
Abstract
Objective To determine if an educational program designed for community pharmacists to help patients self manage their asthma could improve pharmacists abilities to facilitate asthma treatment plans. Setting Hamilton and Toronto, Ontario, Canada. Method A randomized controlled trial involving volunteer community pharmacists who received either an asthma education program (AEP; intervention group) or a delayed AEP (control group). The AEP consisted of a one-day workshop and two follow-up telephone calls. Teaching methods progressed from a didactic approach to self-directed learning and role playing with simulated patients (SPs). The primary outcome was measured by SPs who conducted unannounced pharmacy visits. Main Outcomes Measures The number of appropriate (defined a priori) action plans facilitated by the pharmacist was the primary outcome. Facilitated was defined as the pharmacist recommending a specific plan, taking responsibility for telephoning the physician, or ensuring the patient would take responsibility for contacting the physician. Results Thirty-three pharmacists were randomized to the intervention group and 31 pharmacists were randomized to the control group. Pharmacists in the intervention group facilitated an appropriate plan in 44.8% of situations (117 out of a possible 261) compared with 29.3% (79 out of a possible 270) in the control group, (mean difference 15.5% (95% CI: 7.4–23.8%; P = 0.0004)). Intervention group pharmacists were better able to facilitate plans for the ‘under use of inhaled corticosteroids,’ ‘exposure to pet dander as an asthma trigger,’ and ‘overuse of short-acting beta-agonist’ problems. Intervention group pharmacists exhibited better overall communication skills (including empathy, coherence, verbal skills, and nonverbal skills). Conclusion This AEP produced improvements in pharmacists’ abilities to facilitate plans for SPs in a community pharmacy setting.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Impact on practice
-
A multi-method asthma continuing education program can produce improvements in pharmacists’ abilities to facilitate asthma management or treatment plans.
-
Using the standardized approach of simulated patient to measure the effect of the workshop at the practice site makes it possible to identify which asthma-related problems (such as the underuse of inhaled corticosteroids) pharmacists could manage better than others (such as identifying cost as a barrier to inhaled corticosteroids).
-
Less than half of the pharmacists in both groups were able to facilitate plans for five of nine common asthma-related problems presented to them demonstrating that improvements in asthma knowledge and management skills are still needed.
-
This study provides insight into the elements of a continuing education program that were successful and the elements that should be improved in future delivery.
Introduction
When patients with asthma participate in managing their disease they achieve better health outcomes [1–4]. Patient participation—or asthma self-management—involves asthma patients actively participating in their health care by (1) identifying and avoiding asthma triggers, (2) recognizing the early signs of severity of an asthma attack, (3) participating in the development of their personal action plan, (4) becoming competent in using assistive devices, and (5) becoming confident, taking responsibility for and using their action plan for early intervention and self-management to prevent flare ups [5, 6]. Asthma self-management has been shown to reduce asthma-related hospitalizations and emergency room visits, unscheduled physician visits, days lost from work, episodes of nocturnal asthma and to improve the use of beta-2-agonists and inhaled or oral corticosteroids [7, 8]. In contrast, when asthmatic patients received education only through the method of transferring information, improved health outcomes have not been shown to be achieved [9].
Many studies have examined the effect of various levels of asthma education provided by nurses and physicians to patients [2, 10–12]. Pharmacists have explicitly promoted their role in the care of asthma patients [13, 14], and a number of randomized controlled trials have shown the benefits of using pharmacists as a patient educators [15–18].
All of these studies demonstrate the impact that pharmacists can have on facilitating changes in asthma therapy for patients [15–18]. Pharmacists see asthma patients regularly in a community pharmacy, often many times in between physician visits. Therefore, community pharmacists are in an excellent position to identify patients who would benefit from asthma education.
To teach patients to self-manage asthma, pharmacists must have the necessary knowledge and skills. These abilities include how to identify if a patient’s asthma is controlled or uncontrolled, identify drug or non-drug-related issues that may be hindering a patient’s asthma control, identify patients without an emergency action plan, and facilitate a plan with the patient and his/her physician to help improve the patient’s asthma control. If pharmacists shift their focus from delivering information about drug therapy to integrating drug and device information into a program focusing on achieving asthma control then pharmacists and patients would be approaching asthma management from similar perspectives.
Aims of the study
The objective of this study was to examine whether an educational program for pharmacists improved the pharmacists’ ability to facilitate asthma management or treatment plans in their practice site.
Methods
Design
This study was a randomized controlled trial approved by the St. Joseph’s Hospital Research Ethics Board (Hamilton, Ontario).
Study participants
Participants were volunteer pharmacists and were included if they worked more than 20 h per week in the same community pharmacy located close to the study center. Pharmacists were excluded from the study if they had ever participated in an intense asthma training program prior to the study, if their main language of practice was not English, if they were not available to attend our workshop study dates, or if another pharmacist from their practice site had all ready been included in the study.
Randomization and blinding
Pharmacists were randomized in blocks of six from a random numbers table. The research team and participating pharmacists were not blinded to group allocation, however simulated patients (SPs) performing outcomes evaluation were blinded to assignment of the pharmacists to intervention or control groups.
Intervention
The educational intervention consisted of a one-day workshop and, two follow-up telephone calls two and four weeks after the workshop. Pharmacists in the intervention group received the workshop before primary study outcomes were measured whereas those in the control group received the workshop afterwards. The workshop focused on therapeutic topics including knowledge of asthma and its drug therapies, the role of peak expiratory flow monitoring, and inhaler and device use. Skill-building topics focused on how to introduce the concept of asthma self-management with patients, a structured interview process for assessing patients and how to develop a patient’s asthma action plan. A variety of teaching methods were chosen (e.g. didactic, group work, role playing) to transition participants through the three major orientations of learning: transmission (facts, skills, and values transmitted in the traditional way), transaction (intelligent problem solving occurring through dialogue between the learners and educators), and transformation (personal and social transformation to incorporate learning into practice through self-inquiry and self-reflection) [19].
A tool-kit of resources was designed for pharmacists participating in the educational intervention and the one-day workshop taught pharmacists how to use these tools. The kit included: (1) a set of critical reviews of the literature formatted as one to three page summaries (Critically Appraised Topics or CATs [20], relating to common asthma drug-related problems for both physician and patient audiences (e.g. benefits of inhaled corticosteroids, role of long-acting beta-agonists), (2) a tool to prompt pharmacists to collect pertinent patient information, (3) a template letter for pharmacist communication with a physician, and (4) a pharmacist to patient documentation sheet (otherwise referred to as a personal asthma treatment plan).
Pharmacists received two follow-up telephone calls before the SP visits. Before the phone call, pharmacists completed a self-evaluation of their behavior and motivation to provide pharmaceutical care for patients with asthma (Behavioural Pharmaceutical Care Scale [BPCS] modified only by changing all general statements on chronic disease to specific statements on asthma) [21]. The results of this self-evaluation were used to structure and discuss any individual issues the pharmacists may have faced when trying to provide better care for patients with asthma at their practice sites.
Previous studies examining pharmacist interventions in asthma care have included structured educational programs for pharmacists with some similarities to the intervention delivered in this study [15–18, 22]. This study was particularly focused on gaining a better understanding about how the intervention (i.e. education program) specifically affected pharmacist assessment skills and the information and recommendations provided by the pharmacists in practice so that the relationship between the intervention and direct patient-focused educational outcomes could be determined.
Outcome measures
Primary outcome
SPs from programs at the University of Toronto and McMaster University measured the primary outcome which was the number of plans that a pharmacist facilitated during unannounced visits from three SPs. The primary outcome measure was used to represent the ability of pharmacists to facilitate a plan for asthma-related problems in a realistic work environment. A total of four patient-actors were trained for each case. The SPs received structured training on delivering their case and documenting their findings on structured data collection forms prior to visiting the pharmacies. Each SP was responsible for scheduling pharmacy visits. SPs were provided a picture of each study participant to ensure they approached the correct pharmacist in each pharmacy. Visits occurred at peak and slow times for feasibility reasons, however, if the pharmacist was too busy during their first encounter to engage the SP the SP was instructed to go back to the pharmacist a second time.
For this study, a pharmacist-facilitated plan was defined as the pharmacist recommending a specific plan, taking responsibility for telephoning the physician, or ensuring the patient would take responsibility for contacting the physician. The SPs visited pharmacists’ practice sites between three and five weeks after the workshop. Each SP had three asthma-related problems that the pharmacist needed to identify, create a plan for, and facilitate the uptake of the plan in order to achieve an acceptable or optimal score. After each visit, the SP completed a four-part structured outcome evaluation form outlining items related to the (1) the questions the pharmacist asked during a history or dialogue, (2) the information the pharmacist provided, (3) the recommendations the pharmacist provided, or the plans that were suggested to resolve or facilitate the action plan for each asthma-related problem, and (4) the evaluation of communication skills.
The items on the forms were structured as a series of questions with responses of yes, no and don’t know. If the SP rated the item as don’t know they were instructed to write in comments to elaborate on the situation. Ratings provided by the SPs were categorized into optimal, acceptable, and unacceptable facilitation of an asthma management plan according to predetermined criteria. For example, the pharmacist interaction was categorized as acceptable in the under-use of inhaled corticosteroid (case 1) if the SP indicated that the pharmacist had instructed the patient to start using the inhaled corticosteroid as prescribed. If the pharmacist also provided instructions on minimizing the risk of osteoporosis by addressing lifestyle issues and stated they were going to call the physician to inform the physician of the intervention then the encounter was categorized as optimal. If the pharmacist did not encourage use of the inhaled corticosteroid or did not discuss the issue then the encounter was categorized as unacceptable.
The primary outcome measure graded the ability of pharmacists to conceive action plans based on three categories: optimal, acceptable, and unacceptable. Example outcome assessment criteria are provided in Appendix 1. Criteria for classification as optimal, acceptable, or unacceptable responses by the pharmacist were determined a priori because they varied by patient case and each encounter was evaluated.
Secondary outcomes
The SPs evaluated pharmacists’ general communication skills using the Global Rating Scale (GRS) [23]. The GRS has five domains, empathy, coherence, verbal expression, non-verbal expression, and overall knowledge and skills.
Sample size and analysis
The sample size of 31 per group was based on the intervention group facilitating at least two more problems (of a potential nine problems) (22% difference) compared to the control group, a standard deviation of 0.3, a power of 80%, and an alpha of 0.05.
To test for differences between intervention and control groups, significance levels were based on the Student’s t-statistic when comparing means and on the chi-square or Fisher’s exact statistic when comparing proportions. Ninety-five percent confidence intervals are reported on the differences between means and proportions for the primary and relevant secondary outcomes. Repeated measures analysis of variance (ANOVA) was used to identify whether treatment group (primary outcome), asthma-related problem, or the interaction between treatment group and asthma-related problem were associated with the primary outcome. Statistical analyses were conducted using the SAS Software System (Version 6.12, SAS Institute Inc., SAS Campus Drive, Cary, NC).
Results
Enrollment and dropouts
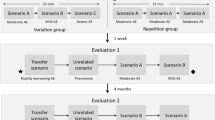
Of the 160 pharmacists that were screened for inclusion, 33 pharmacists were allocated to the intervention group and 31 pharmacists were allocated to the control group (see Fig. 1 for further details of allocation and dropouts). Five (7.8%) pharmacists dropped out of the study. Four pharmacists dropped out of the intervention group, one did not want to complete the SP visits after the first experience, and three were lost to follow up. One pharmacist dropped out of the control group because of a disagreement with the pharmacy manager. Fifteen (52%) of the 29 pharmacists completing the study received two follow up telephone calls and 14 (48%) of the 29 pharmacists completing the study received two follow-up telephone calls.

Study flow diagram
Demographics of participants
The characteristics of participating pharmacists are shown in Table 1. No statistically significant differences were found between groups for any of the demographic characteristics measured. The intervention and control groups were similar in terms of self-reported age, sex, education level, employment status, and pharmacy staffing (number of pharmacists or technicians). While not statistically significant, a notable difference between groups was seen in the number of prescriptions dispensed per month and the number of new prescriptions dispensed per month, and the number of telephone calls to a drug information center which were all higher in the intervention group.
Facilitated plans (primary outcome)
Pharmacists in the intervention group produced 117 appropriate (53 optimal plus 64 acceptable) and 128 unacceptable plans during their interactions with SPs. Pharmacists in the control group produced 79 appropriate (21 optimal, 58 acceptable) and 187 unacceptable plans during their interactions with the SPs (Table 2 and Fig. 2). Therefore, pharmacists in the intervention group produced an appropriate plan in 44.8% of situations (117/261) compared with 29.3% (79/270) of appropriate plans produced by the control group pharmacists [95% CI on difference, 7.4–23.8%] (P = 0.0004, based on intention to treat ANOVA controlling for type of problem seen). Incomplete problems for the intervention pharmacists remaining in the study represent 6.0% (16/261) of the possible problems while incomplete problems for control pharmacists represent 1.5% (4/270) of possible problems. No discernable patterns to explain why certain problems had incomplete data collection could be identified.


(A) Percentage of optimal, acceptable, and unacceptable plans facilitated by pharmacists for Case 1: a very recent ER visit; (B) Percentage of optimal, acceptable, and unacceptable plans facilitated by pharmacists for Case 2: uncontrolled and unaware; (C) Percentage of optimal, acceptable, and unacceptable plans facilitated by pharmacists for Case 3: I’m new in town; and (D) Total percentage of optimal, acceptable, and unacceptable plans facilitated by pharmacists for all three SP visits
The repeated measures ANOVA analysis showed that the treatment group (P = 0.0004) and asthma-related problem (P = 0.0001) were each individually associated with the ability to facilitate a plan. The interaction between the treatment group and asthma-related problem was not associated with the ability to facilitate a plan.
Pharmacists in the intervention group were better able to facilitate plans for the following three problems: ‘the under use of inhaled corticosteroid’ in case 1 (93% vs. 67% plans facilitated), ‘the identification of pet dander as an asthma trigger’ (54% vs. 10% plans facilitated), and ‘the overuse of short-acting beta-agonist’ (89% vs. 50% plans facilitated) (see Table 2 for case descriptions). There was also a trend in favor of the intervention group identifying the problem and facilitating the plan for the problem of ‘when additional therapy besides beta-agonist and corticosteroid was needed’ (18% vs. 3% plans facilitated).
Less than 50% of pharmacists in both groups were able to facilitate plans for the majority of asthma-related problems. More than half of the pharmacists could not facilitate a plan for five of the nine common asthma-related issues presented to them. These issues were: the cost of a new inhaled corticosteroid, poor perceiver of asthma symptoms, additional therapy needed, smoking trigger, and lack of an emergency asthma action plan.
Communication skills
Pharmacists in the intervention group exhibited better overall communication skills compared to those in the control group (Table 3). This difference was statistically significant in favor of the intervention group for two of the three cases presented to the pharmacists. In both intervention and control groups, pharmacists exhibited better communication skills when presented with Case 1 and Case 3 compared to Case 2 (Table 2).
Modified Behavioural Pharmaceutical Care Scale
Pharmacists in the intervention group generated a total overall mean (SD) score on the modified BPCS of 76.62 (SD, 25.60) compared with pharmacists in the control group who generated a total overall mean score of 72.63 (SD, 26.92) (P = 0.58). There were no statistically significant differences seen between the intervention and control groups in the modified BPCS sub-domains of documentation, patient assessment, implementation and monitoring, and referral and consultation.
Follow up telephone call and sequencing of SP visits
Participating in a follow up call did not affect the pharmacists’ abilities to facilitate more plans. Sequencing of SP visits, representing whether pharmacists improved in their abilities to facilitate plans over time, did not affect the outcome of the study.
Type of asthma-related problem presented to participating pharmacists
Independent of group assignment, pharmacists were able to identify a problem and then facilitate a plan for certain problems better than others (the type of problem was an independent predictor of outcome regardless of assignment to the intervention or control group) (P = 0.0001). Pharmacists were better able to facilitate plans for problems presenting in Case 1 (44% of plans facilitated for presenting problems), and Case 3 (51%), compared with Case 2 (20%).
Discussion
This randomized controlled trial demonstrated that a specially designed asthma continuing education workshop could produce improvements in pharmacist’s abilities to facilitate plans for SPs. Achieving a successful study outcome required the pharmacist to go beyond identifying a problem and suggesting therapeutic options; it required the pharmacist to choose a solution with the patient and facilitate a plan to implement that solution so that the patient could leave the pharmacist with the ability to manage their asthma more effectively. The pharmacists participating in the workshop also demonstrated improved communication skills compared to their control counterparts.
The workshop was particularly successful in improving pharmacists’ ability to identify and facilitate plans for inhaled corticosteroid under use (in one of the cases), short-acting beta-agonist over use, and triggering asthma due to pet dander. While all problem areas in the SPs cases were incorporated into workshop, not all problems were covered using the same teaching methods or with equal emphasis. This may account for the variation in the abilities of the pharmacists to facilitate appropriate plans across asthma-related problems. There was one issue, inhaled corticosteroid underuse, presented in two cases. The pharmacists were able to handle this issue more effectively in the first case compared with the third case likely because two different contexts were used to present the issue. Further understanding of how context relates to problem identification is warranted.
Pharmacists who participated in the workshop also demonstrated better communication skills on objective assessment. This study showed that pharmacists can have an objective improvement in their communication skills if it is a focus of the training program. Improved communication is an important contributing factor to establish and maintain a successful clinician–patient interaction [24–28].
This study had a number of strengths in its design. It used a randomized controlled methodology. The primary outcome evaluation was conducted by SPs who were blinded to group assignment. Ninety-two percent of participants randomized were assessed for the primary outcome. There were three repeated evaluations of each pharmacist. The intervention was designed to be generalizable and transferable. The workshop used a mixture of teaching methods, beginning with didactic methods and ending with independent learning to help the pharmacist move from a traditional method of learning to one that had the greatest ability to transform their practice. The workshop focused on assessing the patient for control of their asthma so that pharmacists would be adopting a similar perspective to the patient (i.e. starting from the clinical problem) which would lead to more effective and meaningful dialogue.
There were a number of limitations to our study. First, the pharmacists participating in this study were volunteers and so may have been more highly motivated than their peers. Second, the participating pharmacists reported that sometimes they could detect the SP, particularly during for the second and third case due to heightened awareness. Third, this study did not measure the effect of the workshop on direct patient outcomes. Fourth, the time lag between the workshop and the objective outcome assessment may have been too short for pharmacist to integrate the complex behavior changes needed to change practice. Fifth, the BPCS was slightly modified from the original version by focusing the questions to experience with asthma patients with all other wording remaining the same, however, the modified scale was not revalidated based on the slightly revised wording. Sixth, SP encounters were not audiotaped so that fidelity of the assessment of outcomes was unable to be evaluated and the inter-rater reliability among SPs was not assessed. Finally, the study did not measure the maintenance of behavior change over the long term.
The principles of continuing medical education (CME) are analogous to those used for pharmacy continuing education. Interactive CME (i.e. CME that enhances activity and provides the opportunity to practice skills) is generally more effective than didactic CME in changing physician performance or patient outcomes [29, 30]. Sequencing of educational sessions also appears to have greater impact [29–31]. Determining the physicians’ practice or learning needs is necessary for effective education as this leads to increased potential for change. Each of the above variables was included in designing the intervention for this study. Other strategies that may improve some aspects of physician performance in the short-term include use of reminders, audit and feedback, computerized practice-based information, use of education or opinion leaders [29, 30, 32]. These strategies were not used in this study. The addition of these other methods could be considered for future integration and evaluation to determine if multiple methods have an additive effect.
Randomized controlled trials focusing on other populations that objectively evaluated the effects of pharmacist education to detect DRPs in the elderly [33], detect and resolve DRPs in community pharmacist practice [34], and to counsel on sunscreen use and photosensitizing medication [35] demonstrated that use of multiple educational techniques (i.e. two or more of providing written information, group education, videotape, one-to-one education) improves pharmacists’ abilities. Other studies have shown that pharmacists delivering pharmaceutical care can improve on patient-focused outcomes or reduce costs associated with asthma care [15, 16, 22, 36]. All of these involved training programs for pharmacists in the intervention group but details of the educational strategies used within the training programs are unknown. Further, none specifically examined whether the training programs improved pharmacists’ knowledge and skills for providing care to patients with asthma. This study is unique because it examined how knowledge and skills gained in a continuing education program were applied in practice and provided insight into the elements of a continuing education program that were successful and the elements that should be improved in future delivery.
Conclusion
This unique asthma education program produced improvements in pharmacists’ care to SPs.
References
Mesters I, Meertens R, Kok G, Parcel GS. Effectiveness of a multidisciplinary education protocol in children with asthma (0–4 years) in primary health care. J Asthma 1994;31(5):347–59
Boulet LP, Boutin H, Cote J, Leblanc P, Laviolette M. Evaluation of an asthma self-management education program. J Asthma 1995;32(3):199–206
Yoon R, McKenzie DK, Bauman A, Miles DA. Controlled trial evaluation of an asthma education programme for adults. Thorax 1993;48(11):1110–6
Mayo PH, Weinberg BJ, Kramer B, Richman J, Seibert-Choi OS, Rosen MJ. Results of a program to improve the process of inpatient care of adult asthmatics. Chest 1996;110(1):48–52
Green LW, Frankish CJ. Theories and principles of health education applied to asthma. Chest 1994;106(4:Suppl):219s–30s
Cote J, Golding J, Barnes G, Boulet LP. Educating the educators. How to improve teaching about asthma. Chest 1994;106(4:Suppl):242S–7S
Gibson PG, Powell H, Coughlan J, Wilson AJ, Abramson M, Haywood P, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2002;(3): CD001117. DOI 10.1002/14651858.CD001117
Newman S, Steed L, Mulligan K. Self-management interventions for chronic illness. Lancet 2004;364(9444):1523–37
Gibson PG, Powell H, Coughlan J, Wilson AJ, Hensley MJ, Abramson M, et al. Limited (information only) patient education programs for adults with asthma. Cochrane Database Syst Rev 2002;(1):CD001005. DOI 10.1002/14651858.CD001005
Allen RM, Jones MP, Oldenburg B. Randomised trial of an asthma self-management programme for adults. Thorax 1995;50(7):731–8
Bailey WC, Richards JMJ, Brooks CM, Soong SJ, Windsor RA, Manzella BA. A randomized trial to improve self-management practices of adults with asthma. Arch Intern Med 1990;150:1664–8
Kotses H, Stout C, McConnaughy K, Winder JA, Creer TL. Evaluation of individualized asthma self-management programs. J Asthma 1996;33:113–8
Role of the pharmacist in improving asthma care. National Asthma Education and Prevention Program. Am J Health Syst Pharm 1995;52(13):1411–6
The role of the pharmacist in improving asthma care. National Asthma Education and Prevention Program. Am Pharm 1995;NS35(11):24–9
McLean W, Gillis J, Waller R. The BC Community Pharmacy Asthma Study: a study of clinical, economic and holistic outcomes influenced by an asthma care protocol provided by specially trained community pharmacists in British Columbia. Can Respir J 2003;10(4):195–202
Weinberger M, Murray MD, Marrero DG, Brewer N, Lykens M, Harris LE, et al. Effectiveness of pharmacist care for patients with reactive airways disease: a randomized controlled trial. JAMA 2002;288(13):1594–1602
Stergachis A, Gardner JS, Anderson MT, Sullivan SD. Improving pediatric asthma outcomes in the community setting: does pharmaceutical care make a difference? J Am Pharm Assoc (Wash) 2002;42(5):743–52
Cordina M, McElnay JC, Hughes CM. Assessment of a community pharmacy-based program for patients with asthma. Pharmacotherapy 2001;21(10):1196–1203
Miller JP, Seller W. Curriculum perspectives and practice. Mississauga: Copp Clark Pitman; 1990
Sauve S, Lee HN, Meade MO, Lang JD, Farkouh M, Cook DJ, et al. The critically appraised topic: a practical approach to learning critical appraisal. Ann RCPSC 1995;28(7):396–8
Odedina FT, Segal R. Behavioural pharmaceutical care scale for measuring pharmacists’ activities. Am J Health Syst Pharm 1996;53:855–65
Mangiapane S, Schulz M, Muhlig S, Ihle P, Schubert I, Waldmann HC. Community pharmacy-based pharmaceutical care for asthma patients. Ann Pharmacother 2005;39(11):1817–22
Austin Z, Dolovich L, Lau E, Tabak D, Sellors C, Marini A, et al. Teaching and assessing primary care skills: the family practice simulator model. Am J Pharm Educ 2005;69:500–7
Kurtz SM, Laidlaw T, Makoul G, Schnabl G. Medical education initiatives in communication skills. Cancer Prev Control 1999;3(1):37–45
Colliver JA, Swartz MH, Robbs RS, Cohen DS. Relationship between clinical competence and interpersonal and communication skills in standardized-patient assessment. Acad Med 1999;74(3):271–4
Roter DL, Hall JA, Kern DE, Barker LR, Cole KA, Roca RP. Improving physicians’ interviewing skills and reducing patients’ emotional distress. A randomized clinical trial. Arch Intern Med 1995;155(17):1877–84
Simpson M, Buckman R, Stewart M, Maguire P, Lipkin M, Novack D, et al. Doctor-patient communication: the Toronto consensus statement. BMJ 1991;303(6814):1385–7
Charles C, Gafni A, Whelan T. Shared decision making in the medical encounter: what does it mean? (or it takes at least two to tango?). Soc Sci Med 1997;44:681–92
Davis D, Thomson O’Brien MA, Freemantle N, Mazmanian P, Taylor-Vaisey A. Impact of Formal Continuing Medical Education. Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health outcomes? JAMA 1999;282:867–74
Davis DA, Taylor-Vaisey A. Translating guidelines into practice: a systematic review of theoretical concepts, practical experience and research evidence in the adoption of clinical practice guidelines. CMAJ 1997;157:408–16
Clark N, Gong M, Schork A, Evans D, Roloff D, Hurwitz M, et al. Impact of education for physicians on patient outcomes. Pediatrics 1998;101(5):831–6
Stalsby-Lundborg C, Wahlstrom R, Oke T, Tomson G, Diwan V. Influencing prescribing for urinary tract infections and asthma in primary care in Sweden: a randomized controlled trial of an interactive educational intervention. J Clin Epidemiol 1999;52(8):801–12
Kimberlin CL, Bernardo DH, Pendergast JF, McKenzie LC. Effects of an educational program for community pharmacists on detecting drug-related problems in elderly patients. Med Care 1993;31:451–68
Currie JD, Chrischilles EA, Kuehl AK, Buser RA. Effect of a training program on community pharmacists’ detection of and intervention in drug-related problems. J Am Pharm Assoc 1997;NS37:182–91
Mayer JA, Eckhardt L, Stepanski BM, Sallis JF, Elder JP, Slymen DJ, et al. Promoting skin cancer prevention counseling by pharmacists. Am J Public Health 1998;88:1096–9
Schulz M, Verheyen F, Muhlig S, Muller JM, Muhlbauer K, Knop-Schneickert E, et al. Pharmaceutical care services for asthma patients: a controlled intervention study. J Clin Pharmacol 2001;41(6):668–76
Acknowledgments
This study was supported by an unrestricted educational grant from Merck Frosst Canada Inc., and in-kind contribution from Agro Health Associates Inc., and the Centre for Evaluation of Medicines. Conflict of interests: No conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Appendix 1: Example outcome assessment criteria
Appendix 1: Example outcome assessment criteria
Asthma-related problem (case 1, problem 1): The patient is experiencing uncontrolled asthma because she is not using her inhaled corticosteroid (she stopped due to a fear of steroid-induced osteoporosis).
Outcome assessment key: under-use of inhaled corticosteroid
-
a.
optimal plan
-
patient to start using ICS as prescribed and
-
patient to minimize risk of osteoporosis by addressing one or more of the following lifestyle issues: ensuring adequate calcium intake, reducing caffeine intake, following an appropriate exercise routine and
-
one (or more) of following:
-
patient to start monitoring symptoms into symptom diary to reinforce positive benefit of ICS therapy or
-
pharmacist will call MD to inform of intervention or
-
pharmacist will follow-up with patient to monitor progress by a specified time period
-
-
b.
Acceptable plan
-
patient to start using ICS as prescribed
-
c.
Unacceptable plan
-
patient to discuss concerns with MD or
-
ICS prescription put ‘on hold’ or
-
Issue not discussed at all
Asthma-related problem (case 2, problem 1): The patient is experiencing uncontrolled asthma because he has re-started smoking.
Outcome assessment key: smoking trigger
-
a.
Optimal plan
-
patient to consider quitting smoking in the near future and
-
one of the following:
-
pharmacist to follow up in weeks-months to re-introduce idea of smoking cessation or
-
pharmacist to begin discussion on options for smoking cessation
-
-
b.
Acceptable plan
-
patient to consider quitting smoking in the near future
-
c.
Unacceptable plan
-
no plan or recommendation or
-
issue not discussed at all
Rights and permissions
About this article
Cite this article
Dolovich, L., Sabharwal, M., Agro, K. et al. The effect of pharmacist education on asthma treatment plans for simulated patients. Pharm World Sci 29, 228–239 (2007). https://doi.org/10.1007/s11096-006-9080-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-006-9080-0