
Abstract
Motor imagery (MI, the mental representation of an action without engaging in its actual execution) is a therapeutically relevant technique to promote motor recovery after neurologic disorders. MI shares common neural and psychological bases with physical practice. Interestingly, both acute and progressive neurologic disorders impact brain motor networks, hence potentially eliciting changes in MI capacities. How experimental neuroscientists and medical practitioners should assess and take into account these changes in order to design fruitful interventions is largely unresolved. Understanding how the psychometric, behavioral and neurophysiological correlates of MI are impacted by neurologic disorders is required. To address this brain-behavior issue, we conducted a systematic review of MI data in stroke, Parkinson’s disease, spinal cord injury, and amputee participants. MI evaluation methods are presented. Redundant MI profiles, primarily based on psychometric and behavioral evaluations, emerged in each clinical population. When present, changes in the psychometric and behavioral correlates of MI were highly congruent with the corresponding motor impairments. Neurophysiological recordings yielded specific changes in cerebral activations during MI, which mirrored structural and functional reorganizations due to neuroplasticity. In this view, MI capacities may not be deteriorated per se by neurologic diseases resulting in chronic motor incapacities, but adjusted to the current state of the motor system. Literature-driven orientations for future clinical research are provided.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Motor Imagery
Motor Imagery (MI) is the internal representation of an action without engaging in its physical execution. Neuroimaging findings provided evidence that MI and physical practice (PP) are functionally equivalent, i.e., recruit overlapping brain regions within the brain motor networks underlying motor preparation and execution, including pre-motor, parietal, primary somatosensory and motor cortices (for reviews, see Munzert and Zentgraf 2009; Jeannerod 1994, 2001; Guillot et al. 2014; Munzert et al. 2009; Lotze and Halsband 2006; Guillot et al. 2012a; Hetu et al. 2013; Holmes and Collins 2001). Cerebral networks controlling MI and PP of the same task are hierarchically organized, with higher recruitment of central and cerebellum motor regions during PP (Macuga and Frey 2012). Reduced activation intensities by 30 to 50 % are usually recorded during MI within the primary motor and somatosensory cortices (Lotze and Halsband 2006; Porro et al. 1996). Functional differences between MI and PP primarily account for the absence of overt motion and lack of movement-related sensory feedback under the MI condition. Brain motor system activation is stronger for MI modalities presenting a “small subjective distance between the self and his own imaginal experience” (Jeannerod 1995). Due to their embodied nature, first person (i.e., ‘seen from inside’) and kinesthetic MI have greater functional equivalence with PP (Solodkin et al. 2004; Guillot et al. 2009; Lorey et al. 2009; Stinear et al. 2006; Lotze and Halsband 2006). Likewise, MI expertise leads to more focused recruitment of the brain motor networks and higher activation intensities (Guillot et al. 2008; Lebon et al. 2012; Marks and Isaac 1995; van der Meulen et al. 2012; Williams et al. 2012; Lorey et al. 2011).
The involvement of a task-specific corticospinal network during MI is also largely documented (for review, see Stinear 2010). Typically, a transcranial magnetic stimulation (TMS) pulse is applied to the primary motor cortex as participants engage into MI (Fig. 2b). Pyramidal neurons are activated trans-synaptically through electromagnetic induction (Rothwell 1991), and the resulting motor evoked potential is recorded at the peripheral level using surface electromyography (EMG; Fig. 2b). Stimulations protocols, by varying the number, intensity and frequencies of magnetic pulses, allow specific investigations of intra-cortical facilitation or inhibition during mental and motor tasks (Reis et al. 2008; Dayan et al. 2013). Facilitation of the corticospinal tract during MI (e.g., reduced motor threshold, decreased motor evoked potentials latencies and increased amplitude, or higher extension of the cortical sites of facilitation as compared to rest) is reduced compared to PP (Clark et al. 2004; Leonard and Tremblay 2007), but is nonetheless specific according to the prime agonist muscles of the imagined task (Kasai et al. 1997; Facchini et al. 2002; Stinear and Byblow 2003; Rossini et al. 1999), similarly as during motor preparation (Tomberg and Caramia 1991). Furthermore, corticospinal facilitation is time-locked to the imagined phases of muscle activation (Fadiga et al. 1999; Levin et al. 2004). For instance, Stinear and Byblow (2003) reported facilitation of thumb abductor muscles only when participants imagined the contraction phase of the corresponding movement. Corticospinal facilitation during MI accounts for both increased intra-cortical facilitation and reduced intra-cortical inhibition (Stinear 2010; Takemi et al. 2013) and resembles that elicited by small muscle contractions (Abbruzzese et al. 1999). However, TMS studies provided inconclusive results as regards facilitation of spinal motoneurons during MI (Stinear 2010, for a specific discussion). This was typically addressed in TMS designs by recording Hoffman’s reflex as participants engaged during MI. EMG experiments, by contrast, provided evidence for facilitation of Hoffman’s reflex during MI (Bonnet et al. 1997; Hale et al. 2003), thus supporting the possible recruitment of alpha motor neurons. Since the pioneering work by Jacobson (1930, 1932), subliminal muscle activations during MI were regularly reported, and the properties of the somatic signals resembled actual motor commands (Wehner et al. 1984). Muscles responses are further known to increase according to the physical effort required by the imagined action (Bakker et al. 1996; Boschker 2001). While some authors challenged the hypothesis of muscle responses during MI, or their specificity (e.g., Shaw 1938), Gandevia et al. (1997) argued on the basis of microneurographic recordings that during MI trials eliciting sufficiently strong neuromuscular activity, sensory feedback from spindles were also present, thus describing a subliminal feedback loop of motor control which could reinforce motor programs (i.e., the psycho-neuromuscular theory of motor learning). Recently, Guillot et al. (2007) observed that muscles responses during MI mirrored the contraction type, and preserved both muscles synergies and agonist/antagonist patterns of coordination (see Fadiga et al. 1998; Tamaki et al. 2013 for analogous conclusions on the basis of TMS findings).
Overall, a strong neuroscientific background supports the central elaboration of motor command signals during MI (Guillot et al. 2012a). However, the neural commands for muscular contractions are blocked at some level of the motor system by active inhibitory mechanisms (Jeannerod 1994; Berthoz 1996; Lotze et al. 1999; Guillot et al. 2012a). MI can thus be considered a “special form of motor behavior”, intermediate in the continuum extending from motor preparation to motor execution (Stephan et al. 1995; Stephan and Frackowiak 1996; Nikulin et al. 2008; Stinear 2010).
Mental Practice
“In contrast to the imagery process per se, mental practice (…) consists of a training method by which the internal reproduction of a given motor act is repeated extensively with the intention of improving performance”, Jackson et al. (2001, p. 1133).
Since Warner and McNeill (1988), theoretical rationale supporting the use of mental practice (MP; i.e., as described in Jackson et al. 2001; see above) in neurologic rehabilitation benefited from neuroimaging evidence of functional equivalence between MI and PP (e.g., Munzert et al. 2009; Mulder 2007; Jackson et al. 2001; Decety 1993). MP might, like PP training, induce activity-dependant neuroplasticity (i.e., the capacity of the neural tissue to reorganize its anatomical and functional synaptic properties). Brain imaging studies in healthy participants (HPs) disclosed MP-dependant neuroplasticity yielding motor performance improvements (Jackson et al. 2003; Pascual-Leone et al. 1995; Lacourse et al. 2004; Zhang et al. 2011, 2012; Nyberg et al. 2006; Ranganathan et al. 2004). It is however well-admitted that MP benefits do not outperform those elicited by PP. Their combination yielded stronger improvements in motor learning and rehabilitation (Feltz and Landers 1983; Driskell et al. 1994; Guillot and Collet 2008; Jackson et al. 2001).
“If you cannot perform an action physically, you cannot imagine it in a way that is necessary for a high degree of functional equivalence”.
This theoretical postulate by Olsson and Nyberg (2010; p. 711) challenges the therapeutic rationale supporting MP programs in neurologic rehabilitation. Previous reviews explored the best rules for MI practice in medicine and disciplines related to motor performance (e.g., Schuster et al. 2011; Braun et al. 2008, 2013), or discussed how a specific component of MI accuracy could be altered by neurologic diseases (e.g., Malouin and Richards 2010; Sharma et al. 2006; Munzert et al. 2009; Guillot et al. 2012b). Nonetheless, to the best of our knowledge, a systematic review of MI evaluation methods and data from clinical experiments are lacking. MI evaluation in healthy individuals ideally requires combining tools from different scientific fields, namely i) psychometric tests, ii) behavioral tests using mental chronometry and iii) neurophysiological measures of central and peripheral nervous system activities (Collet et al. 2011; Guillot and Collet 2005b). Accurate MI performance is expected to elicit similar psychometric, behavioral and neurophysiological correlates as PP of the same task (for reviews, see Annett 1995; Collet et al. 2011; Holmes and Collins 2001; Guillot and Collet 2005b). We sought to provide such analysis on the basis of experimental data in stroke (STR), Parkinson’s disease (PKD), spinal cord injury (SCI) and amputated (AMP) participants. In a first part, we introduce descriptive data related to the literature database search. We then discuss the specificities of MI evaluation techniques used in clinical settings while the third part is designed to provide a review of MI data. On this basis, literature-driven orientations for future research are considered.
Literature Review
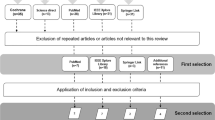
Biomedical studies were selected from the MEDLINE®/PubMed® database up to August 2013. Were included: i) MP studies (i.e., longitudinal studies testing MP efficacy in clinical rehabilitation settings), and ii) MI studies (i.e., transversal MI studies reporting MI data on the basis of psychometric, behavioral and neurophysiological evaluations). Were excluded: i) brain-computer interfaces studies with a primary methodological focus, ii) experiments including participants with various pathologies within the same experimental group, and iii) review articles discussing MI issues in several clinical populations, which could thus not be categorized as belonging to the field of STR, SCI, PKD, or AMP research. A large sample of 192 references meeting the inclusion criteria emerged (Table 1), using the search terms “Motor imagery”, “Movement Imagery”, “Imagery”, “Imagination”, “Mental practice”, “Mental training” and “Motor imagery training” in combination with “stroke”, “Parkinson”, “Amputee”, “Amputation”, “spinal cord injury” using the “AND” Boolean operator.
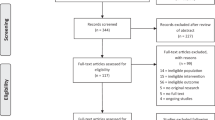
In the STR group, we collected a similar number of MI and MP studies (Table 1), and detected an initial burst of publications in 2004 (Fig. 1). In PKD, SCI and AMP populations only few MP studies were found [i.e., range = 4–6, representing 19 % (PKD), 29 % (SCI), and 22 % (AMP) of MP studies].

MI, MP studies and reviews published per year in stroke, spinal cord injury, Parkinson’s disease and amputee participants (source: MEDLINE®/PubMed®). The TOTAL dotted line is to be referred to on the right axis. For purposes of graphical display, the y-axis scale was half-reduced for studies in Parkinson’s disease, spinal cord injury and amputee participants. MI: Motor Imagery, MP: Mental Practice
Motor Imagery Studies
Forty two percent of MI studies (range = 35–50 % across clinical populations) conducted psychometric evaluations, 35 % (range = 10 -- 41 % across clinical populations) conducted behavioral evaluations, and 57 % (range = 38–90 %) conducted neurophysiological recordings. 40 % (range = 38 -- 62 % across clinical populations) used more than one assessment method. We identified two different types of designs. In 85 % of the experiments, the participants were explicitly instructed to engage into MI (n.b., most experiments involved first-person visual MI, sometimes combined with kinesthetic information). In another 15 %, they were requested to solve a cognitive task implicitly requiring MI, but were not instructed to engage into MI. In 86 % of these implicit MI studies, participants were requested to determine laterality of some body parts as fast and accurately as possible. Other implicit MI paradigms required determining feasibility or limb posture during virtual grasping of visually presented tri-dimensional objects (e.g., Frak et al. 2004; Johnson 2000; Johnson et al. 2002). In the following sections, we will basically refer to “MI” and “implicit MI” when required. Implicit MI tests are objective and reproducible, but do not control individual cognitive strategies used to solve the task.
Explicit and implicit MI experiments both afford standardized evaluations, but relate differently to motor cognition. Explicit MI is a “dynamic state during which the representation of a given motor act is internally rehearsed without motor output” (Decety and Grezes 1999). MI thus involves motor simulation, i.e., predictive models derived from the efferent copy of the motor command (Grush 2004; Wolpert and Flanagan 2001; Demougeot and Papaxanthis 2011; Wolpert and Ghahramani 2000). Conversely, implicit MI can be regarded as a “prospective action judgment” or a “perceptually induced motor decision” (Johnson et al. 2002; Jeannerod 2001), and primarily addresses participant’s capacities to engage into projection and manipulation of their body schema (Parsons 1987a, b).
Mental Practice Studies
MP studies primarily investigated efficacy of the technique on motor disabilities (88 %). Reviewing efficacy of MI training is not the purpose of the present work, as this issue has already been extensively considered in recent review papers (see Schuster et al. 2011 for recent reviews; Faralli et al. 2013; Bowering et al. 2013; Malouin et al. 2013). Inclusion of MP experiments in this systematic review was necessary to understand how MI was evaluated in clinical research protocols. Such evaluations have two purposes: i) determining participant’s capability to engage into MP (preliminary MI evaluation), and ii) determining MI quality during MP interventions (control of MI training).
Previous research yielded that only 11 MP medical studies out of 37 included MI assessments (Schuster et al. 2011, 2012c). In the present literature review, 48 % of MP studies included preliminary MI assessments. Psychometric assessment methods were by far the most frequently encountered (96 %), followed by behavioral and neurophysiological methods (respectively, 36 and 3 %). Only 19 % used more than one assessment method. Present data corroborate Schuster et al. (2011)’s conclusions concerning limited attention paid to preliminary MI evaluation. Description of the methods used to control MP lacked in 43 % of studies. MP was mainly controlled by means of psychological and behavioral tests (79 and 24 %, respectively).
Motor Imagery Evaluation Methods in Clinical Experiments
Clinical evaluations, practical aspects related to their clinical use, and components of MI quality being measured are summarized in Table 3 (p. 23).
Psychological Methods
Oral debriefs, MI questionnaires and self-report ratings are reliable psychometric methods to evaluate MI quality in HPs (Guillot and Collet 2005b). Tests which we will refer to as “congruency tests” were also found in clinical studies.
Explicit Motor Imagery
Oral debriefs were primarily used to control adherence to MI instructions during preliminary assessments (e.g., Kuhn et al. 2006). Oral debriefs also served to control MP (e.g., Dijkerman et al. 2004; Simmons et al. 2008). Generally speaking, use of oral debriefs is mentioned but detailed report of its content lacking. The interview procedures were almost never detailed. To date, only one study reported detailed MI content, use and experience along the course of MP on the basis of oral debriefs (Schuster et al. 2012b).
Standardized questionnaires evaluating MI “vividness” and “ease” were widely used in MI and MP designs (respectively 38 and 21 % of studies). Most MI vividness questionnaires were developed and validated in HPs (the Vividness of Visual Imagery Questionnaire, VVIQ; Marks 1973; the Vividness Movement Imagery Questionnaire, VMIQ; Isaac et al. 1986; and its revised version, VMIQ-2; Roberts et al. 2008; the Questionnaire upon mental imagery, QMI; Sheehan 1967). Vividness questionnaires required participants to perform MI of several standardized motor tasks, sometimes preceded by their physical execution. Participants then provided a vividness score on a 5 or 7-level Likert scale, typically ranging from no image at all / vague perception up to identical sensory experience as PP. Ease questionnaires measured the experienced difficulty at performing MI, again using Likert-type scales ranging from very easy to very difficult (e.g., the Movement Imagery Questionnaire, MIQ; Hall and Martin 1997; and its two revised versions, MIQ-R and MIQ-RS; Hall and Pongrac 1983; Gregg et al. 2010). Some ‘ease’ questionnaires designed for HPs were also shown reliable for assessments in clinical populations (e.g., the MIQ-RS; Butler et al. 2012). However, questionnaires items frequently involved movements which were not targeted by the rehabilitative intervention, or single-joint movements that were not goal-directed. Such tasks are in opposition with those used in MP designs (i.e., MI of goal-directed actions involving affected body parts). Questionnaires items also involved motor tasks entirely decoupled from clinical participant’s current motor capabilities (e.g., “Jumping straight in the air”). In some clinical interventions, experimenters relevantly adapted questionnaires’ content to participant’s motor repertoire, for instance by removing items that persons could no longer perform (Dickstein et al. 2004; Diers et al. 2010; Welfringer et al. 2011). To date, the only questionnaire designed to assess MI in participants with motor impairments, and used to assess vividness in each of our populations of interest, is the Kinesthetic and Visual Imagery Questionnaire (KVIQ; Malouin et al. 2007). A recent questionnaire was also developed for assessment of gait MI vividness after PKD, albeit data revealed limited sensitivity to gait-related disorders (Pickett et al. 2012). Importantly, MI ease and vividness can be collected by means of self-reports using Likert-type or visual analogous scales (Gustin et al. 2010; Lotze et al. 2001; Moseley 2007). Compared to standardized questionnaires, these can be collected from any MI task, and represent user-friendly techniques in clinical settings. MI questionnaires enable standardized assessments and provide a general psychometric index. Yet, these remain highly subjective methods. Schuster et al. (2012c) validated in STR and PKD subjects the translation of the Imagix software (Fournier 2000) which allows more objective assessments of MI vividness and modality. Ultimately, logbooks enable collection of most psychometric MI data (vividness, ease and accuracy) and can be used to control unsupervised MP (Jackson et al. 2004; Dijkerman et al. 2004; Gaggioli et al. 2009; Braun et al. 2010, 2011).
Psychometric evaluations also included “congruency” tests (Samuel et al. 2001; Li 2000; Hotz-Boendermaker et al. 2008; Sharma et al. 2009a, b; de Vries et al. 2011; Braun et al. 2011; Szameitat et al. 2012). Congruency tests address the accuracy of MI (i.e., exactness of MI content). Participants are first requested to perform MI of a sequential motor task (i.e., involving various sets of movements, or cyclical repetitions of the same action). They are then interrupted at some point of the process controlled by the experimenter. Finally, participants verbally describe the MI content at the point of interruption. MI accuracy can also be evaluated after completion of the imagined actions. For instance, participants chose among various pictures representing different body positions which corresponds to the body position achieved through MI (Li 2000; de Vries et al. 2011), or described orally the final imagined body position. The “Questionnaire of mental imagery: rotation of hands” (Sirigu and Duhamel 2001) is a congruency test which was used to investigate MI accuracy in STR participants with and without visual neglect (Vromen et al. 2011). Congruency tests also enabled to control of MP (Kim et al. 2011; Muller et al. 2007).
Implicit Motor Imagery
Psychometric implicit MI assessments focused on accuracy. In mental rotation of body parts paradigms (e.g., recognition of laterality), accuracy referred to the number of correct answers over the total number of presented stimuli (Nico et al. 2004; Helmich et al. 2007; Fiori et al. 2013; Yan et al. 2012). In implicit MI tasks involving determination of action feasibility, or body postures compatibility during hand-objects interactions, accuracy referred to congruency between participants’ “prospective action judgments” and the actual feasibility / compatibility (Johnson et al. 2002; Johnson 2000; Frak et al. 2004; Buxbaum et al. 2005).
Behavioral Methods
Explicit Motor Imagery
Mental chronometry affords investigation of the time course of information processing by the CNS (Posner 1978). As MI implies absence of overt motion, a relevant ‘behavioral’ evaluation method consists in recording the duration of MI (Collet et al. 2011; Malouin et al. 2008b). The ability to achieve tight temporal correspondences between MI and PP time is a reliable marker of MI accuracy (for a recent review, see Guillot et al. 2012b). Mental chronometry tests allowed both preliminary MI assessments (Malouin et al. 2009b; Simmons et al. 2008; Sharma et al. 2009a, b) and control of MI training (Malouin et al. 2004c; Dunsky et al. 2006, 2008; Braun et al. 2011). Behavioral methods represent an objective approach to the issue of MI evaluation in clinical populations, but do not provide any qualitative information about MI content proper.
Correspondence between MI and PP times is often referred to as “temporal equivalence” in the scientific literature. However, temporal equivalence indiscriminately referred across experiments to i) statistically significant correlations between MI and PP durations (i.e., “temporal congruence”), or ii) absence of statistically significant differences between mean/median MI and PP durations (i.e., “isochrony”). Temporal congruence and isochrony are however distinct components of MI accuracy. In the perspective of using mental chronometry in clinical research, this point must be clarified. The statement of “temporal equivalence” should ideally refer to presence of both temporal congruence (i.e., correlation between MI and PP durations) and isochrony (i.e., absence of difference between MI and PP durations). If MI and PP involve common motor planning strategies, the time necessary to complete the two tasks should be close (Decety and Michel 1989; Decety et al. 1989). Factors affecting PP duration (e.g., task complexity) should elicit a parallel increase in MI durations. Therefore, PP and accurate MI times should be correlated. Uncorrelated MI and PP durations unambiguously reflect MI deficits (e.g., Sirigu et al. 1996; Danckert et al. 2002). Temporal congruence thus implies that factors impacting PP timing yield parallel changes on MI timing. The effects of task complexity (Sirigu et al. 1996; Danckert et al. 2002), task duration (Malouin et al. 2008b, a), limb dominance (Decety and Boisson 1990; Dominey et al. 1995), and laterality of the motor deficits (i.e., task actual duration performed with spared or impaired peripheral effectors; Decety and Boisson 1990; Sirigu et al. 1995, 1996; Raffin et al. 2012a) were thus tested in clinical evaluations. Isochrony, similarly as temporal congruence, reflects the recruitment of predictive models for actual actions during MI (Guillot et al. 2012b; Papaxanthis et al. 2002). While absence of isochrony can be due to MI deficits (e.g., inconsistencies between motor predictions and actual motor capabilities), it may also result from factors external to the subject. For instance, movements longer than 30 s tend to be underestimated, whereas the opposite is observed for complex or short-lasting motor sequences (Guillot et al. 2012b). Contrary to temporal congruence, the relationship between isochrony and MI ability is not straightforward. MI and PP durations can be highly correlated, yet with persistent overestimation or underestimation of PP durations due to task specificities.
Standardized chronometric tests generally involved motor sequences ranging from 5 to 30 s (Table 2). When a short motor task (i.e., inferior to 3 or 5 s) was used, it was being repeated several times in order to make the resulting duration compatible with reliable chronometric measurements (e.g., stepping actions; Malouin et al. 2008b, a). Some tests did not record MI durations per se, but the number of motor sequences mentally completed within a predetermined time period (e.g., Stinear et al. 2007; Malouin et al. 2009b, 2008a, b). Experimenters checked presence of a linear increase in the number of repetitions according to increasing time periods allocated to MI (i.e., an index of temporal congruence). Experimenters also checked that the number of imagined movements was similar to the number of movements physically performed within an identical time period (i.e., an index of isochrony). Some behavioral MI assessments did not involve recordings of PP durations. Such behavioral methods appeared of specific interest to limit interferences between PP and MI processes in people with motor incapacities (Table 2). Raffin et al. (2012a) tested the effect of body posture on MI durations in AMP subjects. Participants were requested to imagine a pointing action with their arm being alternatively in a physically compatible or incompatible position for physical execution of the task. Congruent body position was expected to exert a priming effect on MI, which should be facilitated in the case of compatible body position (i.e., hence eliciting shorter durations compared to MI performed with the arm being in an incompatible body position; Sirigu and Duhamel 2001). This test allowed objective assessment temporal congruence in spite of missing limb due to AMP.
Behavioral MI tests involved both goal-oriented movements with a clear functional purpose and single-joint movements decoupled from the environmental context (Table 2). In the latter case, motor tasks are easier to control and reproduce. Motor tasks for behavioral MI tests can be adapted to suit participant’s current motor capabilities (Malouin et al. 2008b). Behavioral assessments may involve cueing conditions. For instance, Sirigu et al. (1996) used a metronome and participants indicated at which point they could no longer follow its pace during actual and imagined finger tapping (Table 2). Dunsky et al. (2006) controlled accuracy of MP using a metronome: its cadence was set up to the natural gait cadence of STR participants. After initiation of imagined gait, beats were interrupted, and participants were requested to announce completion of six additional mental steps. This approach afforded control of MP timing, and can be viewed as a ‘behavioral’ MI congruency test. Some authors suggested that MI should be performed before PP during behavioral tests, in order to prevent the use of alternative cognitive strategies such as counting (Sharma et al. 2009a, b; Malouin et al. 2008b). Others instructed to perform PP before MI of the task (Stinear et al. 2007; Wu et al. 2010).
Implicit Motor Imagery
Behavioral implicit MI assessments investigated participants’ reaction times (RTs); i.e., considered the time elapsed between presentation of the to-be-rotated stimulus and participant’s answer, which includes the reaction time proper and the movement time required to trigger an answer command.Footnote 1 RTs increase proportionally with the distance separating stimulus orientation from the actual body position, thus supporting that participants imagine their own body parts moving towards the stimulus (Parsons 1987a, b, 1994). The effects of actual body posture (i.e., longer RTs expected when the body is in an incompatible position; Nico et al. 2004; van Nuenen et al. 2012), motor impairment (i.e., different RTs expected if the to-be-rotated stimuli involves affected or unaffected body parts; Helmich et al. 2007), and dominance side (i.e., longer RTs expected for recognition of laterality of stimuli corresponding to the non-dominant side; Dominey et al. 1995; Nico et al. 2004) on RTs were used in clinical studies. Implicit MI designs also involve the presentation of two identical visual stimuli with different spatial orientations. Participants were then requested to identify whether the two stimuli were identical (e.g., whether the two hands are of identical laterality). RTs increased proportionally with the degree of mental rotation needed for their alignment. With reference to Shepard and Cooper (1986) the slope coefficient of the regression function between RTs and degrees of mental rotation required to solve the implicit MI task provides the RT / degree, i.e., an index of mental rotation processes. The y-intercept of the regression function reflects cognitive processes distinct from mental rotation proper, for instance spatial encoding or preparation of the behavioral response (e.g., Amick et al. 2006 for an illustration). Implicit MI assessments did usually not require PP of the task, excepted when congruency between “prospective action judgments” and PP was evaluated (Buxbaum et al. 2005).
Neurophysiological Methods
Neurophysiological methods involve recordings of both central and peripheral nervous system activities during MI (Collet et al. 2011; Guillot and Collet 2005b). Neurophysiological evaluations mainly consisted in CNS recordings using brain imaging [magnetoencephalography, functional magnetic resonance imaging (fMRI), and positron emission tomography; see Fig. 2c for classic scanning designs] or TMS techniques (representing respectively 74 and 20 % of MI studies involving neurophysiological measurements). Investigation of the neurophysiological correlates of MI in STR, SCI, PKD and AMP people was reported in 60 % of MI studies. These were however rarely used in MP designs, presumably due to medical, material and temporal constraints. Neurophysiological recordings are objective, but difficult to relate to the psychometric and chronometric indexes of MI (Table 3). Further research in this direction is required. Nonetheless, neurophysiological methods enable direct investigation of the functional equivalence between MI and PP, and determine whether the cerebral substrates underlying MI (or implicit MI) are comparable in clinical populations and HPs. They have thus powerful implications concerning the possibility of using MI to induce MP-dependant neuroplasticity.

Illustration of neurophysiological methods to assess MI. a. Experimental settings combining central (Magnetoencephalography, CTF-MEG system - 275 Channels, CERMEP - Imagerie du vivant) and peripheral electrophysiological recordings (Electrodermal recordings using two 30 mm2 unpolarizable Ag/AgCl electrodes placed on the second phalanx of the second and third fingers of the non-dominant hand; Clark Electromedical Instruments, Ref. E243) during MI of a prehensile task. b. Figure-of-eight coil used for transcranial magnetic stimulation of the contralateral primary motor cortex during MI of forearm movements (used with permission from Professor Kuniyasu Imanaka). Motor potentials evoked by transcranial magnetic stimulation, usually compound potentials of three or four ‘indirect’ waves, are recorded in the prime movers of the imagined action by surface electromyography. They are of reduced magnitude compared to PP. c. Schematic representation of a block-design (left side) and an event-related design (right side) that can be used in MI paradigms. Most reviewed MI experiments implemented block designs. In the block design, several trials (black arrows) are performed successively during periods of 20–30 s for each condition. Before block onset, instructions are provided to participants during brief periods (2–10 s). Brief ‘rest’ periods distinct from control condition can also be included to prevent from physical/mental fatigue in clinical populations. In the event-related design, each experimental condition is presented at random (vertical bars and arrows). MI: Motor Imagery, TMS: Transcranial Magnetic Stimulation, EMG: electromyography
Central Nervous System Recordings
MI and implicit MI experiments both involved CNS recordings (i.e., representing 68 and 33 % of MI studies, respectively). Due to methodological limitations (e.g., the need to keep the head motionless during scanning), simple motor tasks without functional purpose usually supported CNS recordings (e.g., 65 % of brain imaging MI studies). MI tasks nonetheless involved body limbs targeted by the rehabilitative intervention (e.g., actions with the affected upper or lower limbs, respectively for the purposes of prehension and gait rehabilitation).
Peripheral Recordings
Somatic and autonomic responses can be recorded at the peripheral level of the motor system due to selective and incomplete inhibition of motor command signals during MI (Collet and Guillot 2009).
No relationship between EMG activity and the components of MI quality emerged in HPs (Guillot and Collet 2005b; Guillot et al. 2010). In STR participants, Dickstein et al. (2005) found no correlation between subliminal EMG activity during MI and MIQ scores. By contrast, Heremans et al. (2008) provided evidence that recording eye movements during MI with electro-oculography enabled objective assessment of MI quality. Particularly, task-related eye movements were reproduced during accurate MI of visuo-motor tasks (i.e., a tight correspondence in the number and amplitude of eye movements was recorded; Heremans et al. 2008). However, the relevance of electro-oculography recordings for assessment of MI quality of tasks with a poor visuo-motor component may be more limited.
Autonomic nervous system responses (e.g., cardiorespiratory and electrodermal activities) are usually elicited as early as participants engage into MI, and enable objective evaluations of MI quality (Collet et al. 2013 for a review). Only reports of electrodermal recordings were found in reviewed experiments. Electrodermal activity reflects the activity of eccrines sweat glands. These are under the unique control of the sympathetic branch of the autonomic nervous system (Shields et al. 1987) and can be recorded from various neurologically healthy body regions (e.g., hand palm, neck; Matsunaga et al. 1998; Yildiz et al. 2007). Electrodermal responses are characterized by sudden baseline drops in skin resistance, immediately followed by a slower and regular return to baseline (Fig. 2a). Phasic activity reflects mobilization of mental resources during MI, particularly vigilance and attention. In this view, recording phasic activity during MI of complex and goal-directed tasks is of primary interest. Electrodermal responses duration were correlated to MI vividness in HPs (Guillot and Collet 2005b; Di Rienzo et al. 2012). Interestingly, the tonic level can be used as an index of mental fatigue and physiological arousal during MP sessions (Collet et al. 2011). Skin resistance should return to basal levels after MI trials, without progressive increase towards higher values in the case of sustained sympathetic activity throughout the session (Collet et al. 2011). Decay in task novelty, for instance repeated MI of the same action, might result in increased tonic level and decreased sudomotor responses amplitude and duration. Monitoring electroencephalographic activity could also be a direct approach to this issue (e.g., Rushby et al. 2013 for an illustration of combined electroencephalographic and skin resistance recordings in subjects with brain injuries).
Motor Imagery Correlates in Clinical Populations
In this section, we seek to delineate the psychometric, behavioral and neurophysiological correlates of MI after STR, SCI, PKD and AMP. MI and implicit MI results are discussed separately. We dissociated MI changes which were specific to a given state of neurologic impairment (i.e., severity, nature, stage of the pathology) from redundant changes in MI capacities reflecting the impact of the disease on MI quality (i.e., neurologic MI profiles).
Psychological Correlates
Explicit Motor Imagery
A first category of experiments yielded high MI vividness scores in the clinical populations of interest (Malouin et al. 2004c, a; Dickstein et al. 2004; Jackson et al. 2004; Dickstein et al. 2005; Grangeon et al. 2012b; Malouin et al. 2009b; Alkadhi et al. 2005; Heremans et al. 2011; Lotze et al. 2001; Hovington and Brouwer 2010; Raffin et al. 2012a; Butler et al. 2012; Schuster et al. 2012a; Peterson et al. 2012). Neurologic participants achieved vivid visual or kinesthetic MI, similarly as HPs, and reported identical MI ease on the basis of Likert self-reports (Stinear et al. 2007; Cramer et al. 2005; Tremblay et al. 2008; Marconi et al. 2007; Sharma et al. 2009a). Congruency tests evidenced preserved MI accuracy in STR, PKD and SCI people (Sharma et al. 2009a, b; Hotz-Boendermaker et al. 2008; de Vries et al. 2011; Samuel et al. 2001). We did not find reports of psychometric MI congruency tests in AMP subjects.
In a second category of experiments, psychometric evaluations yielded selective MI deficits corresponding to the actual clinical impairments, particularly in STR, PKD and AMP participants with lateralized motor incapacities. Malouin et al. (2009a) described reduced MI vividness in AMP participants for KVIQ items involving the missing limb. Vividness scores resembled those obtained in a group of HPs who underwent limb immobilization. Malouin et al. (2009a) further reported that onset of walking with prosthesis correlated with increased KVIQ scores on the amputated side. These findings confirmed previous observations by Nico et al. (2004), and presumed integration of prosthesis with a natural functionality to the body schema (i.e., by opposition to purely esthetic limb prosthesis). Lower MI vividness for impaired limbs was also observed in STR participants with lateralized motor impairments (Dettmers et al. 2012; Malouin et al. 2008a). In PKD subjects, Heremans et al. (2011) did not observe asymmetrical MI vividness KVIQ scores. By contrast, Randhawa et al. (2010) observed higher variability of KVIQ scores during axial movements (i.e., head and trunk movements in the sagital plane). The authors stated that “difficulty in axial imagery may be a result of changes in muscles that accompany PKD”. Authors thus related MI vividness changes to PKD-related motor deficits. In the studies by Szameitat et al. (2012) and Raffin et al. (2012a), STR and AMP participants experienced lower MI ease for actions involving impaired / missing limbs. Li (2000) finally observed reduced MI accuracy when the task involved impaired limbs in cortical and putamen STR participants. Contrary to other populations, the psychometric correlates of MI appeared unaffected in SCI subjects (Grangeon et al. 2012b; Alkadhi et al. 2005; Hotz-Boendermaker et al. 2008). It was recently advanced, that SCI subjects might benefit from other sensory input than proprioception (e.g., visual input through observation) to maintain and update motor representations (Di Rienzo et al. 2013).
Implicit Motor Imagery
Implicit MI accuracy was reported intact in some experiments including STR, PKD and AMP subjects (Johnson 2000; Johnson et al. 2002; Buxbaum et al. 2005; van Nuenen et al. 2012; Heremans et al. 2011; Helmich et al. 2007; Curtze et al. 2010).
Selective MI accuracy deficits corresponding to actual motor impairments were also reported among the same populations of interest, particularly in persons presenting lateralized motor symptoms. For instance, STR and PKD subjects showed reduced MI accuracy for recognition of limbs corresponding to the damaged side (Dominey et al. 1995; Daprati et al. 2010). STR subjects with visual neglect exhibited MI deficits restricted to the neglected side (Coslett 1998), albeit Vromen et al. (2011) did not replicate this finding.
In specific cases, reduced implicit MI accuracy were detected regardless the actual motor deficits (Johnson et al. 2002; Schwoebel et al. 2002; Fiori et al. 2013; Tomasino et al. 2003; Frak et al. 2004; Yan et al. 2012; Vromen et al. 2011; Nico et al. 2004). Frak et al. (2004) reported, in PKD participants, an impaired capacity to predict feasibility of sizing actions which could still be performed physically. Amick et al. (2006) observed that implicit MI accuracy was impaired in hemi-PKD participants according to the visual field of stimulus presentation. The authors argued for differential involvement of the fronto-parietal networks underlying mental rotation, causing impairment of mental rotation processes in left, but not in right hemisphere PKD. Nico et al. (2004) observed that AMP participants who lost their non-dominant limb had identical implicit MI accuracy scores as HPs, whereas those who lost their dominant limb presented overall reduced accuracy. Fiori et al. (2013) recently showed that SCI participants with complete motor deficits presented higher accuracy scores than HPs. Particularly, they did not present a burst in error rate when to-be-rotated stimuli were displayed in difficult orientations. This pattern of results was present for MR of both hands and letters and the authors concluded that complete deafferentation and deefferentation leaded, due to reduced capabilities to interact with the environment, to the emergence of cognitive strategies based on semantic knowledge and memory which replaced reference to the body schema.
Motor Imagery Profiles Based on Psychometric Data
Briefly speaking, psychometric evaluations yielded three redundant MI data profiles. Intact MI capacities (i.e., high performance or identical results as in HC; 46 % of MI studies with psychometric data), or selective deficits according to the current motor incapacities. These two neurologic MI profiles represented 93 % of pooled psychometric data in STR, SCI, PKD and AMP participants (Table 4). MI and implicit MI deficits reflected actual motor impairment in 65 % of cases. Finally, for implicit MI only, deficits irrespective of the actual motor deficit were reported in STR, PKD and AMP (i.e., 23 % of studies).
Behavioral Correlates
Explicit and Implicit Motor Imagery
Temporal equivalence referred the literature to temporal congruence, isochrony, or both. In reviewed experiments, we noted a huge variability in chronometric data interpretation, particularly concerning isochrony. Importantly, HPs failed in some studies to achieve isochrony, particularly during MI of complex hand motor sequences requiring a high degree of accuracy (e.g., Sabate et al. 2004, 2007; Stinear et al. 2007; Raffin et al. 2012a). Accordingly, mental chronometry assessments in HPs are crucial for interpretation of chronometric MI data in clinical populations.
A first class of chronometric evaluations yielded identical MI and implicit MI capacities in clinical populations and HPs (Johnson 2000; Johnson et al. 2002; Malouin et al. 2008b; Heremans et al. 2011; Grangeon et al. 2012b; Decety and Boisson 1990; Di Rienzo et al. 2013; Raffin et al. 2012a; Helmich et al. 2011; Curtze et al. 2010). Behavioral MI tests which did not involve PP of the task (see Table 2) disclosed preserved MI timing congruency in STR, AMP and PKD subjects (Snijders et al. 2011; Malouin et al. 2008b; Raffin et al. 2012a). Importantly, two patterns of chronometric data support preserved MI timing accuracy: i) identical behavioral MI and implicit MI correlates to those recorded in HPs (Johnson 2000; Johnson et al. 2002; Malouin et al. 2009b; Thobois et al. 2002; Grangeon et al. 2012b; Di Rienzo et al. 2013), and ii) temporal congruence / isochrony between MI and PP with parallel increases in durations due to the presence of motor deficits (Sirigu et al. 1995; Thobois et al. 2000, 2002; Gonzalez et al. 2005; Sabate et al. 2004, 2007; Decety and Boisson 1990; Heremans et al. 2012, 2011; Malouin et al. 2009a; Dominey et al. 1995).Footnote 2 Interestingly, this neurologic MI profile was early formalized in a pioneering review by Jeannerod (2001).
Other mental chronometry experiments evidenced MI deficits (i.e., absence of temporal congruence and / or isochrony compared to MI of healthy body parts or MI of the same action in HPs) restricted to MI of affected limbs after AMP, STR and PKD (Sirigu et al. 1996; Dominey et al. 1995; Sabate et al. 2004; Daprati et al. 2010; Wu et al. 2010; Dettmers et al. 2012; Liepert et al. 2012; Raffin et al. 2012a).Footnote 3 For instance, AMP participants showed similar patterns of temporal correspondences as HPs during MI of the unaffected limb but exhibited overestimation of PP durations when imagining the same action with the amputated limb (Raffin et al. 2012a).
Chronometric data finally revealed MI deficits unrelated to motor incapacities, particularly after STR and PKD (Sirigu et al. 1996; Danckert et al. 2002; Sabate et al. 2004; Frak et al. 2004; Malouin et al. 2004b; Yan et al. 2012). Overall, such MI deficits reflected the effect of the neurologic disorder on higher cognitive processes. For instance, a link between bilateral slowing of MI times and working memory impairments after STR was reported (Malouin et al. 2004b, 2012). Working memory is involved in generation, maintenance and controllability of motor images (Malouin et al. 2004b, 2012). Implicit MI paradigms also yielded non motor-related MI impairments. Yan et al. (2012) reported that deficient spatial encoding and spatial information processing, due to impaired neural processing within the visuo-motor network, elicited longer RTs in STR compared to HPs irrespectively of the hand (i.e., affected or unaffected) involved. Frak et al. (2004) evidenced that bilateral idiopathic PKD subjects did not show RTs changes exhibited by HPs while determining feasibility of sizing an object according to different orientations (i.e., shorter responses when stimuli were presented in preferred orientations). Finally, Nico et al. (2004) observed delayed RTs, during complex implicit MI tasks in subjects amputated from their dominant upper limb (i.e., determining laterality of hands in difficult orientations). Again, these were irrespective of the actual motor deficit and suggest preferential use of the dominant limb when reference to the body schema was required.
Motor Imagery Profiles Based on Behavioral Data
Four neurologic MI data profiles emerged from behavioral tests (Table 5): i) identical behavioral correlated as in HPs (i.e., 27 % of MI studies), ii) preserved temporal coupling between MI and PP durations, yet with parallel increases in tasks duration compared to HPs due to the presence of a motor deficit (i.e., 54 %), iii) temporal uncoupling between MI and PP durations, or delayed RTs during implicit MI, restricted to MI involving impaired limbs (i.e., 43 %) and iv) MI (or implicit MI) impairments irrespective of clinical deficits (i.e., 19 %).
Neurophysiological Correlates
Peripheral Somatic and Neurovegetative Recordings
Peripheral somatic and neurovegetative recordings were rarely used in MI and MP studies (13 and 3 %, respectively).
EMG recordings were primarily used to ensure that MI was completed without any concomitant muscle activity, but not to evaluate MI capacities per se (e.g., Cunnington et al. 1997; Kuhn et al. 2006; Heremans et al. 2012). EMG recordings were shown reliable to differentiate MI from attempted PP with the amputated limb (Raffin et al. 2012b, a). Efficacy of MP controlled with EMG neurofeedback finally provided mixed results in STR rehabilitation (Hemmen and Seelen 2007; Hwang et al. 2010). Generally speaking, the ability to engage the somatic motor system into the production of muscle responses is altered in persons suffering from direct CNS damage (i.e., STR, SCI and PKD participants), and may not be related to MI abilities. By contrast, Heremans et al. (2012) observed that oculomotor activity elicited enabled reliable assessment of MI quality in PKD.
Electrodermal recordings were encountered in three experiments, and obtained by placing the electrodes on body regions with spared autonomic pathways in SCI participants (Grangeon et al. 2012a, b; Di Rienzo et al. 2013). Sympathetic responses duration during MI were similar to those elicited during PP, which provided objective information concerning MI quality during preliminary assessments (Grangeon et al. 2012a; Di Rienzo et al. 2013). Grangeon et al. (2012a) reported that the level of injury and autonomic dysreflexia history negatively correlated with electrodermal responses amplitude. Further reports of the autonomic nervous system correlates of MI in clinical MI research should be encouraged, because the lack of available data at this point prevents from drawing any definitive conclusions concerning their possible use and relevance for clinical evaluations of MI quality.
Central Nervous System Recordings
Transcranial Magnetic Stimulation Data
TMS findings in STR and PKD participants support that corticospinal facilitation during MI of affected body parts is diminished within the clinically affected cerebral hemisphere (Battaglia et al. 2006; Filippi et al. 2001; Tremblay et al. 2008), but otherwise intact (Filippi et al. 2001; Battaglia et al. 2006). Nonetheless, STR participants had preserved capacities to elicit an effector-specific pattern of corticospinal facilitation (Cincotta et al. 1999; Cicinelli et al. 2006; Battaglia et al. 2006). MI may thus be efficient to stimulate the corticomotor pathways and promote motor recovery (Cicinelli et al. 2006). This perspective was challenged by other TMS findings, particularly in STR participants with right hemisphere damage (Stinear et al. 2007). Participants failed to elicit corticospinal facilitation during MI of upper limb actions involving both the STR-affected and STR-unaffected sides, thus pointing out the specific role of the right hemisphere on “higher order aspects of movement planning” (Stinear et al. 2007). In the same vein, Liepert et al. (2012) reported that STR persons with severe somatosensory deficits had reduced corticospinal facilitation during MI of affected body parts as compared to STR participants without somatosensory deficits (i.e., “pure motor” STR) and HPs. The data provided evidence of the specific role of somatosensory inputs in shaping the behavioral and CNS correlates of MI. In PKD participants tested “off” medication, corticospinal facilitation of affected body parts was absent during MI, a finding interpreted in terms of PKD effects on brain motor functions (Filippi et al. 2001; Tremblay et al. 2008). In AMP participants, corticospinal facilitation during MI evidenced weakened inhibitory interactions between foot and hand motor cortices, and thus mirrored sensorimotor neuroplasticity (Marconi et al. 2007). Obviously, corticospinal facilitation was absent during MI of infra-lesional actions in SCI participants (Cramer et al. 2007). Taken together, TMS data in STR, PKD and AMP people highlight selective effects of neurologic impairments on primary sensorimotor recruitment during MI. Impaired facilitation seemed restricted to the clinically affected hemisphere in lateralized STR and PKD participants (i.e., weaker, lower or no facilitation observed as compared to HPs; or reduced facilitation compared to that elicited within the healthy cerebral hemisphere). This neurologic MI profile corroborates psychometric and behavioral observations. Analysis of whole brain imaging data is needed to understand MI changes in clinical populations.
Brain Imaging
Explicit Motor Imagery
This section focuses on brain activity during MI of impaired movements. The neural networks of MI in clinical populations systematically differed from those in HPs’. Overall, brain activity mirrored neurologic impairments and adaptive neuroplasticity (Figs. 3, 4, 5, 6 and 7; Sharma et al. 2009a, b; Cramer et al. 2005; Alkadhi et al. 2005; Hotz-Boendermaker et al. 2008; Thobois et al. 2000, 2002; Snijders et al. 2011; Lotze et al. 2001; MacIver et al. 2008).

Brain activity during MI of actions with STR-affected body parts reflecting neuroplasticity / motor recovery after stroke. Information is based on the results of brain imaging MI studies. 1: Primary motor cortex, 2: Posterior subdivision of primary motor cortex, 3: Pre-motor cortex, 4: Supplementary motor area, 5: Pre-frontal cortex, 6: Precuneus, 7: Cerebellar hemisphere, 8: Anterior subdivision of primary somatosensory cortex, 9: Frontal cortex, 10: Orbitofrontal cortex, 11: Inferior parietal lobe, 12: Anterior temporal lobe extending to insula on the ipsilateral side. Anatomical location of brain regions may be approximate for purposes of visual display. Dotted lines delineate subcortical structures. PP: Physical Practice, MI: Motor Imagery, STR: Stroke, HPs: Healthy Participants

Brain activity during MI of PKD-affected actions reflecting hypo- and compensatory activations. Information is based on the results of brain imaging MI studies. 1: Precuneus , 2: Lingual Gyrus, 3: Pre-motor cortex, 4: Anterior Cingulate cortex, 5: Inferior parietal Lobule, 6: Occipital Lobe, 7: Dorsolateral prefrontal cortex, 8: Superior Parietal Lobule, 9 : Supplementary motor area, 10: Right extrastriate body area, 11: Occipito-parietal cortex, 12: Cerebellum, 13: Primary motor cortex, 14: Cuneus , 15: Middle temporal gyrus / Visual area 5, 16: Primary somatosensory area 3a, 17: Parietal operculum, 18: Cerebellar vermis, 19: Pedunculo-pontine nucleus / Mesencephalic locomotor region, 20: Posterior hipoccampus, A = Intraparietal sulcus (Cremers et al. 2012), B = Parieto-occipital sulcus (Cremers et al. 2012). Anatomical location of brain regions may be approximate for purposes of visual display. Dotted lines delineate subcortical structures. MI: Motor Imagery, PKD: Parkinson’s Disease, HPs: Healthy Participants

Brain activity during MI of affected limb reflecting motor symptoms or the effect of treatment in Parkinson’s disease participants. Information is based on the results of brain imaging MI studies. 1: Precuneus, 2: Lingual Gyrus, 3: Pre-motor cortex (dorsal and lateral), 4: Anterior cingulated cortex, 5: Brodmann 3a, 6: Dorsal pre-motor cortex, 7: Thalamic ventral intermediate nucleus, 8: Supplementary motor area, 9: Inferior frontal gyrus, 10: Putamen, 11: Dorsolateral pre-frontal cortex, 12: Occipital cortex, 13: Mesencephalic locomotor region, 14: Posterior parietal cortex / precuneus, 15: Pre-supplementary motor area. Anatomical location of brain regions may be approximate for purposes of visual display. Dotted lines delineate subcortical structures. MI Motor Imagery, PKD Parkinson’s Disease

Brain activity during MI of movements with the amputated limb reflecting neuroplasticity after amputation. Information is based on the results of brain imaging MI studies. 1: Primary motor cortex, 2: Primary somatosensory cortex, 3: Left insula, 4: Ventral posterior lateral thalamic nucleus, 5: Supplementary motor area. Anatomical location of brain regions may be approximate for purposes of visual display. AMP: amputee, MI: Motor Imagery

Schematic representation of brain activity during MI of infra-lesional movements in SCI participants reflecting adaptive neuroplasticity. Study by Olsson et al. (2012) was considered reflecting activity-dependent rather than SCI-dependent neuroplasticity and not included in the figure. Information is based on the results of brain imaging MI studies. 1: Primary motor cortex, 2: Primary somatosensory cortex, 3: Anterior insula, 4: Premotor cortex, 5: Supplementary motor area, 6: Perigenual anterior cingulate cortex, 7: Pre-supplementary motor area, 8: Cingulate motor area, 9: Superior parietal cortex, 10: Inferior parietal cortex, 11: Pre-frontal cortex, 12: Secondary somatosensory cortex, 13: Putamen, 14: Caudate nucleus, 15: Thalamus, 16: Dorsolateral pre-frontal cortex, 17: Globus pallidus / Pallidum, 18: Pre-motor ventral, 19: Cerebellar cortex, 20: Larsell lobules HVIIA. Anatomical location of brain regions may be approximate for purposes of visual display. Dotted lines delineate subcortical structures. PP: Physical Practice, MI: Motor Imagery, HPs: Healthy Participants, SCI: Spinal Cord Injury
Brain imaging data provided evidence of preserved functional equivalence after STR. Nair et al. (2005) reported that cerebral activity reflected compensatory neuroplasticity related to the motor deficit (i.e., MI recruited similar networks as PP of actions with impaired limbs). MI also mirrored neuroplasticity associated with motor recovery (see Fig. 3; Kimberley et al. 2006; Butler and Page 2006; Sharma et al. 2009a, b; Szameitat et al. 2012). Recruitment of cortical resources within the unaffected cerebral hemisphere unveiled a STR-related compensatory network (Fig. 3; Kimberley et al. 2006; Sharma et al. 2009b; De Vico Fallani et al. 2013). Recruitment of sensorimotor and pre-motor regions within the unaffected hemisphere correlated with the clinical deficit (Sharma et al. 2009a, b). Conversely, increased recruitment of the precuneus and cerebellum, and focused recruitment of temporal and occipital regions within the unaffected hemisphere, reflected functional recovery (see Fig. 3; Nair et al. 2005; Butler and Page 2006). MI finally revealed brain motor system reorganizations which were not detectable during PP (e.g., Sharma et al. 2009a, b; Kimberley et al. 2006). Sharma et al. (2009a) observed an analogous pattern of activations during MI of affected limb in STR and HPs. However, between-group differences emerged in functional connectivity between frontal and pre-motor regions (Fig. 3). Page et al. (2009) provided fMRI evidence that MP promoted contralateral and ipsilateral sensorimotor reorganizations, with enhanced beneficial effects on motor recovery [e.g., increased scores on functional arm tests (Fulg-Meyer assessment and Action Research Arm test)] compared to PP training alone (see also results by Sun et al. 2013).
After hemi-PKD (i.e., lateralized motor symptoms), reduced activities were observed within the prefrontal, pre-motor, sensorimotor and parietal cortices of the clinically affected hemisphere (Cunnington et al. 1997; Thobois et al. 2000; Samuel et al. 2001). Changes were also reported at the subcortical level, with decreased activity in the ipsilateral cerebellum and cingulate areas (Thobois et al. 2000; Samuel et al. 2001). Hypo-activations were assumed to reflect deficits in motor preparation (Thobois et al. 2000; Samuel et al. 2001; Cunnington et al. 1997, 2001). In parallel, compensatory brain activations were observed in ipsilateral pre-motor, central and parietal regions compared to HPs (Fig. 4; Cunnington et al. 1997; Thobois et al. 2000; Samuel et al. 2001). Brain imaging thus revealed a pattern of inter-hemispheric compensation, presumably resulting from adaptive neuroplasticity. Other brain imaging data provided evidence for increased dependence on visual information during both MI and implicit MI performance, mediated by pre-motor and occipital regions (Figs. 4 and 5; Helmich et al. 2007; van Nuenen et al. 2012; Wai et al. 2012).
Specific cerebral patterns of activity characterized PKD-related motor symptoms, such as tremor, freezing of gait or the absence of medication (Fig. 5). Reduced cingulate cortex, parietal and supplementary motor area activity during MI of walking reflected difficulties in establishing somatosensory and motor predictions in freezing of gait (Snijders et al. 2011; Poliakoff 2013). These data corroborate behavioral observations by Cohen et al. (2011). Experimental results support preserved functional equivalence after PKD, but patterns of cerebral activity differed from HPs due to the effect of the disease on brain motor functions (Fig. 4; for a discursive review, see Poliakoff 2013). Functional equivalence between MI and PP seems preserved after PKD. MI thus allows the study of brain motor functions after PKD (Maillet et al. 2012). Subramanian et al. (2011) evidenced that fMRI neurofeedback enabled PKD subjects to voluntarily recruit the supplementary motor area – with similar intensities as during PP. Clinically meaningful motor improvements (i.e., increased movement speed on a finger-tapping test and reduced Unified Parkinson’s Disease Rating Scale scores) were observed after several weeks of home-based MP. These effects were not achieved by PKD participants who practiced MP without neurofeedback. The data confirm that functional equivalence with PP is a key factor underlying MP efficacy in rehabilitation.
MI of actions involving an amputated limb recruits effector-specific brain regions within the somatosensory and motor homunculi, i.e., areas previously dedicated to the control of the amputated limb (Ersland et al. 1996; Hugdahl et al. 2001; da Paz et al. 2000). Raffin et al. (2012b) provided the first fMRI evidence for a functional distinction between MI and attempted PP with an amputated upper limb. The neuro-architecture of MI was similar whether MI involved the healthy or amputated limb: “The network (…) did not appear to change according to which hand (phantom or intact) performed the task”, Raffin et al. (2012b), p. 537. Overall, functional equivalence between MI and PP is preserved after AMP. MacIver et al. (2008) observed that MP literally reversed cortical reorganizations and alleviated phantom limb pain. MI of movements with the missing upper limb after training no longer resulted in excessive bilateral activations of the primary motor and somatosensory face regions, nor within ipsilateral hand area within the primary somatosensory cortex (Fig. 6).
Extensive primary somatosensory and motor reorganizations occur after AMP. Expansion of the cortical surface corresponding to unaffected body parts towards adjacent deafferented cortical sites is well-documented (Knecht et al. 1996; Pascual-Leone et al. 1996; Karl et al. 2001; Ramachandran et al. 2010). These cortical changes were associated with the occurrence of phantom limb pain (e.g., Flor et al. 1995; Lotze et al. 2001), and termed “maladaptive plasticity”. Maladaptive plasticity was reflected in the cerebral substrates of MI (Fig. 6). Lotze et al. (2001) observed that AMP participants with phantom limb pain recruited the face area within the sensorimotor cortex during MI of hand movements, a pattern absent in pain-free AMP subjects. Diers et al. (2010) noted that only AMP participants with phantom limb pain failed to elicit primary sensorimotor activity during MI of actions executed with the phantom limb. MI thus seems to replicate a pathological state where the motor system fails to elicit the sensorimotor demand of MI. MI mirrored neuroplasticity-related differences between AMP participants with and without phantom limb pain. Rosen et al. (2001) attempted to segregate the cerebral substrates underlying phantom limb pain in a case study (Fig. 6).
Data support preservation of motor representations after SCI (Sabbah et al. 2002, 2000; Lacourse et al. 1999; Alkadhi et al. 2005; Hotz-Boendermaker et al. 2008). In spite of consistent cerebral reorganizations due to deafferentation and deefferentation (for a review, see Kokotilo et al. 2009), cerebral patterns of activity during MI were largely similar to those in HPs (Gustin et al. 2010; Hotz-Boendermaker et al. 2008; Alkadhi et al. 2005; Cramer et al. 2005; Sabbah et al. 2002). A SCI participant even showed similar changes as HPs in cerebral recruitment during MI of familiar vs. unfamiliar actions (i.e., recruitment of the pre-motor network only during MI of familiar motor acts; Olsson 2012). Nonetheless, quantitative differences were reported in SCI subjects. Compared to HPs, greater activity was observed within the contralateral primary sensorimotor cortex during MI of spared (Sabbah et al. 2002) and impaired movements (Alkadhi et al. 2005; Hotz-Boendermaker et al. 2008; Gustin et al. 2010). Reduced activation volumes were also reported (Sabbah et al. 2002; Cramer et al. 2005). Discrepancies might account for the mode of stimulus delivery and the type of MI task (i.e., with or without visual cueing; analytic vs. functional task). Hotz-Boendermaker et al. (2008) noted that MI reproduced compensatory activations assumed to reflect altered “input and output” during PP due to SCI (Fig. 7). Lacourse et al. (1999) observed that MI and attempted PP elicited analogous EEG responses from the pre-motor and primary motor cortices in participants with paraplegia and quadriplegia during MI of infra-lesional actions. Conversely, the time course of EEG responses remained dissociable between the two tasks in HPs, as revealed by cross-correlation analyses. In the same vein, Cramer et al. (2005) evidenced that the reduction in primary motor cortex activation observed during MI compared to PP in HPs was absent in participants with SCI. Alkadhi et al. (2005) reported that during MI of foot movements, SCI participants recruited neural networks underlying both PP and MI in HPs with higher activation intensities. Higher levels of primary sensorimotor activity and poor changes in primary motor cortex activation intensities between MI and PP suggests strengthened functional equivalence after SCI (Fig. 7). The hypothesis of weakened motor inhibition was advanced (Lacourse et al. 1999). SCI participants may no longer require inhibiting motor output during MI since spinal damage prevents the transmission of the neural orders to the peripheral effectors (Lacourse et al. 1999). Albeit this hypothesis remained an inference, a direct link between sites of inhibitory activity and primary motor cortex activation during MI was recently evidenced with magnetoencephalography (Di Rienzo et al. 2013).
Only one study investigated MP-induced neuroplasticity after SCI (Cramer et al. 2007). SCI participants benefited from MP to improve performance of spared motor functions (i.e., increased speed of execution of sequential tongue movements). Motor improvements were associated with increased putamen and globus pallidus activation (Fig. 7; Cramer et al. 2007). MP was also delivered to alleviate neuropathic pain after SCI, which was associated with maladaptive plasticity within the primary somatosensory and motor cortices (Wrigley et al. 2009; see Gustin et al. 2008 for a brief discussion). MI of purely analytic infra-lesional movements failed to alleviate, and worsened below-level neuropathic pain (Gustin et al. 2008). Gustin et al. (2010) evidenced MI-related activations within the pain neural matrix which correlated with pain increases (Fig. 7). It is possible that MI elicits a conflicting state of body awareness due to mismatching between motor output and sensory input (Moseley 2007; Harris 1999). MI of walking, conversely, decreased at- and below-level neuropathic pain, yet to a lesser extent than walking within a virtual environment (Moseley 2007). Functional tasks involving congruent representations of the whole body might contribute to restore coherence in a mismatching state of body awareness (Moseley 2007; Harris 1999). Isolated MI of neurologically impossible movements might cause an opposite effect (Gustin et al. 2008, 2010).
Implicit Motor Imagery
Following STR, Yan et al. (2012) observed impaired cognitive processing during the different cognitive sub-stages of implicit MI (i.e., spatial encoding and mental rotation), due to weaker frontal, central and parietal activity within the stroke-affected hemisphere. In PKD participants, fMRI recordings revealed that complex tasks involving PKD-affected limbs recruited a compensatory visual network (i.e., including the extrastriate visual area and the parieto-occipital cortex; Helmich et al. 2007). These findings were recently confirmed by TMS (van Nuenen et al. 2012). Interestingly, tremor in PKD improved neural function within a cortical-subcortical somatosensory and pre-motor network underlying increased implicit MI performance. The ventral intermediate nucleus showed both tremor-related and implicit MI-related activity. The ventral intermediate nucleus projects to the somatosensory cortex, where the activity was superior during implicit MI in tremulous compared to non-tremulous PKD subjects (Helmich et al. 2011).
Motor Imagery Profiles Based on Neurophysiological Data
MI Capacities in Clinical Populations
We reviewed to which extent psychological, behavioral and neurophysiological correlates of MI were affected by neurologic disorders. Several neurologic MI (and implicit MI) profiles emerged based on psychometric and behavioral evaluations. Psychometric and behavioral correlates of MI yielded either preserved or selective MI deficits corresponding to the motor impairments (Tables 4 and 5). Two additional profiles were specific to behavioral evaluations (i.e., temporal coupling preserved but reflecting the timing of slower motor performance on impaired actions; and impaired temporal coupling irrespective of the actual motor deficit; Table 5). Neurophysiological findings systematically underlined differences with HPs when participants with motor disabilities engaged into MI of clinically affected movements. Functional equivalence was nonetheless preserved, MI recruiting the reorganized motor networks of PP. Brain correlates thus mirrored brain changes due to the neurologic disease or related to adaptive neuroplasticity (Figs. 3, 4, 5, 6 and 7). This might account for the large prevalence of MI profiles reflecting actual motor impairments (Tables 4 and 5). Brain imaging data thus strongly challenged the assumption that movements which can no longer be physically performed “cannot be imagined in a way that is necessary for functional equivalence” (Olsson and Nyberg 2010).
Motor Imagery Profile After Spinal or Peripheral Damage
When the neurologic pathology did not involve direct cerebral damage, i.e., after SCI and AMP, psychological and behavioral correlates of MI were poorly affected (Tables 4 and 5). Changes might occur in AMP, but were restricted to MI of the missing limb (Table 4 and 5). Brain imaging investigations of MI in SCI and AMP participants revealed that the cerebral networks underlying PP and MI were reorganized in parallel. Cerebral activity during MI largely overlaps with that in HPs in SCI, or with that of the unaffected limb in AMP subjects. An interesting finding in AMP is that behavioral and neurophysiological correlates of MI support integration of functional limb prosthesis to the body schema (Lotze et al. 2001; Malouin et al. 2009a; Nico et al. 2004). AMP and SCI primarily affected the cerebral correlates of MI through quantitative changes related to neuroplasticity. Since there is no direct cerebral damage, motor representations may be alimented by other sources of sensory input than proprioceptive afferents form impaired body parts (e.g., action observation in SCI participants and sensory input from unaffected body parts in AMP participants). This would explain preservation of psychometric and behavioral MI performance.
Motor Imagery Profile After Cerebral Damage and Disorders
When the neurologic pathology involved direct damage to cerebral structures, i.e., after STR and PKD, psychological and behavioral correlates of MI tended to differ from HPs. Deficits often related to clinical impairments. STR and PKD both induced primarily qualitative changes in cerebral recruitment during MI. Brain imaging data revealed compensatory patterns of cerebral activity, presumably reflecting adaptive neuroplasticity. Importantly, compensatory neural circuits can be targeted by MP. Changes in brain activity during MI and implicit MI compared to HPs might account for psychometric and behavioral MI deficits. Yet, brain changes do not necessarily imply MI deficits (Table 4 and 5). Compensatory neural networks may vicariate anterior implicit MI functions, thus resulting in spared implicit MI performance (e.g., van Nuenen et al. 2012; Johnson et al. 2002).
Theoretical Implications
Integrating Cognitive and Motor Deficits Within Motor Imagery Evaluation Frameworks
Present literature analysis revealed that motor incapacities were strong and reliable predictors of MI capacities after both acute and progressive neurologic disorders. MI was preserved, or altered according to motor impairments in more than 85 % of MI studies. We advocate that MI evaluation frameworks should take into account current motor capacities when determining the standards for “high” MI capacities in these populations. More precisely, a rigorous framework should encompass three distinct levels of analysis to delineate the MI profile:
-
i.
Reference to MI correlates for an action that the participant can perform physically (e.g., movements involving spared effectors in participants with lateralized motor deficits, MI of movements innervated above the neurologic level of SCI).
-
ii.
Reference to MI evaluation standards (e.g., temporal equivalence, scoring threshold for MI questionnaires, recruitment of motor / pre-motor sites during MI, etc.).
-
iii.
Reference to MI performance in HPs undergoing similar evaluations.
Also, most reviewed experiments screened participants with severe cognitive deficits, usually on the basis of the “Mini Mental State Evaluation” (Folstein et al. 1975). Independent testing of working memory in MI designs (Malouin et al. 2004a, 2012; Hovington and Brouwer 2010) and body schema integrity in implicit MI designs (Coslett 1998; Daprati et al. 2010; Tomasino et al. 2003; Nico et al. 2004) may be legitimate on the basis of available scientific data.
Combining Evaluation Methods to Determine the MI Profile
MI and implicit MI paradigms address different components of motor cognition. Among studies assessing both MI and implicit MI performance within the same sample of participants (6 studies involving STR or PKD participants), results between the two evaluation methods were congruent in 40 % of cases (i.e., assessments yielded similar neurologic MI profiles). Of importance, MI profiles cohabitated within a same clinical population for a given evaluation method (Tables 4 and 5). No disease-related characteristics unambiguously predicted such variability. Some MI profiles were more prevalent than others for a given neurologic disease (Tables 4 and 5; STR participants presenting higher variability in MI profiles, which might reflect the variability of the STR lesions and resulting neuroplasticity). In studies involving more than one MI evaluation method (i.e., psychometric, behavioral and neurophysiological), neurologic MI profiles were redundant across evaluation methods in only 45 % of cases. Clinical data confirmed that each type of evaluation addresses a distinct component of MI – hence are complementary (Guillot and Collet 2005a).
As stated by Dettmers et al. (2012): “There is no single and uniform test that can categorize patients’ ability or disability to perform MI”. Literature data strongly supports this view, and, for clinicians, determining the neurologic MI profile may be a relevant and justified approach to this issue. Assessing MI profiles would ideally require a battery of tests combining psychological, behavioral and neurophysiological methods. As subjective and objective MI assessment methods “generally tend (…) to dissociate” these should be combined in priority (Dettmers et al. 2012; Lequerica et al. 2002). For instance, at least psychometric and behavioral methods should be used (see Dickstein et al. 2013 for a relevant illustration). A remarkable assessment battery used to determine participant’s inclusion within MI / MP experiments is the “chaotic” assessment battery (Simmons et al. 2008; Sharma et al. 2008, 2009a, b). There are nonetheless several shortcomings related to the use of this method in clinical research.
Crossing the Bridge Between Psychometric and Behavioral Motor Imagery Correlates and Functional Equivalence
A major finding of the present review is that neurologic deficits resulted in specific patterns of altered subjective experience of MI or temporal equivalence, respectively impacting psychometric and behavioral evaluations in spite of preserved functional equivalence. Relating psychometric and behavioral MI data to functional equivalence patterns is therefore an absolute necessity in order to promote translations from bench to bedside in clinical MI research, which appeared quite limited at this point. This should contribute to delineate the optimal rules for control of MI training in order to promote MP-dependant neuroplasticity. For instance, there may be a positive correlation between MI vividness and primary somatosensory and motor cortex stimulation during MI of impaired actions in AMP and SCI subjects (Lotze et al. 2001; Alkadhi et al. 2005). Confalonieri et al. (2012) described a negative correlation between MI ease of the affected hand (i.e., kinesthetic and visual MIQ-RS subscores) and the percentage of fMRI blood oxygenation level-dependant signal changes within contralesional sensorimotor and pre-motor cortices and ipsilesional hippocampus. Data by Confalonieri et al. (2012) bring decisive insights to current understandings of MI ability in the context of clinical rehabilitation: MI may stimulate primary sensorimotor and pre-motor networks in spite of poor MI ease. Kimberley et al. (2006), however, observed comparable patterns of sensorimotor and pre-motor cortex activity in subgroups of STR participants with high and one with low MI ease scores [see also Cramer et al. (2005) for analogous results in SCI participants]. Overall, the relationship between behavioral and psychometric correlates of MI and functional equivalence remains unexplored, and results may go against preliminary conceptions.
Practical Implications
At this point, the high variability of evaluation methods encountered in clinical MI experiments hampers prescriptive generalizations related to ‘good MI evaluation practice’. Nonetheless, theoretical principles for MI evaluation, rather than practical prescriptions for clinicians, emerged. While the development of further standardized procedures must be encouraged, and their use preferred for homogeneity and reproducibility of results across paradigms, many evaluation techniques can be adapted to the specific context of each clinical experiment (Table 3), and provide reliable information if standardized assessment procedures meeting protocol’s requirements in terms of specificity are unavailable.Footnote 4 There may also be strong complementarities between the two approaches. For instance, standardized behavioral tests can be relevantly combined with ease and vividness self-reports (see Heremans et al. 2011 for a relevant illustration).
Evaluation Methods in Mental Practice Studies
In MP studies, psychological and behavioral MI evaluations suited purposes of i) preliminary MI assessment and ii) control of MP. The two evaluation methods were, however, rarely used concurrently. Their combination should be encouraged to provide complementary information on MI quality (Table 3). Evaluation procedures, as long as they integrate key principles for reliable clinical MI evaluations (Table 2) are infinite in essence and should not be a priori restricted to existing standardized tests.
Albeit obvious, MI evaluations in MP designs should be primarily conducted on tasks involving peripheral effectors involved in MP programs, e.g., simple single-joint actions involving effectors impaired by the pathology (analytic motor functions targeted in physiotherapy) or goal-directed actions with a clear functional purpose (finalized motor sequences usually targeted in occupational therapy) of graded complexity along the course of the intervention (Dickstein et al. 2004; Dunsky et al. 2006; Craje et al. 2010; Grangeon et al. 2012b; Beaumont et al. 2011; Braun et al. 2008). Self-report ratings and chronometric recordings are easily adaptable to such motor tasks. Caution should be exercised as data might mirror motor impairments, yet should not be considered markers of degraded MI quality. Task duration should ideally range from 5 to 25 s (Table 2), to avoid deleterious effects on isochrony (Guillot et al. 2012b). Finally, MI durations must be controlled during MP, and resemble those of the corresponding motor performance to achieve the desired transfer effects on motor behaviors (see data by Louis et al. 2008 for a relevant illustration).
Standardized psychometric and behavioral assessments initially developed for HPs, as well as implicit MI evaluations, may not convey critical information regarding the specific MI skills required to benefit from MP. Such tests should nonetheless not be excluded from MP designs, but preferentially used for the purpose of preliminary assessments, or to familiarize participants with MI (Dominey et al. 1995; Thobois et al. 2002; Snijders et al. 2011). Standardized psychometric and behavioral evaluations provide general information concerning MI capacities, and are reproducible. In the case of persons with severe motor impairments, questionnaire items referring to actions that participants can no longer perform, or with difficulties, should be considered separately in data analysis, or even removed (Dickstein et al. 2004; see also KVIQ-10, which provides a simplified version of the KVIQ; Malouin et al. 2007; Schuster et al. 2012c). To summarize, standardized methods may primarily suit purposes of preliminary MI assessments, whereas non-standardized psychometric and behavioral evaluations may be particularly relevant to control MP.
Evaluation Methods in Motor Imagery Studies
In MI studies, assessment methods were regularly combined (i.e., 50 % of cases; e.g., use of chronometric measures to ensure phase-locked recordings of brain activity during MI). When only one evaluation method was being used, evaluations were typically conducted across several tasks with varying motor and perceptual demands (Sirigu et al. 1996; Johnson et al. 2002).
Explicit Motor Imagery Experiments
Detailed information about the MI modality was missing in 39 % of brain imaging studies. This is surprising as MI modalities involve different levels of functional equivalence with PP, particularly with regards to the recruitment of primary somatosensory and motor structures (Solodkin et al. 2004; Guillot et al. 2009; Lorey et al. 2009). To assist practitioners in the elaboration of fruitful MP designs, future MI studies should address the neural underpinnings of different MI modalities, along with their psychometric and behavioral correlates. For instance, people with neurologic diseases may present reduced capacities to use first-person perspective compared to more external modalities, as revealed by psychometric evaluations (Li 2000; Dettmers et al. 2012; Schuster et al. 2012c). Furthermore, most reviewed experiments involved MI of self-paced movements, and the basic movement parameters were insufficiently described (e.g., speed, repetition rate, amount of force). This may introduce uncertainties in data interpretation, because movement parameters are known to be reflected, for instance, in the brain correlates of MI in HPs (Sauvage et al. 2013).
Reviewed MI studies consisted of transversal experiments focusing on subjects exhibiting stabilized motor impairments. MI research protocols should now consider determining how the psychological, behavioral and neurophysiological correlates of MI are altered in a longitudinal fashion, e.g., during acute, subacute and chronic stages of neurologic disorders. For instance, neuroimaging findings may be a function of time after injury. At this point, we only found one study explicitly addressing this issue, on the basis of single-case chronometric evaluations (Sabate et al. 2007). There is thus a literature gap in this area that needs to be addressed in future experiments.
Implicit Motor Imagery Experiments
Guillot et al. (2012b) underlined that contrary to MI experiments, implicit MI paradigms required forming mental images as fast as possible. MP designs almost never involved implicit MI tasks. Implicit MI evaluations appeared of primary interest for fundamental research issues related to body schema integrity (Nico et al. 2004; Coslett 1998). Nonetheless, data in HPs support that implicit MI such as mental rotation of body parts may not systematically involve motor-related cognitive strategies (Ionta et al. 2012; Conson et al. 2012; Brady et al. 2011; Ni Choisdealbha et al. 2011; Hoyek et al. 2013). These tasks may be solved using purely visual / allocentric cognitive strategies (Hoyek et al. 2013). Data in STR, SCI and AMP participants suggest that MI may promote visual, rather than motor, cognitive strategies. Daprati et al. (2010) evidenced that severely affected STR participants used visual strategies to compensate deficient access to their body schema. STR subjects with mild motor deficit, however, kept referring to their body schema, and showed implicit MI deficits corresponding to their motor incapacities. Likewise, Nico et al. (2004) argued that reduced implicit MI performance in AMP participants could:
To control the use of visual strategies during implicit MI, oral debriefs were used (Nico et al. 2004). Implicit MI data in PKD subjects revealed a neural circuitry for visual compensation during implicit MI (van Nuenen et al. 2012; Helmich et al. 2007), while after SCI, Fiori et al. (2013) provided evidence that implicit MI may no longer involve manipulation of motor representations at all.
Accordingly, extreme caution should be taken when interpreting implicit MI results in clinical populations with severe and chronic motor deficits. Albeit not intuitive, high implicit MI performance (e.g., absence of burst in error rate during recognition of body limbs presented in unfamiliar orientations) may reflect body schema disorders. Particularly, it may indicate use of other strategies than manipulation of motor representations (Fiori et al. 2013; Daprati et al. 2010; Curtze et al. 2010). Complex implicit MI tasks finally appeared more suitable to unveil implicit MI limitations in STR, PKD, SCI and AMP subjects (Nico et al. 2004; Johnson et al. 2002; Helmich et al. 2007; Fiori et al. 2013).
Participant’s Eligibility to Mental Practice
Motor Imagery
In spite of a large body of neuroscience research, it remains unexplored whether high MI skills are necessary to benefit from MP. As recently pointed out by Braun et al. (2011): “at this point (…) it is not known if being able to perform mental imagery necessarily equates to benefiting from it in clinical practice”. Accordingly, screening subjects on the basis of their MI capacities should also be done with extreme caution.
Nonetheless, could screening participants on the basis of their MI capacities be relevant? The possible induction of activity-dependant neuroplasticity by MI training, because of functional equivalence with PP, remains the central component of fruitful MP interventions in rehabilitation, even in the management of non-motor disabilities (e.g., MacIver et al. 2008). An important literature-driven implication is that determining eligibility to MP based on MI capacities should not be screening for high MI skills per se, but determining whether functional equivalence is preserved based on the neurologic MI profile. Along this perspective, implicit MI tests have poor predictive power. For instance, MI experiments revealed that the psychometric, behavioral and neurophysiological correlates of MI, when performed with a high degree of functional equivalence with PP in neurologic populations, differed from those in HPs due to pathologic / adaptive brain changes. The systematic literature review leads to the postulate that, in STR, PKD, SCI and AMP people, i) intact MI capacities (i.e., psychometric and behavioral MI profiles 1 in Tables 4 and 5, or identical brain activity during MI as HPs; or ii) specific MI deficits corresponding to the effect of the disease on actual motor capacities (i.e., psychometric MI profile 2 in Table 4, behavioral MI profiles 2–3 in Table 5, see also Figs. 3, 4, 5, 6 and 7 for brain activation during MI reflecting reorganization of PP motor networks), may reflect intact functional equivalence.
Characteristics of the Neurologic Disease
Present literature review did not unambiguously afford to isolate neurologic characteristics (e.g., lesion type, severity) that hampered MP efficacy. To our knowledge, only one study established a link between the nature of the neurologic damage and the clinical outcome of MP. Butler and Page (2006) reported that a STR participant suffering from a large left parietal cortex lesion failed to benefit from MI training because of reduced MI capacities. Subjects with parietal strokes were a priori excluded from some MP studies (Page et al. 2011a, b). Nonetheless, “screening on the basis of lesion location might be insufficient” (see also conclusions by Schuster et al. 2012c; citation by Simmons et al. 2008). Indeed, STR damage to parietal regions did not systematically resulted in degraded MI capacities across reviewed experiments. Neuroplasticity occurs after STR, which might allow spared brain regions to be “progressively vicarious” of the functions assumed by damaged neurons (Rossini and Pauri 2000). This advocates for more systematic MI evaluations in future MP protocols, which should be clearly preferred to a priori eligibility statements not being supported by data.
By contrast, the repercussion of the neurologic pathology on high-order cognitive functions quasi-systematically hampered the benefits of MP. Particularly, working memory impairment in persons with STR, that nonetheless successfully completed the TDMI test (Table 2), negatively correlated with MP efficacy (Malouin et al. 2004a). In PKD participants, Yaguez et al. (1999) established a direct link between working memory impairments and negative outcome of MP, while Braun et al. (2011) observed that PKD subjects with mild cognitive impairments benefited more from MP than PKD subjects with severe cognitive deficits.
Repeated Motor Imagery Evaluations
STR, SCI, PKD and AMP subjects who benefited from restorative interventions improved their MI capacities (Deutsch et al. 2012; Butler and Page 2006; de Vries et al. 2011; Stevens and Stoykov 2003; Cunnington et al. 2001; Dominey et al. 1995; MacIver et al. 2008; McAvinue and Robertson 2011; Beaumont et al. 2011; Gustin et al. 2010). Participants should thus not be excluded on the basis of a single MI evaluation. This advocates for repeated assessments to define the baseline level of mental performance. MP designs frequently involved repeated PP assessments before delivery of MP. Repeated MI assessments could therefore be easily included, thereby providing adequate control of learning effects. If MI is assessed once, extended familiarization sessions should be considered (see Wondrusch and Schuster 2013 for a standardized procedure). For instance, some authors trained participants to perform MI until they reached the desired level of vividness or isochrony (Lotze et al. 2001; Battaglia et al. 2006; Cremers et al. 2012).
General Conclusion
Neurologic disorders such as STR, SCI, PKD and AMP impact the psychological, behavioral and neurophysiological correlates of MI, thus resulting in highly specific profiles of MI capacities. Functional equivalence between MI and PP was overall preserved. However, cerebral activity reflected structural and functional neuroplasticity. Brain changes were echoed on a congruent fashion in the psychometric and behavioral correlates of MI. Further research is needed to determine the psychometric and behavioral markers of functional equivalence in clinical populations. MI capacities may be degraded per se is some specific cases, but primarily due to the effect of the neurologic pathology on higher order cognitive functions. Such patterns of MI impairments were only observed in certain cases of STR and PKD. After AMP and SCI, cerebral structures remain intact but reshaped. Disturbances of body schema primarily affected implicit MI, particularly during complex tasks involving manipulation of mental representations of affected body parts. These results have strong implications regarding the means of assessment and control of MI in future experiments. A large number of methods allow rigorous MI assessments in MI and MP designs, but these should be combined to determine the neurologic MI profile in the perspective of eligibility to MP.
Notes
Participants with motor deficits are usually requested to press an answer command with lesser or unaffected body parts, or on the basis of eye movements, so as to prevent a confounding effect of motor deficits on RTs.
There are many examples in the MP literature of such tests with STR, PKD, SCI and AMP people.
References
Abbruzzese, G., Assini, A., Buccolieri, A., Marchese, R., & Trompetto, C. (1999). Changes of intracortical inhibition during motor imagery in human subjects. Neuroscience Letters, 263(2–3), 113–116.
Alkadhi, H., Brugger, P., Boendermaker, S. H., Crelier, G., Curt, A., Hepp-Reymond, M. C., et al. (2005). What disconnection tells about motor imagery: evidence from paraplegic patients. Cerebral Cortex, 15(2), 131–140. doi:10.1093/cercor/bhh116.
Amick, M. M., Schendan, H. E., Ganis, G., & Cronin-Golomb, A. (2006). Frontostriatal circuits are necessary for visuomotor transformation: mental rotation in Parkinson’s disease. Neuropsychologia, 44(3), 339–349. doi:10.1016/j.neuropsychologia.2005.06.002.
Annett, J. (1995). Motor imagery: perception or action? Neuropsychologia, 33(11), 1395–1417.
Bakker, F. C., Boschker, M. S. J., & Chung, T. (1996). Changes in muscular activity while imagining weight lifting using stimulus or response propositions. Journal of Sport & Exercise Psychology, 18, 313–324.
Battaglia, F., Quartarone, A., Ghilardi, M. F., Dattola, R., Bagnato, S., Rizzo, V., et al. (2006). Unilateral cerebellar stroke disrupts movement preparation and motor imagery. Clinical Neurophysiology, 117(5), 1009–1016. doi:10.1016/j.clinph.2006.01.008.
Beaumont, G., Mercier, C., Michon, P. E., Malouin, F., & Jackson, P. L. (2011). Decreasing phantom limb pain through observation of action and imagery: a case series. Pain Medicine, 12(2), 289–299. doi:10.1111/j.1526-4637.2010.01048.x.
Berthoz, A. (1996). The role of inhibition in the hierarchical gating of executed and imagined movements. Brain Research. Cognitive Brain Research, 3(2), 101–113.
Bonnet, M., Decety, J., Jeannerod, M., & Requin, J. (1997). Mental simulation of an action modulates the excitability of spinal reflex pathways in man. Cognit Brain Res, 5(3), 221–228. doi:10.1016/S0926-6410(96)00072-9.
Boschker, M. S. J. (2001). Action-based imagery: on the nature of mentally imagined motor actions. Amsterdam: University of Amsterdam.
Bowering, K. J., O’Connell, N. E., Tabor, A., Catley, M. J., Leake, H. B., Moseley, G. L., et al. (2013). The effects of graded motor imagery and its components on chronic pain: a systematic review and meta-analysis. The Journal of Pain, 14(1), 3–13. doi:10.1016/j.jpain.2012.09.007.
Brady, N., Maguinness, C., & Ni Choisdealbha, A. (2011). My hand or yours? Markedly different sensitivity to egocentric and allocentric views in the hand laterality task. PLoS One, 6(8), e23316. doi:10.1371/journal.pone.0023316.
Braun, S., Kleynen, M., Schols, J., Schack, T., Beurskens, A., & Wade, D. (2008). Using mental practice in stroke rehabilitation: a framework. Clinical Rehabilitation, 22(7), 579–591. doi:10.1177/0269215508090066.
Braun, S. M., van Haastregt, J. C., Beurskens, A. J., Gielen, A. I., Wade, D. T., & Schols, J. M. (2010). Feasibility of a mental practice intervention in stroke patients in nursing homes; a process evaluation. BMC Neurology, 10, 74. doi:10.1186/1471-2377-10-74.
Braun, S., Beurskens, A., Kleynen, M., Schols, J., & Wade, D. (2011). Rehabilitation with mental practice has similar effects on mobility as rehabilitation with relaxation in people with Parkinson’s disease: a multicentre randomised trial. Journal of Physiotherapy, 57(1), 27–34. doi:10.1016/S1836-9553(11)70004-2.
Braun, S., Kleynen, M., van Heel, T., Kruithof, N., Wade, D., & Beurskens, A. (2013). The effects of mental practice in neurological rehabilitation; a systematic review and meta-analysis. Frontiers in Human Neuroscience, 7, 390. doi:10.3389/fnhum.2013.00390.
Butler, A. J., & Page, S. J. (2006). Mental practice with motor imagery: evidence for motor recovery and cortical reorganization after stroke. Archives of Physical Medicine and Rehabilitation, 87(12 Suppl 2), S2–11. doi:10.1016/j.apmr.2006.08.326.
Butler, A. J., Cazeaux, J., Fidler, A., Jansen, J., Lefkove, N., Gregg, M., et al. (2012). The Movement Imagery Questionnaire-Revised, Second edition (MIQ-RS) is a reliable and valid tool for evaluating motor imagery in stroke populations. Evidence-based Complementary and Alternative Medicine, 2012, 497289. doi:10.1155/2012/497289.
Buxbaum, L. J., Johnson-Frey, S. H., & Bartlett-Williams, M. (2005). Deficient internal models for planning hand-object interactions in apraxia. Neuropsychologia, 43(6), 917–929. doi:10.1016/j.neuropsychologia.2004.09.006.
Cicinelli, P., Marconi, B., Zaccagnini, M., Pasqualetti, P., Filippi, M. M., & Rossini, P. M. (2006). Imagery-induced cortical excitability changes in stroke: a transcranial magnetic stimulation study. Cerebral Cortex, 16(2), 247–253. doi:10.1093/cercor/bhi103.
Cincotta, M., Tozzi, F., Zaccara, G., Borgheresi, A., Lori, S., Cosottini, M., et al. (1999). Motor imagery in a locked-in patient: evidence from transcranial magnetic stimulation. Italian Journal of Neurological Sciences, 20(1), 37–41.
Clark, S., Tremblay, F., & Ste-Marie, D. (2004). Differential modulation of corticospinal excitability during observation, mental imagery and imitation of hand actions. Neuropsychologia, 42(1), 105–112.
Cohen, R. G., Chao, A., Nutt, J. G., & Horak, F. B. (2011). Freezing of gait is associated with a mismatch between motor imagery and motor execution in narrow doorways, not with failure to judge doorway passability. Neuropsychologia, 49(14), 3981–3988. doi:10.1016/j.neuropsychologia.2011.10.014.
Collet, C., & Guillot, A. (2009). Peripheral responses elicited by motor imagery: A window on central and peripheral nervous system relationships through motor commands inhibition. In S. P. Weingarten & H. O. Penat (Eds.), Cognitive psychology research developments (pp. 1–17). United States: Nova.
Collet, C., Guillot, A., Lebon, F., MacIntyre, T., & Moran, A. (2011). Measuring motor imagery using psychometric, behavioral, and psychophysiological tools. Exercise and Sport Sciences Reviews, 39(2), 85–92. doi:10.1097/JES.0b013e31820ac5e0.
Collet, C., Di Rienzo, F., El Hoyek, N., & Guillot, A. (2013). Autonomic nervous system correlates in movement observation and motor imagery. Frontiers in Human Neuroscience, 7, 415. doi:10.3389/fnhum.2013.00415.
Confalonieri, L., Pagnoni, G., Barsalou, L. W., Rajendra, J., Eickhoff, S. B., & Butler, A. J. (2012). Brain activation in primary motor and somatosensory cortices during motor imagery correlates with motor imagery ability in stroke patients. ISRN Neurol, 2012, 613595. doi:10.5402/2012/613595.
Conson, M., Mazzarella, E., Donnarumma, C., & Trojano, L. (2012). Judging hand laterality from my or your point of view: interactions between motor imagery and visual perspective. Neuroscience Letters, 530(1), 35–40. doi:10.1016/j.neulet.2012.09.051.
Coslett, H. B. (1998). Evidence for a disturbance of the body schema in neglect. Brain and Cognition, 37(3), 527–544. doi:10.1006/brcg.1998.1011.
Craje, C., van der Graaf, C., Lem, F. C., Geurts, A. C., & Steenbergen, B. (2010). Determining specificity of motor imagery training for upper limb improvement in chronic stroke patients: a training protocol and pilot results. International Journal of Rehabilitation Research, 33(4), 359–362. doi:10.1097/MRR.0b013e32833abe8e.
Cramer, S. C., Lastra, L., Lacourse, M. G., & Cohen, M. J. (2005). Brain motor system function after chronic, complete spinal cord injury. Brain, 128(Pt 12), 2941–2950. doi:10.1093/brain/awh648.
Cramer, S. C., Orr, E. L., Cohen, M. J., & Lacourse, M. G. (2007). Effects of motor imagery training after chronic, complete spinal cord injury. Experimental Brain Research, 177(2), 233–242. doi:10.1007/s00221-006-0662-9.
Cremers, J., D’Ostilio, K., Stamatakis, J., Delvaux, V., & Garraux, G. (2012). Brain activation pattern related to gait disturbances in Parkinson’s disease. Movement Disorders, 27(12), 1498–1505. doi:10.1002/mds.25139.
Cunnington, R., Iansek, R., Johnson, K. A., & Bradshaw, J. L. (1997). Movement-related potentials in Parkinson’s disease. Motor imagery and movement preparation. Brain, 120(Pt 8), 1339–1353.
Cunnington, R., Egan, G. F., O’Sullivan, J. D., Hughes, A. J., Bradshaw, J. L., & Colebatch, J. G. (2001). Motor imagery in Parkinson’s disease: a PET study. Movement Disorders, 16(5), 849–857.
Curtze, C., Otten, B., & Postema, K. (2010). Effects of lower limb amputation on the mental rotation of feet. Experimental Brain Research, 201(3), 527–534. doi:10.1007/s00221-009-2067-z.
da Paz, A. C., Jr., Braga, L. W., & Downs, J. H., 3rd. (2000). A preliminary functional brain study on amputees. Applied Neuropsychology, 7(3), 121–125. doi:10.1207/s15324826an0703_1.
Danckert, J., Ferber, S., Doherty, T., Steinmetz, H., Nicolle, D., & Goodale, M. A. (2002). Selective, non-lateralized impairment of motor imagery following right parietal damage. Neurocase, 8(3), 194–204. doi:10.1093/neucas/8.3.194.
Daprati, E., Nico, D., Duval, S., & Lacquaniti, F. (2010). Different motor imagery modes following brain damage. Cortex, 46(8), 1016–1030. doi:10.1016/j.cortex.2009.08.002.
Dayan, E., Censor, N., Buch, E. R., Sandrini, M., & Cohen, L. G. (2013). Noninvasive brain stimulation: from physiology to network dynamics and back. Nature Neuroscience, 16(7), 838–844. doi:10.1038/nn.3422.
De Vico Fallani, F., Pichiorri, F., Morone, G., Molinari, M., Babiloni, F., Cincotti, F., et al. (2013). Multiscale topological properties of functional brain networks during motor imagery after stroke. NeuroImage, 83C, 438–449. doi:10.1016/j.neuroimage.2013.06.039.
de Vries, S., Tepper, M., Otten, B., & Mulder, T. (2011). Recovery of motor imagery ability in stroke patients. Rehabil Res Pract, 2011, 283840. doi:10.1155/2011/283840.
Decety, J. (1993). Should motor imagery be used in physiotherapy? Recent advances in cognitive neurosciences. Physiotherapy Theory and Practice, 9(4), 193–203. doi:10.3109/09593989309036491.
Decety, J., & Boisson, D. (1990). Effect of brain and spinal cord injuries on motor imagery. European Archives of Psychiatry and Clinical Neuroscience, 240(1), 39–43.
Decety, J., & Grezes, J. (1999). Neural mechanisms subserving the perception of human actions. Trends in Cognitive Science, 3(5), 172–178.
Decety, J., & Michel, F. (1989). Comparative analysis of actual and mental movement times in two graphic tasks. Brain and Cognition, 11(1), 87–97.
Decety, J., Jeannerod, M., & Prablanc, C. (1989). The timing of mentally represented actions. Behavioural Brain Research, 34(1–2), 35–42.
Demougeot, L., & Papaxanthis, C. (2011). Muscle fatigue affects mental simulation of action. Journal of Neuroscience, 31(29), 10712–10720. doi:10.1523/JNEUROSCI.6032-10.2011.
Dettmers, C., Benz, M., Liepert, J., & Rockstroh, B. (2012). Motor imagery in stroke patients, or plegic patients with spinal cord or peripheral diseases. Acta Neurologica Scandinavica. doi:10.1111/j.1600-0404.2012.01680.x.
Deutsch, J. E., Maidan, I., & Dickstein, R. (2012). Patient-centered integrated motor imagery delivered in the home with telerehabilitation to improve walking after stroke. Physical Therapy, 92(8), 1065–1077. doi:10.2522/ptj.20110277.
Di Rienzo, F., Collet, C., Hoyek, N., & Guillot, A. (2012). Selective effect of physical fatigue on motor imagery accuracy. PLoS One, 7(10), e47207. doi:10.1371/journal.pone.0047207.
Di Rienzo, F., Guillot, A., Daligault, S., Delpuech, C., Rode, G., & Collet, C. (2013). Motor inhibition during motor imagery: a MEG study with a quadriplegic patient. Neurocase, doi:10.1080/13554794.2013.826685.
Dickstein, R., Dunsky, A., & Marcovitz, E. (2004). Motor imagery for gait rehabilitation in post-stroke hemiparesis. Physical Therapy, 84(12), 1167–1177.
Dickstein, R., Gazit-Grunwald, M., Plax, M., Dunsky, A., & Marcovitz, E. (2005). EMG activity in selected target muscles during imagery rising on tiptoes in healthy adults and poststroke hemiparetic patients. Journal of Motor Behavior, 37(6), 475–483. doi:10.3200/JMBR.37.6.475-483.
Dickstein, R., Deutsch, J. E., Yoeli, Y., Kafri, M., Flash, F., Dunsky, A., et al. (2013). Effects of integrated motor imagery practice on gait of individuals with chronic stroke: a half-cross-over randomized study. Archives of Physical Medicine and Rehabilitation. doi:10.1016/j.apmr.2013.06.031.
Diers, M., Christmann, C., Koeppe, C., Ruf, M., & Flor, H. (2010). Mirrored, imagined and executed movements differentially activate sensorimotor cortex in amputees with and without phantom limb pain. Pain, 149(2), 296–304. doi:10.1016/j.pain.2010.02.020.
Dijkerman, H. C., Ietswaart, M., Johnston, M., & MacWalter, R. S. (2004). Does motor imagery training improve hand function in chronic stroke patients? A pilot study. Clinical Rehabilitation, 18(5), 538–549.
Dominey, P., Decety, J., Broussolle, E., Chazot, G., & Jeannerod, M. (1995). Motor imagery of a lateralized sequential task is asymmetrically slowed in hemi-Parkinson’s patients. Neuropsychologia, 33(6), 727–741.
Driskell, J. E., Copper, C., & Moran, A. (1994). Does mental practice enhance performance? Journal of Applied Psychology, 79, 481–492.
Dunsky, A., Dickstein, R., Ariav, C., Deutsch, J., & Marcovitz, E. (2006). Motor imagery practice in gait rehabilitation of chronic post-stroke hemiparesis: four case studies. International Journal of Rehabilitation Research, 29(4), 351–356. doi:10.1097/MRR.0b013e328010f559.
Dunsky, A., Dickstein, R., Marcovitz, E., Levy, S., & Deutsch, J. E. (2008). Home-based motor imagery training for gait rehabilitation of people with chronic poststroke hemiparesis. Archives of Physical Medicine and Rehabilitation, 89(8), 1580–1588. doi:10.1016/j.apmr.2007.12.039.
Ersland, L., Rosen, G., Lundervold, A., Smievoll, A. I., Tillung, T., Sundberg, H., et al. (1996). Phantom limb imaginary fingertapping causes primary motor cortex activation: an fMRI study. Neuroreport, 8(1), 207–210.
Facchini, S., Muellbacher, W., Battaglia, F., Boroojerdi, B., & Hallett, M. (2002). Focal enhancement of motor cortex excitability during motor imagery: a transcranial magnetic stimulation study. Acta Neurologica Scandinavica, 105(3), 146–151.
Fadiga, L., Buccino, G., Craighero, L., Fogassi, L., Gallese, V., & Pavesi, G. (1998). Corticospinal excitability is specifically modulated by motor imagery: a magnetic stimulation study. Neuropsychologia, 37(2), 147–158. doi:10.1016/S0028-3932(98)00089-X.
Fadiga, L., Buccino, G., Craighero, L., Fogassi, L., Gallese, V., & Pavesi, G. (1999). Corticospinal excitability is specifically modulated by motor imagery: a magnetic stimulation study. Neuropsychologia, 37(2), 147–158.
Faralli, A., Bigoni, M., Mauro, A., Rossi, F., & Carulli, D. (2013). Noninvasive strategies to promote functional recovery after stroke. Neural Plasticity, 2013, 854597. doi:10.1155/2013/854597.
Feltz, D. L., & Landers, D. M. (1983). The effects of mental practice on motor skill learning and performance: a meta-analysis. Journal of Sport & Exercise Psychology, 5, 25–57.
Filippi, M. M., Oliveri, M., Pasqualetti, P., Cicinelli, P., Traversa, R., Vernieri, F., et al. (2001). Effects of motor imagery on motor cortical output topography in Parkinson’s disease. Neurology, 57(1), 55–61.
Fiori, F., Sedda, A., Ferre, E. R., Toraldo, A., Querzola, M., Pasotti, F., et al. (2013). Motor imagery in spinal cord injury patients: moving makes the difference. Journal of Neuropsychology. doi:10.1111/jnp.12020.
Flor, H., Elbert, T., Knecht, S., Wienbruch, C., Pantev, C., Birbaumer, N., et al. (1995). Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature, 375(6531), 482–484. doi:10.1038/375482a0.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12(3), 189–198.
Fournier, J. F. (2000). Imagix: multimedia software for evaluating the vividness of movement-imagery. Perceptual and Motor Skills, 90(2), 367–370.
Frak, V., Cohen, H., & Pourcher, E. (2004). A dissociation between real and simulated movements in Parkinson’s disease. Neuroreport, 15(9), 1489–1492.
Gaggioli, A., Morganti, F., Meneghini, A., Pozzato, I., Greggio, G., Pigatto, M., et al. (2009). Computer-guided mental practice in neurorehabilitation. Studies in Health Technology and Informatics, 145, 195–208.
Gandevia, S. C., Wilson, L. R., Inglis, J. T., & Burke, D. (1997). Mental rehearsal of motor tasks recruits alpha-motoneurones but fails to recruit human fusimotor neurones selectively. Journal of Physiology, 505(Pt 1), 259–266.
Gonzalez, B., Rodriguez, M., Ramirez, C., & Sabate, M. (2005). Disturbance of motor imagery after cerebellar stroke. Behavioral Neuroscience, 119(2), 622–626. doi:10.1037/0735-7044.119.2.622.
Grangeon, M., Charvier, K., Guillot, A., Rode, G., & Collet, C. (2012a). Using sympathetic skin responses in individuals with spinal cord injury as a quantitative evaluation of motor imagery abilities. Physical Therapy, 92(6), 831–840. doi:10.2522/ptj.20110351.
Grangeon, M., Revol, P., Guillot, A., Rode, G., & Collet, C. (2012b). Could motor imagery be effective in upper limb rehabilitation of individuals with spinal cord injury? A case study. Spinal Cord, 50(10), 766–771. doi:10.1038/sc.2012.41.
Gregg, M., Hall, C., & Butler, A. (2010). The MIQ-RS: a suitable option for examining movement imagery ability. Evidence-Based Complementary and Alternative Medicine, 7(2), 249–257.
Grush, R. (2004). The emulation theory of representation: motor control, imagery, and perception. Behavioral and Brain Sciences, 27(3), 377–396. discussion 396–442.
Guillot, A., & Collet, C. (2005). Contribution from neurophysiological and psychological methods to the study of motor imagery. Brain Research. Brain Research Reviews, 50(2), 387–397. doi:10.1016/j.brainresrev.2005.09.004.
Guillot, A., & Collet, C. (2008). Construction of the Motor Imagery Integrative Model in Sport: a review and theoretical investigation of motor imagery use. Int Rev Sport Exerc Psychol, 1(1), 31–44.
Guillot, A., Lebon, F., Rouffet, D., Champely, S., Doyon, J., & Collet, C. (2007). Muscular responses during motor imagery as a function of muscle contraction types. International Journal of Psychophysiology, 66(1), 18–27. doi:10.1016/j.ijpsycho.2007.05.009.
Guillot, A., Collet, C., Nguyen, V. A., Malouin, F., Richards, C., & Doyon, J. (2008). Functional neuroanatomical networks associated with expertise in motor imagery. NeuroImage, 41(4), 1471–1483. doi:10.1016/j.neuroimage.2008.03.042.
Guillot, A., Collet, C., Nguyen, V. A., Malouin, F., Richards, C., & Doyon, J. (2009). Brain activity during visual versus kinesthetic imagery: an fMRI study. Human Brain Mapping, 30(7), 2157–2172. doi:10.1002/hbm.20658.
Guillot, A., Lebon, F., & Collet, C. (2010). Electromyographic activity during motor imagery. In A. Guillot & C. Collet (Eds.), The neurophysiological foundations of mental and motor imagery (pp. 83–93). New York, NY: Oxford University Press.
Guillot, A., Di Rienzo, F., Macintyre, T., Moran, A., & Collet, C. (2012a). Imagining is Not doing but involves specific motor commands: a review of experimental data related to motor inhibition. Frontiers in Human Neuroscience, 6, 247. doi:10.3389/fnhum.2012.00247.
Guillot, A., Hoyek, N., Louis, M., & Collet, C. (2012b). Understanding the timing of motor imagery: recent findings and future directions. International Review of Sport and Exercise Psychology, 5(1), 3–22. doi:10.1080/1750984x.2011.623787.
Guillot, A., Di Rienzo, F., & Collet, C. (2014). The neurofunctional architecture of motor imagery. In T. D. Papageorgiou, G. Christopoulos, & S. Smirnakis (Eds.), Functional magnetic resonance imaging / Book 1: In Tech.
Gustin, S. M., Wrigley, P. J., Gandevia, S. C., Middleton, J. W., Henderson, L. A., & Siddall, P. J. (2008). Movement imagery increases pain in people with neuropathic pain following complete thoracic spinal cord injury. Pain, 137(2), 237–244. doi:10.1016/j.pain.2007.08.032.
Gustin, S. M., Wrigley, P. J., Henderson, L. A., & Siddall, P. J. (2010). Brain circuitry underlying pain in response to imagined movement in people with spinal cord injury. Pain, 148(3), 438–445. doi:10.1016/j.pain.2009.12.001.
Hale, B. S., Raglin, J. S., & Koceja, D. M. (2003). Effect of mental imagery of a motor task on the Hoffmann reflex. Behavioural Brain Research, 142(1–2), 81–87.
Hall, C. R., & Martin, K. A. (1997). Measuring movement imagery abilities: a revision of the movement imagery questionnaire. Journal of mental imagery, 21(1–2), 143–154.
Hall, E. G., & Pongrac, J. (1983). Movement imagery questionnaire. London, Ontario, Canada: University of Western Ontario.
Harris, A. J. (1999). Cortical origin of pathological pain. Lancet, 354(9188), 1464–1466. doi:10.1016/S0140-6736(99)05003-5.
Helmich, R. C., de Lange, F. P., Bloem, B. R., & Toni, I. (2007). Cerebral compensation during motor imagery in Parkinson’s disease. Neuropsychologia, 45(10), 2201–2215. doi:10.1016/j.neuropsychologia.2007.02.024.
Helmich, R. C., Bloem, B. R., & Toni, I. (2011). Motor imagery evokes increased somatosensory activity in parkinson’s disease patients with tremor. Human Brain Mapping. doi:10.1002/hbm.21318.
Hemmen, B., & Seelen, H. A. (2007). Effects of movement imagery and electromyography-triggered feedback on arm hand function in stroke patients in the subacute phase. Clinical Rehabilitation, 21(7), 587–594. doi:10.1177/0269215507075502.
Heremans, E., Helsen, W. F., & Feys, P. (2008). The eyes as a mirror of our thoughts: quantification of motor imagery of goal-directed movements through eye movement registration. Behavioural Brain Research, 187(2), 351–360. doi:10.1016/j.bbr.2007.09.028.
Heremans, E., Feys, P., Nieuwboer, A., Vercruysse, S., Vandenberghe, W., Sharma, N., et al. (2011). Motor imagery ability in patients with early- and mid-stage Parkinson disease. Neurorehabilitation and Neural Repair, 25(2), 168–177. doi:10.1177/1545968310370750.
Heremans, E., Nieuwboer, A., Feys, P., Vercruysse, S., Vandenberghe, W., Sharma, N., et al. (2012). External cueing improves motor imagery quality in patients with Parkinson disease. Neurorehabilitation and Neural Repair, 26(1), 27–35. doi:10.1177/1545968311411055.
Hetu, S., Gregoire, M., Saimpont, A., Coll, M. P., Eugene, F., Michon, P. E., et al. (2013). The neural network of motor imagery: an ALE meta-analysis. Neuroscience and Biobehavioral Reviews, 37(5), 930–949. doi:10.1016/j.neubiorev.2013.03.017.
Holmes, P. S., & Collins, D. J. (2001). The PETTLEP approach to motor imagery: a functional equivalence model for sport psychologists. J Appl Sport Psych, 13(1), 60–83. doi:10.1080/10413200109339004.
Hotz-Boendermaker, S., Funk, M., Summers, P., Brugger, P., Hepp-Reymond, M. C., Curt, A., et al. (2008). Preservation of motor programs in paraplegics as demonstrated by attempted and imagined foot movements. NeuroImage, 39(1), 383–394. doi:10.1016/j.neuroimage.2007.07.065.
Hovington, C. L., & Brouwer, B. (2010). Guided motor imagery in healthy adults and stroke: does strategy matter? Neurorehabilitation and Neural Repair, 24(9), 851–857. doi:10.1177/1545968310374190.
Hoyek, N., Di Rienzo, F., Collet, C., Creveaux, T., & Guillot, A. (2013). Hand mental rotation is not systematically altered by actual body position: Laterality judgment versus same–different comparison tasks. Attention, Perception, & Psychophysics doi:10.3758/s13414-013-0577-z.
Hugdahl, K., Rosen, G., Ersland, L., Lundervold, A., Smievoll, A. I., Barndon, R., et al. (2001). Common pathways in mental imagery and pain perception: an fMRI study of a subject with an amputated arm. Scandinavian Journal of Psychology, 42(3), 269–275.
Hwang, S., Jeon, H. S., Yi, C. H., Kwon, O. Y., Cho, S. H., & You, S. H. (2010). Locomotor imagery training improves gait performance in people with chronic hemiparetic stroke: a controlled clinical trial. Clinical Rehabilitation, 24(6), 514–522. doi:10.1177/0269215509360640.
Ionta, S., Perruchoud, D., Draganski, B., & Blanke, O. (2012). Body context and posture affect mental imagery of hands. PLoS One, 7(3), e34382. doi:10.1371/journal.pone.0034382.
Isaac, A. R., Marks, D. F., & Russell, D. H. (1986). An instrument for assessing imagery of movement. The vividness of movement imagery questionnaire. J Ment Imagery, 10, 23–30.
Jackson, P. L., Lafleur, M. F., Malouin, F., Richards, C., & Doyon, J. (2001). Potential role of mental practice using motor imagery in neurologic rehabilitation. Archives of Physical Medicine and Rehabilitation, 82(8), 1133–1141. doi:10.1053/apmr.2001.24286.
Jackson, P. L., Lafleur, M. F., Malouin, F., Richards, C. L., & Doyon, J. (2003). Functional cerebral reorganization following motor sequence learning through mental practice with motor imagery. NeuroImage, 20(2), 1171–1180. doi:10.1016/s1053-8119(03)00369-0.
Jackson, P. L., Doyon, J., Richards, C. L., & Malouin, F. (2004). The efficacy of combined physical and mental practice in the learning of a foot-sequence task after stroke: a case report. Neurorehabilitation and Neural Repair, 18(2), 106–111. doi:10.1177/0888439004265249.
Jacobson, E. (1930). Electrical measurements of neuromuscular states during mental activities. American Journal of Physiology, 91, 567–608.
Jacobson, E. (1932). Electrophysiology of mental activities. American Journal of Psychology, 44, 677–694.
Jeannerod, M. (1994). The representing brain: neural correlates of motor intention and imagery. Behavioral and Brain Sciences, 17(02), 187–202. doi:10.1017/S0140525X00034026.
Jeannerod, M. (1995). Mental imagery in the motor context. Neuropsychologia, 33(11), 1419–1432.
Jeannerod, M. (2001). Neural simulation of action: a unifying mechanism for motor cognition. NeuroImage, 14(1 Pt 2), S103–109. doi:10.1006/nimg.2001.0832.
Johnson, S. H. (2000). Imagining the impossible: intact motor representations in hemiplegics. Neuroreport, 11(4), 729–732.
Johnson, S. H., Sprehn, G., & Saykin, A. J. (2002). Intact motor imagery in chronic upper limb hemiplegics: evidence for activity-independent action representations. Journal of Cognitive Neuroscience, 14(6), 841–852. doi:10.1162/089892902760191072.
Karl, A., Birbaumer, N., Lutzenberger, W., Cohen, L. G., & Flor, H. (2001). Reorganization of motor and somatosensory cortex in upper extremity amputees with phantom limb pain. Journal of Neuroscience, 21(10), 3609–3618.
Kasai, T., Kawai, S., Kawanishi, M., & Yahagi, S. (1997). Evidence for facilitation of motor evoked potentials (MEPs) induced by motor imagery. Brain Research, 744(1), 147–150.
Kim, J. S., Oh, D. W., Kim, S. Y., & Choi, J. D. (2011). Visual and kinesthetic locomotor imagery training integrated with auditory step rhythm for walking performance of patients with chronic stroke. Clinical Rehabilitation, 25(2), 134–145. doi:10.1177/0269215510380822.
Kimberley, T. J., Khandekar, G., Skraba, L. L., Spencer, J. A., Van Gorp, E. A., & Walker, S. R. (2006). Neural substrates for motor imagery in severe hemiparesis. Neurorehabilitation and Neural Repair, 20(2), 268–277. doi:10.1177/1545968306286958.
Knecht, S., Henningsen, H., Elbert, T., Flor, H., Hohling, C., Pantev, C., et al. (1996). Reorganizational and perceptional changes after amputation. Brain, 119(Pt 4), 1213–1219.
Kokotilo, K. J., Eng, J. J., & Curt, A. (2009). Reorganization and preservation of motor control of the brain in spinal cord injury: a systematic review. Journal of Neurotrauma, 26(11), 2113–2126. doi:10.1089/neu.2008.0688.
Kuhn, A. A., Doyle, L., Pogosyan, A., Yarrow, K., Kupsch, A., Schneider, G. H., et al. (2006). Modulation of beta oscillations in the subthalamic area during motor imagery in Parkinson’s disease. Brain, 129(Pt 3), 695–706. doi:10.1093/brain/awh715.
Lacourse, M. G., Cohen, M. J., Lawrence, K. E., & Romero, D. H. (1999). Cortical potentials during imagined movements in individuals with chronic spinal cord injuries. Behavioural Brain Research, 104(1–2), 73–88. doi:10.1016/S0166-4328(99)00052-2.
Lacourse, M. G., Turner, J. A., Randolph-Orr, E., Schandler, S. L., & Cohen, M. J. (2004). Cerebral and cerebellar sensorimotor plasticity following motor imagery-based mental practice of a sequential movement. Journal of Rehabilitation Research and Development, 41(4), 505–524.
Lebon, F., Byblow, W. D., Collet, C., Guillot, A., & Stinear, C. M. (2012). The modulation of motor cortex excitability during motor imagery depends on imagery quality. European Journal of Neuroscience, 35(2), 323–331. doi:10.1111/j.1460-9568.2011.07938.x.
Leonard, G., & Tremblay, F. (2007). Corticomotor facilitation associated with observation, imagery and imitation of hand actions: a comparative study in young and old adults. Experimental Brain Research, 177(2), 167–175. doi:10.1007/s00221-006-0657-6.
Lequerica, A., Rapport, L., Axelrod, B. N., Telmet, K., & Whitman, R. D. (2002). Subjective and objective assessment methods of mental imagery control: construct validation of self-report measures. Journal of Clinical and Experimental Neuropsychology, 24(8), 1103–1116. doi:10.1076/jcen.24.8.1103.8370.
Levin, O., Steyvers, M., Wenderoth, N., Li, Y., & Swinnen, S. P. (2004). Dynamical changes in corticospinal excitability during imagery of unimanual and bimanual wrist movements in humans: a transcranial magnetic stimulation study. Neuroscience Letters, 359(3), 185–189. doi:10.1016/j.neulet.2004.01.070.
Li, C. R. (2000). Impairment of motor imagery in putamen lesions in humans. Neuroscience Letters, 287(1), 13–16.
Liepert, J., Greiner, J., Nedelko, V., & Dettmers, C. (2012). Reduced upper limb sensation impairs mental chronometry for motor imagery after stroke : clinical and electrophysiological findings. Neurorehab Neural Rep. doi:10.1177/1545968311425924.
Lorey, B., Bischoff, M., Pilgramm, S., Stark, R., Munzert, J., & Zentgraf, K. (2009). The embodied nature of motor imagery: the influence of posture and perspective. Experimental Brain Research, 194(2), 233–243. doi:10.1007/s00221-008-1693-1.
Lorey, B., Pilgramm, S., Bischoff, M., Stark, R., Vaitl, D., Kindermann, S., et al. (2011). Activation of the parieto-premotor network is associated with vivid motor imagery–a parametric FMRI study. PLoS One, 6(5), e20368. doi:10.1371/journal.pone.0020368.
Lotze, M., & Halsband, U. (2006). Motor imagery. Journal of Physiology, Paris, 99(4–6), 386–395. doi:10.1016/j.jphysparis.2006.03.012.
Lotze, M., Montoya, P., Erb, M., Hulsmann, E., Flor, H., Klose, U., et al. (1999). Activation of cortical and cerebellar motor areas during executed and imagined hand movements: an fMRI study. J Cognit Neurosci, 11(5), 491–501. doi:10.1162/089892999563553.
Lotze, M., Flor, H., Grodd, W., Larbig, W., & Birbaumer, N. (2001). Phantom movements and pain. An fMRI study in upper limb amputees. Brain, 124(Pt 11), 2268–2277.
Louis, M., Guillot, A., Maton, S., Doyon, J., & Collet, C. (2008). Effect of imagined movement speed on subsequent motor performance. Journal of Motor Behavior, 40(2), 117–132. doi:10.3200/JMBR.40.2.117-132.
MacIver, K., Lloyd, D. M., Kelly, S., Roberts, N., & Nurmikko, T. (2008). Phantom limb pain, cortical reorganization and the therapeutic effect of mental imagery. Brain, 131(Pt 8), 2181–2191. doi:10.1093/brain/awn124.
Macuga, K. L., & Frey, S. H. (2012). Neural representations involved in observed, imagined, and imitated actions are dissociable and hierarchically organized. NeuroImage, 59(3), 2798–2807. doi:10.1016/j.neuroimage.2011.09.083.
Maillet, A., Pollak, P., & Debu, B. (2012). Imaging gait disorders in parkinsonism: a review. Journal of Neurology, Neurosurgery and Psychiatry, 83(10), 986–993. doi:10.1136/jnnp-2012-302461.
Malouin, F., & Richards, C. L. (2010). Mental practice for relearning locomotor skills. Physical Therapy, 90(2), 240–251. doi:10.2522/ptj.20090029.
Malouin, F., Belleville, S., Richards, C. L., Desrosiers, J., & Doyon, J. (2004a). Working memory and mental practice outcomes after stroke. Archives of Physical Medicine and Rehabilitation, 85(2), 177–183.
Malouin, F., Richards, C. L., Desrosiers, J., & Doyon, J. (2004b). Bilateral slowing of mentally simulated actions after stroke. Neuroreport, 15(8), 1349–1353.
Malouin, F., Richards, C. L., Doyon, J., Desrosiers, J., & Belleville, S. (2004c). Training mobility tasks after stroke with combined mental and physical practice: a feasibility study. Neurorehabilitation and Neural Repair, 18(2), 66–75. doi:10.1177/0888439004266304.
Malouin, F., Richards, C. L., Jackson, P. L., Lafleur, M. F., Durand, A., & Doyon, J. (2007). The Kinesthetic and Visual Imagery Questionnaire (KVIQ) for assessing motor imagery in persons with physical disabilities: a reliability and construct validity study. Journal of Neurologic Physical Therapy, 31(1), 20–29. doi:10.1097/01.NPT.0000260567.24122.64.
Malouin, F., Richards, C. L., Durand, A., & Doyon, J. (2008a). Clinical assessment of motor imagery after stroke. Neurorehabil Neural Rep, 22(4), 330–340. doi:10.1177/1545968307313499.
Malouin, F., Richards, C. L., Durand, A., & Doyon, J. (2008b). Reliability of mental chronometry for assessing motor imagery ability after stroke. Archives of Physical Medicine and Rehabilitation, 89(2), 311–319. doi:10.1016/j.apmr.2007.11.006.
Malouin, F., Richards, C. L., Durand, A., Descent, M., Poire, D., Fremont, P., et al. (2009a). Effects of practice, visual loss, limb amputation, and disuse on motor imagery vividness. Neurorehabilitation and Neural Repair, 23(5), 449–463. doi:10.1177/1545968308328733.
Malouin, F., Richards, C. L., Durand, A., & Doyon, J. (2009b). Added value of mental practice combined with a small amount of physical practice on the relearning of rising and sitting post-stroke: a pilot study. Journal of Neurologic Physical Therapy, 33(4), 195–202. doi:10.1097/NPT.0b013e3181c2112b.
Malouin, F., Richards, C. L., Jackson, P. L., Dumas, F., & Doyon, J. (2010). Motor imagery for optimizing the reacquisition of locomotor skills after cerebral damage. The neurophysiological foundations of mental and motor imagery. A. Guillot and C. Collet. New York, NY, Oxford University Press: 161--176.
Malouin, F., Richards, C. L., & Durand, A. (2012). Slowing of motor imagery after a right hemispheric stroke. Stroke Res Treat, 2012, 297217. doi:10.1155/2012/297217.
Malouin, F., Jackson, P. L., & Richards, C. L. (2013). Towards the integration of mental practice in rehabilitation programs. A critical review. Front Hum Neurosci, 7, doi:10.3389/fnhum.2013.00576.
Marconi, B., Koch, G., Pecchioli, C., Cavallari, P., & Caltagirone, C. (2007). Breakdown of inhibitory effects induced by foot motor imagery on hand motor area in lower-limb amputees. Clinical Neurophysiology, 118(11), 2468–2478. doi:10.1016/j.clinph.2007.08.021.
Marks, D. F. (1973). Visual imagery differences in the recall of pictures. British journal of Psychology, 64(1), 17–24.
Marks, D. F., & Isaac, A. R. (1995). Topographical distribution of EEG activity accompanying visual and motor imagery in vivid and non-vivid imagers. British Journal of Psychology, 86(Pt 2), 271–282.
Matsunaga, K., Uozumi, T., Tsuji, S., & Murai, Y. (1998). Sympathetic skin responses recorded from non-palmar and non-plantar skin sites: their role in the evaluation of thermal sweating. Electroencephalography and Clinical Neurophysiology, 108(5), 482–489.
McAvinue, L. P., & Robertson, I. H. (2011). Individual differences in response to phantom limb movement therapy. Disability and Rehabilitation, 33(23–24), 2186–2195. doi:10.3109/09638288.2011.563816.
Moseley, G. L. (2007). Using visual illusion to reduce at-level neuropathic pain in paraplegia. Pain, 130(3), 294–298. doi:10.1016/j.pain.2007.01.007.
Mulder, T. (2007). Motor imagery and action observation: cognitive tools for rehabilitation. Journal of Neural Transmission, 114(10), 1265–1278. doi:10.1007/s00702-007-0763-z.
Muller, K., Butefisch, C. M., Seitz, R. J., & Homberg, V. (2007). Mental practice improves hand function after hemiparetic stroke. Restorative Neurology and Neuroscience, 25(5–6), 501–511.
Munzert, J., & Zentgraf, K. (2009). Motor imagery and its implications for understanding the motor system. Progress in Brain Research, 174, 219–229. doi:10.1016/S0079-6123(09)01318-1.
Munzert, J., Lorey, B., & Zentgraf, K. (2009). Cognitive motor processes: the role of motor imagery in the study of motor representations. Brain Research Reviews, 60(2), 306–326. doi:10.1016/j.brainresrev.2008.12.024.
Nair, D. G., Fuchs, A., Burkart, S., Steinberg, F. L., & Kelso, J. A. (2005). Assessing recovery in middle cerebral artery stroke using functional MRI. Brain Injury, 19(13), 1165–1176. doi:10.1080/02699050500149858.
Ni Choisdealbha, A., Brady, N., & Maguinness, C. (2011). Differing roles for the dominant and non-dominant hands in the hand laterality task. Experimental Brain Research, 211(1), 73–85. doi:10.1007/s00221-011-2652-9.
Nico, D., Daprati, E., Rigal, F., Parsons, L., & Sirigu, A. (2004). Left and right hand recognition in upper limb amputees. Brain, 127(Pt 1), 120–132. doi:10.1093/brain/awh006.
Nikulin, V. V., Hohlefeld, F. U., Jacobs, A. M., & Curio, G. (2008). Quasi-movements: a novel motor-cognitive phenomenon. Neuropsychologia, 46(2), 727–742. doi:10.1016/j.neuropsychologia.2007.10.008.
Nyberg, L., Eriksson, J., Larsson, A., & Marklund, P. (2006). Learning by doing versus learning by thinking: an fMRI study of motor and mental training. Neuropsychologia, 44(5), 711–717. doi:10.1016/j.neuropsychologia.2005.08.006.
Olsson, C. J. (2012). Complex motor representations may not be preserved after complete spinal cord injury. Experimental Neurology, 236(1), 46–49. doi:10.1016/j.expneurol.2012.03.022.
Olsson, C. J., & Nyberg, L. (2010). Motor imagery: if you can’t do it, you won’t think it. Scandinavian Journal of Medicine and Science in Sports, 20(5), 711–715. doi:10.1111/j.1600-0838.2010.01101.x.
Page, S. J., Szaflarski, J. P., Eliassen, J. C., Pan, H., & Cramer, S. C. (2009). Cortical plasticity following motor skill learning during mental practice in stroke. Neurorehabilitation and Neural Repair, 23(4), 382–388. doi:10.1177/1545968308326427.
Page, S. J., Dunning, K., Hermann, V., Leonard, A., & Levine, P. (2011a). Longer versus shorter mental practice sessions for affected upper extremity movement after stroke: a randomized controlled trial. Clinical Rehabilitation, 25(7), 627–637. doi:10.1177/0269215510395793.
Page, S. J., Murray, C., Hermann, V., & Levine, P. (2011b). Retention of motor changes in chronic stroke survivors who were administered mental practice. Archives of Physical Medicine and Rehabilitation, 92(11), 1741–1745. doi:10.1016/j.apmr.2011.06.009.
Papaxanthis, C., Pozzo, T., Skoura, X., & Schieppati, M. (2002). Does order and timing in performance of imagined and actual movements affect the motor imagery process? The duration of walking and writing task. Behavioural Brain Research, 134(1–2), 209–215.
Parsons, L. M. (1987a). Imagined spatial transformation of one’s body. Journal of Experimental Psychology: General, 116(2), 172–191.
Parsons, L. M. (1987b). Imagined spatial transformations of one’s hands and feet. Cognitive Psychology, 19(2), 178–241.
Parsons, L. M. (1994). Temporal and kinematic properties of motor behavior reflected in mentally simulated action. Journal of Experimental Psychology: Human Perception and Performance, 20(4), 709–730.
Pascual-Leone, A., Nguyet, D., Cohen, L. G., Brasil-Neto, J. P., Cammarota, A., & Hallett, M. (1995). Modulation of muscle responses evoked by transcranial magnetic stimulation during the acquisition of new fine motor skills. Journal of Neurophysiology, 74(3), 1037–1045.
Pascual-Leone, A., Peris, M., Tormos, J. M., Pascual, A. P., & Catala, M. D. (1996). Reorganization of human cortical motor output maps following traumatic forearm amputation. Neuroreport, 7(13), 2068–2070.
Peterson, D. S., Pickett, K. A., & Earhart, G. M. (2012). Effects of levodopa on vividness of motor imagery in Parkinson disease. J Parkinsons Dis, 2(2), 127–133. doi:10.3233/jpd-2012-12077.
Pickett, K. A., Peterson, D. S., & Earhart, G. M. (2012). Motor imagery of gait tasks in individuals with Parkinson disease. J Parkinsons Dis, 2(1), 19–22. doi:10.3233/jpd-2012-11045.
Poliakoff, E. (2013). Representation of action in Parkinson’s disease: imagining, observing, and naming actions. Journal of Neuropsychology. doi:10.1111/jnp.12005.
Porro, C. A., Francescato, M. P., Cettolo, V., Diamond, M. E., Baraldi, P., Zuiani, C., et al. (1996). Primary motor and sensory cortex activation during motor performance and motor imagery: a functional magnetic resonance imaging study. Journal of Neuroscience, 16(23), 7688–7698.
Posner, M. I. (1978). Chronometric explorations of mind. Hillsdale, NJ: Erlbaum.
Raffin, E., Giraux, P., & Reilly, K. T. (2012a). The moving phantom: motor execution or motor imagery? Cortex, 48(6), 746–757. doi:10.1016/j.cortex.2011.02.003.
Raffin, E., Mattout, J., Reilly, K. T., & Giraux, P. (2012b). Disentangling motor execution from motor imagery with the phantom limb. Brain, 135(Pt 2), 582–595. doi:10.1093/brain/awr337.
Ramachandran, V. S., Brang, D., & McGeoch, P. D. (2010). Dynamic reorganization of referred sensations by movements of phantom limbs. Neuroreport, 21(10), 727–730. doi:10.1097/WNR.0b013e32833be9ab.
Randhawa, B., Harris, S., & Boyd, L. A. (2010). The Kinesthetic and Visual Imagery Questionnaire is a reliable tool for individuals with Parkinson disease. Journal of Neurologic Physical Therapy, 34(3), 161–167.
Ranganathan, V. K., Siemionow, V., Liu, J. Z., Sahgal, V., & Yue, G. H. (2004). From mental power to muscle power–gaining strength by using the mind. Neuropsychologia, 42(7), 944–956. doi:10.1016/j.neuropsychologia.2003.11.018.
Reis, J., Swayne, O. B., Vandermeeren, Y., Camus, M., Dimyan, M. A., Harris-Love, M., et al. (2008). Contribution of transcranial magnetic stimulation to the understanding of cortical mechanisms involved in motor control. Journal of Physiology, 586(2), 325–351. doi:10.1113/jphysiol.2007.144824.
Roberts, R., Callow, N., Hardy, L., Markland, D., & Bringer, J. (2008). Movement imagery ability: development and assessment of a revised version of the Vividness of Movement Imagery Questionnaire. Journal of Sport & Exercise Psychology, 20, 200–221.
Rosen, G., Hugdahl, K., Ersland, L., Lundervold, A., Smievoll, A. I., Barndon, R., et al. (2001). Different brain areas activated during imagery of painful and non-painful ‘finger movements’ in a subject with an amputated arm. Neurocase, 7(3), 255–260. doi:10.1093/neucas/7.3.255.
Rossini, P. M., & Pauri, F. (2000). Neuromagnetic integrated methods tracking human brain mechanisms of sensorimotor areas ‘plastic’ reorganisation. Brain Research. Brain Research Reviews, 33(2–3), 131–154.
Rossini, P. M., Rossi, S., Pasqualetti, P., & Tecchio, F. (1999). Corticospinal excitability modulation to hand muscles during movement imagery. Cerebral Cortex, 9(2), 161–167.
Rothwell, J. C. (1991). Physiological studies of electric and magnetic stimulation of the human brain. Electroencephalography and Clinical Neurophysiology. Supplement, 43, 29–35.
Rushby, J. A., Fisher, A. C., McDonald, S., Murphy, A., & Finnigan, S. (2013). Autonomic and neural correlates of dysregulated arousal in severe traumatic brain injury. International Journal of Psychophysiology, 89(3), 460–465. doi:10.1016/j.ijpsycho.2013.05.009.
Sabate, M., Gonzalez, B., & Rodriguez, M. (2004). Brain lateralization of motor imagery: motor planning asymmetry as a cause of movement lateralization. Neuropsychologia, 42(8), 1041–1049. doi:10.1016/j.neuropsychologia.2003.12.015.
Sabate, M., Gonzalez, B., & Rodriguez, M. (2007). Adapting movement planning to motor impairments: the motor-scanning system. Neuropsychologia, 45(2), 378–386. doi:10.1016/j.neuropsychologia.2006.06.025.
Sabbah, P., Leveque, C., Pfefer, F., Nioche, C., Gay, S., Sarrazin, J. L., et al. (2000). Functional MR imaging and traumatic paraplegia: preliminary report. Journal of Neuroradiology, 27(4), 233–237.
Sabbah, P., de, S. S., Leveque, C., Gay, S., Pfefer, F., Nioche, C., et al. (2002). Sensorimotor cortical activity in patients with complete spinal cord injury: a functional magnetic resonance imaging study. Journal of Neurotrauma, 19(1), 53–60. doi:10.1089/089771502753460231.
Samuel, M., Ceballos-Baumann, A. O., Boecker, H., & Brooks, D. J. (2001). Motor imagery in normal subjects and Parkinson’s disease patients: an H215O PET study. Neuroreport, 12(4), 821–828.
Sauvage, C., Jissendi, P., Seignan, S., Manto, M., & Habas, C. (2013). Brain areas involved in the control of speed during a motor sequence of the foot: Real movement versus mental imagery. Journal of Neuroradiology. doi:10.1016/j.neurad.2012.10.001.
Schuster, C., Hilfiker, R., Amft, O., Scheidhauer, A., Andrews, B., Butler, J., et al. (2011). Best practice for motor imagery: a systematic literature review on motor imagery training elements in five different disciplines. BMC Medicine, 9, 75. doi:10.1186/1741-7015-9-75.
Schuster, C., Butler, J., Andrews, B., Kischka, U., & Ettlin, T. (2012a). Comparison of embedded and added motor imagery training in patients after stroke: results of a randomised controlled pilot trial. Trials, 13, 11. doi:10.1186/1745-6215-13-11.
Schuster, C., Glassel, A., Scheidhauer, A., Ettlin, T., & Butler, J. (2012b). Motor imagery experiences and use: asking patients after stroke where, when, what, why, and how they use imagery: a qualitative investigation. Stroke Res Treat, 2012, 503190. doi:10.1155/2012/503190.
Schuster, C., Lussi, A., Wirth, B., & Ettlin, T. (2012c). Two assessments to evaluate imagery ability: translation, test-retest reliability and concurrent validity of the German KVIQ and Imaprax. BMC Medical Research Methodology, 12(1), 127. doi:10.1186/1471-2288-12-127.
Schwoebel, J., Boronat, C. B., & Branch Coslett, H. (2002). The man who executed “imagined” movements: evidence for dissociable components of the body schema. Brain and Cognition, 50(1), 1–16. doi:10.1016/s0278-2626(02)00005-2.
Sharma, N., Pomeroy, V. M., & Baron, J. C. (2006). Motor imagery: a backdoor to the motor system after stroke? Stroke, 37(7), 1941–1952. doi:10.1161/01.STR.0000226902.43357.fc.
Sharma, N., Jones, P. S., Carpenter, T. A., & Baron, J. C. (2008). Mapping the involvement of BA 4a and 4p during Motor Imagery. NeuroImage, 41(1), 92–99. doi:10.1016/j.neuroimage.2008.02.009.
Sharma, N., Baron, J. C., & Rowe, J. B. (2009a). Motor imagery after stroke: relating outcome to motor network connectivity. Annals of Neurology, 66(5), 604–616. doi:10.1002/ana.21810.
Sharma, N., Simmons, L. H., Jones, P. S., Day, D. J., Carpenter, T. A., Pomeroy, V. M., et al. (2009b). Motor imagery after subcortical stroke: a functional magnetic resonance imaging study. Stroke, 40(4), 1315–1324. doi:10.1161/strokeaha.108.525766.
Shaw, W. A. (1938). The distribution of muscular action potentials during imaging. Psychological Record, 2, 195–216.
Sheehan, P. W. (1967). A shortened form of Bett’s questionnaire upon mental imagery. Journal of Clinical Psychology, 23, 386–389.
Shepard, R. N., & Cooper, L. A. (1986). Mental images and their transformations. Cambridge, MA: The MIT Press.
Shields, S. A., MacDowell, K. A., Fairchild, S. B., & Campbell, M. L. (1987). Is mediation of sweating cholinergic, adrenergic, or both? A comment on the literature. Psychophysiology, 24(3), 312–319.
Simmons, L., Sharma, N., Baron, J. C., & Pomeroy, V. M. (2008). Motor imagery to enhance recovery after subcortical stroke: who might benefit, daily dose, and potential effects. Neurorehabilitation and Neural Repair, 22(5), 458–467. doi:10.1177/1545968308315597.
Sirigu, A., & Duhamel, J. (2001). Motor and visual imagery as two complementary but neurally dissociable mental processes. J Cognit Neurosci, 13(7), 910–919.
Sirigu, A., Cohen, L., Duhamel, J. R., Pillon, B., Dubois, B., Agid, Y., et al. (1995). Congruent unilateral impairments for real and imagined hand movements. Neuroreport, 6(7), 997–1001.
Sirigu, A., Duhamel, J. R., Cohen, L., Pillon, B., Dubois, B., & Agid, Y. (1996). The mental representation of hand movements after parietal cortex damage. Science, 273(5281), 1564–1568.
Snijders, A. H., Leunissen, I., Bakker, M., Overeem, S., Helmich, R. C., Bloem, B. R., et al. (2011). Gait-related cerebral alterations in patients with Parkinson’s disease with freezing of gait. Brain, 134(Pt 1), 59–72. doi:10.1093/brain/awq324.
Solodkin, A., Hlustik, P., Chen, E. E., & Small, S. L. (2004). Fine modulation in network activation during motor execution and motor imagery. Cerebral Cortex, 14(11), 1246–1255. doi:10.1093/cercor/bhh086.
Stephan, K. M., & Frackowiak, R. S. (1996). Motor imagery–anatomical representation and electrophysiological characteristics. Neurochemical Research, 21(9), 1105–1116.
Stephan, K. M., Fink, G. R., Passingham, R. E., Silbersweig, D., Ceballos-Baumann, A. O., Frith, C. D., et al. (1995). Functional anatomy of the mental representation of upper extremity movements in healthy subjects. Journal of Neurophysiology, 73(1), 373–386.
Stevens, J. A., & Stoykov, M. E. (2003). Using motor imagery in the rehabilitation of hemiparesis. Archives of Physical Medicine and Rehabilitation, 84(7), 1090–1092.
Stinear, C. M. (2010). Corticospinal facilitation during motor imagery. In A. Guillot & C. Collet (Eds.), The neurophysiological foundations of mental and motor imagery (pp. 47–61). New York, NY: Oxford University Press.
Stinear, C. M., & Byblow, W. D. (2003). Motor imagery of phasic thumb abduction temporally and spatially modulates corticospinal excitability. Clinical Neurophysiology, 114(5), 909–914.
Stinear, C. M., Byblow, W. D., Steyvers, M., Levin, O., & Swinnen, S. P. (2006). Kinesthetic, but not visual, motor imagery modulates corticomotor excitability. Experimental Brain Research, 168(1–2), 157–164. doi:10.1007/s00221-005-0078-y.
Stinear, C. M., Fleming, M. K., Barber, P. A., & Byblow, W. D. (2007). Lateralization of motor imagery following stroke. Clinical Neurophysiology, 118(8), 1794–1801. doi:10.1016/j.clinph.2007.05.008.
Subramanian, L., Hindle, J. V., Johnston, S., Roberts, M. V., Husain, M., Goebel, R., et al. (2011). Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson’s disease. Journal of Neuroscience, 31(45), 16309–16317. doi:10.1523/jneurosci.3498-11.2011.
Sun, L., Yin, D., Zhu, Y., Fan, M., Zang, L., Wu, Y., et al. (2013). Cortical reorganization after motor imagery training in chronic stroke patients with severe motor impairment: a longitudinal fMRI study. Neuroradiology, 55(7), 913–925. doi:10.1007/s00234-013-1188-z.
Szameitat, A. J., Shen, S., Conforto, A., & Sterr, A. (2012). Cortical activation during executed, imagined, observed, and passive wrist movements in healthy volunteers and stroke patients. NeuroImage, 62(1), 266–280. doi:10.1016/j.neuroimage.2012.05.009.
Takemi, M., Masakado, Y., Liu, M., & Ushiba, J. (2013). Event-related desynchronization reflects down-regulation of intracortical inhibition in human primary motor cortex. Journal of Neurophysiology. doi:10.1152/jn.01092.2012.
Tamaki, M., Huang, T. R., Yotsumoto, Y., Hamalainen, M., Lin, F. H., Nanez, J. E., Sr., et al. (2013). Enhanced spontaneous oscillations in the supplementary motor area are associated with sleep-dependent offline learning of finger-tapping motor-sequence task. Journal of Neuroscience, 33(34), 13894–13902. doi:10.1523/jneurosci.1198-13.2013.
Thobois, S., Dominey, P. F., Decety, J., Pollak, P. P., Gregoire, M. C., Le Bars, P. D., et al. (2000). Motor imagery in normal subjects and in asymmetrical Parkinson’s disease: a PET study. Neurology, 55(7), 996–1002.
Thobois, S., Dominey, P., Fraix, V., Mertens, P., Guenot, M., Zimmer, L., et al. (2002). Effects of subthalamic nucleus stimulation on actual and imagined movement in Parkinson’s disease : a PET study. Journal of Neurology, 249(12), 1689–1698. doi:10.1007/s00415-002-0906-y.
Tomasino, B., Ida Rumiati, R., & Arrigo Umiltà, C. (2003). Selective deficit of motor imagery as tapped by a left–right decision of visually presented hands. Brain and Cognition, 53(2), 376–380. doi:10.1016/s0278-2626(03)00147-7.
Tomberg, C., & Caramia, M. D. (1991). Prime mover muscle in finger lift or finger flexion reaction times: identification with transcranial magnetic stimulation. Electroencephalography and Clinical Neurophysiology, 81(4), 319–322.
Tremblay, F., Leonard, G., & Tremblay, L. (2008). Corticomotor facilitation associated with observation and imagery of hand actions is impaired in Parkinson’s disease. Experimental Brain Research, 185(2), 249–257. doi:10.1007/s00221-007-1150-6.
van der Meulen, M., Allali, G., Rieger, S. W., Assal, F., & Vuilleumier, P. (2012). The influence of individual motor imagery ability on cerebral recruitment during gait imagery. Human Brain Mapping. doi:10.1002/hbm.22192.
van Nuenen, B. F., Helmich, R. C., Buenen, N., van de Warrenburg, B. P., Bloem, B. R., & Toni, I. (2012). Compensatory activity in the extrastriate body area of Parkinson’s disease patients. Journal of Neuroscience, 32(28), 9546–9553. doi:10.1523/JNEUROSCI.0335-12.2012.
Vromen, A., Verbunt, J. A., Rasquin, S., & Wade, D. T. (2011). Motor imagery in patients with a right hemisphere stroke and unilateral neglect. Brain Injury, 25(4), 387–393. doi:10.3109/02699052.2011.558041.
Wai, Y.-Y., Wang, J.-J., Weng, Y.-H., Lin, W.-Y., Ma, H.-K., Ng, S.-H., et al. (2012). Cortical involvement in a gait-related imagery task: comparison between Parkinson’s disease and normal aging. Parkinsonism & Related Disorders, 18(5), 537–542. doi:10.1016/j.parkreldis.2012.02.004.
Warner, L., & McNeill, M. E. (1988). Mental imagery and its potential for physical therapy. Physical Therapy, 68(4), 516–521.
Wehner, T., Vogt, S., & Stadler, M. (1984). Task-specific EMG-characteristics during mental training. Psychological Research, 46(4), 389–401.
Welfringer, A., Leifert-Fiebach, G., Babinsky, R., & Brandt, T. (2011). Visuomotor imagery as a new tool in the rehabilitation of neglect: a randomised controlled study of feasibility and efficacy. Disability and Rehabilitation, 33(21–22), 2033–2043. doi:10.3109/09638288.2011.556208.
Williams, J., Pearce, A. J., Loporto, M., Morris, T., & Holmes, P. S. (2012). The relationship between corticospinal excitability during motor imagery and motor imagery ability. Behavioural Brain Research, 226(2), 369–375. doi:10.1016/j.bbr.2011.09.014.
Wolpert, D. M., & Flanagan, J. R. (2001). Motor prediction. Current Biology, 11(18), R729–732.
Wolpert, D. M., & Ghahramani, Z. (2000). Computational principles of movement neuroscience. Nature Neuroscience, 3(Suppl), 1212–1217. doi:10.1038/81497.
Wondrusch, C., & Schuster, C. (2013). A standardized motor imagery introduction program (MIIP) for neuro-rehabilitation: development and evaluation. Front Hum Neurosci, 7, doi:10.3389/fnhum.2013.00477.
Wrigley, P. J., Press, S. R., Gustin, S. M., Macefield, V. G., Gandevia, S. C., Cousins, M. J., et al. (2009). Neuropathic pain and primary somatosensory cortex reorganization following spinal cord injury. Pain, 141(1–2), 52–59. doi:10.1016/j.pain.2008.10.007.
Wu, A. J., Hermann, V., Ying, J., & Page, S. J. (2010). Chronometry of mentally versus physically practiced tasks in people with stroke. American Journal of Occupational Therapy, 64(6), 929–934.
Yaguez, L., Canavan, A. G., Lange, H. W., & Homberg, V. (1999). Motor learning by imagery is differentially affected in Parkinson’s and Huntington’s diseases. Behavioural Brain Research, 102(1–2), 115–127.
Yan, J., Guo, X., Jin, Z., Sun, J., Shen, L., & Tong, S. (2012). Cognitive alterations in motor imagery process after left hemispheric ischemic stroke. PLoS One, 7(8), e42922. doi:10.1371/journal.pone.0042922.
Yildiz, S. K., Turkoglu, S. A., Yildiz, N., Ozturk, A., & Tore, F. (2007). Sympathetic skin responses of the face and neck evoked by electrical stimulation. Autonomic Neuroscience, 134(1), 85–91.
Zhang, H., Xu, L., Wang, S., Xie, B., Guo, J., Long, Z., et al. (2011). Behavioral improvements and brain functional alterations by motor imagery training. Brain Research, 1407, 38–46. doi:10.1016/j.brainres.2011.06.038.
Zhang, H., Xu, L., Zhang, R., Hui, M., Long, Z., Zhao, X., et al. (2012). Parallel alterations of functional connectivity during execution and imagination after motor imagery learning. PLoS One, 7(5), e36052. doi:10.1371/journal.pone.0036052.
Acknowledgments
We gratefully acknowledge Audrey Fournié for her technical assistance in data collection.
Conflict of Interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material
(DOC 125 kb)
Rights and permissions
About this article
Cite this article
Di Rienzo, F., Collet, C., Hoyek, N. et al. Impact of Neurologic Deficits on Motor Imagery: A Systematic Review of Clinical Evaluations. Neuropsychol Rev 24, 116–147 (2014). https://doi.org/10.1007/s11065-014-9257-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-014-9257-6