
Abstract
CanRisk is a tool to assess the seismic vulnerability of buildings in Canada. CanRisk models that support the individual evaluation of reinforced concrete, masonry, steel, and timber-frame buildings have been recently developed. Herein, a new model for CanRisk is presented that quantifies an individual’s risk of earthquake injury, the number of injuries, and provides an injury profile of life-threatening injuries at the building scale. The model uses an evidence-based and multi-disciplinary approach to identifying risk factors that affect an individual’s likelihood of being injured in an earthquake. The model implements fuzzy synthetic evaluation to quantify seismic risk, combines Hazus methodology with methodology presented herein to estimate number of injuries, and uses a decision matrix to generate the injury profiles. The model is designed to include the ability to test the benefits of mitigation strategies such as the retrofit of operational and functional components and the implementation of earthquake safety campaigns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Earthquake casualties are the consequences of the intensity of ground shaking, earthquake resistance of buildings and its operational and functional components (OFC), as well as human behaviour. Seismic events are unique and dynamic with varying causal factors leading to injuries. As such, it is difficult to estimate earthquake-related injuries. In order to underpin casualty loss estimation methodologies and better support informed decision making in emergency management, detailed information of risk factors from case studies must be compiled and studied. Identifying and understanding the causative factors of injuries can aid in the development of effective mitigation and preparedness strategies, and reduce the overall number of injuries.
The purpose of the CanRisk tool is to assess the seismic vulnerability of buildings in Canada. This seismic assessment tool integrates building vulnerability, site seismic hazard, and building exposure from detailed building-specific engineering data. CanRisk has a modular architecture and can therefore incorporate any number of modules to evaluate the risk of various aspects to the built environment. It currently includes modules to evaluate the earthquake resistance of reinforced concrete buildings (Tesfamariam and Saatcioglu 2010), unreinforced masonry buildings (Elsabbagh 2013), timber-frame buildings (Komsari 2014), steel buildings (Saatcioglu personal communication 2014), and the injury module described herein. CanRisk utilizes detailed structural parameters in its evaluation of building performance which leads to a more accurate estimation of damageability (degree of damage to a building; a value between 0 and 1).
This article presents the rationale and development of an evidence-based injury model for the CanRisk program. The purpose of the CanRisk earthquake injury model is to quantify the risk to injury, the number and distribution of injuries, and to provide a profile of life-threatening injuries at the building scale. The model outputs can equally apply to a single unit within a building or to an entire structure and are dependent on the earthquake preparedness decisions of the ‘owner.’ For example, the owner of a high-rise 50 + unit apartment building may choose not to engage in any earthquake preparedness activities or may choose to engage in mitigation strategies such as sending an informative brochure to all units in the building. In this case, the building owner can, to some extent, reduce the unit dwellers’ risk of being injured in an earthquake. The overall aim of the model is to facilitate informed decision making in emergency management (EM) with the ability to test potential mitigation and preparedness strategies, and to provide loss estimations that will aid in the development of realistic earthquake scenarios. This injury model is designed for the CanRisk program, but its underlying evidence-based theory has international application.
1.1 Risk terminology
Risk can be generally defined as the damage/impact that will be caused by a future earthquake in a given area, and is the product of hazard, vulnerability, and exposure. In this paper, risk is an inclusive and broad term that refers to a qualitative degree of exposure and vulnerability to a hazard rather than expressing risk as a probability. The output of the ‘Risk to Injury’ model denotes the likelihood of being injured in an earthquake. Risk factors are attributes and/or characteristics of individuals, groups or communities that may develop negative outcomes such as factors that may increase an individual’s likelihood of being injured.
2 Rational
The three primary factors that influence earthquake injuries are (1) earthquake shaking characteristics (e.g., magnitude, attenuation, amplification), (2) the performance of structural building systems (e.g., seismic force resisting system, building design, quality of construction, irregularities, year of construction) and their OFCs (e.g., architectural, mechanical/electrical, building contents), and (3) social factors (e.g., patterns of human activity, earthquake awareness/preparedness, and human behaviour) (Alexander 1996).
Firstly, the majority of earthquake injuries occur during ‘felt’ ground motions. In general, the prevalence of injury is greater closer to the rupture plane and decreases with epicentral/hypocentral distance. Peek-Asa et al. (2003) found that for every ~ 1 km increase in hypocentral distance, there was a 10 % decrease in the risk to injury. However, isolated concentrations of injuries have been documented and are commonly related to soil conditions and poor building resistance. In Canada, seismic wave amplification from soft soil conditions is well documented. For example, approximately 95 % of reported damage during the 1988 M5.9 Saguenay earthquake occurred on soft soils, up to distances of 350 km (Paultre et al. 1993; Lamontagne 2002).
Secondly, international case studies clearly establish that the structural aspects of the built environment are the most notorious mechanism of earthquake casualties. Partial or complete building collapse is the primary cause of serious and fatal injuries. While the likelihood of collapse is lower in regions in which modern seismic safety provisions are incorporated into building codes, the consequences can be catastrophic (e.g., Meadow Apartments in the 1994 M6.7 Northridge earthquake, the Canterbury Television building in the 2011 M6.3 Christchurch earthquake). Structural failure is the primary cause of fatal injuries in North American earthquakes but constitute <10 % of non-fatal injuries (e.g., Durkin et al. 1991a). Building performance during ground motion, and therefore its damageability, is a primary contributor to the risk of being injured. Building types also play a role in the risk of being injured and the consequent distribution of injuries (Noji et al. 1990; Coburn and Spence 2002). Additionally, building types can also influence the progression of injury severity due to degree of cavitation after a collapse and search and rescue (SAR) capabilities (see Scawthorn 1989; Coburn and Spence 2002).
In buildings that are more structurally resilient to lateral forces, operational and functional components (OFCs) are more likely to cause injuries (Ohashi and Ohta 1984; Durkin 1985). OFCs are classified as (1) architectural and non-structural, (2) mechanical, electrical and plumbing, or (3) general building content. In North American earthquakes, a high proportion of damage is due to OFCs (Bruneau and Lamontagne 1994; Coburn and Spence 2002). For example, during the 1994 M6.7 Northridge earthquake, OFCs were responsible for approximately five fatalities and over 7000 injuries (McKevitt et al. 1995). Therefore, the primary factor of injury prevention is the development of superior building codes that are strictly enforced (Lomnitz 1970; Coburn and Spence 2002) as well as active and timely implementation of structural and non-structural retrofits (Bruneau 1990; Mitchell et al. 1995).
Thirdly, human behaviour and choices made before, during, and after earthquake shaking influence the risk of being injured. Previous earthquake experience influences the personal decision-making process in many ways, such as taking proactive steps to increase the safety of one’s family (securing heavy objects, family emergency planning and drills), and providing an experiential knowledge on the psychological/psychosocial intensity of an earthquake event (Dooley et al. 1992; Russell et al. 1995; Shaw et al. 2004; Nguyen et al. 2006).
In earthquakes of all magnitudes, there is generally enough time to react before peak motion (Lomnitz 1970; Armenian et al. 1992; Roces et al. 1992; Durkin and Thiel 1992). During North American earthquakes, one of the common reactions is to rapidly exit a building during shaking. Additionally, being among the ‘unfamiliar,’ that is, in an unfamiliar place or with unfamiliar people at the time of the earthquake can foster stress and a greater urge to flee (Mawson 2005). Such reaction increases an individual’s risk to injury from falling OFCs such as masonry elements and cladding/glass (Du Ree 1941; Durkin et al. 1991a). However, based on recent case studies of Californian earthquakes, falling is the most common mechanism of injury (Durkin et al. 1991a; Peek-Asa et al. 1998; McArthur et al. 2000). In developed regions, taking protective cover (‘Drop, Cover, and Hold On’) is the most prudent action and best practice during earthquake shaking. These actions can significantly reduce the risk of serious and fatal injuries (Durkin and Murakami 1988). Therefore, active knowledge in earthquake safety does play a major role in the reduction in earthquake injuries.
Other influential risk factors are time of day and ambient air temperature. Research reveals that the time of day of an earthquake influences the risk to injury because of human activities (e.g., Tierney 1990; Zuccaro and Cacace 2011). In North America and other developed regions, daytime earthquakes will likely produce more casualties due to mass evacuations (evacuations from high-rise buildings, shopping malls, theatres, etc.), traffic light failure, road damage, and falling OFCs (Peek-Asa et al. 1998). Time of day is also an influential factor of life-threatening injuries because it is an indicator of body positioning. For example, head and spinal injuries are more common during daytime earthquakes when the occupant is sitting, standing, or leaning with their head and back exposed to falling OFCs (Maruo and Matumoto 1996).
Ambient air temperature directly affects an individual’s core body temperature. Core body temperature characterizes two important factors of risk to injury: (1) exposure and the development of hypothermia and (2) the development and progression of crush syndrome. Hypothermia occurs when the core body temperature decreases due to ambient air temperature or other stimuli such as severe trauma or hemorrhagic shock. A normal body temperature is ~37 °C, and mild hypothermia develops as the body temperature decreases below 36 °C. Symptoms of severe hypothermia begin to develop at ~33 °C and can greatly compound an individual’s health. Additionally, case studies (e.g., Mulvey et al. 2008) and animal research (e.g., Takagi et al. 2011; Schaser et al. 2006) suggest that core body temperature may also influence the development of crush syndrome and/or similar clinical signs. However, more data and medical research are needed to find a definitive correlation between core body temperature and the development/progression of crush syndrome.
3 Methodology
The CanRisk injury model is a proactive (mitigation and preparedness) tool for decision makers and is most useful at the household to municipal levels, but has application up to the national level. It serves three main functions: (1) to evaluate the risk/likelihood of being injured, (2) to profile life-threatening injuries (a short summary of injury details), and (3) to estimate the number and distribution of injuries by both building and non-building factors (Fig. 1). Additionally, the model is designed to evaluate the outcomes of specific mitigation decisions, such as how OFC retrofits and earthquake safety/preparedness strategies affect the risk to injury. The primary framework of the injury model uses fuzzy synthetic evaluation (FSE) to determine the likelihood of being injured. Life-threatening injury profiles are evaluated using a decision matrix, and the estimation of number of injuries is calculated using a combination of Hazus methodology (FEMA 2012) and the CanRisk ‘Risk to Injury’ FSE output.

Conceptual framework of the CanRisk injury model (Ploeger 2014)
3.1 Risk factors and data
The injury model risk factors are evidence-based and derived from case studies and reports (e.g., academic literature/peer-reviewed journals, government- and agency-issued reports) which provide qualitative evidence of the indicators of risk. For example, ‘lessons learned’ offer constructive comments on the challenges and successes of the earthquake impact, such as the importance of OFC retrofits (e.g., McKevitt et al. 1995) or consequences of OFC failure (Du Ree 1941). The derived key risk factors are damageability, building type, OFC hazards, familiarity, previous earthquake experience, time of day, ambient air temperature and earthquake safety education. Further discussion concerning the aforementioned risk factors can be found in Ploeger (2014).
Before the risk factors were incorporated into the model, they were treated in a manner to best represent how that particular factor influences the likelihood of being injured. The simplest treatments were (1) time of day where the input is either day or night and (2) damageability as this is the direct output of the CanRisk engineering models. A more involved treatment was capturing previous earthquake experience which entailed a GIS approach and implemented an adapted Injury Severity Score (ISS) procedure which is used in emergency medicine. A summary of the treatment of data (risk factors) is presented in Table 1; more details can be found in Ploeger (2014).
Ground motion is not explicitly included in the CanRisk injury model because it is already considered in the CanRisk engineering models and incorporated in the damageability risk factor. In the CanRisk engineering models, seismic hazard values are embedded in the hazard module in the form of spectral accelerations obtained from the uniform hazard spectra (UHS) specified in the National Building Code of Canada for each municipality in Canada. These are the current hazard values provided by the Geological Survey Canada which reflect the expected seismicity in different parts of the country to be used for analysis and design of buildings. The hazard values are modified (i.e., amplified or de-amplified) by incorporating site soil conditions to reflect the effects of local soil conditions on buildings, which can be quite significant. The hazard values, as modified for local soil conditions, are used in the CanRisk engineering modules, which provide information on the type, geometry and structural characteristics of buildings, while also reflecting the damage potential of non-structural elements present in the building. With this and other data provided in the engineering modules, the fundamental period of the building is computed, whereupon the corresponding spectral value can be obtained and combined with the effects of building vulnerabilities (structural irregularities, year of construction, quality of construction, building type, etc.). The final output of the engineering modules is damageability which is then input in the CanRisk injury module.
The synthesis and analysis of data from medical case studies also support risk factors. An earthquake injury dataset consisting of 44 international case studies of 19 earthquakes was compiled. The injury dataset represents over 50,000 individual injuries and was coded to include information on: (a) time of day; (b) ICD-10 taxonomy (International Classification of Diseases); (c) body location of injury (upper body, trunk or lower body); (d) inferred severity (minor, serious and life-threatening); and (e) most frequently observed damage state of buildings in the case study region. The Wilcoxon signed-ranked test was used in R (R version 3.0.1) to determine the significant differences in proportions of injury characteristics within the datasets. As expected, many results are statistically marginal (p value ≤0.25) due to the nature of the quantification of earthquake injuries in case studies such as their inherent incomplete and ambiguous nature, and the lack of published datasets. However, the stronger observations show effects/patterns of injuries that are further contextualized and supported by medical insights from case studies. These stronger observations (Table 2) are used in the CanRisk injury model to support the inclusion of parameters, membership functions, and weights.
3.2 Evaluation of ‘Risk to Injury’ and fuzzy synthetic evaluation
The CanRisk ‘Risk to Injury’ model is designed to incorporate two broad concepts that contribute to injury, and these are (1) the influence of building structural and OFC damage factors, and (2) non-building influences, such as various psychological/psychosocial, environmental and social factors.
Fuzzy logic is a method that can systemically handle the inherent limitations of disaster-related risk such as limited, ambiguous or deficient data and concepts. Fuzzy synthetic evaluation (FSE) uses a hierarchical approach and calculates a single output from multiple quantitative and qualitative inputs as well as expert judgment. FSE is an ideal methodological approach for this study as data are both qualitative and quantitative, and datasets on earthquake injuries are limited and incomplete; therefore, considerable expert judgment is required. FSE is also the basis of the engineering models of the CanRisk program.
The hierarchical structure of the FSE method provides a logical order of the casual relationships between the risk factors (Elsabbagh 2013). Membership functions and a rule base are established for each pair of risk factors. The aggregation of arguments continues up the hierarchy until they are incorporated into one final pairing, in this case the building influence and non-building influence. As with all other pairings, the output is a crisp value between 0 (low likelihood) and 1 (high likelihood); the final pairing outputs the likelihood of being injured. An overview of the hierarchical framework of the ‘Risk to Injury’ FSE and its risk factors is presented in Fig. 2.

Overview of the hierarchical framework of the ‘Risk to Injury’ FSE (Ploeger 2014)
The CanRisk injury model was constructed in the MathWorks ® MATLAB environment using the Fuzzy Logic Toolbox. Each risk factor was assigned a membership function with a numerical range which can also be described linguistically (Table 3). Membership functions are a necessary step for fuzzification; the process where input variables are transformed into the fuzzy sets. A fuzzy set consists of membership functions where an input factor can have partial membership in multiple ranges. Once risk factors are paired and assigned membership functions, IF-THEN rules are created to evaluate the relationship between each factor. Finally, de-fuzzification involves the evaluation of the processed fuzzy values and generates a single numeric output. An overview of the analytic workflow of the ‘Risk to Injury’ FSE is presented in Fig. 3.

Analytic workflow of the ‘Risk to Injury’ FSE
3.3 Life-threatening injury profile
Life-threatening injuries create an exceptional demand on medical resources including medical equipment, pharmaceuticals and specialists. They are also of interest to emergency managers, especially those responsible for medical care facilities/hospitals and paramedic operations because of their unique requirements. For these reasons, life-threatening head/spinal, trunk, orthopedic, and crush injuries were selected for evaluation.
The injury profiles are constructed using a decision matrix of the varying risk factors, these are earthquake safety education, time of day, OFC hazards/retrofit decisions, damageability, air temperature, and building type. Each risk factor has various parameters to describe each state (e.g., active earthquake safety education) which are ordered from most influential to least influential (Table 4), weighted and normalized (Ploeger 2014). Some of these ‘orders’ are straightforward such as education, OFC hazards and building type (i.e., active training is more effective than no safety education); however, the time of day, damageability, and temperature parameters vary because they may influence some types of injuries more than others (e.g., orthopedic injuries are more likely to occur during the day and crush injuries are more likely at night). Ranking and weighting these factors are based on qualitative and quantitative evidence, and expert judgment. For example, life-threatening head/spinal injuries have four associated risk factors; the most influential is OFC hazards/retrofit decisions and the least is earthquake safety education. Therefore, the OFC hazards are multiplied by four, while earthquake safety education is multiplied by one. The sum of the risk factors for each type of injury will determine if the risk of life-threatening head/spinal, trunk, orthopedic, and crush injuries is low, moderate, or high.
3.4 Estimation of number and distribution of injuries
CanRisk’s estimation of the number and distribution of injuries combines Hazus methodology with the aforementioned ‘Risk to Injury’ FSE output. Hazus casualty methodology utilizes North American datasets to calculate injuries; however, it only considers injuries due to structural and OFC damage. Hazus methodology calculates the expected number of injuries using casualty rate tables arranged by damage state and building type (see FEMA 2012 Chapter 13). However, considering that the primary cause of injury in North American earthquakes is related to non-building factors such as attempting to rapidly exit a building and falling, the CanRisk injury model attempts to capture these additional injuries that are not included in the traditional Hazus methodology. Therefore, the CanRisk injury model includes not only Hazus casualty rate tables but also incorporates the FSE output of the ‘Risk to Injury’ as an indicator for non-building-related injuries.
In order to determine the likely range of non-building-related injuries, the analysis of a ‘mechanism of injury’ dataset was required. This dataset was compiled and represented 21 international case studies of 17 earthquakes. Of these, only 16 case studies were selected for analysis because they contained fall-related (non-building-related) injuries. A histogram of the proportions revealed a non-normal distribution, and the range of possible fall injuries was determined by the 10th (0.096) and 90th (0.502) percentiles. However, as seen in previous earthquakes [e.g., 1964 M7.6 Niigata, Japan earthquake (Ohashi and Ohta 1984), and the 1994 M6.7 Northridge earthquake (Peek-Asa et al. 1998; McArthur et al., 2000; Mahue-Giangreco et al. 2001)], fall-related injuries can constitute more than 50 % of all injuries. Equations 1a and 1b denote the calculation of the number of non-building injuries in the CanRisk model where upper (a) and lower (b) equations represent the percentile bounds:
where \(NInj_{\text{nonbldg}}\) is the total number of individuals with non-building (e.g., fall-related) injuries, \({\text{Risk}}_{\text{Inj}}\) is the CanRisk FSE output of ‘Risk to Injury’ (0–1), \(N_{\text{occupants}}\) is the number of occupants within the building, and \(NInj_{\text{Hazus}}\) is the total number of building-related injuries as determined by the Hazus casualty rate tables (FEMA 2012).
It is acknowledged that the above equations may seem disproportional as the fewer number of people injured by building factors (Hazus methodology) increases the chance of being injured by non-building factors (‘Risk to Injury’ multiplier). In most cases, the injuries sustained by the onset of building and OFC failure supersede those from non-building factors. For example, a serious Falling on Outstretched Hand(s) (FOOSH) injury is typically not comparable to the severity and medical resources needed to treat a crush injury. However, in earthquakes with few building failures as often seen in North America, non-building injuries like falls can represent a major stressor on medical and emergency response resources.
The distribution of fall/non-building injuries in each severity class (minor, serious, and life-threatening) is determined by trends observed in the injury dataset. All injuries consistent with FOOSH/fall-related characteristics were extracted from the injury dataset. Severity 1 (minor) and severity 2 (serious) injuries included all arm, shoulder girdle, and leg injuries; minor injuries also included all general sprains and strains. Severity 3 (life-threatening) injuries included the entire severity 3 orthopedic injury dataset which does not include crush injury. It is assumed that the majority of the above injuries were sustained from non-building factors (i.e., tripping, falling or jumping). Under these assumptions, an ordinal logistic regression using R (R version 3.0.1) was used to determine the probabilities of sustaining a minor, serious or life-threatening non-building injury (Table 5). Fatal injuries are not accounted for as these types of injuries were not included in the injury dataset and therefore could not be calculated. The ordinal logistic regression included two categories, most observed damage and earthquake safety education. The former was selected because more damage leads to additional obstacles during and after shaking, and increases an individual’s chance of tripping. The latter was selected because earthquake education is an indicator if an individual will attempt to rapidly exit a building. Although no fatal fall injuries were included in the ordinal logistic regression, these types of injuries are possible (McKevitt et al. 1995). The total number of injuries per unit (e.g., building) is calculated by the total number of non-building injuries (Eqs. 1a, 1b) and the total number of building-related injuries.
An additional feature of the CanRisk injury model is a graphical output of critical exposure. The output denotes the approximate number of hours until critical exposure; that is, when the core body temperature drops below 33 °C. A thermometric model was utilized to show the relationships between ambient air temperature and core body temperature. Details on the ancillary thermometric model are not discussed in this paper; however, the model is adapted from Iampietro (1961), Bell et al. (1992), and ISO 8996 (2004).
3.5 Limitations in model approach
The computation of earthquake risk is a complex task, and for this reason, it is exceptionally difficult to model. Assumptions and limitations are intrinsic to the development of loss estimation and injury risk methodology, but these can enlighten issues of reproducibility as well as challenges within this research field. The following are some of the major assumptions/limitations used in this model:
-
1.
Traditional casualty loss estimation methodology is empirical and frequently based on previous experience (e.g., Fulford et al. 2002; Spence et al. 2011; FEMA 2012). In North America, there are very few contemporary earthquakes and even fewer in Canada with which to assemble a comprehensive injury database. Even international case studies offer few relevant earthquake datasets. The lack of these datasets and the reporting of earthquake injuries is attributable to the lack of standardized methods to collect data, the interpretations of injury severity, lack of epidemiological data of the patient, and the chaotic nature of post-earthquake situations (Alexander 1985; Durkin 1985; Alexander 1996; Peek-Asa et al. 1998; Ramirez and Peek-Asa 2005; Auf der Heide 2006; Stallings 2002; Ardagh et al. 2012).
-
2.
An inherent characteristic of loss estimation research is the lack of available data and having to wait for earthquakes to occur to test a model. Tools can be calibrated, validated, and refined with the use of empirical data. Calibration and validation of earthquake loss estimation models have utilized historical data (e.g., Frolova et al. 2011; Trendafiloski et al. 2011a, b) and newly acquired data from recent and relevant earthquakes (e.g., Zuccaro and Cacace 2011; Astoul et al. 2013; Sedan et al. 2013). However, many models (e.g., Jones and Dhu 2002; Scheulen et al. 2009) including Canadian models (e.g., Ploeger 2008) still require further data for validation.
-
3.
The statistical analysis of the injury dataset yielded few statistically significant results (p value ≤0.05). However, in this study, statistical tests were used to help identify effects/trends rather than making a definitive statement of reality (Nuzzo 2014). All identified observations (Table 2) were also supported by firsthand/primary qualitative observations made in medical case studies and reports.
-
4.
Limitations in the available qualitative and quantitative data lead to assumptions and generalizations in the translation of the datasets to risk factors. An example to demonstrate a generalization of the coded dataset is that all minor injuries included sprains, strains, contusions, open wounds, and soft tissue injuries, but some of these ‘assumed minor injuries’ may have been serious or life-threatening in reality.
-
5.
An unanticipated trend was observed in ordinal logistic regression results of the probabilities of minor, serious, and life-threatening non-building injuries (Table 5); the chances of minor injuries increase when earthquake safety education is low. There are three possibilities for this trend. (1) In the dataset used for the ordinal logistic regression analysis, light damage and low earthquake education were represented by two earthquakes, one of them was the 2011 M6.3 Christchurch earthquake. Research and data reporting from this earthquake have been exemplary, and may offer better recording/reporting of earthquake injuries (minor to life-threatening) and therefore skewed data toward minor injuries. All three earthquakes representing light damage and high earthquake education were twentieth-century earthquakes from California (1989 Loma Prieta, 1992 Landers, and 1994 Northridge earthquakes). Researchers have noted that a significant number of minor injuries were likely treated but not reported (Durkin and Thiel 1992; McKevitt et al. 1995; McArthur et al. 2000). (2) Moderate damage is classified as primarily structural failures of moderate material (e.g., timber-frame) and/or low-rise buildings. Only one earthquake represented moderate damage and high earthquake education which was the 1995 M6.9 Great Hanshin (Kobe) Japan earthquake. This particular earthquake had numerous timber-frame building collapses. Most earthquakes with moderate damage and low earthquake education had URM building collapses. It is possible that there is a fundamental difference in the epidemiology of injuries with these conditions and therefore cannot be compared. For example, perhaps life-threatening orthopedic injuries in URM collapses are less survivable which leads to fewer injuries being reported, while these types of injuries in timber-frame collapses have higher chances of survival. Other fundamental differences are that injuries from developing and developed regions cannot be compared due to different post-earthquake medical treatment and advanced care capacities. (3) Another possibility could be that one or both of the categories (damage and earthquake safety education) do not influence non-building/‘fall-related’ injuries, though this possibility would oppose observations from international earthquake injury literature.
-
6.
In Eqs. 1a and 1b, the 0.096 and 0.502 values were determined by the ‘mechanism of injury’ dataset in which all case studies with documented fall-related injuries were selected and used to construct a histogram. This variable was calculated using the 10th and 90th percentile which can change when newer data become available. Additionally, these variables do not consider the unique circumstances where significantly more fall-related injuries are possible.
4 Sensitivity analysis and validation
A sensitivity analysis of the ‘Risk to Injury’ FSE was performed using an iterative process. A select number of numeric inputs were chosen that best represent each risk factor. All possible combinations of these inputs were evaluated to determine the sensitivity of each risk factor. As anticipated, the most sensitive input is damageability, followed by OFC hazards/retrofit decisions; represented by the building influence axis in Fig. 4. Academic literature clearly documents damageability as the primary predictor of injuries; injuries due to OFCs are also clearly established. Earthquake safety education is the most influential non-building factor (non-building influence axis). Familiarity, previous earthquake experience, time of day, and body temperature are less sensitive. This is partially due to (1) the emphasis placed on known influences in the fuzzy rule-based knowledge, and (2) the hierarchical framework as the aforementioned factors undergo more fuzzy inferences (Fig. 2). However, combinations of the most influential parameters of these factors (unfamiliar, little experience, daytime earthquake, and/or serious hypothermia) increase sensitivity.

Sensitivity analysis results of building versus non-building factors (Ploeger 2014)
There are very few case studies that provide an extensive epidemiology of earthquake injuries, that is, all documented injuries for a building where many risk factors are known. Durkin et al. (1991b) present an example of such a case study which details the injuries of 22 survivors of an eight-story reinforced concrete medical resident dormitory that collapsed during the 1985 M8.0 Michoacan (Mexico City) earthquake (Table 6). In this case study, many survivors sustained multiple injuries, but only the most serious injury was considered.
In this example, there are inconsistencies in the estimation of the number of injuries which is expected because the Hazus methodology is calibrated using Californian earthquakes. For example, as dictated in the Hazus methodology, the complete collapse of a reinforced concrete building would cause the following distribution of injuries, 40 % minor, 20 % serious, 5 % life-threatening, and 10 % fatal. On the other hand, the ‘Risk to Injury’ and the life-threatening injury profiles are more consistent with actual observations. Head and spinal injuries received moderate risk, while trunk, serious orthopedic, and crush injury are ranked as high risk. Serious orthopedic and crush injury (including compression) had the highest observations, while trunk injuries only had one observation. However, upon further inspection, two crush injuries and two orthopedic injuries were located in the trunk.
5 Results and discussion
The purpose of this article is to present the rationale and development of the CanRisk injury model. However, results will be presented to demonstrate the utility of this tool based on a generic set of conditions (Table 7). Four building types which represent the major construction materials are selected: W1 a light timber-frame building, URMM a mid-rise unreinforced masonry building, C1H a high-rise concrete moment frame building, and S1L a low-rise steel moment frame building. Only residential occupancies are considered in this demonstration: RES1 is a single-family dwelling which typically consists of wood and URM building types, and RES3D which is a 10–20 unit multi-family dwelling. All scenarios consider a location with little experience (e.g., Ottawa), a temperature >10 °C, and a daytime event. A RES1 building is assumed to have an occupancy of five, while the multi-family dwelling as an assumed occupancy of 50. A direct application of this tool to a case study of Ottawa, Canada, can be found in Ploeger (2014).
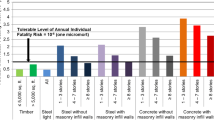
The results show that, under similar conditions, concrete and steel buildings will lead to an increased likelihood of being injured due to the nature of construction material as this reflects the potential mass, height, and volume of the debris as well as the challenges to remove the rubble. Additionally, RES1 and RES3D have inherent differences in OFC hazard; the hazard is higher in multi-family dwellings due to additional electrical and mechanical OFCs that are present in larger buildings and smaller living spaces. However, Fig. 5 shows the unique risk of URM buildings in which out-of-plane failures prior to structural failure can increase an individual’s likelihood of being injured due to the heavy and blunt attributes of brick/stone as well as the resultant rubble. In all scenarios, the likelihood of being injured is stable until extensive damage is initiated. When the building is relatively intact, then the primary mechanism of injury is due to a combination of OFC hazards and earthquake safety education. Arguably, many of these injuries can be prevented with appropriate mitigation and preparedness strategies. As seen in Table 7, the combination of OFC retrofits and active training can significantly reduce the likelihood of being injured and reduce the number of injuries. The user can test strategies by investigating various combinations of strategies such as OFC retrofits (e.g., to architectural/non-structural, mechanical/electrical and/or building content components) and earthquake safety educations (e.g., none, reading, visual, and/or active).

Compares eight scenarios input into the CanRisk injury model which represents the four common building types and the influence of mitigation and preparedness strategies (OFC retrofits and earthquake safety education). The points refer to the various building types: Timber frame (circle), unreinforced masonry (square), concrete moment frame (triangle), and steel moment frame (diamond). The solid lines are scenarios without CanRisk mitigation strategies, and the dotted lines are scenarios with CanRisk mitigation strategies
At the onset of extensive structural damage, likelihood of being injured approximately doubles because structural elements begin to fail; these elements tend to be heavy and/or create tripping hazards. Partial or complete failure presents the highest likelihood of being injured; however, risk decreases when the individual has adequately retrofitted OFCs as well as takes cover under a sturdy piece of furniture.
The above example demonstrates the utility of the CanRisk injury model as an EM tool to aid in decision making. However, this model can also facilitate decision making of a home owner right up to the Federal government (Table 8). To further demonstrate the ease of use for decision makers, the model is also designed to show the FSE outputs to all the pairing influences (e.g., building influence, psycho-environmental influence) and the final output is also expressed in descriptive terms (e.g., ‘Very Low’ to ‘Extreme’). Incidentally, the CanRisk injury model has already been implemented in an institutional-wide simulation cell exercise whereupon the results were useful for exercising institutional security procedures and the coordination between emergency management teams.
The methods used in the development of the CanRisk injury model present an innovative approach to evaluating an individual’s likelihood of being injured in an earthquake as well as providing important medical details to decision makers. Firstly, the compilation and analysis of earthquake injury and mechanism datasets have provided valuable insight into patterns and distributions of earthquake injuries. Secondly, in North America, there are few earthquake models that provide detailed information on earthquake injuries. Hazus, although monumental, only accounts for the number and distribution of casualties that are building-related and do not include non-building-related injuries such as falls nor does it provide specific details on life-threatening injuries. The CanRisk injury model attempts to capture these additional injuries as well as provides information on an individual’s risk to life-threatening head/spinal, trunk, orthopedic, and crush injuries.
Thirdly, the application of fuzzy methodology is a useful approach to multi-criteria decision making and has recently been gaining acceptance in various field such as civil engineering (e.g., Abdul-Rahman et al. 2013), environmental monitoring (e.g., Wang et al. 2009; Mi et al. 2011), and medicine (e.g., Bates and Young 2003). The fuzzy approach has many similarities to traditional multi-criteria analysis such as (1) the ability to incorporate quantitative and qualitative attributes/criteria, (2) the ability to include incommensurable units, (3) incorporating many attributes, and (4) accounting for subjectivity and uncertainty. However, a fundamental difference is that FSE, in particular, does not evaluate and rank a series of possible alternative decisions but rather evaluates the attributes/criteria and outputs a single value. This difference and the ability to systematically handle incomplete and ambiguous data as well as the ability to capture imprecision in natural language make the FSE approach ideal for this type of study.
Lastly, the CanRisk injury model evaluates information on a building-by-building basis and provides decision makers with information that can reduce the likelihood of being injured. Additionally, decision makers can evaluate preparedness and mitigation strategies such as OFC retrofits and earthquake safety programs, facilitate emergency planning such as resource acquisitions and stockpiles, and utilize the program to build scenarios for training purposes.
The following are recommendations for future work:
-
1.
Casualty loss estimation methodology is underpinned by evidence-based research and analysis. Therefore, it is imperative that case studies are assembled and made available. With larger datasets and qualitative observations, loss estimation methodology can be better refined, including the contributions detailed in this article.
-
2.
An international framework for recording, standardizing and reporting earthquake injuries is needed. Even contributions from a single institution are useful in loss estimation research. Therefore, it is encouraged that medical care facility emergency management committees facilitate and support a framework to record earthquake-related injuries. This can be accomplished in several ways including tailored medical charts (i.e., how were you injured?), an assigned personnel or volunteer to record such information, or a pretested standardized questionnaire to collect relevant data after the earthquake.
-
3.
A partner-enabled approach to case studies is also beneficial. Pretested standardized questionnaires can be constructed and given to participating institutions, agencies, and businesses to enable a cohort study of injuries and their mechanisms.
-
4.
Researchers should make a better effort to publish earthquake case studies that include injuries. Even moderate earthquakes such as the 2010 M5.0 Val-des-Bois that affected the Ottawa, Canada, region can provide important observations, challenges, successes, and ‘lessons learned.’
6 Conclusion
Earthquakes present a significant exposure to danger and threaten the integrity, security, and well-being of communities. Earthquake risk is complex and infused with imprecision, ambiguity and limited data, making it difficult to model. However, modeling is a useful exercise and can facilitate informed decision making in emergency management. The CanRisk injury model enables decision makers to test potential mitigation and preparedness strategies which can aid in the design of effective emergency plans and promote community and medical care facility resilience. Additionally, the CanRisk injury model outputs can aid in the development of a realistic earthquake scenario that can be utilized as an educational tool and for training purposes (e.g., tabletop exercise).
The CanRisk injury model is designed for a Canadian setting, but it has international application in other developed and/or similar regions. The validation results of the model are promising, but loss estimation studies must rely mostly on future damaging earthquakes for validation. Nonetheless, the CanRisk injury model risk factors are supported not only by an extensive review on multi-perspective, international scholarly case studies but also on the compilation and analyses of injury and mechanism datasets.
References
Abdul-Rahman H, Wang C, Lee YL (2013) Design and pilot run of fuzzy synthetic model (FSM) for risk evaluation in civil engineering. J Civ Eng Manag 19:217–238
Alexander D (1985) Death and injury in earthquakes. Disasters 9:57–60
Alexander D (1996) The health effects of earthquakes in the mid-1990s. Disasters 20:231–247
Ardagh MW, Richardson SK, Robinson V, Than M, Gee P, Henderson S, Khodaverdi L, McKie J, Robertson G, Schroeder PP, Deely JM (2012) The initial health-system response to the earthquake in Christchurch, New Zealand, in February, 2011. Lancet 372:2109–2115
Armenian HK, Noji EK, Oganesian AP (1992) A case-control study of injuries arising from the earthquake in Armenia, 1988. Bull World Health Organ 70:251–258
Astoul A, Filliter C, Mason E, Rau-Chaplin A, Shridhar K, Varghese B, Varshney N (2013) Developing and testing the Automated post-event earthquake loss estimation and visualization (APE-ELEV) technique. Bull Earthq Eng 11:1973–2005
Auf der Heide E (2006) The importance of evidence-based disaster planning. Ann Emerg Med 47:34–49
Bates HT, Young MP (2003) Applying fuzzy logic to medical decision making in the intensive care unit. Am J Crit Care Med 167:948–952
Beinin L (1985) Public health consequences of earthquakes. Medical consequences of natural disasters. Springer, Berlin, pp 12–27
Bell DG, Tikuisis P, Jacobs I (1992) Relative intensity of muscular contraction during shivering. J App Physiol 72:2336–2342
Bruneau M (1990) Preliminary report of structural damage from the Loma Prieta (San Francisco) earthquake of 1989 and pertinent to Canadian structural engineering practice. Can J Civil Eng 17:198–208
Bruneau M, Lamontagne M (1994) Damage from 20th century earthquakes in eastern Canada and seismic vulnerability of unreinforced masonry buildings. Can J Civil Eng 21:643–662
Coburn A, Spence R (2002) Earthquake protection. Wiley, West Sussex
Dooley D, Catalano R, Mishra S, Serxner S (1992) Earthquake preparedness: predictors in a community survey. J Appl Soc Psychol 22:451–470
Du Ree AC (1941) Fire-department operations during the Long Beach earthquake of 1933. Bull Seism Soc Am 31:9–12
Durkin ME (1985) Behavior of building occupants in earthquakes. Earthq Spectra 1:271–283
Durkin ME, Murakami HO (1988) Casualties, survival, and entrapment in heavily damaged buildings. In: Proceedings of ninth world conference on earthquake engineering, Tokyo–Kyoto, 02–09 Aug 1988
Durkin ME, Thiel CC Jr (1992) Improving measures to reduce earthquake casualties. Earthq Spectra 8:95–113
Durkin ME, Thiel CC Jr, Schneider JE, De Vriend T (1991a) Injuries and emergency medical response in the Loma Prieta earthquake. Bull Seism Soc Am 81:2143–2166
Durkin ME, Coulson AH, Hijar M, Kraus J, Murakami HO (1991b) The survival of people in collapsed buildings. Disaster chronicles: earthquake in Mexico, September 19 and 20, 1985, vol 3. Panamerican Health Organization, Washington D.C, pp 55–76
Elsabbagh A (2013) Seismic risk assessment of unreinforced masonry buildings using fuzzy based techniques and the regional seismic risk assessment of Ottawa, Ontario. M.ASc. thesis. University of Ottawa
Federal Emergency Management Agency (2012) Hazus ®-MH 2.1—Earthquake model technical manual. Federal Emergency Management Agency, Washington D.C
Frolova N, Larionov V, Bonnin J (2011) Earthquake casualties estimation in emergency mode. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes: progress in modelling and mitigation. Advanced in natural and technological research, vol 29. Springer, The Netherlands, pp 107–124
Fulford G, Jones T, Stehle J, Corby N, Robinson D, Schneider J, Dhu T (2002) Earthquake risk. In: Dhu T, Jones T (eds) Earthquake risk in newcastle & lake Macquarie. Geoscience Australia, Canberra, pp 103–122
Iampietro PF (1961) Prediction of skin temperature of men in the cold. J App Physiol 16:405–408
International Standard Organization (2004) ISO8996:2004 Ergonomics of the thermal environment—determination of metabolic rate
Jones T, Dhu T (2002) Summary. Earthquake risk. In: Dhu T, Jones T (eds) Earthquake risk in newcastle & lake Macquarie. Geoscience Australia, Canberra, pp 1–14
Komsari S (2014) Seismic risk assessment of wood frame construction using fuzzy based techniques. M.ASc. thesis. University of Ottawa
Lamontagne M (2002) An overview of some significant eastern Canadian earthquakes and their impacts on the geological environment, buildings and the public. Nat Hazards 26:55–67
Lomnitz C (1970) Casualties and behaviour of populations during earthquakes. Bull Seism Soc Am 60:1309–1313
Mahue-Giangreco M, Mack W, Seligson H, Bourque LB (2001) Risk factors associated with moderate and serious injuries attributable to the 1994 Northridge earthquake, Los Angeles, California. Ann Epidemiol 11:347–357
Maruo S, Matumoto M (1996) Spinal fractures resulting from the 1995 Great Hanshin earthquake of the Kobe–Osaka area of Japan. Spinal Cord 34:382–386
Mawson AR (2005) Understanding mass panic and other collective responses to threat and disaster. Psychiatry 68:95–113
McArthur DL, Peek-Asa C, Kraus JF (2000) Injury hospitalizations before and after the 1994 Northridge, California earthquake. Am J Emerg Med 18:361–366
McKevitt WE, Timler PAM, Lo KK (1995) Nonstructural damage from the Northridge earthquake. Can J Civil Eng 22:428–437
Mi C, Zhang X, Li S, Yang J, Zhu D, Yang Y (2011) Assessment of environment lodging stress for maize using fuzzy synthetic evaluation. Math Comput Model 54:1053–1060
Mitchell D, DeVall RH, Saatcioglu M, Simpson R, Tinawi R, Tremblay R (1995) Damage to concrete structures due to the 1994 Northridge earthquake. Can J Civil Eng 22:361–377
Mulvey JM, Awan SU, Qadri AA, Maqsood MA (2008) Profile of injuries arising from the 2005 Kashmir earthquake: the first 72 h. Injury 39:554–560
Nguyen LH, Shen H, Ershoff D, Afifi AA, Bourque LB (2006) Exploring the casual relationship between exposure to the 1994 Northridge earthquake and pre- and post-earthquake preparedness activities. Earthq Spectra 22:569–587
Noji EK, Kelen GD, Armenian HK, Oganessian A, Jones NP, Siverston KT (1990) The 1988 earthquake in Soviet Armenia: a case study. Ann Emerg Med 19:891–897
Nuzzo R (2014) Statistical errors. Nature 506:150–152
Ohashi H, Ohta Y (1984) Importance of indoor and environmental performance against an earthquake for mitigating casualties. In: Proceedings of the eighth world conference on earthquake engineering, San Francisco, United States, 21–28 July 1984, pp 65–662
Ozdogan S, Hocaoglu A, Caglayan B, Imamoglu OU, Aydin D (2001) Thorax and lung injuries arising from the two earthquakes in Turkey in 1999. Chest 120:1163–1166
Papadopoulos IN, Kanakaris N, Triantafillidis A, Stefanakos J, Kainourgios A, Leukidis C (2004) Autopsy findings from 111 deaths in the 1999 Athens earthquake as a basis for auditing the emergency response. Br J Surg 91:1633–1640
Paultre P, Lefebvre G, Devic J-P, Cote G (1993) Statistical analyses of damages to buildings in the 1988 Saguenay earthquake. Can J Civil Eng 20:988–998
Peek-Asa C, Kraus JF, Bourque LB, Vimalachandra D, Yu J, Abrams J (1998) Fatal and hospitalized injuries resulting from the 1994 Northridge earthquake. Int J Epidemiol 27:459–465
Peek-Asa C, Ramirez M, Seligson H, Shoaf K (2003) Seismic, structural, and individual factors associated with earthquake related injury. Inj Prev 9:62–66
Ploeger SK (2008) Applying the HAZUS-MH software tool to assess seismic hazard and vulnerability in downtown Ottawa, Canada. M.Sc. thesis, Carleton University
Ploeger SK (2014) Development and application of the CanRisk injury model and a disaster spatial decision support system (SDSS) to evaluate seismic risk in the context of emergency management in Canada: Case study of Ottawa, Canada. Ph.D. Dissertation, University of Ottawa
Ramirez M, Peek-Asa C (2005) Epidemiology of traumatic injuries from earthquakes. Epidemiol Rev 27:47–55
Roces MC, White ME, Dayrit MM, Durkin ME (1992) Risk factors for injuries due to the 1990 earthquake in Luzon, Philippines. Bull World Health Organ 70:509–515
Russell LA, Goltz JD, Bourque LB (1995) Preparedness and hazard mitigation actions before and after two earthquakes. Environ Behav 27:744–770
Saatcioglu, M. (2014). Personal communication. University of Ottawa
Scawthorn C (1989) Estimation of post-earthquake search and rescue personnel and equipment needs. In: Jones N, Noji E, Smith G, Krimgold F (eds) International Workshop on earthquake injury epidemiology for mitigation and response. Johns Hopkins University, Baltimore, United States. Springer, 10–12 July 1989, pp 394–414
Schaser K-D, Stover JF, Melcher I, Lauffer A, Haas MP, Bail HJ, Stockle U, Puhl G, Mittlmeier TW (2006) Local cooling restores microcirculatory hemodynamics after closed soft-tissue trauma in rats. J Trauma 61:642–649
Scheulen JJ, Thanner MH, Hsu EB, Latimer CK, Brown J, Kelen GD (2009) Electronic mass casualty assessment and planning scenarios (EMCAPS): development and application of computer modelling to selected national planning scenarios for high-consequence events. Ann Emerg Med 53:226–232
Sedan O, Negulescu C, Terrier M, Roulle A, Winter T, Bertil D (2013) Armagedom—a tool for seismic risk assessment illustrated with applications. J Earthq Eng 17:253–281
Shaw R, Shiwaku K, Kobayashi H, Kobayashi M (2004) Linking experience, education, perception and earthquake preparedness. Disaster Prev Manage 13:39–49
Sheng C-Y (1987) Medical support in the Tangshan earthquake: a review of the management of mass casualties and certain major injuries. J Trauma 27:1130–1135
Shoaf KI, Nguyen LH, Sareen HR, Bourque LB (1998) Injuries as a result of California earthquakes in the past decade. Disasters 22:218–235
Spence R, So E, Jenkins S, Coburn A, Ruffle S (2011) A global earthquake building damage and casualty database. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes: progress in modelling and mitigation. Advanced in natural and technological research, vol 29. Springer, The Netherlands, pp 65–79
Stallings RA (2002) Methodological issues. In: Rodriguez H, Quarantelli EL, Dynes RR (eds) Handbook of disaster research. Springer, New York
Takagi R, Fujita N, Arakawa T, Kawada S, Ishii N, Miki A (2011) Influence of icing on muscle regeneration after crush injury to skeletal muscles in rats. J App Physiol 110:382–388
Tanaka H, Oda J, Iwai A, Kuwagata Y, Matsuoka T, Takaoka M, Kishi M, Morimoto F, Ishikawa K, Mizushima Y, Nakata Y, Yamamura H, Iraide A, Shimazu T, Yoshioka T (1999) Morbidity and mortality of hospitalized patients after the 1995 Hanshin-Awaji earthquake. Am J Emerg Med 17:186–191
Tesfamariam S, Saatcioglu M (2010) Seismic vulnerability assessment of reinforced concrete buildings using hierarchical fuzzy rule base modeling. Earthq Spectra 26:235–256
Tierney KJ (1990) Developing multivariate models for earthquake casualty estimation. In: Workshop on modelling earthquake casualties for planning and response, Pacific Grove United States, 04–06 December 1990
Trendafiloski G, Wyss M, Rosset P (2011) Loss estimation module in the second generation software QLARM. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes: progress in modelling and mitigation, Advanced in Natural and Technological Research, vol 29. Springer, The netherlands, pp 95–106
Wang J-H, Lu X-G, Jiang M, Li X-Y, Tian JH (2009) Fuzzy synthetic evaluation of wetland soil quality degradation: a case study on the Sanjiang Plain, Northeast China. Pedosphere 19:756–764
Zuccaro G, Cacace F (2011) Seismic casualty evaluation: the Italian model, an application to the L’Aquila 2009 event. In: Spence R, So E, Scawthorn C (eds) Human casualties in earthquakes: progress in modelling and mitigation. Advanced in natural and technological research, vol 29. Springer, The Netherlands, pp 171–184
Acknowledgments
The author would like to acknowledge Dr. Gilles Lamothe from the Department of Mathematics and Statistics at the University of Ottawa for his insight and assistance with the statistical analysis of the datasets. The author would also like to thank Dr. Ollie Jay and Matthew Cramer (Ph.D. Candidate) from the School of Human Kinetics at the University of Ottawa for the modification and use of their thermometric model.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ploeger, S.K., Elsabbagh, A., Saatcioglu, M. et al. Development of the CanRisk earthquake injury model. Nat Hazards 80, 1171–1194 (2016). https://doi.org/10.1007/s11069-015-2017-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11069-015-2017-y