
Abstract
Objective To assess the costs incurred by the public health services and patients as a result of tuberculosis (TB) treatment. Setting The study was conducted in a government hospital located in the northern region of Malaysia. Method Retrospective data were collected from medical records and the patients were observed until the completion of their medication. A pharmacoeconomic evaluation was applied to calculate direct and indirect costs. Main Outcome Measure Direct and indirect costs of tuberculosis treatment in a government health institution. Results Two hundred and one tuberculosis patients were included in the study. Different regimens with various durations of treatments were used. The direct medical and non-medical costs as well as indirect costs were calculated and were found to be as follows: US$61.44 for anti-tuberculosis drugs and supplies, US$28.63 for X-ray examinations, US$28.53 for laboratory tests, US$20.03 for healthcare staff time, US$4.28 for hospitalisation, US$43.20 for overhead costs, US$608.11 for transportation and meals and US$118.78 for time away from work. The cost to the patients constitutes approximately 80% of the total cost of the treatment. Conclusion The cost of treating the illness of tuberculosis per patient was US$916.4. The cost of anti-tuberculosis drugs constituted the highest proportion of the cost to the public health services (31.7%) while the cost to the patient constituted the major proportion of the total cost of the illness (79.4%).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In spite of the availability of effective anti-tuberculosis drugs, tuberculosis (TB) is considered as the first single infectious killer disease in the world. Approximately one third of the world’s population is infected with Mycobacterium Tuberculosis, with approximately 9 million new cases and 3 million deaths per year [1–4]. Approximately 75–80% of tuberculosis cases are in the economically productive age group, especially in developing countries, where 95% of new cases and deaths occur [5].
The economic impact of tuberculosis comes from the large direct and indirect costs incurred by the patients, suffered as a result of loss of income following the inability to work (average of 20–30% of annual household income) and premature deaths (fifteen years of lost income) [6].
Studies conducted in some developing countries found that the average cost for the treatment of susceptible tuberculosis was in the range of US$276–1,546; for multi-drug resistant tuberculosis, this was US$1,000–10,000 [6, 7].
The Malaysian National Tuberculosis Control Programme (NTB) was launched in 1961. At that time, tuberculosis was the number one cause of morbidity and mortality. As in other developing countries, and in spite of the implementation of the World Health Organization (WHO) and Malaysia Tuberculosis Control Programme guidelines and recommendations (that resulted in the treatment of tuberculosis patients through directly observed therapy which was the most cost-effective means of combatting non-adherence to the intermittent (less than daily) regimens of therapy [8]), the number of tuberculosis patients was steadily rising annually at the incidence rate of 62.3 per 100,000 individuals in the year 2001 [9].
The implementation of NTB activities in Penang, a state in the northern region of Malaysia, was achieved through the State TB Managerial Team of the state. This part of the country also witnessed an annual increase of tuberculosis cases with the incidence rate of 61.7 in the year 2001 [10].
This study was conducted to determine the economic burden of tuberculosis treatment in Penang both for the patient and the payer i.e., the government, and to provide to the policy-makers and health planners the information on the cost to treat these cases. This information would give justification for the continuous financial allocation for tuberculosis treatment and its management and more importantly, for health promotion and preventive measures. This study would also provide preliminary findings for future cost-effectiveness studies to identify effective new interventions in the service delivery with lower costs.
Methods
Study design
Retrospective and prospective prevalence-based partial pharmacoeconomic evaluations were used in this study. In this study, the authors have considered only the cost factors and not the outcomes of therapy. All costs were calculated according to the societal perspective (i.e., most of the relevant and important costs and consequences that individual members of the society could experience related to tuberculosis were included). Prior to the data collection process, permission to conduct this study was obtained directly from the director of the hospital and the relevant heads of departments. Verbal consent was obtained from each patient. Patient confidentiality has been strictly maintained throughout the study period.
All types of direct costs were obtained from different hospital departments while the indirect costs to the patient were estimated by interviewing 30 patients who were randomly selected. The total costs studied included direct medical costs covering the assessed cost of hospitalisation, medications, diagnostic laboratory tests, X-ray films and reagents and the cost of time incurred by health personnel. For example, the total cost of the laboratory tests used for tuberculosis patients throughout the treatment period was obtained by multiplying the total number of each type of laboratory test with the cost per test. The personnel cost was estimated by using the cost per minute according to the government monthly salary. The health personnel in this study included all staff from different departments dealing with tuberculosis patients at the diagnosis stage, during the treatment process or during the hospitalisation period. The cost of working time spent by health personnel was estimated for X-ray staff, laboratory staff, pharmacy staff, Chest Clinic staff, staff involved in DOT and ward staff. All costs of anti-tuberculosis drugs were calculated according to the standard government drugs price list.
Direct non-medical costs included the cost of transportation to the clinic and back home, meals and telephone, electricity and water bills. The standard government transportation rate produced by the Ministry of Finance was used in the calculation of the total cost of transportation by multiplying the distance from home to the clinic (both ways) for each patient with the cost per kilometre (approximately US$0.13 per kilometre). The total cost of food throughout the period of treatment was estimated by multiplying the total number of visits with the average cost per meal (i.e., US$0.79). The costs of building, vehicles and equipment were excluded in this study because the information could not be obtained and the reliability of the sources of information was questionable. Overhead costs or utilities included in the study were electricity consumed in the clinic and the water and telephone bills incurred throughout the period of the study. These costs were obtained from the management office and they were estimated according to the actual bills incurred in the hospital for the specified period of time.
Indirect costs included the cost of time away from work or lost of productivity. For the estimation of the cost of time away from work, a simple survey was conducted on 30 patients chosen randomly from the list of TB patients to determine the time during which the patient was not able to work due to the illness and to obtain the patient’s monthly income when he or she was healthy and working (i.e. time (day) away from work × daily wage/patient = out-of-work cost).
All costs were calculated in Malaysian currency (RM) and converted to American dollars according to the 2003 exchange rate of US$1.00 = RM 3.80.
Study location, time frame and population
Penang is one of the fourteen states in Malaysia. It is an island, which is separated from the west coast of Peninsular Malaysia by the Straits of Malacca. The island measures a modest two hundred eighty five square kilometres and is inhabited by 1,337,400 people. Penang was selected for this study for its high prevalence of tuberculosis cases compared with other states [10].
The community varies from poor to rich and there are different ethnic groups––Malays, Indians with the majority group being Chinese. The Chest Clinic at the Penang Hospital was the location selected for this study because of the large tuberculosis case loads, the availability of essential data, a good recording and reporting system and the presence of a consultant.
The study population consisted of all tuberculosis patients, on directly observed treatment (DOT), who started a new course of treatment at the clinic from May 2002 to February 2003 and these cases were followed through until the completion of treatment in August 2003. Patients were excluded from the study if they were transferred from the hospital to complete their treatment at other health facilities, if they were without treatment during the observation period or if they died before the completion of treatment. All patients studied were required to go to the hospital during working hours to take their medication under the direct observation of the Chest Clinic nurses. Pulmonary and extra-pulmonary patients were attended upon daily for the first two months and then twice weekly for the remainder of the duration of treatment.
The drug regimen was prescribed according to the type of tuberculosis disease. In the case of susceptible tuberculosis, patients were mainly taking three or four drugs in the initial two-month phase and two or three drugs in the subsequent four-month phase. Essential anti-tuberculosis drugs were rifampicin, isoniazid, pyrazinamide, ethambutol and streptomycin. Pyridoxine was given to prevent side-effects of isoniazid drugs. If the patients suffered relapses, interrupted their treatment or did not respond to the regimen given for susceptible tuberculosis, a retreatment regimen consisting of rifampicin, isoniazid, pyrazinamide, ethambutol and streptomycin was used for the initial two months while in the subsequent phase, streptomycin was added for one month, and rifampicin, isoniazid and ethambutol for another 5 months.
Data analysis
The statistical package for the social sciences (SPSS) for the Windows version (11.0) and Microsoft Excel were used for data analysis. All findings were reported descriptively using percentages; the currency used was in US dollars.
Results
Demographic and clinical analysis
All patients selected were managed to be interviewed and followed up. One hundred and forty-nine (74.2%) of the tuberculosis cases were male patients and 52 cases (25.8%) were females. Most of the patients were within the 15–54 age group (66.2%), which is considered the most economically productive. Sixty-eight patients (33.8%) were more than 54-years-old. There were 112 Chinese patients (55.7%), followed by 68 Malay patients (33.8%), 19 Indian patients (9.5%) and two Indonesian patients (1.0%). One hundred and seventy-seven patients (88.0%) had completed primary and secondary schools, seven patients (3.6%) had university education while 17 patients (8.4%) possessed no formal education. One hundred and six patients (52.8%) were not working, 71 patients (35.3%) had a monthly income of less than US$263.15 and only 24 patients (11.9%) enjoyed a monthly income of more than US$263.15. One hundred and sixty-seven patients (83.1%) had pulmonary tuberculosis, 22 patients (10.9%) had extra-pulmonary tuberculosis, six patients (3.0%) had tuberculosis in combination with HIV, three patients (1.5%) had drug resistant tuberculosis and three others (1.5%) had both pulmonary and extra-pulmonary tuberculosis. Other information on the drug regimen and duration of treatment is shown in Table 1.
Cost analysis
Costs to the public health services (direct medical and non-medical costs)
Table 2 shows the total costs incurred by the public health services. The study found that the average number of X-ray films used per patient was between five and six films. The cost per film was US$4.87 (including reagents). Therefore, the total cost of X-ray examinations (including supplies and reagents) was US$5,754.47 with an average cost incurred per cured patient being US$28.62.
Laboratory tests represented the initial step in the diagnosis, management and monitoring of tuberculosis patients till the patients were cured. In the clinic, tuberculosis patients were ranked as group “C” patients. This meant that they were charged at the lowest price for all laboratory tests used. The results showed that the total cost for all tests was US$5,734.47.
The total cost of anti-tuberculosis drugs and supplies used based on the government drugs price list was US$12,350.75 and the cost per patient was US$61.44. The total cost of time spent by the health staff was US$4,026.46. The cost of hospitalisation per day, including food, was US$0.79 and therefore, the total cost incurred by each patient was US$860.52.
Overhead costs or utilities cost estimated was US$8,684.21 and the cost per patient was US$43.20.
Cost to patients
Cost of transportation (direct non-medical cost). Table 3 shows the costs borne by the patients for transportation, food and time lost due to illness. The transportation cost per patient was US$516.87, which constituted 71.1% of the total costs incurred by the patient.
Cost of meals (direct non-medical cost). As mentioned, all patients underwent their treatment through the directly observed short-course therapy. Therefore, patients would make frequent visits to the clinic––either daily or twice weekly––to have their tuberculosis treatment. During these visits, it was estimated that a patient needed to have one meal per visit, the estimated average cost per meal being US$0.79. The total cost of food throughout the period of treatment was US$18,340.26, by multiplying 23,231 visits with US$0.79 (i.e., the average cost per meal). The cost to the family member accompanying the patient was not calculated because the data were collected retrospectively and this information was not found in the records.
Cost of time away from work (indirect cost). The average time away from work was 14.15 days (ranging from 0 to 84 days) and the average of money lost per patient was US$118.78.
Cost of treatment per patient cured
Table 4 shows that the money paid by patients constituted approximately 80.0% of the total costs of the tuberculosis treatment compared to 20% covered by the government health services.
Discussion
The study found that 88.1% of the patients had only attained a low level of education. In terms of age distribution, the study found that 65.8% of the patients were within the age range of 15–54 years. As frequently reported in studies, e.g., those conducted by Lyawoo (2004) [9] and Zwarenstein et al (1998) [11] , this would be considered the most economically productive period of a person’s life. The economic impact of tuberculosis comes from the largest direct and indirect cost to the patient due to lost of income by disability to work and premature death. Tuberculosis is the first killer that kills nearly two million people yearly at their most economically productive age. According to WHO, 20–30% of an annual household income (3–4 months) is lost due to the illness and about 15 years of income is lost due premature deaths [6].
It was determined that pulmonary tuberculosis was suffered by more than 82.0% of patients, while extra-pulmonary tuberculosis constituted 10.8%. Therefore, there was a higher proportion of pulmonary tuberculosis patients. This result is consistent with the national data reported by Lyawoo [9]. Pulmonary TB commonly accompanies with extra-pulmonary tuberculosis [2, 13]. It is estimated that one person with active tuberculosis left untreated will infect 10–15 people in the community annually. This is avoidable and if proper preventive measure is implemented.
Since HIV infection was considered the strongest risk factor for the development of active tuberculosis disease [12, 13], the Malaysian Tuberculosis Control Programme had recommended that the HIV test should be carried out for all patients. TB has continued to thrive in low-income countries to the extent where TB was identified as the infectious disease causing the largest burden of ill health to adult populations worldwide. In these nations, the advent of HIV has made this situation even worse. The study found that the test had actually been conducted for the majority of the patients. In addition, the study also found that other laboratory tests were used to monitor drugs side-effects, such as to the liver, and therefore, the liver function test had to be carried out. These additional tests would definitely contribute to the higher costs of managing the patients. But however, these proactive initiatives would definitely contribute to cost saving from unnecessary consequences due to HIV including its related ill-effects and side-effects of drugs. In addition, patient with HIV positive has different treatment regimen as compared to patient without HIV positive. Treatment for TB will be effective if this condition is known.
The study found that a large proportion of direct medical costs from the total costs of illness was associated with anti-tuberculosis drugs (32.4%) at the cost per patient equivalent to US$61.44, which was similar to the finding by Islam (2002) who compared the drug costs with overall total expenditure (37.8%) [14]. On the other hand, as reported in the Sanderson (1995) findings [15], the study also found that there was an additional cost associated with streptomycin (which is the only drug used through injection). This drug required additional supplies (i.e., water for injection and syringes) and therefore, it contributed an additional cost in the management of the patients.
Since an active monitoring programme had been implemented for tuberculosis patients at the clinic, a higher cost was associated with laboratory examinations per patient. The study found that the cost of laboratory tests per treated patient was US$28.50 which constituted 3.1% and 15.2% of the total costs and costs of government health services, respectively.
Hospitalisation was recommended only in the initial intensive phase of treatment for patients with advanced tuberculosis, patients with other complications such as HIV, patients with drug resistant tuberculosis or those who may not have adhered to the prescribed treatment. The costs of treating patients with TB remains high, especially when patients require hospitalisation. Furthermore, extra costs are incurred if multi-drug resistant strains develop as a result of patient non-compliance with treatment. These costs result from lengthy hospitalisation, expensive second-line drugs and sometimes surgery. Therefore, the cost for hospitalisation per patient in this study (i.e., US$4.30) was considered low. Sanderson (1995) reported that the cost of hospitalisation per patient had been US$23.13.
The implementation of treatment for tuberculosis patients was achieved through the direct observation strategy. For that, the cost associated with transportation to and from the clinic constituted a high portion of the costs to the patient and to the total costs of treatment, 71.0% and 56.5%, respectively. The estimated cost of meals for patients during the treatment period was calculated as 12.5% of patient costs and 9.9% of the total cost of treatment. This cost had not been mentioned or calculated in other studies.
The cost associated with the loss of productivity (i.e., US$118.78) constituted 16.3% of the costs incurred by the patient and 12.9% of the total costs. Different explanations can possibly be made for this low cost estimate. Active health education and periodical seminars might encourage people to seek for immediate treatment by attending to health centres which offer tuberculosis services instead of taking a long time treating themselves via religious practitioners, herbal medicine and divining [16] all of which might cause unnecessary health consequences to the patients and increase the economic burden of the society.
Similar to the findings of the previous study [17], the costs to the patients constituted approximately 80% of the total costs of the treatment. The costs to the patients could have been reduced through early diagnosis and detection to avoid loss of time away from work due to illness and by applying an alternative treatment design to reduce the cost of transportation which was incurred by patients e.g., the patient took their drugs weekly or fortnightly from the nearest health unit in the initial phase and monthly in the subsequent phase.
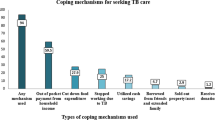
In addition, tuberculosis causes social and psychological problems such as person with this disease may be rejected from the society or may not accepted for marriage. Due loss of income, households may make strategies to reduce total family expenses such as by removing their children from school, decreasing of food intake by the family, sell assets and borrow money for their daily living. Fortunately, these situations in Malaysia are reduced because all patients with TB are given free drugs and treatments by the government.
This study is the first of its kind in Malaysia and has definitely contributed significant information to the policy makers, healthcare managers and practitioners; this is in spite of the fact that some of the relevant information on costs could not be obtained when it was conducted. The study would have been more meaningful if the sample size had been larger. The authors hope that more studies related to tuberculosis will be conducted in the future, taking into consideration the few limitations made evident in this study. The inclusion of other types of costs e.g., mortality costs and the effect on the society, could make such studies even more informative.
Recommendations
Since the costs to the patients were high compared to the costs to the public health services, it is recommended that further research be conducted to create an alternative treatment design to reduce these costs. Further prospective studies in cost-effectiveness are required to determine actual clinical outcomes and the most cost-effective drug regimens used for tuberculosis treatment. There are additional costs associated with streptomycin compared with ethambutol. Ethambutol is the companion drug to prevent drug resistance. Centers for Disease Control and Prevention (2003) preferred that ethambutol to be used as first-line treatment and streptomycin as second-line [18]. Furthermore, streptomycin has limited penetration into membranes. Therefore, it is recommended that the extended use of ethambutol should be reviewed and supported, if possible, to reduce the costs of treatment.
Conclusion
The pharmacoeconomic analysis showed that the estimated average cost of the tuberculosis treatment per patient is US$916.40. The cost of anti-tuberculosis drugs constitutes the highest portion of the costs incurred by the government health services. The cost of transportation to and from the Chest Clinic constituted the major portion of the costs to the patient. The cost of tuberculosis treatment increases with the increase in the duration of the regimen (the longer the duration, the higher the cost of treatment).
References
World Health Organization. Anti-tuberculosis drug resistance in the world. Geneva: WHO Global TB Programme; 1997.
Elsony A, Suliaman E, Shinawy A. Manual of tuberculosis control programme in Sudan, 3rd ed. Sudan: Federal Ministry of Health; 2000.
American Thoracic Society. Diagnostic standard, classification of TB in adults and children. Am. J. Respir. Care Med. 2000;161:1376–95.
World Health Organization. Towards a TB free future. Geneva: WHO/CDS/STB; 2001.
The Caribbean Epidemiology Centre. Tuberculosis manual of prevention & control procedures 1st ed. Trinidad; 1997.
World Health Organization. The economic impacts of tuberculosis. Amsterdam: Stop TB Initiative; 2000.
Wyss K, Kilima P, Lorenz N. Cost of tuberculosis for household and health care providers in Dar es Salaam, Tanzania. Trop. Med. Int. Health 2001;6:60–8.
Iseman M, Chan E. Current medical treatment for tuberculosis. BMJ 2002;320:282–6.
Lyawoo K. Tuberculosis in Malaysia: problems and prospect of treatment and control. Tuberculosis 2004;84:4–7.
Malaysia Tuberculosis Control Programme. NTB report for the year 2001. Malaysia: Ministry of Health; 2001.
Zwarenstein M, Schoeman J, Vundule C, Lombard C, Tatley M. Randomised controlled trial of self-supervised and directly observed treatment of Tuberculosis. Lancet 1998;352:1340–1343.
Jerant A, Bannon M, Rittenhouse S. Identification and management of Tuberculosis. Am. Fam. Physician 2000;61:2667–2678.
Centers for Disease Control and Prevention. Core curriculum on tuberculosis, 4th ed. Atlanta: Department of Health & Human services; 2000.
Islam M, Wakai S, Ishikawa N, Chowdhury A, Vaughan J. Cost-effectiveness of community health workers in tuberculosis control in Bangladesh. Bull. World Health Organ. 2002;80:445–50.
Sanderson P. An economic evaluation of alternative programme designs for Tuberculosis control in rural Uganda. Soc. Sci. Med. 1995;40:1203–1212.
Hurtiga A, Pande S, Porter J, Dam D. Tuberculosis treatment and private practitioners in Kathmandu Valley. J. Nap. Med. Assoc. 2000;39:163–8.
Guwatudde D, Zalwango S, Kamy M, Debanne S, Diaz M, Okwera A, Mugerwa R, King C, Whalen C. Burden of tuberculosis in Kamala, Uganda. Bull. World Health Organ. 2003;81(11):799–805.
Centers for Disease Control and Prevention. morbidity and mortality weekly report–treatment of tuberculosis. June 20, 2003/52(RR11);1–77.
Acknowledgements
The authors would like to thank all staff at the Chest Clinic of the Penang Hospital for their continuous help and their endless patience in searching for the files of tuberculosis patient throughout the data collection period. Their assistance is greatly appreciated.
Conflict of interests
We would like to declare that there is no conflict of interests in conducting this research. This study was conducted as part of the MSc research.
Author information
Authors and Affiliations
Corresponding author
Additional information
The Publisher apologises for the extreme delay in publication of this article.
Rights and permissions
About this article
Cite this article
Elamin, E.I., Ibrahim, M.I.M., Sulaiman, S.A.S. et al. Cost of illness of tuberculosis in Penang, Malaysia. Pharm World Sci 30, 281–286 (2008). https://doi.org/10.1007/s11096-007-9185-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-007-9185-0