiency were present in 10, 6.3%), 59 (37.1%) were controlled by ongoing pharmacological treatment, 36 (22.6%) had discordant GH and IGF-I-values, and 29 (18.2%) had still active disease (median follow-up in this group was 9 months).

Proportion of patients of the series (n = 159) achieving hormonal targets at the last evaluation
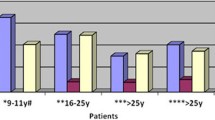
By evaluating the outcome with a multimodal approach (Fig. 2), we found that safe GH and normal IGF-I had been achieved in 124 and 101 patients of the whole series (78 and 63.5%), in 58 and 43 patients submitted to NS (80.5 and 59.7%), in 23 and 22 of those submitted to NS + RT (95.8 and 91.7%), in 41 and 32 of those treated only with drugs (70.7 and 55.2%, increased to 82.6 and 60.9% if considering only patients treated with modern long-acting drugs) (drugs as adjuvant treatment if needed after NS and/or RT). Hypopituitarism had occurred in 25, 66.6, and 13.8% in the three groups, respectively.

Safe GH (empty bars), normal IGF-I (full bars) and both targets (gray bars) obtained by different treatment modalities (expressed as percentage of the total population in each group). Drugs had been employed in all groups, but in groups II, III, and IV they had been used as adjuvant treatment after NS and/or RT. In group VI only results of modern long-acting drugs were considered
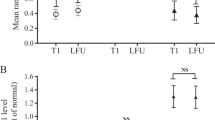
At multivariate analysis (Fig. 3), previous RT and NS were significant positive predictors of cure (p = 0.0013 and 0.0041, respectively) (Fig. 3a), whereas follow-up, year of diagnosis and previous NS were significant positive predictors of control (p = 0.0024, 0.0268, and 0.0297, respectively) (Fig. 3b). Diabetes was a negative predictor both of cure and control (p = 0.0084 and 0.01, respectively). Sex, age, baseline GH levels, hyperPRL, tumor size, extrasellar extension, and invasiveness were not independent predictors either of cure or control (all p > 0.05).

Multivariate analysis as for cure (on the left panel) or control (on the right panel) of the disease, defined as the concomitant achievement of safe GH and normal IGF-I levels. Each of the parameters listed on the y-axis is depicted by a square (pointing to the mean) and a horizontal bar (showing 95% confidence intervals). Significant independent predictors (positive or negative if on the right or on the left, respectively, of the vertical neutral line in each panel) are shown by an asterisk
Discussion
We present here the outcome of different treatments in a large series of acromegalic patients followed-up for more than 20 years in the same center. This setting gave us the opportunity to evaluate results obtained with constantly shared criteria, even though updated according to literature progress.
A few epidemiological observations deserve to be underlined. Even though it must be stressed that diagnostic delay is a rough estimation performed only in a few patients, the lack of improvement throughout the years suggests that acromegaly is still an underestimated disease. The loss to follow-up is remarkably low in this series, pointing to trust that patients give to health team, when it satisfies their expectations in coping with such a multifaceted disease. Also deaths were few and occurred at advanced age, in contrast to what reported in old epidemiologic series [2]. It seems thus that the advancement of knowledge and care for this disease has a major impact at least on survival.
Prevalence of disease is reported to be near 60 per million [1]. In this series the calculated prevalence was 80.2 per million. It must be stressed that this figure might be even underestimated, because it is likely that at least a few patients missed our survey or were diagnosed and followed-up in the nearby town of Milan. Our findings thus point to a higher prevalence of acromegaly, as recently suggested [14].
As for morbidity, hypertension, cardiopathy and glucose metabolism alterations are largely prevalent and are well-known to have a major impact on complications and survival. Owing to criteria used for diagnosis, may be that prevalence of hypertension and diabetes in this series was underestimated. Sleep apnea was not actively pursued by us until recently, and thus was not diagnosed. On the contrary, neuropathy was diagnosed in a large portion in this series, mainly owing to our politics of extensive searching for it. Neoplasms are still under discussion as complications of the disease [3]. Most patients reported in old studies died of cardiovascular diseases. Nowadays, with the large availability of effective therapeutic tools, many patients survive long-term with well-controlled GH hypersecretion, leaving thus room to the development of neoplastic diseases, typically affecting older populations. Organ distribution of neoplasms seems different in this series as compared to that observed in general population (as suggested by low rank of lung and prostate tumors, contrary to what is commonly reported in general population), calling for a specific role played by GH/IGF-I hypersecretion [15].
As for therapeutic options, according to existing guidelines, NS by transsphenoidal approach is usually considered the first choice treatment [16]. However, neurosurgical outcome depends mainly on three variables: the size and invasiveness of the adenoma, GH levels, and the expertise of neurosurgeon [17]. It is well-known that success rate is higher than 75% in micro-adenomas, but drops to near 50% in macro-adenomas (that are the vast majority of acromegalic patients), and below 30% in invasive adenomas [18]. The same authors showed that success rate was higher than 85% in patients whose GH levels were below 10 μg/L, but fell to 67 and 51% when GH was 10–25 μg/L or higher than 25 μg/L, respectively [18]. Surgical skill is the last but not least factor impacting on surgical success rate, as shown by the increase from 37 to 81% of success rate when operations were performed by the same skilled neurosurgeon as compared to results obtained by different operators [19]. Surgical results in our series were very poor, with a total success rate below 20%. Our results reproduced the same rank according to adenoma size and basal GH levels as those reported in main surgical series, showing progressively worse results in micro-, macro-, and invasive adenomas, as well as in patients with increasing GH levels. Anyway, our success rate was worse in each category, strengthening the belief that reported results always reflect the best, whereas results in “normal” and peripheral conditions rank worse. Moreover, a learning curve does not seem to be involved, because more recent results were not different from the oldest ones, as already shown by the recent German series [17] reproducing the same results as the oldest one [20]. In contrast with recently reported data [21], surgical results in our series were better in patients that had been pharmacologically treated before surgery versus those directly operated on. Since this was a retrospective study, we cannot rule out that the latters had worse conditions prompting urgent intervention and, furthermore, at multivariate analysis pretreatment was not an independent predictor of surgical success. In a small sample of our series we confirmed data reported by Colao et al. [22], about better results obtained by pharmacological treatment after surgical debulking without cure. As a further caveat for surgery, in this series we observed complications, mainly hypopituitarism, in a quarter of patients, but also an unexplained post-operative death and three long-term relapses.
A second therapeutic option is fractionated RT, burdened by variable efficacy and severe delay, high prevalence of hypopituitarism [23], increased cerebro-vascular mortality [10, 24, 25] and the occurrence of second neoplasm in central nervous system in previously RT patients [26]. Even more recent and refined techniques, allowing the delivery of a highly collimated dose in a single session, do not seem to obtain better results after 4 years of follow-up [27, 28], and their long-term safety is still unknown. In this series cure was obtained in nearly half of RT patients (differences among techniques are to be accounted for to the different lengths of follow-up), with the burden of hypopituitarism in all, including GH deficiency in many. As for safety, no secondary tumor was disclosed up to now, whereas cerebro-vascular disease (stroke or cognitive dysfunction) cannot be attributed to previous RT in the individual patients, owing to their large prevalence in elderly patients.
The third therapeutic option for acromegaly, pharmacotherapy, was employed at first to reduce GH/IGF-I hypersecretion in patients unsuitable or unwilling to undergo NS, or after its failure. Only recently, thanks to the development of effective and long-lasting drugs, it has been suggested as primary treatment at least in selected cases.
DA are able to control hormonal hypersecretion only in a minority of patients, with mild GH hypersecretion and associated hyperPRL [29–31], as confirmed in this series.
SA represent now the milestone in the medical treatment of acromegaly [32]. When used as long-acting formulations, to be injected every 4 weeks, SA obtain control both of GH/IGF-I hypersecretion in 50–70% of patients, and tumor growth in all, shrink pituitary tumors by 20–70% of baseline in 50–80% of patients, abate symptoms, stop or revert progression of comorbidities in many [3, 33]. SA were largely employed in this series, obtaining safe GH and normal IGF-I in 52 and 35.5%, respectively, which even increased to 60.9 and 42.9%, respectively, when using long-acting analogs. These results may seem worse, at least as for IGF-I levels, than those recently reported [34, 35], but, on the one hand recently introduced IGF-I reference values in our laboratory are much more restrictive than previously reported, and, on the other, it is well-known that compliance is optimal only during a controlled study. As already reported [34–37], results of SA as primary or adjuvant treatment were not different. In contrast to what recently reported [38], but in agreement with others [39], acute octreotide administration was useless in predicting response to long-term treatment. Owing to the large prevalence of responsiveness to SA in acromegalic population and the very little difference in post-test probability as compared to pre-test one, it seems thus better to evaluate results of a short (3–6 months) treatment, that were convincingly reported to predict reliably the results of chronic treatment [34, 35].
Combined treatment with DA and SA obtained targets in one-fifth of patients, with the proportion increasing to one-third when only results of modern long-acting drugs of the two classes were considered, in agreement with previously reported results [40].
Pegvisomant, the first drug acting as an antagonist at the level of GH receptor, obtains IGF-I normalization in over 90% of treated patients [41, 42]. However, many drawbacks dampen still its generalization, such as the lack of control on tumor volume, concern about liver toxicity, the need for daily injections, and high cost. In this series it was employed only marginally and its results are thus not fully assessable.
At first sight NS, RT, and drugs obtained targets in 20, 50, and 50%, respectively. But if results of multimodal therapy were considered, as reported in Figs. 1 and 2, far better results were obtained, so that only 18% of patients had still active full-blown disease (most after a short follow-up). Since different GH assays with better and better performance were used as they became available, a word of caution is mandatory in the interpretation of hormonal results analyzed retrospectively throughout such a large span of years. Anyway, the portion of patients lost to follow-up (or dead not in recent years) is really little, so that we believe this caveat does not really affect our results.
No gender difference was observed in results obtained in our series, in apparent contrast with data previously reported [43–46], but in this series we focused only on the achievement of targets without considering subtle differences among subgroups whose meaning is only pathophysiological.
In conclusion, it seems that an individually tailored approach fully evaluating the disease, its extension and complications in each patient can optimize results and control complications.
Abbreviations
- ACTH:
-
Adrenocorticotropin
- DA:
-
Dopamine agonist drugs
- FN:
-
False negatives
- FP:
-
False positives
- GH:
-
Growth hormone
- GHRH:
-
GH-releasing hormone
- GK:
-
Gamma-knife radio-surgery
- IGF-I:
-
Insulin-like growth factor I
- LAR:
-
Long-acting repeatable
- LR:
-
Likelihood ratio
- MRI:
-
Magnetic resonance imaging
- NS:
-
Neurosurgery
- OGTT:
-
Oral glucose tolerance test
- Postodd:
-
Estimated post-test odd
- Preodd:
-
Estimated pre-test odd
- PRL:
-
Prolactin
- RT:
-
Radiotherapy
- SA:
-
Somatostatin analogs
- TN:
-
True negatives
- TP:
-
True positives
References
Melmed S (2006) Acromegaly. N Engl J Med 355:2558–2573
Wright AD, Hill DM, Lowy C, Fraser TR (1970) Mortality in acromegaly. Q J Med 39:1–16
Colao A, Ferone D, Marzullo P, Lombardi G (2004) Systemic complications of acromegaly: epidemiology, pathogenesis and management. Endocr Rev 25:102–152
Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman L, Ho K, Veldhuis J, Wass J, Von Werder K, Melmed S (2000) Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab 85:526–529
Bates AS, Van’t Hoff W, Jones JM, Clayton RN (1993) An audit of outcome of treatment in acromegaly. Q J Med 86:293–299
Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ, Ibbertson HK (1994) Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol (Oxf) 41:95–102
Swearingen B, Barker FG, Katznelson L, Biller BMK, Grinspoon S, Klibanski A, Moayeri N, Black PM, Zervas NT (1998) Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab 83:3419–3426
Biermasz NR, Dekker FW, Pereira AM, van Thiel SW, Schutte PJ, van Dulken H, Romijn JA, Roelfsema F (2004) Determinants of survival in treated acromegaly in a single center: predictive value of serial insulin-like growth factor I measurements. J Clin Endocrinol Metab 89:2789–2796
Holdaway IM, Rajasoorya CR, Gamble GD (2004) Factors influencing mortality in acromegaly. J Clin Endocrinol Metab 89:667–674
Kauppinen-Mäkelin R, Sane T, Reunanen A, Valimaki MJ, Niskanen L, Markkanen H, Loyttyniemi E, Ebeling T, Jaatinen P, Laine H, Nuutila P, Salmela P, Salmi J, Stenman UH, Viikari J, Voutilainen E (2005) A Nationwide Survey of Mortality in Acromegaly. J Clin Endocrinol Metab 90:4081–4086
Dorin RI, Qualls CR, Crapo LM (2003) Diagnosis of adrenal insufficiency. Ann Int Med 139:194–204
Lopez-Schmidt I, Lahner H, Mann K, Petersenn S (2003) Diagnosis of adrenal insufficiency: Evaluation of the corticotropin-releasing hormone test and basal serum cortisol in comparison to the insulin tolerance test in patients with hypothalamic-pituitary-adrenal disease. J Clin Endocrinol Metab 88:4193–4198
Ghigo E, Aimaretti G, Arvat E, Camanni F (2001) Growth hormone-releasing hormone combined with arginine or growth hormone secretagogues for the diagnosis of growth hormone deficiency in adults. Endocrine 15:29–38
Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A (2006) High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab 91:4769–4775
Samani AA, Yakar S, LeRoith D, Brodt P (2007) The role of the IGF system in cancer growth and metastasis: overview and recent insights. Endocr Rev 28:20–47
American Association of Clinical Endocrinologists Acromegaly Guidelines Task Force (2004) Medical guidelines for clinical practice for the diagnosis and treatment of acromegaly. Endocr Pract 10:213–225
Nomikos P, Buchfelder M, Fahlbusch R (2005) The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol 152:379–387
De P, Rees DA, Davies N et al (2003) Transsphenoidal surgery for acromegaly in Wales: results based on stringent criteria of remission. J Clin Endocrinol Metab 88:3567–3572
Yamada S, Aiba T, Takada K, Ozawa Y, Shimizu T, Sawano S, Shishiba Y, Sano T (1996) Retrospective analysis of long-term surgical results in acromegaly: preoperative and postoperative factors predicting outcome. Clin Endocrinol (Oxf) 45:291–298
Fahlbusch R, Honegger J, Buchfelder M (1992) Surgical management of acromegaly. Endocrinol Metab Clin North Am 21:669–692
Losa M, Mortini P, Urbaz L, Ribotto P, Castrignano T, Giovanelli M (2006) Presurgical treatment with somatostatin analogs in patients with acromegaly: effects on the remission and complication rates. J Neurosurg 104:899–906
Colao AM, Attanasio R, Pivonello R, Cappabianca P, Cavallo LM, Lasio G, Lodrini A, Lombardi G, Cozzi R (2006) Partial surgical removal of growth hormone-secreting pituitary tumors enhances the response to somatostatin analogs in acromegaly. J Clin Endocrinol Metab 91:85–92
Biermasz NR, Pereira AM, Neelis KJ, Roelfsema F, Romijn JA (2006) Role of radiotherapy in the management of acromegaly. Exp Rev Endocrinol Metab 1:449–460
Mestron A, Webb SM, Astorga R, Benito P, Catala M, Gaztambide S, Gomez JM, Halperin I, Lucas-Morante T, Moreno B, Obiols G, de Pablos P, Paramo C, Pico A, Torres E, Varela C, Vazquez JA, Zamora J, Albareda M, Gilabert M (2004) Epidemiology, clinical characteristics, outcome, morbidity and mortality in acromegaly based on the Spanish Acromegaly Registry. Eur J Endocrinol 151:439–446
Ayuk J, Clayton RN, Holder G, Sheppard MC, Stewart PM, Bates AS (2004) Growth hormone and pituitary radiotherapy, but not serum insulin-like growth factor-I concentrations, predict excess mortality in patients with acromegaly. J Clin Endocrinol Metab 89:1613–1617
Minniti G, Traish D, Ashley S, Gonsalves A, Brada M (2005) Risk of second brain tumor after conservative surgery and radiotherapy for pituitary adenoma: update after an additional 10 years. J Clin Endocrinol Metab 90:800–804
Attanasio R, Epaminonda P, Motti, Giugni E, Ventrella L, Cozzi R, Farabola M, Loli P, Beck-Peccoz P, Arosio M (2003) Gamma-knife radiosurgery in acromegaly: a 4-year-follow-up study. J Clin Endocrinol Metab 88:3105–3131
Castinetti F, Taieb D, Kuhn JM, Chanson P, Tamura M, Jaquet P, Conte-Devolx B, Regis J, Dufour H, Brue T (2005) Outcome of gamma knife radiosurgery in 82 patients with acromegaly: correlation with initial hypersecretion. J Clin Endocrinol Metab 90:4483–4488
Jaffe CA, Barkan AL (1992) Treatment of acromegaly with dopamine agonists. Endocrinol Metab Clin North Am 21:713–735
Abs R, Verhelst J, Maiter D, Van Acker K, Nobels F, Coolens JL, Mahler C, Beckers A (1998) Cabergoline in the treatment of acromegaly: a study in 64 patients. J Clin Endocrinol Metab 83:374–378
Cozzi R, Attanasio R, Barausse M, Dallabonzana D, Orlandi P, DaRe N, Branca V, Oppizzi G, Gelli D (1998) Cabergoline treatment in acromegaly: a renewed role for dopamine agonist? Eur J Endocrinol 139:516–521
Newman CB (1999) Medical therapy for acromegaly. Endocrinol Metab Clin North Am 28:171–190
Freda PU, Katznelson L, van der Lely AJ, Reyes CM, Zhao S, Rabinowitz D (2005) Long-acting somatostatin analog therapy of acromegaly: a meta-analysis. J Clin Endocrinol Metab 90:4465–4473
Cozzi R, Attanasio R, Montini M, Pagani G, Lasio G, Lodrini S, Barausse M, Albizzi M, Dallabonzana D, Pedroncelli AM (2003) Four-year treatment with octreotide-long-acting repeatable in 110 acromegalic patients: predictive value of short-term results? J Clin Endocrinol Metab 88:3090–3098
Cozzi R, Montini M, Attanasio R, Albizzi M, Lasio G, Lodrini A, Doneda P, Cortesi L, Pagani G (2006) Primary treatment of acromegaly with octreotide LAR: a long-term (up to 9 years) prospective study on its efficacy in the control of disease activity and on tumor shrinkage. J Clin Endocrinol Metab 91:1397–1403
Newman CB, Melmed S, George A, Torigian D, Duhaney M, Snyder P, Young W, Klibanski A, Molitch ME, Gagel R, Sheeler L, Cook D, Malarkey W, Jackson I, Vance ML, Barkan A, Frohman L, Kleinberg DL (1998) Octreotide as primary treatment for acromegaly. J Clin Endocrinol Metab 83:3034–3040
Attanasio R, Baldelli R, Pivonello R, Grottoli S, Bocca L, Gasco V, Giusti M, Tamburrano G, Colao A, Cozzi R (2003) Lanreotide 60 mg, a new long-acting formulation: effectiveness in the chronic treatment of acromegaly. J Clin Endocrinol Metab 88:5258–5265
Karavitaki N, Botusan I, Radian S, Coculescu M, Turner HE, Wass JAH (2005) The value of an acute octreotide suppression test in predicting long-term responses to depot somatostatin analogues in patients with active acromegaly. Clin Endocrinol (Oxf) 62:282–288
Pokrajac A, Claridge AG, Shakoor SKA, Trainer PJ (2006) The octreotide test dose is not a reliable predictor of the subsequent response to somatostatin analogue therapy in patients with acromegaly. Eur J Endocrinol 154:267–274
Cozzi R, Attanasio R, Lodrini S, Lasio G (2004) Cabergoline addition to depot somatostatin analogs in resistant acromegalic patients: efficacy and lack of predictive value of prolactin status. Clin Endocrinol (Oxf) 61:209–215
Trainer PJ, Drake WM, Katznelson L, Freda PU, Herman-Bonert V, van der Lely AJ, Dimaraki EV, Stewart PM, Friend KE, Vance ML, Besser GM, Scarlett JA, Thorner MO, Parkinson C, Klibanski A, Powell JS, Barkan AL, Sheppard MC, Malsonado M, Rose DR, Clemmons DR, Johannsson G, Bengtsson BA, Stavrou S, Kleinberg DL, Cook DM, Phillips LS, Bidlingmaier M, Strasburger CJ, Hackett S, Zib K, Bennett WF, Davis RJ (2000) Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N Engl J Med 342:1171–1177
van der Lely AJ, Hutson RK, Trainer PJ, Besser GM, Barkan AL, Katznelson L, Klibanski A, Herman-Bonert V, Melmed S, Vance ML, Freda PU, Stewart PM, Friend KE, Clemmons DR, Johannsson G, Stavrou S, Cook DM, Phillips LS, Strasburger CJ, Hackett S, Zib KA, Davis RJ, Scarlett JA, Thorner MO (2001) Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. Lancet 358:1754–1759
Parkinson C, Ryder WDJ, Trainer PJ, the Sensus Acromegaly Study Group (2001) The relationship between serum GH and serum IGF-I in acromegaly is gender-specific. J Clin Endocrinol Metab 86:5240–5244
Parkinson C, Renehan AG, Ryder WD, O’Dwyer ST, Shalet SM, Trainer PJ (2002) Gender and age influence the relationship between serum GH and IGF-I in patients with acromegaly. Clin Endocrinol (Oxf) 57:59–64
Engström BE, Burman P, Karlsson FA (2002) Men with acromegaly need higher doses of octreotide than women. Clin Endocrinol (Oxf) 56:73–77
Cozzi R, Attanasio R, Grottoli S, Pagani G, Loli P, Gasco V, Pedroncelli AM, Montini M, Ghigo E (2004) GH and IGF-I levels in acromegalic patients during treatment with Somatostatin analogs: should hormonal targets be lowered to assert a good control of the disease? J Endocrinol Invest 27:1040–1047
Acknowledgments
We are indebted to all the physicians and nurses who took care of the patients throughout the years, as well as to all the patients who trusted us and allowed us to get insight into the different aspects of this fascinating disease.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Attanasio, R., Montini, M., Valota, M. et al. An audit of treatment outcome in acromegalic patients attending our center at Bergamo, Italy. Pituitary 11, 1–11 (2008). https://doi.org/10.1007/s11102-007-0059-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-007-0059-1