
Purpose
The purpose of the present study was to explore the involvement of indoxyl sulfate (IS) in nephrotoxicity and central nervous system (CNS) toxicity in cisplatin (CDDP)-treated rats.
Materials and Methods
Renal function was evaluated by serum creatinine and BUN levels. The IS levels in the serum, brain and kidney was monitored by high-performance liquid chromatography method. Body weight and rectal temperature were monitored. Real-time PCR analysis was performed to examine rPer2 mRNA expression.
Results
Renal function deteriorated in a time-dependent manner after administration of CDDP. The concentration of IS in the serum, brain and kidney markedly increased 24–84 h after commencement of CDDP treatment. The observed increase in the levels of serum creatinine, BUN and IS was suppressed by concomitant administration of AST-120. Rectal temperature was significantly lowered 72–92 h after CDDP-treatment, which was partially restored by coadministration of AST-120. Moreover, the amplitude of rectal temperature rhythms was disrupted by treatment with CDDP. Circadian rhythm of rPer2 mRNA expression, a clock gene, in suprachiasmatic nucleus (SCN) and kidney was disturbed in CDDP-treated rats.
Conclusions
An increase in the IS level and the associated disturbance to the circadian rhythm are involved in the renal and CNS toxicities in CDDP-treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Cisplatin (CDDP) is one of the most effective chemotherapeutic agents used in the treatment of human solid tumors. However, dose-related nephrotoxicity frequently limits the use of CDDP at optimal doses (1). The primary targets of CDDP-induced injury in the kidney appear to be the proximal straight and distal convoluted tubules (2), where the drug accumulates and causes cellular damage by multiple mechanisms including transient oxidative stress, DNA damage, apoptosis and inflammation (3,4).
Indoxyl sulfate (IS) is one of the uremic toxins that circulate at elevated concentration in the serum of patients with uremia. Because IS is mainly excreted via the kidney, the toxin cannot be efficiently removed from uremic patients with renal failure (5). IS is synthesized in the liver from indole, which is produced from tryptophan by intestinal flora (6,7). Increased serum levels of uremic toxins accelerate the deterioration of renal function in patients with chronic renal failure (CRF) (8). Administration of AST-120, an oral adsorbent consisting of porous spherical particles of carbon, lowers the serum and urinary concentration of IS by adsorbing indole in the gastrointestinal tract (9). Miyazaki et al. proposed that the progression of renal dysfunction might be associated with the expression of a few specific genes, such as transforming growth factor-β1 (TGF-β1), tissue inhibitor of metalloproteinase-1 (TIMP-1) and pro-α1(I) collagen in the kidney (8). Intriguingly, the expression of these genes is suppressed by administration of AST-120 (10). IS is also reported to induce the production of free-radicals and activate NF-κB up-regulating plasminogen activator inhibitor-1 (PAI-1) expression in renal tubular cells (11). These findings suggest that increased concentration of uremic toxins in the renal tubules exacerbates the further deterioration of renal function (5). Although many studies have been carried out to investigate the role of uremic toxins on CRF, the pathological and physiological role of uremic toxins in acute renal failure (ARF) has never been established.
Most mammals have a circadian rhythm, which is controlled by a circadian clock. In human, sleep–wake, hormonal secretion (12) and autonomic cycle, such as body temperature, blood pressure and peak flow (13,14), are regulated by the circadian rhythm, which is synchronized by environmental time cues, especially light (15). In the rodent brain, the center of the circadian clock is located principally in the suprachiasmatic nucleus (SCN) of the hypothalamus, and oscillates in a self-sustained manner (16). Recently, structural homologues of the Drosophila clock gene period (dPer), Period (PER) 1–3, have been identified in mammals (17). The mammalian clock genes appear to regulate circadian expression not only in the SCN but also in other peripheral tissues (18). Dissociation and slow resynchronization of clock genes between the SCN and other peripheral oscillators is thought to be responsible for physiological symptoms such as sleep disorder, headache and fatigue (19,20).
In general, renal failure causes multiple physiological changes involving central nervous system (CNS) dysfunction, such as uremic encephalopathy, which is associated with problems of cognition and memory, with progression to delirium, convulsions and coma (21). Although the distribution of CDDP in tissue is mainly confined to the kidney rather than the brain (22), many cases of CDDP-induced CNS toxicity have been reported. The main symptoms are fatigue, visual disturbance, seizure, headache, changes in mental status and anxiety (23,24). The mechanism of CDDP-induced CNS toxicity and its relationship with nephrotoxicity remain poorly understood.
The purpose of the present study was to examine the effect of CDDP-induced ARF on physiological function, particularly renal and CNS functions. We found that the concentration of IS markedly increased in the serum, brain and kidney of CDDP-treated rats, thereby accelerating renal and CNS toxicities. In addition, the circadian rhythm of rPer2 mRNA expression in the brain and kidney were disrupted in rats treated with CDDP. The CDDP-induced toxicities was partially inhibited by concomitant administration of a uremic toxin adsorbent agent, AST-120.
MATERIALS AND METHODS
Materials
CDDP was kindly donated by Nihonkayaku (Tokyo, Japan). AST-120 was kindly donated by Daiichi Sankyo Co., LTD., (Tokyo, Japan). IS was obtained from Sigma-Aldrich (St Louis, MO). All other chemicals were of analytical grade and commercially available.
Experimental Animals
Studies were performed using male Sprague-Dawley rats initially weighing 90–120 g (Kyudo Co., LTD., Fukuoka, Japan). The rats were housed in a standard animal maintenance facility at constant temperature (21–23C°), humidity (50–70%) with 12 h light/dark cycles (ZT, zeitgeber time; ZT0, light on; ZT12, light off) for at least 1 week before the day of the experiment. A lubricated thermocouple was inserted 2 cm into the rectum of rats and the rectal temperature was determined using a digital thermometer (Digital thermometer KN-91, Natsume, Tokyo, Japan). The research adhered to the provisions of “Principles of Laboratory Animal Care” (NIH Publication #85-23, revised in 1985).
CDDP-induced Acute Renal Failure
Rats were divided into three different groups as follows: saline-treated control rats, CDDP-treated with 10 mg/kg rats, coadministration of CDDP 10 mg/kg and AST-120 rats. Rats were treated with saline or CDDP (10 mg/kg dose) intraperitoneally at ZT14. AST-120 was administrated at ZT14 daily for 3 days. AST-120 was suspended in water and administrated (5 g/kg) 30 min before CDDP injection. To ascertain whether CDDP altered the body weight or circadian rhythm of rectal temperature and rPer2 mRNA expression in SCN and whole kidney, each parameter was determined at ZT2, ZT6, ZT10, ZT14, ZT18 and ZT22 on days 1 and 3 after initiation of drug treatment. Serum and tissue samples were collected under pentobarbital anesthesia (50 mg/kg). For the measurement of blood urea nitrogen (BUN) and serum creatinine (SCr), serum samples were collected at ZT2 and ZT14 of day 1 and day 3 after initiation of drug treatment. For the measurement of IS concentration, serum and tissue samples were collected at ZT2 and ZT14. A sample (0.5 g) of each tissue was homogenized in 5 mL of 1 M KH2PO4. A 50 μL aliquot of this solution was added directly to 100 μL of methanol. After centrifugation at 3,000 × g for 10 min, the supernatant was assayed by HPLC.
HPLC Conditions
The HPLC system consisted of a Shimadzu LC-10ADVP pump (Shimadzu, Kyoto, Japan) and a Shimadzu RF-10AXL fluorescence spectrophotometer. A column of LiChrosorb RP-18 (Cica Merck, Tokyo, Japan) was used as the stationary phase. The mobile phase consisted of acetate buffer (0.2 M, pH 4.5). The flow rate was 1.0 mL/min. IS was detected by means of a fluorescence monitor: excitation at 280 nm, emission at 375 nm.
mRNA Isolation and cDNA Synthesis
The brain and whole kidney were quickly dissected at ZT2, ZT6, ZT10, ZT14, ZT18 and ZT22 on days 1 and 3 after initiation of drug treatment. Coronal hypothalamic slices (500 μm) were prepared through the SCN using rodent brain matrix (RBS-A1-C, Muromachi, Tokyo, Japan). The SCN was punched out bilaterally from hypothalamic slices. For mRNA extraction, the MagNA Pure LC mRNA Isolation Kit II (Roche Diagnostics, Basel, Switzerland) was used. In this automated process, the tissue samples were lysed in a buffer containing a chaotropic salt and an RNase inactivator. The samples were homogenized with Lysing Matrix D (Qbiogene Inc., Carlsbad, CA) and FastPrep (Qbiogene Inc.) at an oscillation speed of 4.5 for 30 s. The 3′-poly (A+) from the released mRNA was hybridized to the added biotin-labeled oligo (dT). This complex was immobilized onto the surface of streptavidin-coated magnetic beads. After a DNase digestion step, unbound material was removed by several washing steps. Purified mRNA was then eluted (elution volume, 50 μL) with a low-salt buffer. cDNA was synthesized using a High-Capacity cDNA Archive Kit (Applied Biosystems Inc., Foster City, CA). Briefly, 50 μL of mRNA substrate, 10 μL of RT buffer, 4 μL of dNTP mixture, 10 μL of RT random primers, 5 μL of MultiScribe reverse transcriptase, and 21 μL of nuclease-free water were used for cDNA synthesis. After each reverse transcription, cDNA was stored −30°C.
Real-time PCR Analysis
We performed TaqMan quantitative real-time RT-PCR using an ABI PRISM 7900 sequence detection system (Applied Biosystems Inc.) to determine the expression level of rPer2. Eukaryotic 18S ribosomal RNA (18S rRNA) was used as an internal standard. TaqMan 18S rRNA control reagents, primer sets and Assays-on-Demand Product for rPer2 were purchased from Applied Biosystems Inc. as follows: 18S rRNA, 4319413E; rPer2, Rn00581577_m1.
Statistical Analysis
Data were analyzed statistically by analysis of variance (ANOVA). A P-value of less than 0.05 was considered statistically significant.
RESULTS
Body Weight, BUN and SCr Changes in Rats Treated with Saline or CDDP
Body weight changes in rats treated with saline or CDDP (10 mg/kg) are shown in Fig. 1A. The body weight of each rat at the initial treatment period (0 hour) was adjusted to 1.0. The body weight of rats treated with CDDP decreased to 0.86 at 96 h. Figure 1B and C show BUN and SCr changes in rats after treatment with saline or CDDP. Both BUN and SCr levels of rats treated with CDDP markedly increased in a time-dependent fashion from 72 h after treatment with CDDP, but not with saline.

Body weight (A), BUN (B) and SCr (C) changes in rats treated with saline or CDDP. Rats were treated with saline (open circles) or CDDP 10 mg/kg (solid squares). Body weight observed in each rat at the initial treatment hour (0 h) was adjusted to 1.0. BUN and SCr change in rats after treatment with saline (white bars) or CDDP 10 mg/kg (black bars). Data are expressed as means ± SE (N = 6−8). ***P < 0.001; **P < 0.01, significant difference between rats treated with saline or CDDP.
Endogenous IS Concentration in Rats Treated with CDDP
Endogenous IS concentrations in serum, brain and kidney treated with CDDP are shown in Fig. 2. IS level in the kidney of CDDP-treated rats was elevated significantly after 24 h of the treatment, and further increased in a time-dependent manner. The significant increase in serum was observed after 72 h after the CDDP treatment. The IS level in the brain was significantly elevated after 84 h of the treatment. Thereafter, the level of IS in CDDP-treated rats increased markedly in a time-dependent manner. Specifically, the endogenous IS level in serum, brain and kidney increased by 28-, 4.0- and 6.2-fold at 84 h, respectively.

Endogenous IS concentration changes in rats treated with CDDP. HPLC analysis of endogenous IS in the serum (A), brain (B) and whole kidney (C) of rats treated with CDDP 10 mg/kg. Data are expressed as means ± SE (N = 5−7). ***P < 0.001; **P < 0.01; *P < 0.05, significant difference from rats at initial trearment hour (0 h).
Effect of Coadministration of AST-120 on Body Weight, BUN, SCr and Endogenous IS levels in Rats Treated with CDDP
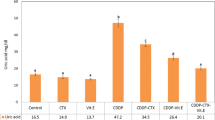
Figure 3 shows the effect of coadministration of AST-120 on body weight, BUN, SCr and IS concentration in the serum, brain and kidney of rats at 96 h after treatment with CDDP. The body weight of each rat at the initial treatment hour (0 hour) was adjusted to 1.0. There was no significant difference in body weight between the CDDP-treated rats and the CDDP- and AST-120-treated rats at time 0. At 96 h after treatment with CDDP, the level of BUN, SCr and IS in serum, brain and kidney was markedly elevated compared with those of the saline-treated rats. The coadministration of CDDP and AST-120 resulted in a lower level of BUN and SCr compared to the rats treated with CDDP alone. In addition, IS levels in the serum, brain and kidney of the CDDP- and AST-120-treated rats were significantly lower compared with those of the CDDP-treated rats.

Effect of coadministration of AST-120 and CDDP on body weight (A), BUN (B), SCr (C) and endogenous IS in serum (D), brain (E) and kidney (F) in rats. Body weight changes in rats after treatment with saline (open circles), CDDP 10 mg/kg (solid squares) or coadministration of AST-120 and CDDP 10 mg/kg (open squares). Body weight observed in each rat at the initial treatment hour (0 h) was adjusted to 1.0. BUN and SCr were measured at 96 h after treatment with saline (open bar), CDDP 10 mg/kg (solid bar) or coadministration of AST-120 and CDDP 10 mg/kg (shaded bar). Data are expressed as means ± SE (N = 6−7). **P < 0.01, compared with the each value (Scheffes’s F test). Endogenous IS in serum, brain and kidney were measured at 96 h after treatment with saline (open bar), CDDP 10 mg/kg (solid bar) or coadministration of AST-120 and CDDP 10 mg/kg (shaded bar). Data are expressed as means ± SE (N = 7). **P < 0.01; *P < 0.05, compared with the each value (Bonferroni F test).
Changes in Circadian Rhythms of Rectal Temperature after Treatment with CDDP or Coadministration of AST-120
To examine the influence of treatment with CDDP or coadministration of CDDP and AST-120 on circadian rhythms of rectal temperature, rats were housed in a light-controlled room (ZT, zeitgeber time; ZT0, light on; ZT12, light off). Figure 4 shows circadian rhythms of rectal temperature at 24–44 h (Fig. 4A) and 72–92 h (Fig. 4B) after treatment with saline, CDDP or the coadministration of CDDP and AST-120. The saline-treated rats showed a robust circadian rhythm with lower temperature during the light phase and higher temperature during the dark phase. The mean level of rectal temperature was highest at ZT18 and lowest at ZT6. Rats treated with CDDP or coadministered with CDDP and AST-120 showed a decreased amplitude of rectal temperature rhythm (P = 0.087 and P = 0.096, respectively). Furthermore, the CDDP and CDDP/AST-120 group of rats displayed a lowered rectal temperature at 24–44 h after initiation drug treatment. In the CDDP-treated rats, rectal temperature rhythm was disrupted (P = 0.78) and significantly lower at 72–92 h. However, rats treated with CDDP and AST-120 showed only a slight decrease in rectal temperature at 72–92 h, although the rectal temperature rhythm was still disrupted (P = 0.97).

Circadian rhythms of rectal temperature in each rat at 24–44 h (A) and 72–92 h (B) after treatment with saline, CDDP or coadministration of AST-120 and CDDP. Rectal temperature in each rat at 24–44 h and 72–92 h after treatment with saline (open circles), CDDP (solid squares) or coadministration of AST-120 and CDDP (open squares). The rats were housed under 12-h light/12-h dark. ZT0 is light on and ZT12 is light off. The open bars indicate the light-on phase, and the solid bars indicate the light-off phase. Data are expressed as means ± SE (N = 4−7). Rectal temperature following treatment with saline after 24–44 h and 72–92 h shows significant 24-h rhythms (P < 0.01, respectively, ANOVA). **P < 0.01; *P < 0.05, significant difference between rats treated with CDDP or coadministration of AST-120 and CDDP (Bonferroni F test).
Altered Circadian Rhythms of rPer2 mRNA Expression in SCN and Kidney after Treatment with CDDP or Coadministration of CDDP and AST-120
Real-time PCR analysis of rPer2 expression was carried out to examine the influence of treatment with CDDP, or coadministration of CDDP and AST-120, on circadian rhythm of rPer2 mRNA expression in the SCN (Figure 5A and B) and kidney (Fig. 5C and D). Analysis was performed at 24–44 h (Fig. 5A and C) and 72–92 h (Fig. 5B and D) after the start of drug treatment. In saline-treated rats, rPer2 mRNA expression exhibited robust circadian rhythm in both the SCN and kidney, showing normal circadian rhythm with lower levels during the light phase and higher levels during the dark phase. At 24–44 and 72–92 h after treatment with saline, the rPer2 mRNA level in the SCN was highest at ZT14 and lowest at ZT2, whereas rPer2 mRNA level in kidney was highest at ZT14 and lowest at ZT6. At 24–44 and 72–92 h after treatment with CDDP, rPer2 mRNA in the SCN and kidney exhibited circadian rhythm, but with a synchronized gap of circadian rhythm phase compared with saline-treated rats. At 24–44 h after treatment with CDDP, the rPer2 mRNA level in the SCN was highest at ZT10 and lowest at ZT18, whereas the rPer2 mRNA level in the kidney was highest at ZT18 and lowest at ZT2. At 72–92 h after treatment with CDDP, the rPer2 mRNA level in the SCN was highest at ZT10 and lowest at ZT6, whereas in the kidney the rPer2 mRNA level was highest at ZT10 and lowest at ZT2. Furthermore, at 24–44 and 72–92 h after the coadministration of CDDP and AST-120, rPer2 mRNA in the SCN exhibited no circadian rhythm (P = 0.12 and P = 0.52, respectively), whereas rPer2 mRNA in the kidney did show circadian rhythm (P < 0.01, P < 0.01, respectively). At 24–44 after coadministration of CDDP and AST-120, rPer2 mRNA level in the kidney was highest at ZT18 and lowest at ZT6. However, at 72–92 h after coadministration of CDDP and AST-120, the rPer2 mRNA level in the kidney was highest at ZT14 and lowest at ZT22. Notably, at 72–92 h after treatment with CDDP or coadministration of CDDP and AST-120, the rhythm of rPer2 mRNA expression in kidney was disturbed and decreased compared with control rats.

Circadian rhythms of rPer 2 mRNA expression in the SCN (A, B) and the kidney (C, D) at 24–44 (A, C) and 72–92 h (B, D) after treatment with saline, CDDP or coadministration of AST-120 and CDDP. Real-time PCR analysis of rPer2 in the SCN and the kidney were measured at 24–44 and 72–92 h after treatment with saline (open circles), CDDP (solid squares) or coadministration of AST-120 and CDDP (open squares). The peak value observed in saline-treated rats were adjusted to 1.0 after normalization with 18s rRNA. The rats were housed under 12-h light/12-h dark. ZT0 is light on and ZT12 is light off. The open bars indicate the light-on phase, and the solid bars indicate the light-off phase. Data are expressed as means ± SE (N = 4−6). All groups except for coadministration of AST-120 and CDDP rats in the SCN show significant 24-h rhythms (P < 0.01, respectively, ANOVA). **P < 0.01; *P < 0.05, significant difference between rats treated with saline or CDDP. ## P < 0.01; # P < 0.05, significant difference between rats treated with saline or coadministration of AST-120 and CDDP (Bonferroni F test).
DISCUSSION
The present study has established that an increase in the endogenous concentration of IS in serum, brain and kidney of rats occurs after treatment with CDDP. Especially, the accumulation of IS in the kidney was observed in an early stage at 24 h after the CDDP treatment, followed by the increase of IS levels in serum and brain (Fig. 2). IS is thought to induce free radical production and activate NF-κB, which up-regulates plasminogen activator inhibitor-1 (PAI-1) expression in renal tubular cells (11). IS has also been recognized as a typical circulating uremic toxin that is involved in glomerular sclerosis and interstitial fibrosis (5,8,10). It is thought that IS is primarily eliminated from the serum into urine via the kidney by active tubular secretion. The renal uptake of IS is mediated by organic anion transporters expressed at the basolateral membranes of renal tubular cells (25). In particular, the renal uptake of uremic toxins, such as 3-carboxy-4-methyl-5-propyl-2-furanpropionate (CMPF) and hippuric acid including IS, was reported to be mediated by organic anion transporters, OAT1 and/or OAT3 (26). Therefore, the renal excretion of a particular uremic toxin could be limited by competitive inhibition of the transporters by other uremic toxins. In addition to direct inhibition of renal uptake of uremic toxins via OATs, previous studies revealed that renal OAT1 expression was down-regulated in 5/6 nephrectomized rats as a model of CRF (27). As a consequence, the accumulation of these uremic toxins in the body could lead to the further progression of renal dysfunction in CRF (28). These findings suggest that during ARF, saturation of OAT-mediated excretion of the uremic toxins and down-regulation of the transporters might cause an increase in the systemic level of IS. In addition, AST-120 is considered to exert its effects on the progression of CRF by removing IS or their precursors in the digestive tract (10). In this study, we found that the coadministration of CDDP and AST-120 resulted in a lower serum level of BUN and SCr as well as IS compared with the CDDP-treated rats (Fig. 3). Furthermore, the IS level in brain and kidney of the CDDP-AST-120 group of rats was significantly lower compared with the CDDP-treated rats. The lower concentration of IS in the kidney correlates with the decreased incidence of ARF.
Thermoregulation is orchestrated by the preoptic area of the brain (29). In order to maintain a strict control of body temperature, the thermoregulatory center needs to receive prompt and accurate information from thermoreceptors in the body. In rodents, body temperature varies according to the circadian rhythm and is regulated by the autonomic nervous system (15). The present study shows that CDDP-treated rats have a significantly lower rectal temperature and that these changes are time-dependent (Fig. 4). Simultaneously, the IS level in the brain increased in a time-dependent manner (Fig. 2B). In particular, at 72 h after the initiation of treatment with CDDP, rectal temperature was significantly depressed compared with the saline-treated control rats. The frequency of food and water intake by the CDDP-treated rats was reduced in comparison with the control group (data not shown). However, the decrease in rectal temperature in the CDDP-induced rats at 72–84 h was eliminated significantly by coadministration of AST-120. The coadministration of AST-120 did not affect the observed changes in body weight and eating/drinking behavior of the rats, compared with the CDDP-treated rats (data not shown). It seems that the change in body weight caused by CDDP-induced toxicity to digestive tract. Sato et al. reported that there was no difference in serum concentration and urinary excretion of CDDP during 72 hr period after the CDDP injection between the CDDP-treated and CDDP-AST-120-treated rats (30). Accordingly, coadministration of AST120 with CDDP could not affect the CDDP-induced toxicity to digestive tract. This could be a possible reason why the change in body weight caused by CDDP was not affected by the coadministration of AST-120 with CDDP (Fig. 3A). Therefore, an elevated level of IS together with decreased locomotor activity could explain, at least in part, the lower rectal temperature. A previous study reported that the accumulation of IS and a neurotransmitter metabolite in the brain caused CNS dysfunction in rats with CRF (31). In addition, it was reported that increases in uremic toxins cause hypothermia (32). Hence, the present results indicate that an increased IS level in the brain might disrupt thermoregulatory mechanisms and induce a decreased rectal temperature. Hypothermia causes several undesirable effects such as metabolic disturbance, arrhythmia, impaired cardiac function and coagulopathy (33). Moreover, induction of hypothermia can result in intestinal ischemic injury due to a reduction in intestinal blood flow (34). Therefore, AST-120 could prove to be effective in preventing the adverse reactions caused by CDDP.
In human, sleep–wake, hormonal secretion (12), blood pressure, peak flow (14) and the autonomic cycle, such as body temperature (13), have circadian rhythms that are synchronized with the 24 h of the day. These changes were reported to be regulated primarily by SCN (35). The present study reveals decreased amplitude of rectal temperature rhythm between 24–44 h after treatment with CDDP (Fig. 4A). However, the level of IS in the brain did not increase at 24 and 36 h after the CDDP treatment (Fig. 2B). In addition, the coadministration of CDDP and AST-120 had no effect on the disrupted circadian rhythm of rectal temperature. These results indicate that disrupted circadian rhythm occurs regardless of the increased concentration of IS in the brain. Therefore, we examined the clock gene regulation in the SCN and kidney to clarify the disruptive circadian rhythm of rectal temperature.
The biological and physiological rhythms are regulated primarily by clock genes in SCN and peripheral tissues (16,18). In general, expression of clock genes between SCN and peripheral tissue are synchronized by neurotransmitters or humoral signals (36,37). Among the clock genes, the role of Per2 on rhythm regulation has been well studied. It was reported that Per2 mutations exert effects on physiological rhythms, leading to arrhythmia and advance of the sleep–wake rhythm (38,39). A previous study also reported that rPer2 expression in SCN showed a peak at ZT14 and trough at ZT2 (40), comparable with the present findings (Fig. 5A and B). Notably, we found that the treatment of rats with CDDP, or coadministration of CDDP and AST-120, results in a gap of phase circadian rhythm of rPer2 mRNA expression in the SCN and kidney at 24–44 h after commencement of treatment. Moreover, we observed that the behavioral rhythms of food and water intake were disturbed (data not shown). As reported previously, the rhythmicity of locomotor activity was severely altered by the continuous administration of corticosterone or a time-restricting feeding schedule, whereas the rhythmic phase of clock genes in the SCN was unaffected (41). Thus, it does not seem plausible that altered locomotor activity, such as food and water intake, could result from changes in rPer2 expression in the SCN.
The present study shows that treatment with CDDP elevates the level of IS in the brain at 84 h, although a phase gap in the circadian rhythm of rPer2 mRNA expression was also observed at 24–44 h. Coadministraion of CDDP and AST-120 had no significant effect on the phase gap of rPer2 mRNA rhythm. There was no report that IS directly caused disturbance of the circadian rhythm and Per 2 gene expression. Thus, our results indicate that the phase gap of rPer2 mRNA might occur regardless of the increase of IS in brain. Studies into the distribution of CDDP have shown that the drug does not accumulate in the brain because it cannot efficiently penetrate the blood-brain barrier. Intriguingly, however, the level of CDDP is greatest in the kidney (22). Therefore, changes in the rPer2 mRNA rhythm in the SCN does not appear to be a direct effect caused by CDDP and/or an increased level of IS. In contrast, changes of rPer2 mRNA rhythm in the kidney could be due to a direct effect of CDDP. In the present study, we have found that a temporal relationships of serum and renal IS accumulation with renal toxicity (Figs. 1 and 2). In addition, a phase gap of rPer 2 mRNA rhythm was observed during 24–44 hr in the SCN as well as in the kidney in rats treated with CDDP (Fig. 5A and C). Furthermore, there are reports indicating that clock gene expressions are synchronized in SCN and peripheral organs mediated by neurotransmitters or humoral signals (36,37). As renal IS accumulation was elevated after 24 hr of CDDP injection, renal IS and/or renal dysfunctions, which was caused after 36 hr of the injection, might affect the renal clock gene expressions, followed by disturbances of rPer 2 gene rhythm in the SCN. Glucocorticoid and vasopressin were suggested to be possible endogeneous factors in the sympathetic control of circadian rhythm between SCN and peripheral organs (37). Precise feedback mechanism for synchronization between the SCN and kidney remain to be solved. The present findings suggest for the first time that IS is involved, at least in part, in the disturbances of circadian rhythm induced by CDDP-caused acute renal failure.
Many cases of CDDP-induced CNS toxicity have been reported despite the poor penetration/distribution of this drug in the brain. The primary symptoms are fatigue, visual disturbance, seizure, headache, changes in mental status and anxiety (23,24). The dissociation and slow resynchronization of clock genes between SCN and other peripheral oscillators might explain, at least in part, some of the physiological symptoms such as sleep disorder, headache and fatigue (19,20). Moreover, previous reports suggested that accumulation of uremic toxins and neurotransmitter metabolites in the brain affect CNS function (31).
In conclusion, after treating rats with CDDP we observed an increase of IS in the brain and dissociation of rPer2 mRNA rhythm between the SCN and kidney. These findings suggest that some symptoms of CDDP-induced CNS toxicity, such as fatigue, are caused by an increase in the IS level in the brain and the concomitant dissociation of rhythmicity regulation of clock genes between the SCN and kidney.
Abbreviations
- IS:
-
indoxyl sulfate
- ARF:
-
acute renal failure
- CRF:
-
chronic renal failure
- SCN:
-
suprachiasmatic nucleus
- CNS:
-
central nervous system
- ZT:
-
zeitgeber time
- Per2 :
-
period 2
- SCr:
-
serum creatinine
References
F. Ries and J. Klastersky. Nephrotoxicity induced by cancer chemotherapy with special emphasis on cisplatin toxicity. Am. J. Kidney Dis. 8:368–379 (1986).
J. Deng, Y. Kohda, H. Chiao, Y. Wang, X. Hu, S. M. Hewitt, T. Miyaji, P. McLeroy, B. Nibhanupudy, S. Li, and R. A. Star. Interleukin-10 inhibits ischemic and cisplatin-induced acute renal injury. Kidney Int. 60:2118–2128 (2001).
G. Ramesh, and W. B. Reeves. TNF-alpha mediates chemokine and cytokine expression and renal injury in cisplatin nephrotoxicity. J. Clin. Invest. 110:835–842 (2002).
W. Lieberthal, V. Triaca, and J. Levine. Mechanisms of death induced by cisplatin in proximal tubular epithelial cells: apoptosis vs. necrosis. Adv. Physiol. Educ. 270:700–708 (1996).
T. Niwa, and M. Ise. Indoxyl sulfate, a circulating uremic toxin, stimulates the progression of glomerular sclerosis. J. Lab. Clin. Med. 124:96–104 (1994).
D. H. Bueschkens, and M. E. Stiles. Escherichia coli variants for gas and indole production at elevated incubation temperatures. Appl. Environ. Microbiol. 48:601–605 (1984).
E. Banoglu, G. G. Jha, and R. S. King. Hepatic microsomal metabolism of indole to indoxyl, a precursor of indoxyl sulfate. Eur. J. Drug Metab. Pharmacokinet. 26:235–240 (2001).
T. Miyazaki, M. Ise, H. Seo, and T., Niwa. Indoxyl sulfate increases the gene expression of TGF-beta 1, TIMP-1 and pro-α1(É) collagen in uremic rat kidneys. Kidney Inter., Suppl. 62:S15–S22 (1997).
T. Niwa, T. Nomura, S. Sugiyama, T. Miyazaki, S. Tsukushi, and S. Tsutsui. The protein metabolite hypothesis, a model for the progression of renal failure: an oral adsorbent lowers indoxyl sulfate levels in undialyzed uremic patients. Kidney Inter., Suppl. 62:S23–S28 (1997).
T. Miyazaki, I. Aoyama, M. Ise, H. Seo, and T. Niwa. An oral sorbent reduces overload of indoxyl sulphate and gene expression of TGF-β1 in uremic rat kidneys. Nephrol. Dial. Transplant. 15:1773–1781 (2000).
M. Motojima, A. Hosokawa, H. Yamato, T. Muraki, and T. Yoshioka. Uremic toxins of organic anion up-regulate PAI-1 expression by induction of NF-κB and free radical in proximal tubular cells. Kidney Int. 63:1671–1680 (2003).
A. van Coevorden, J. Mockel, E. Laurent, M. Kerkhofs, M. L’Hermite-Baleriaux, C. Decoster, P. Neve, and E. van Cauter. Neuroendocrine rhythms and sleep in aging men. Am. J. Physiol. 260:E651–E661 (1991).
D. Gupta, A. N. Aggarwal, S. Chaganti, and S. K. Jindal. Reducing the number of daily measurements results in poor estimation of diurnal variation of peak expiratory flow in healthy individuals. J. Postgrad. Med. 46:262–264 (2000).
A. M. Richards, M. G. Nicholls, E. A. Espiner, H. Ikram, M. Cullens, and D. Hinton. Diurnal patterns of blood pressure, heart rate and vasoactive hormones in normal man. Clin. Exp. Hypertens., Part A Theory Pract. 8:153–166 (1986).
W. E. Scales, A. J. Vander, M. B. Brown, and M. J. Kluger. Human circadian rhythms in temperature, trace metal, and blood variables. J. Appl. Physiol. 65:1840–1846 (1988).
M. H. Hastings. Central clocking. Trends Neurosci. 20:459–464 (1997).
H. Tei, H. Okamura, Y. Shigeyoshi, C. Fukuhara, R. Ozawa, M. Hirose, and Y. Sakaki. Circadian oscillation of a mammalian homologue of the Drosophila period gene. Nature 389:512–516 (1997).
K. Kume, M. J. Zylka, S. Sriram, L. P. Shearman, D. R. Weaver, X. Jin, E. S. Maywood, M. H. Hastings, and S. M. Reppert. mCRY1 and mCRY2 are essential component of negative limb of the circadian clock feedback loop. Cell 98:193–205 (1999).
S. Yamazaki, R. Numano, M. Abe, A. Hida, R. Takahashi, M. Ueda, G. D. Block, Y. Sakaki, M. Menaker, and H. Tei. Resetting central and peripheral circadian oscillators in transgenic rats. Science 288:682–685 (2000).
A. B. Reddy, M. D. Field, E. S. Maywood, and M. H. Hastings. Differential resynchronization of circadian clock gene expression within the suprachiasmatic nuclei of mice subjected to experimental jet lag. J. Neurosci. 22:7326–7330 (2002).
A. C. Schoots, P. M. De Vries, R. Thiemann, W. A. Hazejager, S. L. Visser, and P. L. Oe. Biochemical and neurophysiological parameters in hemodialyzed patients with chronic renal failure. Clin. Chim. Acta 185:91–107 (1989).
C. L. Robert, P. S. Richard, and C. Harold. The antitumor agent cis-Pt (NH3)2Cl2: distribution studies and dose calculation for 192mPt and 195mPt. J. Nucl. Med. 14:191–195 (1972).
I. J. Berman, and M. P. Mann. Seizures and transient cortical blindness associated with cis-platinum (II) diamminedichloride (PPD) therapy in a 30-year-old man. Cancer 45:764–766 (1980).
C. Verschraegen, C. A. Conrad, and W. K. Hong. Subacute encephalopathic toxicity of cisplatin. Lung Cancer 13:305–309 (1995).
T. Deguchi, M. Nakamura, Y. Tsutsumi, A. Suenaga, and M. Otagiri. Pharmacokinetics and tissue distribution of uraemic indoxyl sulphate in rats. Biopharm. Drug Dispos. 24:345–355 (2003).
T. Deguchi, S. Ohtsuki, M. Otagiri, H. Takanaga, H. Asaba, S. Mori, and T. Terasaki. Major role of organic anion transporter 3 in the transport of indoxyl sulphate in the kidney. Kidney Int. 61:1760–1768 (2002).
I. Aoyama, A. Enomoto, and T. Niwa. Effects of oral adsorbent on gene expression profile in uremic rat kidney: cDNA array analysis. Am. J. Kidney Dis. 41:S8–S14 (2003).
M. Motojima, A. Hosokawa, H. Yamato, T. Muraki, and T. Yoshioka. Uraemic toxins induce proximal tubular injury via organic anion transporter 1-mediated uptake. Br. J. Pharmacol. 135:555–563 (2002).
J. A. Boulant. Hypothalamic mechanisms in thermoregulation. Fed. Proc. 40:2843–2850 (1981).
T. Sato, S. Miyazaki, and S. Mohri. Effects of an oral adsorbent on cisplatin-induced nephropathy in rats. Nippon Jinzo Gakkai Shi 38:290–295 (1996).
S. Ohtsuki, H. Asaba, H. Takanaga, T. Deguchi, K. Hosoya, M. Otagiri, and T. Terasaki. Role of blood-brain barrier organic anion teansporter 3 (OAT3) in the efflux of indoxyl sulfate, a uremic toxin: its involvement in neurotransmitter metabolite clearance from the brain. J. Neurochem. 83:57–66 (2002).
M. Hohenegger, H. Echsel, M. Vermes, and H. Raneburger. Influence of some uremic toxins on oxygen consumption of rats in vivo and in vitro. Adv. Exp. Med. Biol. 212:99–104 (1987).
D. I. Sessler. Mild perioperative hypothermia. N. Engl. J. Med. 336:1730–1737 (1997).
R. W. Powell, D. L. Dyess, J. N. Collins, W. S. Roberts, E. J. Tacchi, A. N. Swafford Jr, J. J. Ferrara, and J. L. Ardell. Regional blood flow response to hypothermia in premature, newborn, and neonatal piglets. J. Pediatr. Surg. 34:193–198 (1999).
N. F. Ruby, J. Dark, D. E. Burns, H. C. Heller, and I. Zucker. The suprachiasmatic nucleus is essential for circadian body temperature rhythms in hibernating ground squirrels. J. Neurosci. 22:357–364 (2002).
C. K. Song, and T. J. Bartness. CNS sympathetic outflow neurons to white fat that express MEL receptors may mediate seasonal adiposity. Am. J. Physiol., Regul. Integr. Comp. Physiol. 281:R666–R672 (2001).
R. M. Buijs, S. J. Chun, A. Niijima, H. J. Romijn, and K. Nagai. Parasympathetic and sympathetic control of the pancreas: a role for the suprachiasmatic nucleus and other hypothalamic centers that are involved in the regulation of food intake. J. Comp. Neurol. 431:405–423 (2001).
C. Kopp, U. Albrecht, B. Zheng, and I. Tobler. Homeostatic sleep regulation is preserved in mPer1 and mPer2 mutant mice. Eur. J. Neurosci. 16:1099–1106 (2002).
K. L. Toh, C. R. Jones, Y. He, E. J. Eide, W. A. Hinz, D. M. Virshup, L. J. Ptacek, and Y. H. Fu. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science 291:1040–1043 (2001).
K. Ohishi, K. Sakamoto, T. Okada, T. Nagase, and N. Ishida. Humoral signals mediate the circadian expression of rat period homologue (rPer2) mRNA in peripheral tissues. Neurosci. Lett. 256:117–119 (1998).
F. Damiola, N. Le Minh, N. Preitner, B. Kornmann, F. Fleury-Olela, and U. Schibler. Restricted feeding uncouples circadian oscillators in peripheral tissues from the central pacemaker in the suprachiasmatic nucleus. Genes Dev. 14:2950–2961 (2000).
Acknowledgments
This work was supported, in part, by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science, Sports, and Culture of Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
K.I. and H.W. contributed equally to this work.
Rights and permissions
About this article
Cite this article
Iwata, K., Watanabe, H., Morisaki, T. et al. Involvement of Indoxyl Sulfate in Renal and Central Nervous System Toxicities During Cisplatin-induced Acute Renal Failure. Pharm Res 24, 662–671 (2007). https://doi.org/10.1007/s11095-006-9183-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-006-9183-2