
Abstract
Abstract
Physicochemical and biopharmaceutical properties of drug substances and dosage forms can be highly affected by the particle size, a critical process parameter in pharmaceutical production. The fundamental issue with particle size analysis is the variety of equivalent particle diameters generated by different methods, which is largely ascribable to the particle shape and particle dispersion mechanism involved. Thus, to enable selection of the most appropriate or optimal sizing technique, cross-correlation between different techniques may be required. This review offers an in-depth discussion on particle size analysis pertaining to specific pharmaceutical applications and regulatory aspects, fundamental principles and terminology, instrumentation types, data presentation and interpretation, in-line and process analytical technology. For illustration purposes, special consideration is given to the analysis of aerosols using time-of-flight and cascade impactor measurements, which is supported by a computational analysis conducted for this review.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Particles of active and nonactive pharmaceutical ingredients exist in the majority of pharmaceutical products as dry powders, liquid and semisolid dispersions ranging from nanocolloids to millimeter-size granules, depending on the dosage form and route of administration (Fig. 1). The particle size and shape can influence a large variety of important physical properties, manufacturing processability and quality attributes, including:
-
Dissolution rate and bioavailability of active pharmaceutical ingredients.
-
Drug release rate for sustained and controlled release formulations.
-
In vivo particle distribution and deposition, absorption rate and clearance time, especially for aerosols and different colloid systems designed for targeted drug delivery.
-
Content and dose uniformity and other properties related to the physicochemical stability.
-
Aerosolization behaviour and performance of respiratory formulations.
-
Flow and packing properties, mixing and segregation of powders, rheological characteristics of liquid and semisolid formulations.
-
“Grittiness” of solid particles in chewable tablets, dermal ointments, creams, and irritability of ophthalmic preparations.

Particle size range for different dosage forms and routes of administration.
These properties ultimately affect the safety and efficacy of drugs. The emergence of a range of novel particle engineering technologies and the availability of new sophisticated characterization methods allow one to consider the “design by first intent” of particles with tailored physicochemical character and functionality. There is also recognition of the importance of the quality control, process consistency and economics even in more traditional manufacturing processes (2). The purpose of particle size analysis is to obtain quantitative data on the mean size, particle size distribution (PSD) and shape of the compounds to be used in pharmaceutical formulation. The particle size analysis is also required to assure the quality of the final dosage forms and drug delivery systems. In addition, there has been an increased interest in incorporating particle size instrumentation into the process monitoring and control including automated production units. However, the data inconsistency between different methods, or even between similar instruments of different manufacturer brands, make validation for the GLP and cGMP very difficult (2–5). In the AAPS workshop report on particle size analysis (2), it is emphasized that the diversity of particle treatments, methods of particle size analysis, expression and interpretation of data, and process applications results in complicated and sometimes confused criteria for selection, adoption, or relevance of the available techniques. There are fundamental methodological issues related to “what is being measured” but also challenges specific to the pharmaceutical analysis, as listed below:
-
Requirements for a new method development based on specific drug physical form and intended drug delivery application.
-
Limited sample quantities, especially in the early drug development stage.
-
Highly nonspherical shape of many pharmaceuticals leading to complex data interpretation.
-
Agglomeration, instability and other physical changes occurring during measurements.
-
Necessity of developing specialized methods for quality control, for example, in the areas of inhalable and parenteral products.
-
Challenges of online analysis as a part of the system for designing, analyzing, and controlling manufacturing processes (Process Analytical Technology, PAT).
-
Regulatory requirements.
The objectives of the present review are twofold. First, the methodologies of particle size analysis are discussed around the fundamental concept of equivalent particle diameter, taking into account the influence of particle shape and particle dispersion. The key questions here are common to a range of pharmaceuticals including dry powders, suspensions, aerosols, emulsions and nanoparticles. In parallel, the methodologies are reviewed for specific pharmaceutical applications. Illustrated by relevant examples from other fields, the emphasis is placed on dry powder inhalation formulations. This is one of the most difficult and controversial area of particle characterization which has a direct and obvious implication in the dosage form performance. It also serves well to illustrate the general methodological issues with particle size analysis.
Particle Size and Product Performance
Respiratory Drug Delivery
The performance of inhalation devices mainly depends on the geometric and aerodynamic PSD, particle shape and powder dispersion characteristics (4,6–10). There are three main aerosol deposition mechanisms for pulmonary delivery of drugs: inertial impaction, sedimentation and Brownian diffusion (11). In general, particles with mass–median aerodynamic diameter (MMAD) ranging from 1–5 μm, are deposited in the bronchial and alveolar regions predominantly by sedimentation, and have the best pulmonary penetration (4), and are within the optimum size range for most oral inhalation products (12). Yet, better understanding of the underlying pathophysiology in disease states can allow further fine-tuning of particle size for more efficient pulmonary drug delivery. For illustration purposes, let us consider the case of asthma, a common disease treated with two types of inhalational pharmacotherapeutic agents, i.e., brondilators (short-acting β agonists) and anti-inflammatory agents (steroidal compounds). In bronchodilatation therapy, it has been found that regional targeting of inhaled β2-agonist to the proximal airways is more important than distal alveolar deposition (13). It has been shown with micron particles of different sizes (1.5, 3 and 6 μm) that, although smaller particles have greater total lung deposition, farther distal airways penetration, and more peripheral deposition, larger particles are more efficacious and afford greater bronchodilatation (13), indicating that particles within the upper range of 1–5 μm are more desirable for bronchodilators. In contrast, distal lung diseases appear to increase the risk of recurrent asthma exacerbation, and inflammatory response in the distal lung can exceed that in the large airways (14). Extra-fine aerosols (MMAD: 1.1–2.1 μm) have better access to distal lung, with less oropharyngeal deposition, and most importantly, produce beneficial changes in distal lung function (14). The aforementioned findings suggest that inhalation steroidal compounds should be targeted on this distal airway region, and particles within the lower range of 1–5 μm are more desirable for anti-inflammation control. It should also be noted that while there are currently no DPI formulations with MMAD in the submicron range, almost all formulations have a submicron-size particle fraction. Such particles (<0.5 μm) are likely to be exhaled and this may represent a dosing problem.
The recent trend of systemic pulmonary drug delivery makes it very important to understand the correlation between the aerodynamic diameter, determined by in vitro measurements or in vivo lung deposition studies, and different geometric diameters measured by a variety of nonaerodynamic techniques. Advanced respiratory formulations may consist of porous or highly nonspherical microparticles or nanoparticles. The particle deposition, expressed in terms of the fine particle fraction (FPF), mainly depends on the aerodynamic PSD and MMAD, whereas the geometric (volume or surface-to-volume) PSD determine the interparticle interactions, emitted dose and dose uniformity, dissolution rate and particle uptake. For example, large porous particles containing therapeutic proteins have typical MMAD within 1.5–4.0 μm size range, with corresponding volume mean diameter, VMD, between 3–12 μm (15,16). These particles may show very high FPF reaching 65–95% and increased bioavailability due to increased dissolution rate and delayed natural phagocytic clearance (17). Similarly, porous PLGA particles loaded with a nonapeptide deslorelin were prepared with VMD about 13.8 μm and the bulk density <0.1 g/cm3 (18). Such large particles afforded sustained peptide release in rat lungs for over 7 days because of their reduced uptake into the respiratory epithelial cells when compared to solid PLGA particles with the same MMAD. Particle shape is also extremely important. For example, elongated crystals of cromoglycic acid and nedocromil sodium (19) or very thin plates of salmeterol xinafoate (7) had geometric dimensions between 2–5 μm but a significantly smaller MMAD (0.7–2 μm). The particle clearance rate is also shape-dependent, with elongated particles such as fibers being more difficult to remove from the lungs (20).
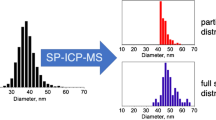
Nanoparticles hold promise in pulmonary delivery due to the homogeneity and increased efficiency of nanosuspensions. For example, nanosuspensions of budesonide (mean size 500 nm) showed a significant increase in FPF by 53–88% compared to microsuspensions (mean size 4 μm) (21). Nanoparticles of poorly water-soluble drugs have a higher overall dissolution rate and may have a very specific interaction route with both the trachea-bronchial and alveolar epithelium. Ultrafine nanoparticles (<150 nm) showed delayed lung clearance, increased interaction/binding with certain proteins and enhanced translocation from the epithelium into circulation and subsequent target organs (22).
A specific reference should be made to drug–lactose blend which is currently the most common type of dry powder inhalation (DPI) formulation. A small amount of lactose fine (<5–10 μm) particles is often incorporated to promote deaggregation in the turbulence created by inhalation. Increasing the amount of fine carrier particles in ternary interactive mixtures, up to a certain weight proportion, can improve the aerosol performance of dry powder inhalation formulations (23–26). Addition of fine particles to spray-dried or crystalline lactose 63–90 μm can also decrease specific charges (27), and the adhesion of lactose particle (4–15 μm) to gelatin capsules appears to be proportional to the particle size for homogeneous surfaces (28). Removal of such fine particles by wet decantation abolishes the dependence of particle dispersion on the volume mean diameter of the carriers (29). Thus it appears that the aerosol performance is associated with the presence of fine adhered particles among the carriers, but not the inherent particle size of carriers (29). The presence of fine lactose particles (VMD = 5.8 μm) can also facilitate physical disruption of the strong cohesive interaction between drug particles, such as nedocromil sodium trihydrate, by decreasing the number of drug–drug contacts and increasing the separation distance between the neighboring drug particles (30). Given the strong influence of lactose fines on the overall performance of dry powder inhalation formulations, it is suggested that during particle size analysis of carrier, the weight percentage of lactose fine (<10 μm) as well as common statistic parameters (e.g., d 10 , d 50 , d 90 , and etc.) should be monitored in the whole system.
The particle size requirements for nasal sprays are less stringent and less well established than those for pulmonary delivery (12). Classic literature suggests that the optimum particle size for deposition in the nasal cavity is 10 μm MMAD (31). The more acceptable particle size range is 4.8–23 μm (32). Nevertheless, a wide range of particle size distribution is possible for nasal delivery of pharmaceuticals documented in contemporary literature, ranging from nano-size (33) to 45 μm (34), or even up to 125 μm (35).
Oral Dosage Forms
Besides the pulmonary and nasal spray formulations, another well-documented example is the tablet dosage form. The particle size range for direct-compression tablets tends to be within the 100–200 μm range, mostly because of their required compaction behaviour and powder flow properties. However, smaller particle sizes of about 20–50 μm are likely to be optimal for chewable (taste-masked) and fast-disintegrating tablets, where the controlled dissolution and grinding-attrition characteristics become more important. The particle size has a profound influence on almost every step in tablet manufacturing, including mixing (36), granulation (37), compression (38), and coating (39). Particle shape has also been reported to affect mixing (36) and tabletting processes (40). Besides the manufacturability of tablets, the dissolution rate, which is proportional to surface area of drugs, is largely dependent on particle size distribution of drug particles (41). This is particularly important for drugs in Biopharmaceutical Classification System Class II (low solubility; high permeability) as the bioavailability is typically governed by drug dissolution in this category (42). To account for the effect of particle shape on dissolution rate, correctional factors may be introduced to consider the geometric and material influences (43). By manipulating particle size of both actives and/or excipients, dissolution rate can be enhanced via micronization and nano-sizing (44), or reduced via formulation into a controlled release preparation by direct compression with polymers, such as hydroxypropyl methylcellulose (45). However, care should be taken to ensure the increase of effective surface area in comminuted samples, as aggregate formation may negate the beneficial effects of micronized or nano-sized materials.
In addition to the standard tablets, the dissolution performance of matrix-type controlled release tablets is highly influenced by drug’s and/or excipient’s particle size. Drug percolation threshold, the critical porosity where the pore network just begins to span the whole matrix, is linearly correlated with drug particle size in matrix tablets (46). Dissolution data, such as critical time of kinetic change, are related to drug particle size (47), and excipient/drug particle size ratio (48). Extent of burst release can be modulated by controlling the particle size of sodium alginate via formation of an initial alginic acid gel barrier (49). Lag time in matrix tablet designed for colonic delivery can increase with decreasing the particle size of channeling agent (e.g., NaCl, Emdex®), as a consequence of the smaller pores formed by its dissolution (50). In addition to the dissolution profiles, crushing strengths of matrix tablets can also be affected by particle size (51).
Bioavailability enhancement for water-insoluble drugs in oral dosage forms may be achieved for drug nanoparticles, through their enhanced suspension homogeneity and delivery efficiency as well as increased residence time (reduced clearance). For oral bioavailability, a typical increase of AUC by a factor 2.5 was observed with reduction of particle size from 1,000 to 400 nm (52,53). The same study also reported a reduction of feeding/fasting effects by a factor of 3–4. Other advantages include enhanced dose proportionality and earlier onset of action. Nanoparticles were also shown to exhibit increased bioadhesion and/or increased uptake in the intestinal and inflamed colonic mucosa (52,53).
Ophthalmic, Topical and Transdermal Drug Delivery
The particle size of ophthalmic controlled-release formulations has proved to be very important in balancing between the drug release rate, bioavailability improvement, patient comfort and ease of use (54). When appropriately formulated for ophthalmic delivery, the particles are retained in the ocular cul-de-sac and the drug released at a rate that is neither too fast nor too slow to allow adequate drug penetration into ocular tissues. Nanoparticles (typically about 300 nm) without bioadhesion can be eliminated from the precorneal site almost as quickly as aqueous solutions. Microparticles (mean diameter 1–3 μm) may be better suited for controlled release, but the presence of coarse particle fraction above 25 μm makes them less tolerable and can cause irritation to the eye. One of the main challenges in developing such particulate systems is the manufacturing complexity and particle size control during large-scale manufacturing (54).
In topical and transdermal drug delivery, particle size is a crucial factor for some applications. If the drug is suspended in a vehicle, particle size may become a key regulator of flux (55). If the drug has a low solubility in the vehicle, decreasing the particle size can promote drug delivery by increasing dissolution rate of particles (55). Particle size also exerts a significant influence on cutaneous penetration pathways: particles greater than 10 μm remain on the skin surface; particles between 3–10 μm concentrate in the hair follicles; particles smaller than 3 μm may penetrate both the follicles and stratum corneum (56). For particles smaller than 3 μm, including nanoparticles for most cases, percutaneous absorption is mainly via the follicular route. Skin penetration of polymeric polystyrene nanoparticles (20 and 200 nm) is achieved by follicular localization, but there are no alternative nonfollicular penetration pathways (57). Similar results are obtained in minoxidil with block copolymer nanoparticles (40 nm and 130 nm) (58). Judicious choice of particle size in topical formulations not only can maximize local efficacy inside skin area but also can minimize potential systemic adverse reactions.
Parenteral Formulations
Since currently most parenteral formulations are solution-based products, particle size analysis is normally focused on the detection of particulate contamination (Table I), where the possible sources are foreign matters, drug precipitation or formulation incompatibility. Such particulate contamination can lead to vascular occlusion and pulmonary embolism and should be tightly controlled. For the same safety concern, particles of micron-size range (>1 μm) should be excluded from intravenous nanosuspension formulations. Moreover, increased particle size can decrease both injectability and syringeability. Clogging of the needle may occur due to blockage by a single particle or by bridging effect of multiple particles, and therefore, the individual particle size should be less than approximately one third of the needles’ internal diameter.
For parenteral suspensions, as the specific surface area is directly related to dissolution rate, particle size is important in determining in vivo drug release pattern. The applications of nanosuspensions are rapidly growing, in all areas of IV, IM, ID, SC and brain-intrathecal delivery. For example, for IV injection of anticancer agents, many of which are water-insoluble, nanosuspensions (99% cumulative PSD <1 μm size) become increasingly important for drug delivery. For fast pharmacokinetics, rapid plasma dissolution of nanoparticles provided tissue distribution equivalent to that for solution formulation as shown for flurbiprofen (20,53). On the other hand, enhanced ID depot delivery via slow dissolution could also be achieved and enhanced SC delivery (47%) was observed for nanosuspensions versus microsuspensions (20,53). Another example is the efficacy of nanoparticulate paclitaxel in MV-522 human lung xenograft murine tumor model (i.e., Taxol 30 mg/kg versus 90 mg/kg nanoparticulate suspensions) where the nanoformulation shows a multifold decrease in tumor weight versus the almost constant tumor weight observed for the taxol administration (20,53).
In the extensively investigated area of targeted delivery, mononuclear phagocytes, dendritic cells, endothelial cells, and cancers (tumor cells and tumor neovasculature) are all important targets for nanoparticles, with mean particles sizes often smaller than 100 nm. Here both the diagnostic and therapeutic potentials of nanomedicine are clearly evident (59). The size and size distribution of the nanoparticles have a key role in determining their fate and therapeutic effects following administration, and their interaction with the cell membrane and their penetration across the physiological drug barriers (60). Nanoparticles below approximately 150 nm diameter have a prolonged half-life in the systemic circulation due to a slower uptake by microphages. However the size is not the only factor affecting this uptake. For example, micron-long wormlike micelles (with 10–100 nm cross section) showed circulation times of several days (20,61). Compared to spherical liposomes, these polymersomes (composed of e.g., PEG-PLA and PEG-PCL) are more robust and capable of prolonged systemic circulation. Different in vivo studies show that these wormlike structures behave as nanoparticles to the cell and the body. This indicates that all particulate properties such as size, shape and surface characteristics need to be investigated in such formulations.
Although uniform size distribution may be preferred in many applications, a mixture of nanoparticles of different particle sizes can be used to incorporate the desired release kinetics in the design of chemotherapy to individualize therapy for patients (60). As nanotechnology becomes increasingly hyped in both public and scientific communities, concerns over its toxicity are also highlighted (62). Particle size dependent pathological change in lung has been reported in mice exposed with nano-sized colloidal silica (63). It has been recommended that size distribution and shape should be characterized for nanomaterials in routine toxicity screening tests (64). Therefore, particle size analysis of nanoparticles is not limited to quality and efficacy assessment, but also serves as an integral part in product safety control.
Regulatory Issues
It is clear that there is an increasing emphasis placed on particle size analysis in regulatory control. Although the general guidelines of the International Conference on Harmonization (ICH) are applicable in most countries, subtle differences in these guidelines specified by various national Pharmacopoeia still exist. Table I contains the reference sources of particle size analysis in different Pharmacopoeias and the ISO Standards for particle sizing that include the definitions as well as the technical characteristics and working principles of the most common particle sizing instruments. As shown in Table I, only a few particle sizing instruments are included in the Pharmacopoeial monographs. This, of course, does not preclude any other suitable particle characterization technique, provided that this can be justified by the application and rigorous data analysis. Factors such as speed, cost and computerization of particle size analysis in pharmaceutical industry lead to adaptation of several types of instruments which are able to measure the PSD of small samples in very short periods of time compared to classical Pharmacopoeial characterization techniques such as sieves and sedimentation rate based methods (Table I). As a general rule, the laboratory and process particle sizing instrumentation used in pharmaceutical industry complies with the data electronic format regulations, such as FDA 21 CFR Part 1 (65), allowing FDA to accept electronic records and signatures in place of paper records and handwritten signatures. This regulation describes controls to ensure that electronic records and signatures are trustworthy, reliable and compatible with FDA work.
The ICH Guidelines explicitly states that particle size is one of the physicochemical properties influencing the performance of the drug product and its manufacturability (http://www.ich.org). Further specifications are described in ICH Q6A acceptance criteria in new drug substances for solid or suspension drug products (Fig. 2). In oral and injectable suspensions for new drug products, particle size distribution may also be proposed in place of dissolution testing. Regarding particulate matters, parenteral products should have appropriate criteria, including maximum size of coarse particle fraction, clarity of solution, foreign particles, and visible and subvisible particulates. Foreign particulate matter in inhaled and nasal-spray drug products (OINDPs) is one of the active discussion topics between the Pharmaceutical Aerosol Consortium on Regulation and Science (IPAC-RS) and FDA. IPAC recommends full characterization including particle number, size range and identity during development, and particle counting during manufacture for market supply (66). FDA has issued several guidances for the industry related to particle size distributions in a variety of products, such as metered dose inhaler and dry powder inhaler drug products (67), and nasal spray and inhalation solution, suspension, and spray drug products (12), including bioequivalence assessment (68). In addition, preparation of a Common Technical Document for pharmaceutical registration purposes requires the following information sections for particle size analysis (69):
-
Description of manufacturing process and process controls.
-
Identification of the particle size distribution of the drug substance.
-
Specification, and its justification.
-
Analytical procedures, and their validation.
-
Results of batch analyses.
-
Identification of the influence of particle size on product performance.

Algorithm setting acceptance criteria for particle size distribution (according to the Q6A specific drug substance tests of the ICH).
In pulmonary delivery of pharmaceuticals, it is obvious that aerodynamic size distribution is the most important parameter affecting aerosol performance. However, it should be noted that in the FDA guidance document, acceptance criteria expressed in terms of MMAD and GSD alone (representing the measures of the central tendency and spread respectively) as well as in terms of respirable fraction or respirable dose are not considered adequate to characterize the particle size distribution of the whole dose (12,67). FDA recommends that the total mass of drug collected on all stages and accessories should be between 85 and 115% of label claim on a per actuation basis (67). Since the “inhalability” of formulations can also be adversely affected by particle size and shape changes associated with solid-state instability during storage (70), FDA recommends that relative humidity and temperature should be specified and controlled in the test procedure to minimize hygroscopic growth, aggregations of particles, and variability arising from these sources (67). Dose content uniformity tests for both pMDIs and DPIs specify that the amount of active ingredient per determination should be within ±20% of label claim for >90% samples, and ±25% of label claim for all samples, and the mean should be within ±15% of label claim (67). If the first tier of 10 containers fails, the second tier of 30 containers should match the specifications. Emitted particle size distribution for both pMDIs and DPIs should be determined by a multistage cascade impactor. The total mass of drug collected on all stages and accessories should be within ±15% of label claim on a per actuation basis, and that on each stage and each accessory should be reported (67). In addition, more stringent controls in DPIs exist. For instances, the particle size distribution of drug substance in device-metered DPIs should be established and monitored at the initial dose and the last dose of the labeled number of doses (67). The regulatory requirements in spray content uniformity of nasal sprays are relatively less stringent. Droplet and particle size distribution in nasal formulation are required in FDA guidance (12), although the particle size specifications here is less well established than that for pulmonary delivery.
Recommendations and guidelines related to particle size analysis are currently under development and likely to expand significantly in the future. One of the potential expansion areas is the inclusion of new monographs for instrumentation and methodology in the current Pharmacopoeias, for instance, the laser diffraction method and next generation cascade impactor, NGI (see Table I). Another important area is the coordination between regulatory requirements and industrial practice. For instance, there has been controversy with regard to the 85–115% drug mass balance collected on all the stages and accessories of the cascade impactor (67,68). The industry responded to this by forming several working groups and by proposing recommendations for changes (71,72). This led to the relaxation of the spray content uniformity requirement in nasal spray and inhalation solution, suspension and spray drug products (12). The AAPS in conjunction with the FDA and the USP organizes a series of particle size analysis workshops. These workshops plan to discuss the current issues with regard to particle standards, powder sampling, sample preparation, agglomeration, particle shape, validation method, and data interpretation (2).
Particle Size Measurements
General Methodology
Figure 3 illustrates the basic principle of particle size analysis. The sizing methods employed can be subdivided into two major categories: stream-scanning and field-scanning techniques. In the former the particles are examined or counted one at a time and then classified into corresponding size baskets, whereas in the latter, the whole particle assembly is measured simultaneously and the PSD is derived from this integral “field” response. Clearly both categories have their advantages and disadvantages. Due to the fact that the stream scanning provides an additional experimental parameter—the number of particles measured, it usually offers a better resolution, lower quantification limits and more convenient data interpretation (2,73). On the other hand, the field-scanning methods are usually faster, more robust and better suited for online/in-line applications.

Methodology of particle size analysis.
Particle Equivalent Diameter
The particle size, if defined as a “characteristic linear dimension”, is an ambiguous quantity for nonspherical particles. Moreover, with the exception of microscopy, the particle size cannot be measured directly. The data obtained are not a unique property of the particles but depend upon the physical response of the analytical instrument in relation to the size and the shape of the particles. Even for spherical particles, the physical differences, manifested by different equivalent diameters measured, can lead to some discrepancies, typically within 10% in terms of median diameter by volume (10,74–76). For nonspherical particles this deviation is magnified significantly because most sizing methods are designed for spherical particles and cannot discriminate between different shapes. Figure 4 illustrates data obtained for this review on particles of various shapes using three different instruments (see Table II). Only in the case of spherical silica particles, were the data found equal to the true particle diameter. Relatively small deviations were observed in the case of prismatic (tubular) shaped particles of acetaminophen (AP I). Large deviations are encountered for platelet-shaped particles of salmeterol xinafoate and for the highly acicular, needle-like crystals of acetaminophen (AP II). This effect was not related to particles attrition during dispersion but to the particle shape (see below). Furthermore, agglomeration in the case of zinc oxide nanoparticles resulted in data being inconsistent with the size of primary particles. The reason for such deviations is that all these instruments operate on different physical principles and are calibrated for spherical, nonagglomerated particles. This is usually not the case for pharmaceutical materials. Similar observations were made in previous studies on intermethod correlation (2,7,10,74,75). The discrepancies of particle size analysis have been noted for fast-flow lactose that gave an average particle size of 49–86 μm by laser-light scattering and 40 μm by microscopic analysis (77). But even in the case of the same type of measurements, for example, using aerodynamic-inertia principles, the results may depend on specific instrument design. In a comparative study between the Andersen cascade impactor (ACI), next generation impactor (NGI) and time-of-flight aerodynamic particle sizer (APS) (78) for three pMDI-generated formulations, the particle size was underestimated by APS and the data were inconsistent for the two designs of cascade impactor operated under near equivalent conditions. Although some of these discrepancies could be attributed to formulation issues, the dependence of measured aerodynamic diameter on the airflow and instrument geometry cannot be ruled out, as found in some other studies (79–81). It was recommended (78) that both APS and NGI data be evaluated on formulation-by-formulation basis in relation to the large database which already exists for ACI-based measurements.

(a) Particle morphology of: silica, zinc oxide, salmeterol xinafoate; acetaminophen, AP I (prismatic) and acetaminophen, AP II (acicular). (b) Corresponding mean volume diameters measured by time-of-flight (TOF, AeroSizer™ with AeroDisperser, TSI Inc, USA), laser diffraction (LD, Helos/Rodos, Sympatec GmbH, Germany) and Coulter counter (Coulter Multisizer II, Coulter Electronics GmbH, Germany) instruments.
Owing to the aforementioned physical limitations of the measuring techniques, the concept of equivalent particle diameters has been introduced. These are diameters of calibrated spheres that yield the same value of a certain physical property when analyzed under the same condition as the irregularly-shaped particles. For example, the volume-equivalent diameter is the diameter of sphere having the same volume as of nonspherical particle measured by the same particle size instrument. The Stokes equivalent diameter is the diameter of sphere which falls with the same velocity in a liquid as nonspherical particle, etc. It is possible to subdivide all equivalent diameters in two basic groups: geometrical (i.e., related to spherical surface, cross section, volume, etc.) and behavioral (e.g., sedimentation, inertial deposition, etc.) (2). The latter group can be directly associated with some pharmaceutically relevant property during manufacturing or drug delivery. It should also be noted that the equivalent particle diameter is defined not only by the physical particle attribute measured, geometric or behavioral, but also by the measurement technique (e.g., laser diffraction, image analysis, electrical zone sensing, etc.) and often by the data processing algorithm. Therefore the number of different equivalent diameters is almost as great as the number of different particle-sizing methods. Despite this variability, a cross correlation between different techniques is required to determine which equivalent diameter is most relevant for a given API or formulation. Such a combined data analysis enables one to establish the effects of particle shape, particle agglomeration and sample instability on particle size measurements.
Sampling and Dispersion
The main goal of sampling is to withdraw the smallest quantity of the bulk material that can provide a representative PSD. The sampling problems with pharmaceutical powders are usually due to particle segregation or insufficient sampling weight. Segregation may occur as percolation between coarse and fine particle fractions or as agglomeration between different species of multicomponent mixtures. In the case of suspensions, concentration gradients and particle sedimentation may lead to selective sampling. Mixing and/or building sample from a large number of increments can minimize these problems. The following “golden” rules of sampling are recommended for proper powder sampling (82):
-
A powder should be sampled when in motion.
-
The whole of the stream of powder should be taken for many short increments of the time in preference to part of the stream being taken for the whole time period.
Sampling devices confirming these rules are available, such as spinning riffler (82). Unfortunately, reduction of pharmaceutical laboratory samples to milligram quantities may require very specialized powder samplers or sampling from agitated suspensions or fluidised beds.
A more fundamental sampling issue is the number and weight of samples required. The former can be assessed using the following expression (83):
where n is the number of samples required to assume the confidence level t, s is the sample standard deviation and Δd is the maximum allowable difference between the estimate and the actual value of particle diameter. For pharmaceutical applications, a value t = 2 (confidence 95%) is used for working quality and t = 3 (confidence level 99.9%) for total quality (53). For example: s = 0.5 μm, t = 2, Δd = 0.5 μm gives n = 5. Regarding the sample weight, it is clear that the limiting (minimum) weight of sample required is predetermined by the coarse particles in the PSD, because these particles are always underrepresented during sampling. The following relationship can be used (82):
where m s (mg) is the limiting weight, d (μm) is the mean diameter of the coarsest particles in the sample, ρ (g/cm3) is the powder density, σ is the tolerated sampling error, w c is the fractional mass of the coarsest class being sampled. For typical values w c = 0.1; σ = 0.05 (5%); ρ = 0.5 g/cm3, one can estimate that less then 1 mg sample is required for d < 10 μm (fine aerosols), whereas several grams of each sample will be necessary for particles with d = 100–200 μm (oral dosage forms).
Particles of pharmaceutical organic materials can be very cohesive and electrostatically charged, forming agglomerates of different sizes and structures. If the forces holding the primary particles are weak and more of a physical nature, the particles are said to be in the form of soft agglomerates (84). Strongly bonded, “bridged” particles are said to form hard agglomerates, which typically originate from the particle formation process, inadequate cleaning or drying. The primary particle can consist of single crystals, semicrystalline or amorphous solids. The primary particles can also be agglomerates of submicron nuclei and can have hollow or porous structure. As far as particle size analysis is concerned, hard agglomerates are considered as single particles and a part of the overall particle assembly. However, inefficient dispersion of soft agglomerates, which is typically observed in both dry powders and suspensions, can contribute to the largest part of analytical error. The goal is to eliminate as much particle agglomeration as possible from the sample to be analysed and, at the same time to avoid particle attrition (milling), due to the use of excessive dispersion forces.
Depending on the type of measurements, dispersion can be achieved in a liquid cell, with the addition of appropriate surface-active agents. Dispersion can also be achieved by controlled agitation and/or by the application of ultrasound. Polar liquids are typically used to disperse polar solids and nonpolar liquids to disperse nonpolar solids (82). Ionic or nonionic surfactants are selected to match the difference in surface polarity (to increase wetting efficiency). The solids should ideally be practically insoluble in the dispersing solvent. In extreme cases, the solid can be dispersed in its saturated solution in a suitable solvent. Here, there is always a possibility of changing the particle size distribution due to the thermodynamic “Oswald ripening” or recrystallization effects (85). The use of liquid dispersion is required for any submicron system because such particles are impossible to disperse in a dry state. A liquid dispersion aided by ultrasound was also found to be the most efficient method for measurement of primary PSD of some strongly agglomerated inhalation dry powders (10).
Dry-powder dispersers, which are usually attached to standard laser diffraction and time-of-flight instruments, provide a very convenient means to control and study the dispersion effects with micron-size powders (7,10). This is particularly valuable for dry-powder respiratory formulations where such dispersion is directly related to the performance of dry-powder inhalers. Dispersibility of powders in the airflow is defined as the balance of forces generated by the aerodynamic stresses that are necessary in dispersing particles. The mechanism of dispersion is very complex and may involve dispersion by acceleration, by shear flow as well as by impaction or other mechanical forces. It is hardly possible to anticipate all the factors involved, however, it is feasible to carry out a comparative study of different powders for the same device, considering the fluid energy delivered by the air flow, f, and taking as an adequate measure of such energy the magnitude of viscous turbulent stress, τS = K f 3/2. The coefficient, K, describes how efficient the dispersion device is at a constant airflow rate. Empirically, the dispersion profile for each powder can be found as a function of the flow rate or dispersion (differential) pressure, which is progressively related to each other (Fig. 5). The dispersion profile in Fig. 5a shows that the volume mean particle diameter (VMD) reaches a plateau. This means that most agglomerates are dispersed and the corresponding flow rate is optimum for measurements. More cohesive, strongly agglomerated powders disperse at a higher flow rate. In addition to providing the optimum dispersion regime, the dependency similar to that in Fig. 5 is useful in comparing the performance of different powders in DPIs. The dispersion process in the DPI typically occurs in the lower region of flows (<100 l/min) in Fig. 5b which corresponds to the viscous turbulent stress, τS, between 1–30 N/m2 (6–9). This fact explains why the performance of many DPIs filled with micronized drug or drug-lactose powders is relatively low.

(a) Experimental dispersion profiles for two different batches of salmeterol xinafoate (7). (b) Relationship between the dispersing air pressure, flow rate, f, and nozzle viscous turbulent stress, τ S , determined for RODOS (Sympatec GmbH), 4-mm dry powder disperser.
An imaging technique, such as optical or electron microscopy, can provide a useful description of agglomerates of micron- and submicron particles sparingly dispersed over a surface of microscope substrate (87). This approach is based on the fractal theory, which is linked to the image boundary fractal dimension, δ. The process of evaluating the fractal dimension of the boundary involves estimation of its perimeter P, by a polygon with a number of sides, n:
The side λ is known as the resolution parameter. The functional units of the aggregates can be described using their fractional dimensions, which affords a measure of the “ruggedness” of particle structures observed under a microscope. Figure 6 shows an example of this algorithm applied to aggregates of nanoparticles of griseofulvin produced using the supercritical fluid extraction of emulsions (85). Two regions of fractal structure can be seen with δ = 1.12 at highly resolved integration corresponding to packing of individual particles and δ = 1.4 characteristic of agglomeration during drying.

Dependence of the normalized (divided by the mean projected diameter) particles perimeter, P, on normalized resolution parameter, λ, both in logarithmic coordinates, for nanoparticles of griseofulvin shown on the SEM photograph.
For both dry powder and liquid systems, it can be generally concluded that development of an adequate dispersion technique and procedure is at least as important as the particle size analysis itself. For the inhalation powders and submicron systems, control of deagglomeration is the dominant factor which may require validation through the use of a portfolio of complementary techniques (7,10).
Accuracy, Precision and Main Sources of Errors
The following definitions from the Validation of Analytical Procedures (ICH Q2A and Q2B) (http://www.ich.org) are applicable to particle sizing:
Accuracy is the closeness of agreement between the values that are accepted either as a conventional true value or an accepted reference value and the value found (“trueness”). In mathematical terms, ‘accuracy’ can be defined as the mean percentage deviation, Ā, of an experimental particle size distribution (PSD) from the standard PSD (82):
where ΔP is the width of the size class, N is the number of size classes, A is percentage deviation of the measured and standard size for a given size class. A big deviation from standard does not mean that the instrument is in error, but that a different parameter is being measured by the standard technique. This fundamental issue is directly related to the definition of the equivalent particle diameter. Many examples are provided in the pharmaceutical literature. USP monograph<601> (Table I) compares the microscope and aerodynamic measurements for metered-dose inhalers (pMDIs). It is indicated that while particle size measurements by microscopy can be used to evaluate the number of large particles, agglomerates and foreign particulates in the pMDIs emissions, the test should be replaced, whenever possible, with a method to determine the aerodynamic particle size distribution of the drug aerosol leaving the inhaler. The aerodynamic particle size distribution defines the manner in which an aerosol deposits during inhalation. However it is clear that particle size analysis by gravimetrical or centrifugal sedimentation is the most appropriate method for assessment of the pMDI suspension stability. Thus to achieve the accuracy required for a particular pharmaceutical application, the general principle would be to use the measurement technique that resembles the process.
Precision is the closeness of agreement (degree of scatter) between a series of measurements obtained from multiple sampling of the same homogenous sample. Mathematically, precision can be defined as average standard deviation \( \overline{s} \) for a number of measurements (82):
where s is the standard deviation for a given size class. The related term repeatability is used to denote precision under the same operating conditions over a short interval of time (intra-assay precision). Reproducibility is precision between laboratories, as usually applied to standardization of methodology and interlaboratory testing in collaborative studies. These characteristics are very important for all pharmaceutical research, GLP and cGMP because they directly reflect the quality of instrumentation as well as reliability and consistency of the operating procedure (2,88).
Other important characteristics for particle analysis are the resolution and range. Resolution is defined by the width and the number of the individual particle size classes within the measured particle size range. The “dynamic range” is used to describe the size range where the required levels of accuracy and repeatability can be achieved without changing the instrument configuration. The resolution and the dynamic range are often inversely related to each other: the best resolution is often achieved when the instrument is configured to measure a specific and relatively narrow particle size range. For example, there is a well-known problem that the different sizing instruments (with possible exception of electron microscopy) do not cover the entire range of particles used in controlled release (CR), which ranges from a few nanometers for micellar systems to hundreds of μm for large microspheres (88). Particle size range between 0.5–1 μm are shown to be the most problematic with the most inconsistent data obtained by techniques such as light scattering, electrical conductivity and light obscuration. Clearly, this range belongs to the very limit of the most important particle sizing methods (Table II) where the accuracy is the lowest. This is of particular importance for systems with relatively wide, bimodal and multimodal PSDs. In such cases, a combination of electron microscopy with a counting particle size analysis described below may afford the best accuracy and resolution.
Common sources of errors in particle size analysis are as follows:
-
Instrumental (hardware) errors—that reflect the limitations of the analytical method and are generally associated with the accuracy of measurements as described above.
-
Statistical errors—that are mostly dependent on the sampling and dispersion procedures.
-
Data interpretation (software) errors—that can occur due to application of more or less suitable algorithms of computation and analysis.
-
Operator errors—that are normally due to incorrect calibration, set-up, operating procedures.
In general, any particle-sizing instrument has an optimum dynamic range, where the instrumental error is minimum. The sampling error always increases and dispersion error decreases with increasing particle size as explained in the following section. It is possible to separate the instrumental errors from the statistical errors by using different sampling or dispersion sequences (82). The total variation (s 2) is the sum of the individual variations due to measuring procedure and the other factors. For quantitative description, Eqs. 4 and 5 are recommended to be used to describe the accuracy and precision respectively. The assessments, which are based on comparison of the mean particle diameters rather than on the statistics of the whole PSD, often lead to an underestimation of these errors. For example, inhalation compounds may have very similar MMAD and even the same GSD but exhibit completely different PSDs such as monomodal and bimodal distributions and behave differently during aerosolization (89,90).
Validation, Calibration and Verification
During validation, an instrument is subjected to a series of qualification procedures. These qualification procedures check the general operating conditions of an instrument, proper installation of all hardware and software components and proper functioning of components.
Calibration is a process where an instrument is used to measure a known standard and its response is adjusted until the answer given corresponds to the standard. The instrument will then hold this adjustment for a limited period of time and will then gradually depart from the calibrated state. Standard material consists of spherical particles having certified values that are directly traced to the standard “metre” (e.g., via microscopy). Microscopes and image analyzers, both optical and SEM, are usually calibrated using certified graticules. In devices such as TOF and CI, fixed internal calibration methods are provided by the manufacturers. Optical techniques, such as LD, light scattering and DLS, involve the use of a fundamental measuring scale—laser wavelength, and therefore do not require calibration.
Verification or performance qualification procedure is carried out for all instruments to ensure that all specifications (hardware and software) are within the established limits. This is generally accomplished by using a reference material which is a “stable material of arbitrary particle shape, its certified values are referenced to a reference method” (82). The size of the reference material is compared with its certified values to determine instrument accuracy. The reference materials are usually supplied with the instrument in a form of easily dispersible dry powders (e.g. silica, glass, SiC) or stable suspensions of narrowly classified (monodisperse) latex or polystyrene spheres available in both nano- and micron-size ranges. For most measurements, certification is recommended with at least two reference materials corresponding to high and low ends of the dynamic size range.
All points discussed above should be reflected in the standard operation procedures (SOPs) which contain all necessary information for the control and revision of QC and QA documents including functional and design specifications, testing procedures, product release documents, certificates and service guidelines. For example, the development of reliable and validated analytical methods for particle sizing of controlled release (CR) parenterals for use in research and development as well as in manufacturing QC has been one of the subjects of a workshop organized by EUFEPS and AAPS (88). It was noted that the size distribution of microspheres for the final product should be the same as that used for clinical batches. In addition, QC with appropriate validation is needed to determine whether segregation occurs during processing, and if so, what procedures to develop so as to avoid this problem. The same instrument and the same standard operating procedure must be used for QC testing of a given product. This limitation may create problems in scale-up and in manufacturing site changes.
Instrumentation
Microscopy and Image Analysis
Among the techniques most commonly used in the pharmaceutical research and development (Table II), microscopy is often applied as an absolute particle sizing method because this is the only method where the individual particles can be observed, measured and their shape determined (7,5,10,74). Although the theoretical resolution of light microscopy is about 0.2 μm with the high numerical-aperture (NA) immersion objectives, the diffraction halo gives gross overestimation for particles in the lower micron size region. The resolution of an optical microscope is a function of the optical magnification, type, quality of the objective, numerical aperture, type of immersion media and also optical characteristics of particles themselves. Therefore the exact lower limit, with given accuracy should be assessed for each individual microscope. Confocal microscopy can be applied to increase the image contrast, but the general limitation of the optical wavelength remains (91). Determination of particle size using optical method is also limited by statistical considerations during computerized image analysis. The algorithm used typically calculates the equivalent projected-area diameter or projected-perimeter diameter. Since the particle orientation on a substrate usually gives the maximum area, this leads to an apparently larger particle size than that measured by other techniques (82). However, by far the most common error is underrepresentative sampling. The minimum number, N min , of particles to be measured can be estimated in terms of the maximum sampling error of the PSD distribution as N min > 1/s 2. This results in more than 10,000 particles for a maximum standard deviation of 1%. The accuracy largely depends on the coarsest particle class measured. Following ISO 14488 (Table I), the minimum number of particles depends on the PSD and typically more than 1,000,000 particles are necessary to reach a maximum error below 1%.
Although microscopy, in particular, scanning electron microscopy (SEM), is the most essential technique for particle size analysis, it is not very reliable for sizing by itself and should always be used in combination with other techniques. There are large statistical errors and also biases associated with preferential particle orientation and particle agglomeration that are difficult to control and minimize. This in effect will result in low measured particle numbers per image and high computation times. Several imaging techniques are capable of addressing some of these issues. Stream-scanning optical image analysis enables a faster data collection and controlled orientation for micron-size particles (see Data Interpretation and Presentation). Cryo-transmission electron microscopy (Cryo-TEM) can be used to provide information on particles in frozen suspensions without drying, thus avoiding potential problems with particle aggregation. Environmental SEM (ESEM) allows measurement of aqueous dispersions at atmospheric pressure, albeit at the expense of image resolution (92).
There is an expanding group of imaging techniques which can discriminate between active and nonactive pharmaceutical ingredients in formulations: fluorescent confocal microscopy, vibrational spectroscopy (IR, Raman) and SEM with energy-dispersive X-ray (SEM/EDX). For example, Raman chemical imaging was developed for API-specific PSD analysis of several corticosteroid suspensions aqueous nasal spray suspensions (93). 1,600–1,700 cm−1 spectral range allowed ready distinction between the drug and excipients of the mixture as well as drug adhered to excipient particles. Similarly, Raman microscopy was applied to foreign particles testing in inhalation drug products (66). Atomic force microscopy (AFM), is another imaging technique based on scanning (tapping) of nano-scale probes over the sample surface. Although this method is relatively slow and usually requires an elaborate sample preparation, the images are very similar to those obtained by SEM with resolution down to several nm. In addition to the particle size and shape, AFM can also provide information on the particle surface properties, for example, interparticle interactions in the DPI formulations (94).
Laser Diffraction and Static Scattering Techniques
LD is rapidly becoming a preferred standard method for particle sizing in the pharmaceutical industry. This is due to its short analytical time, robustness, high precision, reproducibility, wide measurement range and flexibility of operation using liquid, spray and dry dispersion attachments (7,10,74–76). Most LD instruments employ a standard He–Ne laser light source (632.8 nm wavelength) and consist of an optical system for Fourier transformation of the diffracted light onto a position-sensitive detector. The light scattering pattern from nonspherical particles is very complex, varying as a function of the scattering angle, particle size and shape, and complex refractive index which depends both on the light refraction (real component) and absorption (imaginary component). However, the forward (Fraunhofer) diffraction depends only on the particle size, an azimuthally averaged tangential (Feret’s) diameter. This diameter can be associated with the projected-equivalent diameter that is defined by the overall intensity of the diffracted light. The volume-equivalent diameter is not measured by the laser diffraction technique, although the volume PSD is derived from the Fraunhofer diffraction pattern using a system of linear equations incorporated into the algorithm of the instrument (95,96). Algorithms, based on rigorous Mie scattering theory should be ideally applied for particles below 25 μm (3), however these require the knowledge of complex refractive indices which are not available for most organic materials and not directly measurable with the available instruments. Beekman et al. (3) showed that errors in the estimation of the “effective” refractive index may produce radically different PSDs, particularly for particle below 10 μm. Therefore, in practice, the dispersion errors with small particles and uncertainties introduced by the imaginary component of the refractive index may outweigh the inaccuracy associated with the simplified Fraunhofer theory (96). For nonspherical particles, such as plates and needles oriented randomly, the volume diameter is typically overestimated because of the larger projection diameter for these shapes (Fig. 4b). Another error may originate from high concentration of particles analyzed—high obscuration of laser beam, leading to multiple light scattering and overestimation of particle fines (undersizing the PSD). This can be easily avoided by keeping the obscuration, usually monitored during measurements, within 0.1–0.3 interval. In some instruments, the LD method is combined with multiangle and multiwavelength light scattering measurements, which enable expansion of the dynamic measuring range and essentially become the multiangle static laser light scattering (LLS) method (5,92).
As mentioned before, the equivalent diameter measured by LD is not directly related to the particle volume or surface and therefore care should be taken when interpreting these data for any pharmaceutical application. For the quality control purposes it is sufficient to establish a reliable correlation between the LD data and, for example, PSD measured by image analysis or aerodynamic measurements (3,7,10,76). In the instances where particle size is measured for the dosage form, different formulation ingredients may strongly affect the data. Examples include assessment of powder blending and tablet homogeneity (2), measurements of nebulizer sprays (76,90), phase separation and aggregation in pMDI suspensions (97,98) and deaggregation in DPIs (86).
Finally, it should be noted that techniques such as small-angle X-ray scattering (SAXS) (99) and small-angle neutron scattering (SANS) (92) are essentially based on the same physical principle of light diffraction, but with the application of a much shorter radiation wavelength (typically several Å). This enables an increase of resolution well into the nanoscale region, rendering the observation of colloids, micelles, lamellas and similar nanostructures possible. However these techniques are not for routine or common applications and require considerable specialization in data collection and interpretation. It should also be noted that X-ray powder diffraction analysis (XRPD), sometimes referred to as wide-angle X-ray scattering (WAXS), is strictly not a particle size technique. XRPD allows one to determine the lattice parameters and physical broadening of diffraction peaks as a cumulative measure of crystal lattice imperfections (100). The latter is related to the size effects of crystal defects such as grains, small-angle boundaries and stacking faults which, however, cannot be directly attributed to the geometric particle size.
Dynamic Light Scattering (DLS)
This method, also known as photon correlation spectroscopy (PCS) or quasi-elastic light scattering, is primarily used to measure nanoparticulate colloid systems such as emulsions, micelles, liposomes and nanosuspensions (5,85,90,92). When a laser beam is passed through liquid suspensions containing particles in Brownian motion, it experiences fluctuations in its intensity due to light scattering. In the DLS instrument, measurements of this fluctuation of intensity at a given scatter angle are used to infer the particle size or the ‘hydrodynamic diameter’ of the suspended particles. The DLS instruments measure the fluctuations in the intensity of the scattered light with time in order to generate an exponentially decaying autocorrelation function. This function is then analyzed for characteristic decay times, to determine the diffusion coefficient unique to the scattering suspensions and, in conjunction with the Stokes–Einstein equation, the hydrodynamic radius. The primary advantage of DLS method is that it provides an absolute measurement without any further information about the composition and the optical properties of the particles in suspension. The lower limit of the instrument depends on the laser power and signal-to-noise ratio and can be as low as 2 nm. Hence it can be used to measure the sizes of not only surfactant micelles and colloids but also macromolecules. The data obtained using the instrument is usually in two formats depending on the type of algorithms used for the inversion of the autocorrelation function. A Gaussian distribution is typically used to represent unimodal dispersions. A more complex analysis is required for multimodal (e.g., bimodal) particle size distributions. Introduction of polydispersity can also lead to a significant complication because the equations used to reduce the particle size become more ambiguous and less stable (101). The algorithms used provide information about the mean particle size, widths and peak modes of the particle size distributions. The intensity-based data, collected by the instrument, can be reliably reduced to a volume-weighted PSD. However, large particles (>3 μm) may completely distort the measurements and therefore a complementary analysis with LD or laser scattering instrument is recommended in order to corroborate the results obtained.
One of the disadvantages of the DLS method is that samples in some cases may require significant dilution for accurate size measurements, which can be problematic for measurement of droplet sizes of emulsions. Novel approaches using fiber optics and back-scattering have been developed and implemented in some commercial instruments to allow measurements in concentrated suspensions. Many equipment designed for DLS may also have an attachment for electrophoretic light scattering to measure the zeta-potential important for colloids stability. An interesting variation of DLS is the fluorescence correlation spectroscopy (FCS) (102). FCS is a well-established technique to determine diffusion coefficient, size and mass of particles, as well as to characterize the binding of low molecular weight ligands to larger receptor molecules in solution. In FCS the laser-induced fluorescence of particles out of a very small probe volume is autocorrelated to the diffusion time. A dual-color instrumental extension of the standard confocal FCS setup enables cross-correlation analysis of two different fluorescent species. Thus by labeling different particles it is possible to locate different components inside the particles and yield information about the composition of the complexes. A less-developed Raman correlation spectroscopy (103) extends the domain of optical fluctuation spectroscopy to Raman scattered light, combining the chemical identification obtained by Raman scattering with the particle size and dynamics information obtained by correlation spectroscopy.
Coulter Counter (Electrical Zone Sensing)
This instrument was originally developed for sizing blood cells and cell cultures. Its principle therefore is well suited for the measurement of nonagglomerated and stable suspensions (10,75,82). The particles are suspended in a weak electrolyte and passed through a small orifice, separating two electrodes. As each particle in the electrolyte crosses the orifice it displaces its own volume of electrolyte causing an increase in electrical impedance. This change in impedance generates voltage pulses, which are proportional to the volume of the particles and are used to measure the equivalent volume diameter of the particle. Analysis using Coulter counter is fast and exhibits good reproducibility of measurement. Further, the particle size analysis can be performed in a relatively wide overall size range (Table II), using different electrosensors (aperture tubes). The dynamic range for different tubes varies from 2 to 60% of the orifice diameter because the response from smaller particles is lost in electronic noise whereas a nonlinear response and blockage may occur for larger particles. Calibration is essential for this technique. The difficulties are usually related to the particle dispersion, in particular for highly hydrophobic or poorly wetted materials (10). Difficulties are also encountered for measurement of water-soluble drugs for which the drug solubility in electrolyte needs to be minimal; for porous particles, loose agglomerates (flocs), and lastly for particles with extreme shape (needles, thin plates and rods) where large errors in volume equivalent diameter are observed (82).
Time-of-flight (TOF)
Devices such as API AeroSizer™ and Aerodynamic Particle Sizer (APS) (TSI Inc, US) are based on monitoring time of flight of particles that are accelerated by air streams and expanded at sonic velocities, between two laser beams. Smaller particles are accelerated at a faster rate than larger particles due to differences in mass. The aerodynamic diameter of the particles is calculated using calibration curves for spherical particles of known density incorporated into the data analysis software. Newer versions of this instrument have an improved electronics to minimize coincidence and to extend the dynamic range by measuring single pulses from large particles. TOF is a fast stream-scanning technique, which has the potential for high-resolution measurements within a relatively wide dynamic range. It requires small sample quantities for size analysis. It measures an equivalent aerodynamic diameter and therefore is a logical choice for pharmaceutical aerosol measurements. However, as shown below, this equivalent diameter is different from that obtained at small air velocities and also very sensitive to the particle shape (7,104). When applied without the shape correction factors, the TOF measurement would typically underestimate the particle volume diameter. An integral part of the instrument is an aerodynamic disperser, which may utilize a fluidized bed aerosol generator, lifting powder from a turntable (79) or using an inhaler adapter. Applying the same methodology as shown in Fig. 5, one must ensure that for cohesive powders the dispersing device is adequate for particle deagglomeration, so as to avoid highly significant errors with both accuracy and precision. Large particle number densities, usually for submicron particles, may introduce some artifacts, such as oversizing due to coincidence errors (105).
Cascade Impactor (CI)
Andersen Cascade Impactor (ACI) and the Next Generation Impactor (NGI) (Table I) are the primary techniques used for both the development and QA/QC testing of commercial inhaler products (2,78). Size determination is based on the inertial impaction of aerosolized particles passing through decreasing nozzle apertures onto subsequent deposition stages. Each deposition stage provides a defined aerodynamic cut-off diameter (particles collected with 50% efficiency). The collection plates can be coated to avoid particle bouncing. Humidity, temperature, pressure differential over the inhaler under test and airflow rate can be controlled. The instruments are also supplied with USP induction port, preseparator and fine filter. The impactors are calibrated at certain air flow rates as shown in Table III, the measurements can however be performed at any arbitrary flow rate, defined by the pressure differential over the inhaler device. The USP specifies the measurements performed for DPIs at an airflow rate which produces a pressure drop of 4 kPa over the inhaler to be tested and a duration consistent with the withdrawal of 4 liters of air from the mouth piece of the inhaler. This can be clearly justified by the various flow resistances of different DPIs with obvious implications for the dispersion energy within the inhaler. The standard test conditions for pMDIs are 28–30 l/min. The cut-off diameters for different flow rates can be calculated based on the Stokes equation as discussed in the next sections. The estimation of particle size is typically based on the mass distribution determined by chemical (UV or HPLC) analysis, which is necessary from therapeutic and regulatory perspectives to discriminate between the active (i.e., drug) and inactive (i.e., carrier) substances. The most important parameter measured is the fine particle fraction, FPF, which is defined as the mass of particles (with reference to the emitted dose) below a certain cut-off diameter (e.g., 4.7 μm, i.e., below ACI stage 2). Flat design of NGI is often considered more suitable for automated measurements. NGI also has steeper collection efficiency curves, offering the advantage of more accurate size fractionation (78,106). There are several other impactors included in Pharmacopoeias (Table I), such as Multistage Liquid Impinger (MSLI). Each stage, except Stage 5, of MSLI must be dispensed with 20 ml liquid. The size determination is based on aerosol–liquid interaction, giving more realistic simulation of impaction in the lungs. Although water is the preferred choice of solvent, organic solvents can also be used, particularly for sparingly soluble drugs. This may however create problems in possible solvent evaporation since 60 l/min airflow is normally used in MSLI. Both CI and MSLI measurements are, in general, very time-consuming. Electrical Low Pressure Impactor, ELPI™ (107) is based on charge detection of particles, which enables in situ high-speed analysis of particle fractions deposited on 13 different stages. However this principle does not allow for a direct measurement of the drug mass-weighted distributions and requires a more complex calibration procedure (108).
Data Analysis
Data Interpretation and Presentation for Pharmaceuticals
Knowledge of specific formulation needs and the physical characteristics of the particulate systems is imperative for effective data presentation. Particle size analysis comprises both the measurement and the quantitative description of physical properties of the particulate matter. The analysis in most cases requires a specific size measurement methodology and careful data interpretation. As a general guide, it is appropriate to determine the particle size distribution on the behavioral principle that the measurement technique “closely resembles” the conditions in which the particles will be used: processed, formulated or delivered. The diameters related to filtration and sieving can be used for representation of the size of injectable and oral formulations respectively, aerodynamic equivalent diameter for aerosols and the hydrodynamic sedimentation (Stokes) equivalent diameter for micro and nanosuspensions. When application of behavioral particle equivalent diameter is problematic, a correlation should be made between the physical or biopharmaceutical particle property in question and one of well-defined geometric equivalent diameter. Thus the properties of pharmaceutical formulations such as drug dose and dissolution rate are usually given by the distribution of particulate mass/volume and the surface-volume equivalent diameter (85). The drug chemical and thermodynamic stability information can also be represented using both volume- and surface-volume equivalent diameter (109). Number based distributions are important for quality control purposes, for example, analyzing the presence of foreign particles in injections (see Table I) and respiratory formulations (66).
Correct data presentation and interpretation are essential for consistency and understanding of “what is being measured”. Varying data format, e.g. nature of particle equivalent diameter, type of PSD or definition of appropriate mean diameters, often escapes a clear definition in the pharmaceutical research. This is inconvenient but can be standardized. A more serious issue is that in many cases the raw data obtained by a particle sizing instrument are fitted into a certain mathematical model, particularly for the field-scanning techniques, as dictated by the data collection and interpretation algorithms. This treatment may predispose the data to a particular interpretation or bias such as exaggeration or underestimation of fines, coarse particles or aggregates, systemic shift in the mean particle diameters, appearance of artificial modes in the PSD. For example, laser diffraction instruments may produce artifacts dependent on the model and manufacturer of the instrument because the optics, sensors and software employed can be very different (2,3).
The next section deals with more general mathematical terms and definitions, which can be applied to any data presentation and instrumentation type.
Particle Size Distribution (PSD)
PSD of a powder can be described by the particle dimension, r, assigned as follows: number (r = 0); length (r = 1); projected area, surface area (r = 2); volume r = 3); mass or weight (r = 3, no voids), corresponding to the number-weighted, surface-weighted and volume (or mass)-weighted PSDs respectively. For spherical particles these distributions can be easily converted from one type to another. For nonspherical particles, however, information about the surface and volume shape factors is required for the conversion. As a rule, the volume (mass)-weighted PSD is the most appropriate description for pharmaceutical materials. The number-weighted PSD is useful for determining the size of primary particles in agglomerated systems as well as the tightness of a PSD. The closer the number-weighted and volume weighted PSDs, the narrower the particle size distribution. The graphic presentation of PSD is made in terms of cumulative distribution, Q r , and frequency (density) distribution, q r , calculated from the cumulative data. These parameters are related by the following normalized equation:
where d min and d max define the particle size range. In practice, Eq. 6 is always calculated as a sum of the particle size classes, i.e., individual bins in which the particle are classified by the instrument. A typical PSD with average particle diameters is shown in Fig. 7. The mode average diameter corresponds to the peak and the median represents 50% (of mass, volume or number, d 50 ). The mean particle diameter of a system of unequally sized particles is represented by a system of spheres having only two characteristics of the original distribution. The general equation for calculating the different mean particle diameter values is given below:
where ΔN is the number of particles in a size class. The most commonly used mean particle diameters are: d[1,0]—arithmetic mean diameter which corresponds to the mean linear diameter; d[2,0]—surface mean diameter; d[3,0]—volume mean diameter; d[3,2]—Sauter mean diameter which corresponds to the specific surface area; d[4,3]—volume moment which corresponds to the “gravity center” of volume (or mass)-weighted PSD (82). Any PSD can also be characterized by its standard deviation, σ, from the corresponding mean value, \( {\mathop d\limits^\_ } \):
Approximately, the width of PSD can be estimated by using a parameter called PSD spread. It is calculated from lower and upper fractions of the cumulative PSD as: (d 90 − d 10 ) / d 50 .

A typical volume-weighted particle size distribution (PSD) obtained using an LD instrument (RODOS, Sympatec GmbH) and corresponding average diameters. Notice that both the cumulative and density (frequency) PSDs are presented on the logarithmic scale.
Pharmaceuticals exhibit a wide array of PSDs. Characteristic distributions reminiscent of normal (Gaussian), log-normal and other canonic forms can be observed. Such distributions lend themselves well to mathematical analytical treatment, for example, conversion between different mean diameters, moments and types of PSDs (82). However, in most cases, the PSDs are skewed and have arbitrary forms for which the general Eqs. 6–8 and numerical computations should be applied.
Particle Shape
All the equations above are applicable to equivalent particle diameters, which are influenced by the particle shape. Assuming that the particle shape does not depend on the particle size, its quantitative description can be provided either by particle sphericity, ϕ, or surface-to-volume shape factor, αSV:
Sphericity is defined as the ratio of the surface area of a sphere with equivalent volume diameter d V , to the actual surface area of the particle, defined by the equivalent surface diameter, d S . The maximum ϕ = 1 corresponds to a sphere. Sphericity can be measured using image analysis by directly computing the diameters in Eq. 9. Sphericity is also related to the specific surface area, S, through the following relationship (7):
where the volume-weighted PSD, q 3(x), is determined preferably using a technique based on volume-equivalent particle diameter and S is measured, for example by BET nitrogen adsorption (7). Nonspherical particles are typically observed over all orientations and this causes a broadening in the measured size distribution. Thus even a “monodispersed” assembly of nonspherical particles will have its own PSD. Some artifacts may appear—for example, laser diffraction measurement of acicular particles may exhibit bimodal distribution, which corresponds to the characteristic minimum and maximum diffraction diameters for these particles (95). The shape broadening function can be measured using the same instrument, if monodispersed nonspherical particles are available, for example, from sieving, filtration, sedimentation or other classification techniques. However such an approach has been severely limited by the lack of source of particles with well-defined geometry and density (104). Another possibility is to measure the particle shape under microscope and then calculate the shape broadening function assuming the statistical particle orientation. Figure 8 shows an example of such computation performed for monodispersed powder of salmeterol xinafoate, which consists of very thin platelets (Fig. 4a). It is characteristic for such a PSD to be skewed towards the smaller particle diameters, having the maximum shifted towards the largest particle projection. The equivalent projection area particle diameter, shown in Fig. 8, is the appropriate equivalent diameter for microscopy, scanning optical techniques and also for laser diffraction measurements. The “measured” PSD, q r (x), is a convolution of the “real” PSD, q r0 (x), and the shape broadening function, p(x), normalized accordingly:
Knowing, the function p(x) and experimentally determined function q r (x), the “real” PSD can be deconvoluted numerically from Eq. 11.

There are very few analytical instruments which can determine both the particle shape and size. Some stream-scanning automated image analysis instruments, e.g., Sysmex™ , Malvern, UK and QICPIC™, Sympatec, Germany (110), can determine the particle “circularity” which is defined by the ratio between the particle perimeter and circumference of the projection equivalent circle. Another device (Aspect™ aerosol size and shape analyzer, Biral, UK) is based on anisotropy of laser scattering from individual particles and characterizes particle shape by a single parameter called the asymmetry factor, which is related to the particle aspect ratio, i.e., ratio of the maximum to minimum characteristic particle dimensions. The asymmetry factor takes values between 0 (spherically symmetric particles) and 100 (long fibers).
Aerodynamic Particle Diameter
The concept of aerodynamic diameter, d A , is central to any aerosol measurements and respiratory drug delivery. It is defined as the diameter of spheres of unit density, which reach the same velocity in the air stream as nonspherical particles of arbitrary density. The most important average diameter for aerosols is the mass–median aerodynamic diameter, MMAD, which can be found as d 50 on cumulative mass-weighted (or volume-weighted for solid particles) PSD with the aerodynamic equivalent diameter. Calculations based on the Newton’s general dynamic equation for nonspherical particles with volume-equivalent diameter (d V ) leads to the following equation for the aerodynamic diameter (7,104):
where ρ0 is the unit density (of spherical calibration spheres) and ρ is the particle density. C d is the particle drag coefficient which is generally a function of particle sphericity and particle Reynolds number, \( \operatorname{Re} = {\nu \rho _{a} d_{v} } \mathord{\left/ {\vphantom {{\nu \rho _{a} d_{v} } \mu }} \right. \kern-\nulldelimiterspace} \mu \) where ρa and μ are the air density and viscosity, ν is the particle velocity relative to the air stream. Re A and Re A denote particles with diameters d A and d V respectively. C c is the Cunningham slip correction factor which depends on the particle diameter (80,104) and which becomes significant only for submicron particles (7). Eq. 12 is solved numerically in general cases. This equation is also equally applicable to solid particles, porous particles and aggregates provided that the particle density (or void fraction for aggregates) is known. The flow regimes can be defined as Stokesian (Re < 0.1) and ultra-Stokesian (0.5 < Re < 100) and Newtonian (Re > 100) (62). For the spherical particles in Stokesian flow regime, the drag coefficient assumes the well-known relationship: C d = 24/Re. Therefore, Eq. 12 leads to the simplified expression for Stokes aerodynamic diameter widely used in the aerosol literature:
where χ is the dynamic shape factor, defined as the ratio of the drag force on a particle to the drag force on the particle volume-equivalent sphere at the same velocity. Thus nonspherical particles tend to have a smaller aerodynamic diameter. For liquid aerosols, such as nebulizer and pMDIs sprays, the droplet particle shape is not completely spherical due to deformation by air stresses. For example, it is shown that liquid droplets larger than a few μm aerodynamic diameter were systematically undersized in the TOF measurements (81,104). These measurements are also affected by the instrument type (41,76,78). The relationship (12) also explains why porous particles afford much better aerosols than solid materials—their aerodynamic diameter is reduced compared to the volume equivalent diameter. Interparticulate interactions decrease with an increase of the volume-equivalent diameter and therefore such particles can be aerosolized more readily and penetrate deeper into the respiratory system.
Predictions and Correlations for Aerosol Measurements
As shown by Eq. 12, the aerodynamic diameter depends on the particulate properties (geometric size, shape, surface morphology, density) and on the dynamics of airflow (flow geometry, turbulence, character of the shear and drag forces). Inhalation powders are usually nonspherical and always agglomerated with a possible triboelectrofication effect at high Reynolds numbers characteristic of both the CI and TOF nozzles (7,111). Liquid aerosols frequently exhibit issues with droplet evaporation, phase separation and influence of additives on both droplet atomization and on particle size distribution (76,78,98). Thus there has always been a problem with selection of particle sizing techniques and validation methods for respiratory drug delivery. Clinical in vivo studies on the deposition of different dosage forms using kinetic evaluation and drug assays or direct monitoring of the lungs using gamma scintigraphy are very laborious, costly and impractical in formulation studies. Clearly, the ultimate task is to determine the mass (or volume) PSD based on the equivalent aerodynamic diameter, d A . The cascade impaction method is closest to such measurements, but also very laborious and of low resolution. This method is primarily intended for quality control, where the focus is on the relative measures of product performance. The results obtained in the impactor depend on the airflow rate and the inhaler design. Therefore a systematic, scientifically driven approach to formulation of aerosols requires the use of other particle sizing techniques such as image analysis, laser diffraction and TOF. The correct approach here is to predict the d A values using corresponding geometric equivalent diameters (e.g. volume or projection) and to find a correction factor for d A in different air flows.
It should therefore be emphasized that the aerodynamic diameter is a function of air flow velocity, expressed through Re number [Eq. 12], and consequently is different for all aerodynamic particle measuring devices, and for the human respiratory system. The Stokes flow [Eq. 13] cannot always be applied without introducing a significant systematic error. The following intervals of Re can be calculated for different aerodynamic sizing techniques and particles between 0.5–5 μm:
-
10 < Re < 100: TOF AeroSizer™
-
5 < Re < 50: TOF APS™
-
0.1 < Re < 20: CI
-
0.01 < Re < 2 (human respiratory system between terminal bronchiole and trachea)
In the above calculations, different nozzles and flow rates for both ACI and NGI were taken from reference (112). Apparently, particles change their relative velocity and trajectory continuously in all these instruments, and therefore, it is difficult to define accurately what Re should be taken as the particle Reynolds number. However, both TOF and impactor techniques involve high particle acceleration in the nozzles and, their relative velocity may reach that of the nozzle air velocity (80).
Two approaches can be used to compute d A using Eq. 12. First, the dynamic shape factor can be determined experimentally from sedimentation or TOF measurements (104,113) and then the drag coefficients calculated by applying semiempirical correlations known for spherical particles. The second and more general approach is to describe the particle drag coefficient, C d , as a function of both the particle volume-equivalent diameter (d V ) and particle sphericity (ϕ) (7,114,115). Such semiempirical correlations are typically valid for both the Stokesian and ultra-Stokesian flow regimes. Figure 9a shows how the aerodynamic diameters, calculated using the model by Ganser (115) and Eq. 12, change nonlinearly with their equivalent volume diameter. These are also functions of the particle sphericity, ϕ; particles with small ϕ, such as thin plates, needles and rods have reduced aerodynamic diameters and therefore their volume-equivalent diameters will be underestimated, if such particles can be efficiently dispersed and they do not align themselves in the airflow. Moreover, Fig. 9b shows that the aerodynamic diameter of nonspherical particles is a function of particle Reynolds number (or flow velocity) and decreases at high Re. The underlying reason for this effect is that the dynamic shape factor increases with increase of Re. The effect of underestimation of the diameter for nonspherical particles was observed for the TOF techniques (7,80,104) (also Fig. 4) and cascade impactor (4,7). Furthermore, even for spherical particles with reduced density, such as porous particles designed for deep lung delivery, the aerodynamic diameter depends on Re. As shown in Fig. 10, a significant deviation up to 45% from the square-root dependence (Eq. 13), is expected for light particles in the ultra-Stokesian flow.

(a) Aerodynamic particle diameter as a function of the volume diameter, d V , and sphericity, φ, within the interval 10 < Re < 200 (TOF AeroSizer). (b) The same diameter calculated as a function of the Reynolds number, Re, for particles with sphericity, φ = 0.5. The particles density was assumed to be unity.

Aerodynamic diameter of spherical particles as a function of the particle density and particle Reynolds number calculated for volume diameter d V = 5 μm.
Another well-known assumption of the Stokes flow is made to recalculate the cut-off aerodynamic diameters, d C (Stokes) from calibration diameters, d C0 , in the cascade impactors:
where Q is an arbitrary flow rate and Q 0 , is the calibrated airflow (Table III). For the air flow increase from 30 to 100 l/min in the NGI, Eq. 12 predicts an error of about 15% underestimation of the aerodynamic diameter for particles with d V = 1.5 μm and φ = 0.5 because of the Stokes approximation. Similarly, a systematic error 5–10% may be introduced in Eq. 14 for cut-off diameters of porous particles (see Fig. 10).
Finally, it should be noted that all discussion above is concerned with the effect of inertial impaction, which is valid for relatively large Re > 0.1 and which represents the major deposition mechanism in the upper airways. The other two major phenomena affecting particle deposition in the lungs, sedimentation and diffusion, are also defined by aerodynamic equivalent diameters that are respectively related to the sedimentation velocity and Brownian diffusion in the Stokes flow regime.
In-line/Online Size Analysis and Process Analytical Technology
There is a specialized group of particle sizing instruments and sensors developed for in-line or online applications. In-line typically means that sampler, disperser, and/or sensor are mounted in the production line. A partial flow of particles needed for the analysis is guided through the dispersing system and always recycled into the main production flow. Online configuration is when the disperser and sensor are outside of the production line but closely and directly coupled. A partial flow is fed through the disperser and either recycled or disposed. As a rule, speed, reliability and robustness take priority in these instruments over resolution and accuracy. Optical techniques are noninvasive and lend themselves well to quantitative analysis and are particularly advantageous for dynamic measurements. The advent of high-speed electronics and fast-automated computer systems has greatly facilitated such applications. For example, commercial in-line/online systems exist for laser diffraction equipped with appropriate samplers/dispersers (e.g., Insitec™ by Malvern, UK; Mytos™ and Safir™ by Sympatec, Germany). Particles are usually sampled from an air jet of controlled stream or diluted suspensions. Phase Doppler anemometer (76,116), based on measurement of interference pattern produced by particles moving through intersection of two laser beams, is an excellent instrument to characterize the liquid sprays and particles in jets, giving the particle number count and velocity in addition to the particle diameter. Focused beam reflectance measurements (FBRM™), based on measurement of the time required for a laser beam moving at a fixed velocity to cross a particle (Lasentec™, Mettler Toledo, U.S.), represents one of the few techniques developed for batch-reactor processes. For such applications, sensors have to operate in a harsh, often aggressive environment, resistant to contamination of optical surfaces and high level of background noise. For the nonoptical methods, acoustic attenuation spectrometry (97,117) is capable of particle sizing of concentrated (1–70% w/w) liquid suspensions and slurries within a very wide dynamic range between 0.01–3,000 μm. The disadvantage of this method, however, is the requirement for a precise knowledge of several physical constants for dispersed and continuous media.
In general, the dynamic quality of in situ data is much superior to the ex situ results obtained using standard particle size analysis. The following areas of applications can be distinguished:
-
Investigations into the particle behaviour in different inhalers and sprays.
-
In situ mechanistic studies and optimization of particle formation processes (e.g., spray-drying, crystallization, etc.).
-
Industrial process monitoring and control-process analytical technology (PAT).
For example, Shekunov et al. have studied the dynamic behavior of particles during and after the aerosolization process in DPIs using an LD method (6). Measurements were made in parallel to the Anderson cascade impactor, allowing for a direct comparison between the time-averaged aerodynamic diameter or MMAD given by impactor and the volume particle size distribution reported by in-line laser diffraction. The data was compared in relation to the emitted dose and FPF. This time-resolved analysis differentiated the diffraction patterns produced by the different sections of aerosol cloud such as primary drug particles, aggregates and carrier particles. The cumulative size distribution obtained for different drug powders of salmeterol xinafoate, combined with the computation of the aerodynamic diameter, showed the correct values of FPF. The total emitted dose was in good agreement with the cascade impactor measurements made on the same samples. In a similar study with pMDIs, a simplified theory of particle agglomeration within propellant droplets was tested using a combination of LD (Malvern Spraytec) and TSI APS time-of-flight measurements (98). This study aimed to determine if this mechanism was responsible for the observation that the upper limit deliverable by a pMDI suspension was below 1% w/w. However, the data obtained did not conform to this model; some alternative explanations such as influence of droplet evaporation on the LD measurements and changes in the aerodynamic behaviour of pMDI sprays with increase of the particle concentrations were proposed. Rogueda et al. (97) also used acoustic attenuation spectrometry to study separation phenomena in HFA propellants based on a selection of commercial pMDI suspensions (Ventolin, Flixotide and Salbuhexal). Quantitative data were obtained on the dynamics of flocculation of primary particles before agglomeration into the clusters. After aggregation, the clusters sediment leaving behind the smaller particle, and thus gives rise to apparent decreases in both particle concentration and size. The differences observed between different formulations were attributed to the properties of the primary particles—size and surface characteristics.
In the area of new pharmaceutical technologies, the research challenge is intimately linked with the design of reliable in-line measurements, in order to provide means for scientifically driven process development and optimization. The emphasis is on understanding of the mechanism of particle formation processes leading to process optimization. This principle has, for example, been applied to investigation of processes of spray drying (118,119), crystallization (117,120) and supercritical fluid precipitation (116). For example, laser diffraction and Doppler anemometry in combination with laser interferometry and particle imaging velocimetry (PIV) were used to study the particle formation process by mixing or spraying of organic solutions with supercritical carbon dioxide (116). Special flow-through high-pressure optical cells were built on a modular principle whereby the view area could be moved relative to the nozzle using different lengths of connecting tube sections, thus permitting observation of different flow areas. Such a configuration could also be applied to control the ratio between the feed flows, one of the critical parameters for this process. In a recent study, a very important problem of evaporation kinetics during spray-drying was studied by Dem et al. using a single droplet technique (119). Crystallization of D-mannitol, an excipient for the DPI formulations, was investigated. Information on the evaporation process was obtained through static (elastic) light scattering measurements, while the crystallinity of the resulting material was determined by micro-Raman spectroscopy (nonelastic scattering). By identifying the polymorphic forms generated under different conditions of temperature and relative humidity, a phase diagram of D-mannitol was constructed and the formation of three different polymorphic forms as well as a solution phase at high relative humidity was assigned to distinct regions of process conditions.
The most important application of in-line/online analysis lies in the area of pharmaceutical manufacturing, manifested through the process analytical technology (PAT) initiative. PAT is a collaborative effort between the FDA and industry to facilitate the introduction of new and efficient technologies into the industry. The pharmaceutical manufacturing has been historically based on batch processes followed by laboratory testing and analysis to verify the product quality (121). The majority of such processes have been developed empirically. Automated process controls, process adjustments or improvements were considered difficult for any validated and approved process. However it is quite clear that much advantage is to be gained here by applying the process engineering science. PAT is defined as a system for the analysis and control of manufacturing processes based on timely measurements of critical quality parameters and performance attributes of raw materials and in-process materials. The major goal of PAT is to acquire in-depth knowledge of the process, based on in-process electronic data rather than on laboratory testing of the final product. The definition of the critical parameters, the method of their analysis and control are directly linked to the application of in-line/online techniques. It includes feedback process-control strategies, product-process optimization strategies and information management tools.
Particle size distribution and particle shape, together with some selected chemical and solid-state material properties, usually constitute the critical variables of a pharmaceutical manufacturing process. Typically some relevant mean particle diameters form a part of feedback control loop. In an example of schematic blending process taken from reference (122), the particle sizes of the materials are monitored and controlled at two consecutive process stages prior to tablet compression: first, raw material functionality/dispensing for both active ingredient and excipients and, second, particle size distribution versus the blending time with disintegrant and other excipients (Fig. 11). A major cause of poor content uniformity of solid dosage forms is a mismatch of drug and excipient particle size leading to segregation, especially for low drug to excipient ratio blends (2). The poor content uniformity may result even with ideal mixing if the drug particle size is too large and/or the particle size distribution is too broad. However, reduction of drug particle size can also adversely affect the drug agglomeration and powder flow properties. Therefore there is an optimum range of acceptable drug particle sizes taken as the critical quality parameter. This parameter may also depend on other related properties (e.g., surface, shape, cohesion) of the drug particles as well as those of the excipient materials. Thus the PAT here should be able to provide an information output leading to predictive models and most efficient blending process.

Flow chart showing an example of in-line control of a drug/excipients blending process based on particle size analysis.
Conclusion and Future Prospects
The seemingly inconsistent particle size data, in terms of both accuracy and precision of various instruments, can usually be traced back to the differences in the measured equivalent particle diameters, which may be magnified by the influence of the particle shape and variability of the particle dispersion. The fundamental methodological factors associated with particle shape and aerodynamic particle properties are emphasized in this review. These factors can be taken into account by careful data interpretation and appropriate mathematical description of particle size distribution, in which the conversion between physically different equivalent diameters, e.g., geometric and aerodynamic, is possible and serves as a useful analytical tool. The same instrument and the same method eventually must be used for quality control testing of a given product. However, a cross correlation between different methods is necessary to select a relevant technique and provide in-depth data analysis.
The development of particle sizing instrumentation may be envisaged in the areas of automated size/shape measurements. The application of high-speed systems may be developed for monitoring dynamic processes including more sophisticated analytical systems based on neural nets. This is particularly important for integration of PAT into pharmaceutical manufacturing. A quantitative and consistent measurement of agglomeration phenomena and improvement of the dispersion techniques are required for all classes of particle size instruments. For more comprehensive data interpretation, new computational algorithms tested by empirical models are needed for consistent conversion between different equivalent particle diameters, namely, between the statistical projection diameters given by various imaging instruments and laser diffraction, equivalent volume diameters and aerodynamic particle diameters. It is clear that computational fluid dynamics (CFD) can be applied to predict, with high accuracy, the dynamic shape factors and equivalent aerodynamic (or hydrodynamic) diameters at different flow regimes. This is particularly important in the case of aerosol measurements. An additional problem, with little data presently available, is the preferential particle orientation and characteristic time of particle rotation. Proper control of this problem will provide an understanding of the particle dynamics and enable determination of the particle shape. The particle shape in some cases may vary with the particle size due to different precipitation mechanisms for fine and coarse particle fractions. This problem can only be addressed using high-resolution stream-scanning measurement techniques. Finally, it is clear that as more particle sizing methods become validated and accepted by the pharmaceutical industry, they will be included in Pharmacopoeias and Regulatory Agencies’ guidelines, thus enabling more consistent application of these techniques in pharmaceutics.
References
J. Clarke. Inspired by design: evaluating novel particle production techniques. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, X:287–295 (2006).
D. J. Burgess, E. Duffy, F. Etzler, and A. J. Hickey. Particle size analysis: AAPS workshop report, cosponsored by the Food and Drug Administration and the United States Pharmacopoeia. AAPS J. 6:1–12 (2004).
A. Beckman, D. Shan, A. Ali, W. Dai, S. Ward-Smith, and M. Goldenberg. Micrometer-scale particle sizing by laser diffraction: critical impact of the imaginary component of refractive index. Pharm. Res. 22:518–522 (2005).
T. M. Crowder, J. A. Rosati, J. D. Schroeter, A. J. Hichey, and T. B. Martonen. Fundamental effects of particle morphology on lung delivery: predictions of Stokes’ law and the particular relevance to dry powder inhaler formulation and development. Pharm. Res. 19:239–245 (2002).
R. J. Haskell. Characterization of submicron systems via optical methods. J. Pharm. Sci. 87:125–128 (1998).
B. Y. Shekunov. Production of powders for respiratory drug delivery. In P. York, U. B. Kompella, and B. Y. Shekunov (eds.), Supercritical Fluid Technology for Drug Product Development. New York: Marcel Decker. Drugs Pharm. Sci. 138:247–282 (2004).
B. Y. Shekunov, J. C. Feeley, A. H. L. Chow, H. H. Y. Tong, and P. York. Aerosolisation behaviour of micronised and supercritically-processed powders. J. Aerosol Sci. 34:553–568 (2003).
D. L. French, D. A. Edwards, and R. W. Niven. The influence of formulation on emission, deaggregation and deposition of dry powders for inhalation. J Aerosol Sci. 27:769–783 (1996).
W. I. Li, M. Perzl, J. Heyder, R. Langer, J. D. Brain, K. H. Englmeier, R. W. Niven, and D. A. Edwards. Aerodynamics and aerosol particle deaggregation phenomena in model oral–pharyngeal cavities. J Aerosol Sci. 27:1269–1286 (1996).
C. Bosquillon, C. Lombry, V. Preat, and R. Vanbever. Comparison of particle sizing techniques in the case of inhalation dry powders. J. Pharm. Sci. 90:2032–2041 (2001).
H. M. Courrier, N. Butz, and T. F. Vandamme. Pulmonary drug delivery systems: recent developments and prospects. Crit. Rev. Ther. Drug 19:425–498 (2002).
Center for Drug Evaluation and Research (CDER). Guidance for industry: nasal spray and inhalation solution, suspension, and spray drug products—chemistry, manufacturing, and controls documentation. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Rockville, MD, 2002.
O. S. Usmani, M. F. Biddiscombe, and P. J. Barnes. Regional lung deposition and bronchodilator response as a function of β2-agonist particle size. Am. J. Respir. Crit. Care Med. 172: 1497–1504 (2005).
R. J. Marin. Therapeutic significance of distal airway inflammation in asthma. J. Allergy. Clin. Immunol. 109:S447–S460 (2002).
D. A. Edwards, A. Ben-Jebria, and R. Langer. Recent advances in pulmonary drug delivery using large, porous inhaled particles. J. Applied Physiol. 84:379–385 (1998).
S. P. Duddu, S. A. Sisk, Y. H. Walter, T. E. Tarara, K. R. Trimble, A. R. Clark, M. A. Eldon, R. C. Elton, M. Pickford, P. H. Hirst, S. P. Newman, and J. G. Weers. Improved lung delivery from a passive dry powder inhaler using an engineered PulmoSphere® powder. Pharm. Res. 19:689–695 (2002).
D. A. Edwards, J. Hanes, G. Caponetti, J. Hrkach, A. B. Jebria, M. L. Eskew, J. Mintzes, D. Deaver, N. Lotan, and R. Langer. Large porous particles for pulmonary drug delivery. Science 276:1868–1871 (1997).
K. Koushik, D. S. Dhanda, N. P. S. Cheruvu, and U. B. Kompella. Pulmonary delivery of deslorelin: large porous PLGA particles and HPβCD complexes. Pharm. Res. 21: 1119–1126 (2004).
H. K. Chan and I. Gonda. Physicochemical characterization of a new respirable form of nedocromil. J. Pharm. Sci. 84:692–696 (1995).
B. Shekunov. Nanoparticle technology for drug delivery—from nanoparticles to cutting-edge delivery strategies. Part I. Meeting reports. IDrugs 8:399–401 (2005).
T. S. Weidmann, L. DeCastro, and R. Wood. Nebulization of nanocrystals: production of respirable solid-in-liquid-in-air colloidal dispersion. Pharm. Res. 14:112–116 (1997).
W. G. Kreyling, M. Semmler-Behnke, and W. Moller. Ultrafine particles—lung interactions: does size matter. J. Aerosol Med. 19:74–83 (2006).
P. Lucas, K. Anderson, and J. N. Staniforth. Protein deposition from dry powder inhalers: fine particle multiplets as performance modifiers. Pharm. Res. 15:562–569 (1998).
F. Podczeck. The influence of particle size distribution and surface roughness of carrier particles on the in vitro properties of dry powder inhalations. Aerosol Sci. Tech. 31:301–321 (1999).
M. D. Louey and P. J. Stewart. Particle interactions involved in aerosol dispersion of ternary interactive mixtures. Pharm. Res. 19:1524–1531 (2002).
S. P. Shah and A. Misra. Liposomal amikacin dry powder inhaler: effect of fines on in vitro. AAPS Pharm Sci Tech. 5:1–7 (2004).
F. S. Bennett, P. A. Carter, G. Rowley, and Y. Dandiker. Modification of electrostatic charge on inhaled carrier lactose particles by addition of fine particles. Drug Dev. Ind. Pharm. 25(1):99–103 (1999).
T. H. Ibrahim, T. R. Burk, F. M. Etzler, and R. D. Neuman. Direct adhesion measurements of pharmaceutical particles to gelatine capsule surfaces. J. Adhes. Sci. Technol. 14:1225–1242 (2000).
N. Islam, P. Stewart, I. Larson, and P. Hartley. Effect of carrier size on the dispersion of salmeterol xinafoate from interactive mixtures. J. Pharm. Sci. 93:1030–1038 (2004).
M. J. Clarke, M. J. Tobyn, and J. N. Staniforth. The formulation of powder inhalation systems containing a high mass of nedocromil sodium trihydrate. J. Pharm. Sci. 90: 213–223 (2001).
P. Taylor. Nasal drug delivery. In M. E. Aulton (ed.), Pharmaceutics: The Science of Dosage Form Design, Churchill Livingstone, London, 2002, pp. 489–498.
V. M. Leitner, D. Guggi, A. H. Krauland, and A. Bernkop-Schnurch. Nasal delivery of human growth hormone: in vitro and in vivo evaluation of a thiomer/glutathione microparticulate delivery system. J. Control. Release 100:87–95 (2004).
A. Vila, H. Gill, O. McCallion, and M. J. Alonso. Transport of PLA-PEG particles across the nasal mucosa: effect of particle size and PEG coating density. J. Control. Release 98:231–244 (2004).
J. Varshosaz, H. Sadrai, and R. Alinagari. Nasal delivery of insulin using chitosan microspheres. J. Microencapsul. 21: 761–774 (2004).
R. J. Garmise, K. Mar, T. M. Crowder, C. R. Hwang, M. Ferriter, J. Huang, J. A. Mikszta, V. J. Sullivan, and A. J. Hickey. Formulation of a dry powder influenza vaccine for nasal delivery. AAPS PharmSciTech. 7:E1–E7 (2006).
V. Swaminathan and D. O. Kildsig. Polydisperse powder mixtures: effect of particle size and shape on mixture stability. Drug Dev. Ind. Pharm. 28:41–48 (2002).
T. Shiraishi, A. Sano, S. Kondo, H. Yuasa, and Y. Kanaya. Studies on the granulation process of granules for tableting with a high speed mixer. II. Influence of particle size of active substance on granulation. Chem. Pharm. Bull. 43: 654–659 (1995).
T. Yajima, S. Itai, H. Hayashi, K. Takayama, and T. Nagai. Optimization of size distribution of granules for tablet compression. Chem. Pharm. Bull. 44:1056–1060 (1996).
T. Yao, M. Yamada, H. Yamahara, and M. Yoshida. Tableting of coated particles. II. Influence of particle size of pharmaceutical additives on protection of coating membrane from mechanical damage during compression process. Chem. Pharm. Bull. 46:826–830 (1998).
C. Sun and D. J. W. Grant. Influence of crystal shape on the tableting performance of l-lysine monohydrochloride dihydrate. J. Pharm. Sci. 90:569–579 (2001).
S. Simoes, A. Sousa, and M. Figueiredo. Dissolution rate studies of pharmaceutical multisized powders—a practical approach using the Coulter method. Int. J. Pharm. 127: 283–291 (1996).
J. B. Bressman and C. Reppas. In vitro–in vivo correlations for lipophilic, poorly water-soluble drugs. Eur. J. Pharm. Sci. 11 (Suppl. 2):S73–S80 (2000).
S. Horkovics-Kovats. Characterization of an active pharmaceutical ingredient by its dissolution properties: amoxicillin trihydrate as a model drug. Chemotherapy 50:234–244 (2004).
H. Hu, K. P. Johnston, and R. O. Williams III. Nanoparticle engineering processes for enhancing the dissolution rates of poorly water soluble drugs. Drug Dev. Ind. Pharm. 30:233–245 (2004).
J. Siepmann, H. Kranz, N. A. Peppas, and R. Bodmeier. Calculation of the required size and shape of hydroxypropyl methylcellulose matrices to achieve desired drug release profiles. Int. J. Pharm. 201:151–164 (2000).
I. Caraballo, M. Millan, and A. M. Rabasco. Relationship between drug percolation threshold and particle size in matrix tablets. Pharm. Res. 13:387–390 (1996).
M. J. Fernandez Hervas, M. T. Vela, I. Caraballo, and A. M. Rabasco. Effect of drug particle size on the release behaviour of NaCl-matrix systems. Eur. J. Pharm. Biopharm. 42:208–211 (1996).
A. Miranda, M. Millan, and I Caraballo. Study of the critical points of HPMC hydrophilic matrices for controlled drug delivery. Int. J. Pharm. 311:75–81 (2006).
C. V. Liew, L. W. Chan, A. L. Ching, and P. W. S. Heng. Evaluation of sodium alginate as drug release modifier in matrix tablets. Int. J. Pharm. 309:25–37 (2006).
M. L. Gonzalez-Rodriguez, F. Maestrelli, P. Mura, and A. M. Rabasco. In vitro release of sodium diclofenac from a central core matrix tablet aimed for colonic drug delivery. Eur. J. Pharm. Sci. 20:125–131 (2003).
F. Sadeghi, H. A. Garekani, and F. Goli. Tableting of Eudragit RS and propranolol hydrochloride solid dispersion: Effect of particle size, compaction force, and plasticizer addition on drug release. Drug Dev. Ind. Pharm. 30:759–766 (2004).
B. E. Rabinow. Nanosuspensions in Drug Delivery. Nat. Rev. Drug Discov. 3:785–796 (2004).
B. E. Rabinow. Pharmacokinetics of nanosuspensions. Presentation at Nanotechnology for Drug Delivery Conference, Philadelphia, PA (2005).
S. Ding. Recent developments in ophthalmic drug delivery. PSTT 1:328–335 (1998).
A. C. Williams. Transdermal and Topical Drug Delivery. Pharmaceutical Press, London, 2003.
A. Rolland. Particulate carriers in dermal and transdermal drug delivery: myth or reality? In: A. Rolland (ed.), Pharmaceutical Particulate Cariiers—Therapeutic Applications, Marcel Dekker, New York, 1993, pp. 367–421.
R. Alvarez-Roman, A. Naik, Y. N. Kalia, R. H. Guy, and H. Fessi. Skin penetration and distribution of polymeric nanoparticles. J. Control. Release 99:53–62 (2004).
J. Shim, H. Seok Kang, W. S. Park, S. H. Han, J. Kim, and I. S. Chang. Transdermal delivery of minoxidil with block copolymer nanoparticles. J. Control. Release 97:477–484 (2004).
S. M. Moghimi, A. C. Hunter, and J. C. Murray. Nanomedicine: current status and future prospects. FASEB J. 19:311–330 (2005).
S. S. Feng. Nanoparticles of biodegradable polymers for new-concept chemotherapy. Exp. Rev. Med. Devices 1:115–125 (2004).
D. E. Discher. Nanoparticles, cells, and the body: new lessons from self-assembling polymers. Presentation at Nanotechnology for Drug Delivery Conference, Philadelphia, PA, 2005.
A. Nel, T. Xia, L. Madler, and N. Li. Toxic potential of materials at the nanolevel. Science 311:622–627 (2006).
T. Kaewamatawong, N. Kawamura, M. Okajima, M. Sawada, T. Morita, and A. Shimada. Acute pulmonary toxicity caused by exposure to colloidal silica: particle size dependent pathological changes in mice. Toxicol. Pathol. 33:743–749 (2005).
G. Oberdorster, A. Maynard, K. Donaldson, V. Castranova, J. Fitzpatrick, K. Ausman, J. Carter, B. Karn, W. Kreyling, D. Lai, S. Olin, N. Monteiro-Riviere, D. Warheit, H. Yang, and ILSI Research Foundation/Risk Science Institute Nanomaterial Toxicity Screening Working Group. Principles for characterizing the potential human health effects from exposure to nanomaterials: elements of a screening strategy. Part. Fibre Toxicol. 2:8 (2005).
Food and Drug Administration. Code of Federal Regulations 21, Pt. 1. U.S. Department of Health and Human Services, Food and Drug Administration, Rockville, MD, 1997.
M. Niemann, M. Fusser, and L. Scaffidi. A critical comparison: particle counting with light obscuration and automated Raman microscopy. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, X:529–532 (2006).
Center for Drug Evaluation and Research (CDER). Guidance for industry: metered dose inhaler (MDI) and dry powder inhaler (DPI) drug products, chemistry, manufacturing, and controls. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Rockville, MD, 1998.
Center for Drug Evaluation and Research (CDER). Guidance for industry: bioavailability and bioequivalence studies for nasal aerosols and nasal sprays for local action. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Rockville, MD,, 1999 and 2003.
Center for Drug Evaluation and Research (CDER), and Center for Biologics Evaluation and Research (CBER). Guidance for industry: M4: the CTD—quality questions and answers/location issues. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER), Rockville, MD, 2004.
M. Trunk and C. Weiler. Estimation of the aerodynamic particle size stability of spray-dried powders by thermoanalytical investigations. Proceedings of the Conference on Respiratory Drug Delivery, Palm Desert, CA, IX:385–387 (2004).
ITFG/IPAC Collaboration, CMC Specifications Technical Team, and Particle Size Distribution Working Group. Initial assessment of the ITFG/IPAC aerodynamic particle size distribution database by the CMC Specifications Technical Team of the ITFG/IPAC Collaboration. http://0-www.fda.gov.lilac.une.edu/ohrms/dockets/ac/00/techrepro/3609_rpt2.pdf. Cited 29 Aug 2000.
Inhalation Technology Focus Group/International Pharmaceutical aerosol Consortium on Regulation and Science Tests and Methods Technical Team. Recommendations to the Food and Drug Administration: metered dose inhaler tests and methods in the chemistry, manufacturing, and controls. Draft guidances for metered dose inhalers and dry powder inhalers. Drug Inf. J. 36:549–556 (2002).
F. M. Etzler. Particle size analysis: a comparison of methods. Am. Pharm. Rev. 7:104–108 (2004).
B. H. Kaye, D. Alliet, L. Switzer, and C. Turbitt-Daoust. The effect of shape on intermethod correlation of techniques for characterizing the size distribution of powder. Part 1. Correlating the size distribution measured by sieving, image analysis and diffractometer methods. Part. Part. Syst. Charact. 14: 219–224 (1997).
B. H. Kaye, D. Alliet, L. Switzer, and C. Turbitt-Daoust. The effect of shape on intermethod correlation of techniques for characterizing the size distribution of powder. Part 2. Correlating the size distribution as measured by diffractometer methods, TSI-Amherst aerosol spectrometer and Coulter counter. Part. Part. Syst. Charact. 16:266–272 (1999).
T. E. Corcoran, R. Hitron, W. Humphreys, and N. Chigier. Optical measurement of nebulizer sprays: a quantitative comparison of diffraction, phase Doppler interferometry and time of flight techniques. J. Aerosol Sci. 31:35–50 (2000).
H. G. Brittain, S. J. Bogdanovich, D. E. Bugay, J. DeVincentis, G. Lewen, and A. W. Newman. Physical characterization of pharmaceutical solids. Pharm. Res. 8:963–973 (1991).
J. P. Mitchell, M. W. Nagel, K. J. Wiersema, and C. C. Doyle. Aerodynamic particle size analysis of aerosols from pressurized metered-dose inhalers: comparison of Andersen 8-stage cascade impactor, next generation pharmaceutical impactor and model 3321 aerodynamic particle sizer aerosol spectrometer. AAPS Pharm Sci Tech. 4:1–9 (2003).
M. L. Thatcher, B. A. S. Brown, B. J. Gabrio, and M. Johnson. A rapid protein particle size measurements method for metered dose inhaler development: novel use of the small scale powder disperser and aerodynamic particle sizer. Presented at Annual AAPS Meeting, Denver, CO, 21–25 October 2001.
Y. S. Cheng, E. B. Barr, I. A. Marshall, and J. P. Mitchell. Calibration and performance of an API aerosizer. J. Aerosol Sci. 24:501–514 (1993).
P. A. Baron. Calibration and use of the aerodynamic particle sizer (APS3300). Aerosol Sci. Tech. 5:55–67 (1986).
T. Allen. Particle Size Measurement. Powder Sampling and Particle Size Measurement, vol. 15. Chapman & Hall, London, 1997.
R. Davies. In M. Grayson (ed.), Kirk-Othmer Encyclopedia of Chemical Technology, 3rd ed. John Wiley, 1982, p. 528.
G. Nichols, S. Byard, M. J. Bloxham, J. Botterill, N. J. Dawson, A. Dennis, V. Diart, N. C. North, and J. D. Sherwood. A review of the terms agglomerate and aggregate with a recommendation for nomenclature used in powder and particle characterization. J. Pharm. Sci. 91:2103–2109 (2002).
B. Y. Shekunov, P. Chattopadhyay, J. Seitzinger, and R. Huff. Nanoparticles of poorly water-soluble drugs prepared by supercritical fluid extraction of emulsions. Pharm. Res. 23: 196–204 (2006).
N. Y. K. Chew, B. Y. Shekunov, H. H. Y. Tong, A. H. L. Chow, C. Savage, J. Wu, and H. K. Chan. Effect of amino acids on the dispersion of disodium cromoglycate powders. J. Pharm. Sci. 94:2289–2301 (2005).
B. H. Kaye. Making and characterizing nanopowders. Proceedings of PBS, Chicago, 2001.
D. J. Burgess, D. J. A. Crommelin, A. S. Hussain, and M.-L. Chen. Assuring quality and performance of sustained and controlled release parenterals: EUFEPS Workshop report. AAPS Pharm Sci. 6:1–12 (2004).
J. C. Feeley, P York, B. S. Sumby, H. Dicks, and M. Hanna. In vitro assessment of salbutamol sulphate prepared by micronisation and a novel supercritical fluid technique. Drug Delivery to the Lungs IX:196–199, (1998).
B. Y. Shekunov, P. Chattopadhyay, D. Yim, D. Cippola, and B. Boyd. AERx aerosol properties of drug–lipid nanosuspensions produced using supercritical extraction of emulsion (SFEE). Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, 10:609–612 (2006).
N. B. E. Sawyer, S. P. Morgan, M. G. Somekh, C. W. See, E. Astrakharchik-Farrimond, and B. Y. Shekunov. Amplitude and phase microscopy for sizing of spherical particles. Appl. Opt. 42:4488–4499 (2003).
W. Smith and S. Murdande. Nanosizing for improving the delivery of drugs with poor solubility (in press). Pharm. Res. (2006).
O. Klueva, M. P. Nelson, P. J. Treado, and A. M. Waligorski. An ingredient-specific method for particle size characterization of corticosteroid nasal sprays. Proceedings of the Conference Particles 2006: medical/biochemical, diagnostic, pharmaceutical and drug delivery applications of particle technology. Orlando, FL, pp. 101–102 (2006).
P. M. Young, D. Cocconi, P. Colombo, R Bettini, R. Price, D. F. Steele, and M. J. Tobyn. Characterization of a surface modified dry powder inhalation carrier prepared by “particle smoothing”. J. Pharm. Pharmacol. 54:1339–1344 (2002).
N. Gabas, N. Niquily, and C. Laguerie. Response of laser diffraction particle sizer to anisometric particle. Part. Part. Syst. Charact. 11:121–126 (1994).
S. Röthele, H. Naumann, and M. Heuer. The application of Fraunhofer diffraction below 1 μm to particle size analysis from 0.1μm to 2000μm. Proceedings of the 7th European Symposium on Particle Characterisation, Nürnberg, Germany, 1998.
P. G. Rogueda, V. Buckin, and E. Kudryashov. Size and concentration monitoring of HFA suspensions. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, X:453–456 (2006).
P. G. Rogueda. Particle aggregation in aerosol clouds. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, X:449–452 (2006).
B. Y. Shekunov, P. Taylor, and J. G. Grossmann. Structural phenomena in hydrogel drug systems. J. Cryst. Growth 198–199:1335–1339 (1999).
B. Y. Shekunov, J. C. Feeley, A. H. L. Chow, H. H. Y. Tong, and P. York. Physical properties of supercritically-processed and micronized powders for respiratory drug delivery. KONA Powder Part. 20:178–187 (2002).
D. F. Nicoli, D. C. McKenzie, and J. S. Wu. Application of dynamic light scattering to particle size analysis of macromolecules. Am. Lab. 23:32–40 (1991).
J. Weyermann, D. Lochmann, C. Georgens, I. Rais, J. Kreuter, M. Karas, M. Wolkenhauer, and A. Zimmer. Physicochemical characterisation of cationic polybutylcyanoacrylat-nanoparticles by fluorescence correlation spectroscopy. Eur. J. Pharm. Biopharm. 58:25–35 (2004).
W. Schrof, J. Klingler, S. Rozouvan, and D. Horn. Raman correlation spectroscopy: a method for studying chemical composition and dynamics of disperse systems. Phys. Rev. E 57:R2523–R2526 (1998).
I. A. Marshall, J. P. Mitchell, and W. D. Griffiths. The behaviour of regular-shaped non-spherical particles in a TSI aerodynamic particle sizer. J. Aerosol Sci. 22:73–89 (1991).
W. R. Foss and N. Egilmez-Reynolds. Assessment of the API AeroSizer for measuring the particle size distribution of dry powder aerosols. Proceedings of the Conference on Respiratory Drug Delivery, Palm Harbor, FL, VII:407–410 (2000).
A. Kamiya, M. Sakagami, M. Hindle, and P. R. Byron. Aerodynamic sizing of metered dose inhalers: an evaluation of the Andersen and next generation pharmaceutical impactors and their USP methods. J. Pharm. Sci. 93:1828–1837 (2004).
P. Mikkanen, M. Moisio, J. Ristimaki, T. Ronkko, J. Keskinen, and T. Korpiharji. Measuring DPI charge properties using ELPI. Proceedings of the Conference on Respiratory Drug Delivery, Palm Desert, CA, IX:465–467 (2004).
J. C. Keil, R. Kotian, and J. Peart. Using and interpreting aerosol electrostatic data from electrical low pressure impactor. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, X:605–608 (2006).
H. H. Y. Tong, B. Y. Shekunov, P. York, and A. H. L. Chow. Thermal analysis of trace levels of polymorphic impurity in salmeterol xinafoate samples. Pharm. Res. 20:1423–1429 (2003).
W. Witt, U. Köhler, and J. List. Direct imaging of very fast particles opens the application of the powerful (dry) dispersion for size and shape characterization. PARTEC 2004, Nürnberg.
A. H. Boer, D. Gjaltema, W. Witt, and H. W. Frijlink. The use of laser diffraction technique for the characterisation of the aerosol cloud from inhalation device. Proceedings of the Conference on Respiratory Drug Delivery, Palm Harbor, FL, VII:585–588 (2000).
D. R. Roberts and F. J. Romay. Relationship of stage mensuration data to the performance of new and used cascade impactors. J. Aerosol Med. 18:396–413 (2005).
J. E. Brockmann and D. J. Rader. APS response to nonspherical particles and experimental determination of dynamic shape factor. Aerosol Sci. Tech. 13:162–172 (1990).
R. P. Chhabra, L. Agarwal, and N. K. Sinha. Drag on non-spherical particles: an evaluation of available methods. Powder Technol. 101:288–295 (1999).
G. H. Ganser. A rational approach to drug prediction of spherical and nonspherical particles. Powder Technol. 77:143–152 (1993).
J. Baldyga, M. Henczka, and B. Y. Shekunov. Fluid dynamics, mass transfer, and particle formation in supercritical fluids. In P. York, U. B. Kompella, and B. Y. Shekunov (eds.), Supercritical Fluid Technology for Drug Product Development, Marcel Dekker Series, 2004, 91–157.
P. Mougin and D. Wikinson. In situ measurement of particle size during the crystallization of l-glutamic acid under two polymorphic forms: influence of crystal habit on ultrasonic attenuation measurements. Cryst. Growth Des. 2:227–234 (2002).
I. Zbicinski, C. Strumillo, and A. Delag. Drying kinetics and particle residence time in spray drying. Dry. Technol. 20: 1751–1768 (2002).
C. Dem, M. Egen, M. Krüger, and Juürgen Popp. Understanding the spray design process through single droplet investigations. Proceedings of the Conference on Respiratory Drug Delivery, Boca Raton, FL, 10:257–266 (2006).
A. R. Heath, P. D. Fawell, P. A. Bahri, and J. D. Swift. Estimating average particle size by focused beam reflectance measurement (FBRM). Part. Part. Syst. Charact. 19:84–95 (2002).
L. X. Yu, R. A. Lionberger, A. S. Raw, R. D’Costa, H. Wu, and A. S. Hussain. Applications of process analytical technology to crystallization processes. FDA CDER, Rockville, MD, 2003, pp 1–46.
D. C. Watts (2004). Process analytical technology (PAT): what’s in a name?http://www.fda.gov/cder/OPS/PATCommissionerSem2004/frame.htm.
Acknowledgment
One of the authors (Henry H. Y. Tong) would like to acknowledge the financial support of Macao Polytechnic Institute [Project No. RP/ESS-7/2005].
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shekunov, B.Y., Chattopadhyay, P., Tong, H.H.Y. et al. Particle Size Analysis in Pharmaceutics: Principles, Methods and Applications. Pharm Res 24, 203–227 (2007). https://doi.org/10.1007/s11095-006-9146-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-006-9146-7