
Abstract
This review was aimed at systematically investigating the evidence suggesting that obese individuals demonstrate impaired performance on behavioural tasks examining executive functioning abilities. A systematic review of literature was carried out by searching five separate databases (PsycINFO, MEDLINE, EMBASE, CINAHL and PubMed) and a hand search of relevant journals. Twenty-one empirical papers were identified from the search criteria and the results were considered in relation to different executive functioning domains. There is little consistency of results both within and across different domains of executive functioning. The review suggests that obese individuals show difficulties with decision-making, planning and problem-solving when compared to healthy weight controls, with fewer difficulties reported on tasks examining verbal fluency and learning and memory. A lack of replication and underreporting of descriptive data is a key limitation of studies in this area and further research is needed to examine the mechanisms underpinning the relationship between obesity and executive functioning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The purpose of this review is to examine evidence looking at the relationship between obesity and measures of executive functioning.
Obesity
Obesity is a significant and increasing challenge to public health (Zinzindohoue et al. 2003). Obese individuals often have a reduced life expectancy and increased healthcare needs, mostly due to the elevated risk of co-morbidities which are responsible for 2.5 million deaths a year (Buchwald et al. 2004). The physical consequences associated with obesity, including elevated risk of developing Type 2 Diabetes, hypertension and other cardio-vascular diseases, have been well documented (Avenell et al. 2004) and have influenced public policy relating to the treatment of obesity (NICE 2006).
More recent research however, has sought to look beyond the physical consequences associated with obesity and instead examine the relationship between obesity and cognitive functioning. Initial studies examining the impact of obesity on cognitive functioning found that those individuals with a high Body Mass Index (BMI) scored significantly lower on tests of general cognitive ability and have a steeper longitudinal decline in cognitive ability in comparison to their thinner peers (Dahl et al. 2010). These findings have been consistent amongst groups of overweight children and adolescents (Cserjési et al. 2007) as well as older obese individuals (Gunstad et al. 2010).
Executive Functioning
Executive functioning can be thought of as an umbrella term encompassing a variety of different cognitive domains involved in regulating behaviour and adapting to novelty (Gilbert and Burgess 2008). Such domains include planning, organising, problem-solving, attention, set-shifting and inhibitory control (Lezak 1995). Executive functions are often referred to as “higher level” cognitive abilities due to their putative role in modulating “lower level” abilities (Alvarez and Emory 2006; Gilbert and Burgess 2008). Authors have also noted that executive functioning is a difficult construct to define as it encompasses a wide range of different abilities that are difficult to separate (Morgan and Lilienfeld 2000), although fractionation has been suggested from both behavioural (Miyake et al. 2000) and neuropsychological (Stuss and Alexander 2007) perspectives.
Executive Functioning and Obesity
Whilst a number of studies have reviewed the relationship between executive functioning and eating, with a particular focus on eating disorders such as anorexia nervosa (Lopez et al. 2007), few reviews have specifically examined executive functioning and obesity. Most recently Van den Eynde et al. (2011) reviewed studies examining the relationship between neurocognition and bulimic eating disorders, which included some studies with individuals with Binge eating disorder (BED), many of whom were also obese. They concluded that there was no clear neurocognitive profile of individuals with BED, citing methodological heterogeneity and small sample sizes as a limitation of the current research. It is also important to note that of the studies included in the review only one (Brogan et al. 2010) using a sample size of seventeen reported a mean BMI >30. Most of the other studies did not feature a binge eating group that were clinically obese. As such, this review was not directly examining the relationship between weight and executive functioning, which the current review proposes to do.
Joseph et al. (2011) recently reviewed the neurocognitive link between physical activity and eating behaviour. In particular they discuss the top-down regulatory role of executive functioning and report findings that less efficient response inhibition and poorer decision-making has been found in individuals with an elevated BMI. Whilst this review posits a hypothesis of a neurocognitive link between physical activity and eating behaviour, it did not include a systematic review of empirical data that specifically focused on the executive functioning abilities of obese individuals.
As part of a larger review, Van den Berg et al. (2009) reviewed the evidence that obesity might impact on cognition. Six studies were included in the review and obesity was found to be associated with impaired cognitive performance across one or more cognitive domains. However, the included studies were predominantly examining general intellectual abilities or memory as opposed to executive functioning. So whilst there were some indications of cognitive difficulties in obese individuals, the specific area of executive functioning was not explored in this review.
The Current Review
This review aims to systematically examine all published papers investigating the relationship between BMI and executive functioning. More specifically, it aims to address the following questions;
-
Do overweight/obese individuals demonstrate impaired performance on behavioural tasks of executive functioning when compared to healthy weight controls?
-
If performance is impaired, on which tasks or areas of executive functioning do individuals demonstrate a deviation from healthy controls?
-
Are there other factors which may account for differences in task performance other than BMI?
-
If there is a relationship between BMI and executive functioning, are there any indications of direction of causality or explanations of the nature of this relationship?
Methods
Search Strategy
Potential studies were identified through searching the Titles and Abstracts of articles indexed in PsycINFO, MEDLINE, EMBASE, CINAHL and PubMed. The search term obesity and its relevant synonyms (obes* or overweight or BMI or body mass index or excess weight) were combined with executive function and its specified synonyms (exec* function* or exec* control or neuropsychol* or neurocognit* or exec* dysfunction or mental flexibility). In addition, hand searches of two key journals, Appetite and Obesity were also conducted. Finally, reference lists of papers identified during the searches were also hand searched for additional relevant papers.
Study Selection
As expected, the broad set of search terms identified many publications that were not relevant to the aims of this review. An initial screening was based on the title and abstract of the identified papers. The search was limited to empirical papers written in English that had appeared in peer-reviewed journals published between January 1990 and November 2012. Each study featured human, adult participants aged 18–65 who were either overweight or obese based on Body Mass Index (BMI>25). Each paper included at least one established behavioural measure associated with executive functioning (e.g. verbal fluency (Benton and Hamsher 1976), Wisconsin Card Sort Task (Grant and Berg 1948), Hayling and Brixton (Burgess and Shallice 1997), Iowa Gambling Task (Bechara et al. 1994), Go-No Go task (Logan et al. (1997)), Stop Signal Task (Logan 1994), Trail Making Test (Reitan 1958), Stroop (Trenerry et al. 1989), Digit Span (Wechsler, 1997), Behavioural Assessment of Dysexecutive Syndrome (Wilson et al. 1996) and the Tower of London Task (Shallice 1982). Included papers also had to report sufficient demographic detail (gender, age range and mean, BMI range and mean) as well as clear task descriptions and statistical data to warrant comparison between studies.
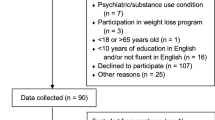
1020 articles were initially identified. 866 were immediately excluded because they did not meet the above criteria or because they were duplications. The abstracts of the remaining 154 articles were reviewed in detail and a further 111 papers were excluded A full text review of the remaining 43 articles was carried out and 22 were excluded for the reasons identified in Fig. 1, which illustrates the selection process for inclusion in this review. A final 21 articles were included for review; these are shown in Table 1.

Flowchart describing results of search strategy used in systematic review
Description of Studies
Study Design and Methodology
All studies, with the exception of two (Smith et al. 2010 and Spitznagel et al. 2011) had a cross-sectional design. The remaining two used a longitudinal design (Spitznagel et al. 2011) and random assignment (Smith et al. 2010). Seven studies used a healthy normal weight control group to compare to an obese group (Cserjesi et al. 2009; Gunstad et al. 2007; Pignatti et al. 2006; Volkow et al. 2008; Svaldi et al. 2010; Nederkoorn et al. 2006; Weller et al. 2008;). Seven studies made further group comparisons by comparing an obese group to a binge eating group or overweight group as well as a control group (Mobbs et al. 2011; Fergenbaum et al. 2009; Davis et al. 2010; Gonzales et al. 2010; Davis et al. 2004; Hendrick et al. 2011; Danner et al. 2012). One study compared performance with three other groups (Brogan et al. 2010). Two studies did not feature a control group, but instead compared performance to normed task data (Pierobon et al. 2008; Boeka and Lokken 2008). Two studies compared a binge eating obese group to a non- binge eating obese group (Duchesne et al. 2010; (Galioto et al. 2012)) and two studies used only one type of participant (Smith et al. 2010; Spitznagel et al. 2011).
The mean sample size used in each study was 103.52 (median = 75) and ranged from 21–408. The age of participants ranged from 18 to 65, with the exception of one study (Gunstad et al. 2007) which split the sample into an old and a young group. Eight studies featured an all female sample (Brogan et al. 2010; Davis et al. 2010; Cserjesi et al. 2009; Svaldi et al. 2010; Nederkoorn et al. 2006; Davis et al. 2004 & Hendrick et al. 2011; Danner et al. 2012), seven studies featured a predominantly female sample (Mobbs et al. 2011; Boeka and Lokken 2008; Pignatti et al. 2006; Duchesne et al. 2010; Smith et al. 2010& Weller et al. 2008; Spitznagel et al. 2011; Galioto et al. 2012), another study used predominantly male participants (Pierobon et al. 2008) and four studies used equivalent numbers from both genders (Fergenbaum et al. 2009; Gunstad et al. 2007; Volkow et al. 2008 & Gonzales et al. 2010). Where comparable numbers of male and female participants were recruited, only one study examined whether gender was a potential co-variate (Fergenbaum et al. 2009) and found that both males and females showed similar levels of impairment. The potential impact of gender on executive functioning in obese individuals remains unclear as most studies did not consider this as a factor; however it is of note that the majority of studies featured predominantly or exclusively female samples.
All studies used the established conventions for determining weight classification according to World Health Organisation (WHO 2011), e.g. underweight: BMI< 18.5; normal: BMI= 18.5-24.99; overweight: BMI= 25-29.99; obese: BMI>30. Nineteen reported a mean BMI and standard deviation, whereas two examined predictors of BMI and so did not report this data (Spitznagel et al. 2011 and Fergenbaum et al. 2009). Of the obese groups recruited across all studies, the mean BMI was 37.1, ranging from 30–61.3. Whilst all studies reported a mean BMI >25 and most had a mean BMI >30, in some studies the standard deviation was large, thus increasing the heterogeneity of the overweight/obese group. In such cases it is not always clear whether the data set was examined for skewness or kurtosis or whether this factor was considered within the statistical analysis. It also makes it difficult to investigate potential differences in executive functioning performance between those who are obese and those who are morbidly obese.
Outcome Measures
Whilst all studies used at least one behavioural measure of executive functioning with obese individuals, studies varied in their reasons for investigating this relationship. Five sought to directly examine the relationship between obesity and cognition (Boeka and Lokken 2008), four of which were specifically interested in impulsivity as a factor (Pignatti et al. 2006; Nederkoorn et al. 2006; Weller et al. 2008 & Davis et al. 2004). Four studies sought to examine the relationship between obesity and cognition in the presence of a third factor e.g. sleep problems (Pierobon et al. 2008), cardiovascular disease, (Fergenbaum et al. 2009) age (Gunstad et al. 2007) or mood (Cserjesi et al. 2009). Three studies examined the relationship between obesity and cognitive functioning using brain imaging (Volkow et al. 2008; Gonzales et al. 2010 and Hendrick et al. 2011). Seven studies sought to compare performance on measures of executive functioning between obese individuals and those with other eating disorders (Mobbs et al. 2011; Svaldi et al. 2010; Brogan et al. 2010; Davis et al. 2010; Duchesne et al. 2010; Danner et al. 2012; Galioto et al. 2012). Two studies were evaluating the effect of a weight loss intervention on executive functioning in obese individuals (Smith et al. 2010) or the impact of executive functioning on ability to lose weight (Spitznagel et al.2011).
Statistical Power and Effect Sizes of the Findings
Adequate sample size is an important consideration when determining whether a study had the necessary statistical power to detect an effect. Similar reviews in this area have suggested that in order to detect a large effect size (Cohen’s d = 0.8) with 80 % power at 0.05 significance level, there would need to be 25 participants in each experimental group (Van den Eynde et al. 2011). Of the twenty-one studies included in this review, eleven would have met these sample size requirements (Fergenbaum et al. 2009, Davis et al. 2010, Cserjesi et al. 2009, Boeka and Lokken 2008, Gunstad et al. 2007, Duchesne et al. 2010, Smith et al. 2010, Nederkoorn et al. 2006, Weller et al. 2008, Spitznagel et al. 2011).
Effect sizes were reported or could be calculated from ten of the studies included in the review. Significant data generally reported medium (0.5) or large (0.8) effect sizes, whereas non-significant data generally had small or medium effect sizes.
Other Factors Impacting Executive Functioning Abilities
When considering the relationship between obesity and executive functioning, it is important to consider any other factors which may be moderating or mediating this effect.
Education/Intelligence
Education level/years was measured in sixteen of the studies reviewed (Brogan et al. 2010;, Cserjesi et al. 2009, Boeka and Lokken 2008, Pignatti et al. 2006, Duchesne et al. 2010, Mobbs et al. 2011; Davis et al. 2010; Pierobon et al. 2008; Gunstad et al. 2007; Volkow et al. 2008; Smith et al. 2010; Gonzales et al. 2010; Weller et al. 2008; Svaldi et al. 2010; Danner et al. 2012 and Spitznagel et al. 2011. Most studies used years of education as an outcome measure, but some also used an IQ estimate (Spot the Word, WAIS III Subscales, Shipley Institute of Living Scale, Ravens Matrices, TONI) (Boeka and Lokken 2008; Pignatti et al. 2006; Duchesne et al. 2010; Pierobon et al. 2008; Gunstad et al. 2007 and Weller et al. 2008) . Seven studies used either education years or IQ estimates as a way of matching clinical and control participants (Brogan et al. 2010;Cserjesi et al. 2009; Boeka and Lokken 2008; Pignatti et al. 2006; Duchesne et al. 2010; Danner et al. 2012 and Svaldi et al. 2010), the remaining nine used education/IQ as a variable. Of those studies, six found that there were no significant differences in education years or IQ between groups; one found that the clinical group had a slightly higher IQ when compared to normed data. In contrast, one study found that not only did years of education differ between clinical and control groups but that this difference moderated the effect of impaired task performance (Davis et al. 2010) with clinical patients no longer demonstrating an impaired performance on IGT when education years were considered. The remaining two (Gunstad et al. 2007 and Smith et al. 2010) which used education/IQ as a covariate with their analyses found that obese individuals were still impaired on tasks of executive functioning even after these factors were considered.
Mood
Fourteen studies used a mood measure within their design (Mobbs et al. 2011; Cserjesi et al. 2009; Pierobon et al. 2008, Boeka and Lokken 2008; Pignatti et al. 2006; Duchesne et al. 2010; Svaldi et al. 2010; Gonzales et al. 2010; Davis et al. 2010; Gunstad et al. 2007; Smith et al. 2010; Danner et al. 2012; Galioto et al. 2012 and Svaldi et al. 2010). Most studies used the Beck Depression Inventory II (BDI-II) as an index of low mood and the State Trait Anxiety Inventory (STAI) as a measure of anxiety.
In relation to depressive symptoms some studies screened out depressed individuals (Duchesne et al. 2010) or did not report their findings vis a vis mood measures (Pigantti, Gunstad et al. 2007 and Smith et al. 2010.) Of those which report data, one found no performance differences between obese individuals and controls (Gonzales et al. 2010) and another found that there was no relationship between depressive symptoms and task performance (Svaldi et al. 2010). Two studies found that obese patients were more depressed than controls (Cserjesi et al. 2009, Boeka and Lokken 2008) and another found no difference between controls and obese individuals, but that obese individuals with BED were more depressed than obese people without. One study reports a trend towards impaired performance on IGT task and overeating in response to depressive symptoms (Davis et al. 2010).
For studies which included a measure of anxiety (Mobbs et al. 2011; Cserjesi et al. 2009, Pierobon et al. 2008; Galioto et al. 2012 and Gonzales et al. 2010), two found that obese individuals did not differ from controls (Pierobon et al. 2008 and Gonzales et al. 2010), one found that obese individuals were more anxious than healthy weight controls and the final study reported that only those who were obese and also had BED reported significantly higher levels of anxiety than either healthy weight controls or obese individuals.
In summary, it is unclear whether obese individuals report higher levels of psychopathology than healthy weight controls as the findings are mixed and the link between either depressive or anxious symptomatology and its impact on task performance has not been examined sufficiently or replicated enough to determine whether it might explain differences on executive functioning task performance. Furthermore, additional factors such as socioeconomic status that could potentially mediate relationships between obesity and performance on executive functions tasks were not investigated in the reviewed studies. Thus the potential mediating impact of additional social and environmental factors has yet to be systematically explored.
Results
Neurocognitive Findings
Consistent with other reviews in this area, (Duchesne et al. 2010 & Van den Eynde et al. 2011) the findings from the reviewed studies were categorised according to the neurocognitive construct e.g.; impulsivity/inhibitory control, set-shifting, verbal fluency and decision-making. However, the classification of specific tasks to a given domain is somewhat arbitrary as tasks may extend across more than one executive functioning domain.
Inhibitory Control/Impulsivity
Stroop Task
Five studies used the Stroop task (Gunstad et al. 2007; Duchesne et al. 2010; Smith et al. 2010; Volkow et al. 2008; Galioto et al. 2012). In this task, individuals are asked to say the ink colour of written words whilst inhibiting reading the word, e.g. “red” written in blue ink. Most studies used the Colour Word variant thus allowing comparisons to be made. One study found that performance on the Stroop task was strongly correlated to BMI with poorer performance associated with higher BMI (Gunstad et al. 2007) and that performance on this task improved following weight loss (Smith et al. 2010). Two found no relationship between Stroop performance and BMI (Volkow et al. 2008; Duchesne et al. 2010) and one found no differences in performance when comparing an obese and BED group (Galioto et al. 2012). Thus there was no consistent evidence that Stroop performance is impaired for obese individuals.
Stop Signal Task or Go- No Go Task
Three studies used a variant of the stop signal task (Nederkoorn et al. 2006; Hendrick et al. 2011; Mobbs et al. 2011). In the stop signal task, participants are asked to respond as quickly as possible on a choice reaction time task, unless a stop signal is presented in which case they must inhibit their response. Two found that there were no significant differences in reaction times between obese and normal weight groups (Nederkoorn et al. 2006 & Hendrick et al. 2011). One study comparing healthy controls, obese participants and obese participants with BED used a slightly different version of the task using food-related and body-related stimuli (Mobbs et al. 2011). Overall both obese groups made more errors than healthy weight controls. Whilst the two obese groups did not differ in reaction times, the BED group made more errors on both food and body stimuli than obese participants. It would seem that obese individuals show mixed performance on the stop signal task.
Hayling Sentence Completion Task
On the Hayling task, where individuals have to inhibit a logical response to specific sentences, Cserjesi et al. (2009) found that obese individuals performed worse than normal weight controls on both parts of the task and therefore demonstrated difficulty both inhibiting a response but also with the control variant of this task which is not specifically measuring inhibition.
There is significant variation in impulsivity/inhibitory control performance reported by different studies, with some reporting that obese individuals demonstrate impaired performance and others not observing any difference in performance. It is worth noting that those not reporting a significant group difference had a sample size ranging from 13–38, whereas those reporting significant group differences had sample sizes ranging from 16–198. It is possible that the failure to detect a group difference, in part reflects insufficient power.
Set-Shifting
Trail Making Test (TMT)
The TMT is a brief executive task with two parts. Part A asks participants to connect a series of numbers on a page in numerical order; Part B asks participants to draw a line connecting numbers and letters spread across a page in alpha numerical order as quickly and accurately as possible, i.e. 1, a, 2, b, 3, c… Part A is used to measure speed of attention and sequencing and part B measures switching in addition to these factors (Spreen and Strauss 1998). Eleven studies used the TMT or a variant of it, as an outcome measure (Fergenbaum et al. 2009; Cserjesi et al. 2009; Pierobon et al. 2008; Boeka and Lokken 2008; Gunstad et al. 2007; Duchesne et al. 2010; Smith et al. 2010; Svaldi et al. 2010; Gonzales et al. 2010; Spitznagel et al. 2011, Galioto et al. 2012). Most studies used the completion time as a dependent variable, of these studies, two found a correlation between increased BMI and increased completion time on TMT part B (Cserjesi et al. 2009; Boeka and Lokken 2008) but no difference on errors. One study found this effect was only significant for females and that it disappeared when other factors were controlled for (Boeka and Lokken 2008). Others showed no difference between obese and BED (Duchesne et al. 2010; Galioto et al. 2012) or between normal, overweight or obese groups (Gonzales et al. 2010).
Other studies computed an equivalent score (Pierobon et al. 2008) or a proportionate score (Svaldi et al. 2010), one reported that clinical groups (including obese and other eating disordered groups) performed more slowly (Svaldi et al. 2010) whilst the other showed no differences between obese and control participants (Pierobon et al. 2008). Two studies used a modified version of the TMT (Gunstad et al. 2007 and Spitznagel et al. 2011), one found a correlation between BMI and performance on Trails B, and one found trails A to be a significant predictor of weight loss at 12 weeks and 12 months. Another found that timed scores on the TMT improved as individuals lost weight (Smith et al. 2010). One study used TMT as a predictor and found that obese individuals were more likely to be correctly classified as obese using the TMT.
Differences in the ways in which studies have computed scores from the TMT make it difficult to directly compare performance of individuals across studies. For those using completion times as an outcome variable, obesity did not independently impact on performance. The results were more mixed for studies that computed a proportionate score, and for those that used an adapted version of the TMT, a group difference was found. For studies that used TMT as a predictor, it appeared to significantly predict weight loss in obese people and conversely as weight decreased, performance on the TMT appeared to improve. However, this finding is based on single studies and has yet to be replicated.
Wisconsin Card Sort Test (WCST)
Three studies used the Wisconsin Card Sort Test (WCST) as part of their testing battery (Boeka and Lokken 2008; Volkow et al. 2008; Duchesne et al. 2010). In the original version of this task, participants are given a deck of cards and asked to sort them according to four different key cards (colour, shape, number etc.). Participants are given feedback on their performance as they sort through the cards and every few trials the sorting rule changes without the participant’s knowledge. Their task is to recognise that a change has happened and start sorting the cards according to the new rule as quickly as possible. Most studies used a variant of Grant and Berg’s 1948 task, allowing for comparison. Studies comparing the performance of obese groups to normal weight individuals found that obese individuals made more errors and more perseverative errors than healthy weight controls (Boeka and Lokken 2008; Volkow et al. 2008). One study compared performance between obese and obese individuals with BED, they found that those with BED made more perseverative errors and set failures than control obese participants (Duchesne et al. 2010). Unfortunately this study did not feature a healthy weight comparison group and so it is not known whether obese individuals would have differed in comparison to healthy controls (as reported in other studies) or whether a group difference is only found when binge eating disorder is considered. Overall, obese individuals do seem to show a tendency to make more perseverative errors on this task but not to the same extent as other eating disordered groups. Perhaps a study comparing performance across different eating disordered and obese groups (Obese, Obese with BED, BN, AN as well as healthy weight controls) may help to disentangle this effect.
On set-shifting tasks, once again the findings are mixed. Obese individuals appear to struggle with the WCST but this is based on a limited number of studies using this paradigm. On other set-shifting tasks where the paradigm has been used more extensively, methodological and scoring differences make it difficult to draw any conclusions from the findings.
Verbal Fluency
Controlled Oral Word Association Test –COWA-T)
Five studies utilised a Verbal Fluency task (Cserjesi et al. 2009; Boeka and Lokken 2008; Smith et al. 2010; Galioto et al. 2012 and Gonzales et al. 2010). In this task, individuals are asked to name as many words as possible beginning with a particular letter within one minute. All studies used the Controlled Oral Word Association Test (COWAT) (Benton and Hamsher 1976). Three found no difference in test performance between obese and non-obese individuals (Cserjesi et al. 2009; Smith et al. 2010, and Gonzales et al.,2010) and one study found obese individuals’ scores were better than normed data (Boeka and Lokken 2008). A further study reported no difference between task performance of obese and BED participants (Galioto et al. 2012). Generally obese individuals show no differences on verbal fluency tasks when compared to control participants and seem to perform equivalently or even better than normed data.
Learning and Memory
Digit Span
Eight studies used digit span as an outcome measure within their study (Cserjesi et al. 2009; Gunstad et al. 2007; Duchesne et al. 2010; Smith et al. 2010; Volkow et al. 2008; Gonzales et al. 2010; Spitznagel et al. 2011; Galioto et al. 2012). Digit span appears as a subtest in the WAIS- III and WMS – III tests and consists of digits forward and digits backwards. Participants are asked to repeat verbally increasing number strings that they hear until they fail to complete two successive trials. For digits backwards, individuals repeat a reversed version of number strings that they hear until they fail two successive trials at a given number string length. All studies with the exception of one (Gunstad et al. 2007) used a Digit span score derived from combined digit span forward and digit span backward scores, thus allowing a comparison across different studies to be made. One study found a correlation between increased BMI and poorer performance on the digit span task (Volkow et al. 2008). One found an impairment in performance when comparing obese individuals with BED and a control obese group (Duchesne et al. 2010) and one study found no group differences in task performance (Galioto et al. 2012). All other studies found no relationship between BMI and digit span. Performance on digit span tasks did not predict weight loss (Spitznagel et al. 2011) or change as a result of weight loss (Smith et al. 2010). A relationship between digit span and BMI was only found when combined with mood measures (Cserjesi et al. 2009) or age (Gunstad et al. 2007).
Obese individuals in general, do not seem to demonstrate difficulty with this specific task and performance does not predict weight loss or change as a result of weight loss. Generally studies that have found a difference in performance between obese individuals and controls are those which have also examined it in relation to another factor e.g. mood, age or BED.
Decision-Making
Iowa Gambling Task
Five studies used the Iowa Gambling Task (IGT) as a measure of executive functioning (Brogan et al. 2010; Davis et al. 2010; Pignatti et al. 2006; Davis et al. 2004; Danner et al. 2012). In this task individuals are given hypothetical money and asked to make decisions to maximise their gains with minimal instruction in relation to the rules. They have to choose between cards from four different decks, two of which yield high immediate gains, but high future losses and two decks which yield low immediate gains but smaller future losses. All studies used the computerised version of Bechara et al. (1994) task and all studies examined both net scores and block scores thus allowing comparisons across studies to be made. Four of the five studies looked at group differences (Brogan et al. 2010; Davis et al. 2010; Pignatti et al. 2006, Danner et al. 2012), whilst one used a regression model (Davis et al. 2004) to analyse the data. Overall, all studies found that obese individuals’ performance was worse than healthy weight controls. Two studies also found that obese individuals were less likely to show an improvement over blocks (Davis et al. 2004; Pignatti et al. 2006). However of the studies which compared performance to that of individuals with eating disorders (e.g. BED and AN compared to obese people), there was no difference between their performance and that of obese individuals (Brogan et al. 2010; Davis et al. 2010; Danner et al. 2012). Several studies also considered the impact of education on task performance; one study found the effect of weight disappeared when educational level was accounted for (Davis et al. 2010), whilst another found it had no effect (Pignatti et al. 2006) and two further studies merely controlled for education (Brogan et al. 2010; Danner et al. 2012). In summary, obese individuals do seem to demonstrate impaired performance on this task compared to healthy weight controls, and in some cases where a comparison was made, they show a level of impairment similar to that shown by clinically eating disordered individuals.
Delay Discounting Task
The delay discounting task looks at how individuals make decisions between low short term gains and higher long term gains. Individuals are offered different monetary values; a lower amount now or a higher amount later on. The length of delay is manipulated and the outcome measure is the point at which someone switches from the delay to an immediate reward. A variant of the delay discounting task was used in three studies (Davis et al. 2010; Nederkoorn et al. 2006; Weller et al. 2008). Whilst the construction of this task appeared consistent across studies, there were differences in the absolute amounts, currency, number of delays and also the way in which participant scores were computed which makes it difficult to compare across studies. One study found no difference in task performance between obese and normal weight controls (Nederkoorn et al. 2006), whilst another study only found a difference when gender was considered in addition to weight, with obese females tending to chose smaller more immediate rewards in comparison to control weight females (Weller et al. 2008). A third study did find a difference between obese and healthy weight control groups, but only when comparing performance at specific time delays (Davis et al. 2010). Overall it seems that performance on this task was mixed when comparing across studies and that any differences observed were subtle or dependent on gender.
Maze Task
In the Maze Task individuals have to identify a hidden pathway through a grid of circles. Individuals receive visual and verbal feedback on performance but have to complete the task twice without an error in order to pass. Three studies used a computerised version of the Austen maze task (Walsh 1994) and both used the number of errors as the dependent variable (Gunstad et al. 2007; Spitznagel et al. 2011; Galioto et al. 2012). One study found that the number of errors was a significant predictor of BMI (Spitznagel et al. 2011) and another found that normal weight individuals performed better than obese individuals (Gunstad et al. 2007), whilst a third found no difference in performance between an obese and a BED group of participants (Galioto et al. 2012). From rather limited evidence, it seems that individuals with a high BMI may have difficulty with the maze errors task.
Game of Dice Task
One study used the Game of Dice task (Svaldi et al. 2010) where participants have to guess the outcome of a dice game with the aim of maximising their gains. The authors reported a significant difference in scores between obese individuals with BED and overweight controls, suggesting that individuals with BED selected more disadvantageous scores more often than those who were overweight but did not have BED.
In summary, obese individuals consistently show poor performance on specific decision-making tasks e.g. Iowa Gambling task, Maze Task and Game of Dice but factors such as education level, gender and binge eating symptomatology can impact upon task performance.
Planning and Problem-solving
Behavioural Assessment of Dysexecutive Syndrome (BADS)
One study comparing obese individuals and obese individuals with BED used three subtests from the BADS which predominantly examine planning and problem-solving (Duchesne et al. 2010). The Zoo Map task requires individuals to plan a journey around a zoo following specific instructions and rules. On this task Duchesne et al. 2010 found that obese individuals with BED made more errors than obese controls but did not differ on planning or completion time or in a second condition when provided with increased task structuring. On the modified six elements task where participants are required to complete some of six different tasks within 10 min following specific rules, the authors found that obese participants with BED performed worse than obese controls. This finding was repeated again on the Action Program Task, where individuals have to problem-solve a practical task with minimal guidance, with obese controls able to complete more of the stages of the task unaided than those with BED.
Whilst the findings indicate that obese individuals with BED show difficulty with planning, the absence of a healthy weight control group makes it difficult to conclude whether or not having a higher BMI generally might contribute to difficulties with decision-making or whether binge eating pathology alone can explain this distinction in task performance. Additionally the findings are based on only one dataset.
Discussion
General Findings
The key question which prompted this review was whether obese individuals demonstrate impaired performance on behavioural tasks of executive functioning when compared to healthy weight controls. Methodological differences and incomplete information in relation to task procedure and the reporting of descriptive data made this a difficult question to answer. Overall, when considering specific domains, obese individuals seem to demonstrate an impaired performance consistently on only one domain of executive functioning; tasks measuring decision-making and on only one other task in the set-shifting domain (WCST). All other domains of executive functioning report mixed findings across studies in relation to the association between obesity and executive functioning. A possible explanation why we might see impairment in only certain areas might be to do with the sensitivity of the tasks used. The majority of behavioural tasks used to examine executive functioning are designed for use with brain injured populations and thus may be insensitive to detecting what may be quite subtle distinctions in executive functioning in obese individuals. This may also explain why differences were only observed in the more complex executive functioning tasks (e.g. IGT, Maze Task) as these tasks were more sensitive at detecting a small deficit. Alternatively, it may be possible that obese individuals show subtle impairments over a range of different aspects of executive functioning, but that studies which failed to detect this effect may have been underpowered and be using an insufficient sample size to detect what may be quite a small effect. It is also worth noting that due to incomplete data sets it was not possible to make a statistical comparison between the different executive functioning domains and so the differences in patterns of result may also reflect statistical chance.
However, even studies which do suggest that obese individuals might demonstrate specific executive impairments need to be interpreted with caution. These findings have their limitations as they are based on a small number of studies and factors such as education, gender and mood also impact on task performance. Unmeasured factors such as socioeconomic status might also play a mediating role. In these domains, but also across the board, there is a need for more study replication and parity across study design to allow for more adequate comparison.
Additionally, a number of studies failed to include effect sizes within their reported statistics or did not report sufficient summary data to allow this to be calculated for the purpose of comparison in relation to the size of the effect they are reporting. Also, most papers did not report a power calculation and several studies may have been underpowered due to small sample sizes.
The Relationship between Obesity and Executive Functioning
Of those studies which did report an association between obesity and impaired executive functioning, the direction of the relationship remains unclear and most studies stress that causality may occur in either direction, with either obesity impacting on executive functioning or impaired executive functioning increasing the risk of obesity. (Boeka and Lokken 2008). Difficulty maintaining weight loss and difficulties adjusting and adhering to post-bariatric lifestyle changes have been used as evidence to support the idea that individuals with executive functioning difficulties may have a propensity to become obese (Boeka and Lokken 2008). Others have suggested that making good food choices in modern life requires forethought, planning and good self-regulation in order to avoid overeating (Davis et al. 2010; Duchesne et al. 2010). These are skills which require good executive functioning abilities and so there is a suggestion that impaired executive functioning leads to obesity via poor food choices. This idea might also fit with the findings from the current review that distinctions between obese and non-obese individuals tends to occur on tasks measuring planning, problem-solving and decision-making, abilities needed to make good food and lifestyle choices. Finally, some studies also report on previous research which showed a reduction in BMI following the administering of methylphenidate, a drug commonly used to treat ADHD (Nederkoorn et al. 2006). The implication drawn from these findings is that the drug enhances inhibitory control leading to reduced calorific intake and weight loss as a result.
However, for this explanation to be true, we would expect poor executive functioning to be directly related to eating behaviour in obese individuals e.g. reporting of overeating/bingeing and poor choices to be directly related to poor task performance. However, a number of studies in this review failed to include a measure of reported eating behaviour and so this comparison could not be made. Of those which did include a measure of eating pathology, this was usually used to help distinguish between obese and obese binge-eating participants and not analysed in conjunction with task performance (Mobbs et al. 2011; Boeka and Lokken 2008; Pignatti et al. 2006; Duchesne et al. 2010) and thus the relationship between eating pathology and executive functioning was not directly examined. Only two studies made such comparison (Davis et al. 2004; Svaldi et al. 2010), neither found a significant correlation between eating pathology (binge frequency, emotional overeating) and performance on executive functioning tasks, although one reported a tendency for those who showed poorer decision-making to also demonstrate overeating tendencies. In order to show that executive functioning might lead to obesity through the mechanism of disordered eating due to poor decision-making/self-control, future research needs to directly compare these factors, preferably using a prospective design allowing pre and post measures to be compared.
In contrast to this potential causal relationship, some studies have suggested that being obese may, (even in the absence of other co-morbidities that might impact on cognitive abilities) lead to impaired executive functioning (Volkow et al. 2008; Gunstad et al. 2007). Studies have suggested that individuals with a larger body mass experience reduced blood flow to certain areas of the brain and therefore the metabolic activity of the brain is reduced and cognitive functioning is negatively affected (Gonzales et al. 2010). Other studies have focussed less on the role of reduced blood flow, but instead on glucose and insulin dysregulation in the brain which may impact specifically on prefrontal regions and dopaminergic systems of the brain and thus impact upon executive functioning (Volkow et al. 2008). Other individuals have suggested that the increase in adipocytes seen in obese individuals could also lead to reduced cognitive functioning (Boeka and Lokken 2008). A further argument suggesting that obesity might contribute to impaired executive functioning, is the finding that cognitive abilities, in particular executive functioning improve following weight loss, suggesting that a reduction in body mass leads to improved executive functioning (Smith et al. 2010; Hendrick et al. 2011) . However some researchers have argued that whilst there is an improvement in executive functioning following weight loss, the level of functioning is still not equivalent to that of a healthy weight individual (Spitznagel et al. 2011). This suggests that even when body mass is reduced, individuals still show a cognitive deficit. Either carrying excess weight is not impacting on cognition or perhaps the effect of a high BMI on cognition cannot be easily reversed following weight loss. To examine the validity of this argument, it would be helpful to see if reduced blood flow to particular regions found in obese individuals reverses following weight loss.
In summary it seems that at present there is no general consensus in relation to the directionality of the relationship between obesity and impaired executive functioning. Impaired executive abilities may lead to poor decision-making, poor inhibition and reduced mental flexibility which could lead to poorer food choices and overeating leading to weight gain. In addition, a number of biological explanations for why obese individuals might demonstrate disrupted brain activation have been suggested which might in turn impact on executive performance (Brogan et al. 2010; Cserjesi et al. 2009; Davis et al. 2010; Svaldi et al. 2010). However, the inconsistency of results between the studies examined here makes it unlikely that any single neurobiological mechanism will provide an adequate account of the link between obesity and executive functioning.
Other factors also make it difficult to determine directionality. For example in the current review, one study made a distinction in decision-making deficits observed between obese individuals and obese individuals with BED with the authors suggesting a continuum of decision-making deficits that were not simply explained by BMI but more related to the presence or absence of eating pathology in addition to BMI. This finding was also replicated in some of the other studies included in the review when comparing obese and obese and BED groups (Duchesne et al. 2010; Mobbs et al. 2011 and Svaldi et al. 2010) where those with BED demonstrated poorer performance than those who were obese. However this result was not found consistently within the literature, with some studies reporting no difference between the two groups when compared to one another (Galioto et al. 2012) or when in the presence of a group of healthy weight controls (Danner et al. 2012). In order to clarify these findings, future research should try to compare performance of healthy weight, obese and BED obese individuals on a range of executive functioning measures.
Implications and Future Research
Whilst this review examined the link between obesity and executive functioning, it did so with some specific limitations. For example the selection criteria for inclusion was that participants had to be eighteen or over, therefore this study excluded a number of interesting recent studies examining the link between childhood obesity and executive functioning. This may have provided some helpful information when thinking about the development of obesity and the causal directionality between executive functioning impairment and obesity (Maayan et al. 2011; Davis et al. 2011; Verdejo-García et al. 2010).
Additionally, future research needs to consider the role of moderating and mediating factors in the relationship between BMI and executive functioning. In particular the roles of mood, gender and education seem to be important, along with social and environmental factors. Examining mood in particular would also link to the direction of research in eating disorders, which are building upon the finding that individuals with eating disorders (Anorexia Nervosa in particular) demonstrate executive impairments and also show difficulty with emotion regulation (Harrison, 2010).
Also this review did not seek specifically to understand or explain the mechanism of executive functioning and eating behaviour. As such the review did not examine how demonstrating an executive functioning impairment might modulate eating behaviour or food choice. As such, whilst this review indicated that there is a link between obesity and executive functioning we cannot yet explain the impact of that link. In order to do this, future research needs to make this link clearer by examining the links between BMI, executive functioning and eating behaviour. Another useful approach could be incorporating eating/food salient stimuli within executive functioning tasks as has been done when looking at executive functioning in the presence of other eating disorders (Bolton 2010; Pender 2011).
In conclusion, whilst a review of the current literature suggests that obese individuals demonstrate consistent impairments on complex executive functioning tasks measuring set-shifting and decision-making, the evidence suggesting a global deficit is less clear. This is in part a reflection of methodological heterogeneity which has led to inconsistent results and difficulty comparing studies. Additionally, future research needs to examine the mechanism of any particular relationship between obesity and executive functioning and in particular its links to eating behaviour.
References
Alvarez, J., & Emory, E. (2006). Executive function and the frontal lobes: a meta-analytic review. Neuropsychology Review, 16(1), 17–42.
Avenell, A., Broom, J., Brown, T., Poobalan, A., Aucott, L., Stearns, S., et al. (2004). Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technology Assessment, 8(21), 1–182.
Bechara, A., Damasio, A., Damasio, H., & Anderson, S. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50, 7–15.
Benton, A., & Hamsher, K. (1976). Multilingual aphasia examination. Iowa City: University of Iowa.
Boeka, A., & Lokken, K. (2008). Neuropsychological performance of a clinical sample of extremely obese individuals. Archives of Clinical Neuropsychology, 23(4), 467–474.
Bolton, H. (2010). Examining perseveration in the context of depression and starvation to inform an understanding of cognitive inflexibility. Doctoral thesis, UCL (University College London).
Brogan, A., Hevey, D., & Pignatti, R. (2010). Anorexia, bulimia, and obesity: shared decision making deficits on the Iowa Gambling Task (IGT). Journal of the International Neuropsychological Society, 16(4), 711–715.
Buchwald, H., Avidor, Y., Braunwald, E., Jensen, M., Pories, W., Fahrbach, K., et al. (2004). Bariatric surgery. JAMA: The Journal of the American Medical Association, 292(14), 1724–1737.
Burgess, P., & Shallice, T. (1997). The Hayling and Brixton tests. Bury St. Edmonds: Thames Valley Test Company.
Cserjési, R., Molnár, D., Luminet, O., & Lénárd, L. (2007). Is there any relationship between obesity and mental flexibility in children? Appetite, 49(3), 675–678.
Cserjési, R., Luminet, O., Poncelet, A., & Lénárd, L. (2009). Altered executive function in obesity. Exploration of the role of affective states on cognitive abilities. Appetite, 52(2), 535–539.
Dahl, A., Hassing, L., Fransson, E., Berg, S., Gatz, M., Reynolds, C., et al. (2010). Being overweight in midlife is associated with lower cognitive ability and steeper cognitive decline in late life. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 65(1), 1–6.
Danner, U., Ouwehand, C., van Haastert, N., Hornsveld, H. & de Ridder, D. (2012). Decision‐making impairments in women with binge eating disorder in comparison with obese and normal weight women. European Eating Disorders Review, 20, 56–62.
Davis, C., Levitan, R., Muglia, P., Bewell, C., & Kennedy, J. (2004). Decision-making deficits and overeating: a risk model for obesity. Obesity, 12(6), 929–935.
Davis, C., Patte, K., Curtis, C., & Reid, C. (2010). Immediate pleasures and future consequences. A neuropsychological study of binge eating and obesity. Appetite, 54(1), 208–213.
Davis, C., Tomporowski, P., McDowell, J., Austin, B., Miller, P., Yanasak, N., et al. (2011). Exercise improves executive function and achievement and alters brain activation in overweight children: a randomised controlled trial. Health Psychology, 20, 91–98.
Duchesne, M., Mattos, P., Appolinário, J., de Freitas, S., Coutinho, G., Santos, C., et al. (2010). Assessment of executive functions in obese individuals with binge eating disorder. Revista Brasileira de Psiquiatria, 32, 381–388.
Fergenbaum, J., Bruce, S., Lou, W., Hanley, A., Greenwood, C., & Young, T. (2009). Obesity and lowered cognitive performance in a Canadian First Nations population. Obesity, 17(10), 1957–1963.
Galioto, R., Spitznagel, M., Strain, G., Devlin, M., Cohen, R., Paul, R., Crosby, R., Mitchell, J. & Gunstad, J. (2012). Cognitive function in morbidly obese individuals with and without binge eating disorder. Comprehensive Psychiatry, 53, 490–495.
Gilbert, S. J., & Burgess, P. W. (2008). Executive function. Current Biology, 18, R110–R114.
Gonzales, M., Tarumi, T., Miles, S., Tanaka, H., Shah, F., & Haley, A. (2010). Insulin sensitivity as a mediator of the relationship between BMI and working memory-related brain activation. Obesity, 18, 2131–2137.
Grant, D., & Berg, E. (1948). A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. Journal of Experimental Psychology, 38, 404–411.
Gunstad, J., Paul, R. H., Cohen, R. A., Tate, D. F., Spitznagel, M. B., & Gordon, E. (2007). Elevated body mass index is associated with executive dysfunction in otherwise healthy adults. Comprehensive Psychiatry, 48(1), 57–61.
Gunstad, J., Lhotsky, A., Wendell, C. R., Ferrucci, L., & Zonderman, A. B. (2010). Longitudinal examination of obesity and cognitive function: results from the Baltimore Longitudinal Study of Aging. Neuroepidemiology, 34(4), 222–229.
Harrison, A. (2010). Emotional Functioning in Eating Disorders: attentional bias, emotion recognition and emotion regulation. Psychological Medicine, 17, 1–11.
Hendrick, O. M., Luo, X., Zhang, S., & Li, C. R. (2011). Saliency Processing and Obesity: A Preliminary Imaging Study of the Stop Signal Task. Obesity, 10, 1–7.
Joseph, R., Alonso-Alonso, M., Bond, D., Pascual-Leone, A., & Blackburn, G. (2011). The neurocognitive connection between physical activity and eating behaviour. Obesity Reviews, 12, 800–812.
Lezak, M. (1995). Neuropsychological assessment. New York: Oxford University Press.
Logan, G. D. (1994). In D. Dagenbach & T. Carr (Eds.), Inhibitory processes in attention, memory and language (pp. 189–239). San Diego: Academic.
Logan, G., Schachar, R., & Tannock, R. (1997). Impulsivity an inhibitory control. Psychological Science, 8, 60–64.
Lopez, C., Tchanturia, K., Stahl, D., Booth, R., Holliday, J., & Treasure, J. (2007). An examination of the concept of central coherence in women with Anorexia Nervosa. International Journal of Eating Disorders, 41, 143–152.
Maayan, L., Hoogendoorn, C., Sweat, V., & Convit, A. (2011). Disinhibited eating in obese adolescents is associated with orbitofrontal volume reductions and executive dysfunction. Obesity, 19, 1382–1387.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cognitive Psychology, 41, 49–100.
Mobbs, O., Iglesias, K., Golay, A., & Van der Linden, M. (2011). Cognitive deficits in obese persons with and without binge eating disorder: investigation using a mental flexibility task. Appetite, 57, 263–271.
Morgan, A., & Lilienfeld, S. (2000). A meta-analytic review of the relationship between antisocial behaviour and neuropsychological measures of executive function. Clinical Psychology Review, 20(1), 113–136.
National Institute for Health and Clinical Excellence. (2006). Obesity: Guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children. CG043. London: National Institute for Health and Clinical Excellence.
Nederkoorn, C., Smulders, F., Havermans, R., Roefs, A., & Jansen, A. (2006). Impulsivity in obese women. Appetite, 47(2), 253–256.
Pender, S. (2011). The neuropsychology of starvation: Set-shifting, central coherence, perseveration, and persistence in a nonclinical sample. Unpublished clinical psychology doctoral thesis, Department of Clinical, Educational, and Health Psychology, University College London.
Pierobon, A., Giardini, A., Fanfulla, F., Callegari, S., & Majani, G. (2008). A multidimensional assessment of obese patients with obstructive sleep apnoea syndrome (OSAS): a study of psychological, neuropsychological and clinical relationships in a disabling multifaceted disease. Sleep Medicine, 9(8), 882–889.
Pignatti, R., Bertella, L., Albani, G., Mauro, A., Molinari, E., & Semenza, C. (2006). Decision-making in obesity: a study using the gambling task. Eating and Weight Disorders, 11(3), 126–132.
Reitan, R. (1958). Validity of the trail making test as an indicator of organic brain damage. Perceptual and Motor Skills, 8, 271–276.
Shallice, T. (1982). Specific impairments of planning. Philosophical Transactions of Royal Society London B: Biological Sciences, 298, 199–209.
Smith, P., Blumenthal, J., Babyak, M., Craighead, L., Welsh-Bohmer, K., Browndyke, J., et al. (2010). Effects of the dietary approaches to stop hypertension diet, exercise, and caloric restriction on neurocognition in overweight adults with high blood pressure. Hypertension, 55(6), 1331–1338.
Spitznagel, M., Garcia, S., Miller, L., Strain, G., Devlin, M., Wing, R. et al. (2011). Cognitive Function Predicts Weight Loss Following Bariatric Surgery. Surgery for Obesity and Related Diseases, 20, 1–7.
Spreen, O., & Strauss, E. (1998). A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary. Oxford: Oxford University Press.
Stuss, D. T., & Alexander, M. P. (2007). Is there a dysexecutive syndrome? Philosophical Transactions of the Royal Society B, 362, 901–915.
Svaldi, J., Brand, M., & Tuschen-Caffier, B. (2010). Decision-making impairments in women with binge eating disorder. Appetite, 54, 84–92.
Trenerry, M. R., Crosson, B., DeBoe, J., & Leber, W. R. (1989). The stroop neuropsychological screening test. Odessa: Psychological Assessment Resources.
Van den Berg, E., Kloppenborg, R., Kessels, R., Kappelle, L., & Biessels, G. (2009). Type 2 diabetes mellitus, hypertension, dyslipidemia and obesity: a systematic comparison of their impact on cognition. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1792(5), 470–481.
Van den Eynde, F., Guillaume, S., Broadbent, H., Stahl, D., Campbell, I., Schmidt, U. et al. (2011). Neurocognition in bulimic eating disorders: a systematic review. Acta Psychiatrica Scandinavica, 124, 120–140.
Verdejo-García, A., Pérez-Expósito, M., Schmidt-Río-Valle, J., Fernández-Serrano, M., Cruz, F., Pérez-García, M., et al. (2010). Selective alterations within executive functions in adolescents with excess weight. Obesity, 18, 1572–1578.
Volkow, N., Wang, G., Telang, F., Fowler, J., Goldstein, R., Alia-Klein, N., et al. (2008). Inverse association between BMI and prefrontal metabolic activity in healthy adults. Obesity, 17(1), 60–65.
Walsh, K. (1994). Neuropsychology: a clinical approach (3rd ed.). Edinburgh: Churchill Livingstone.
Wechsler, D. (1997). WAIS-III, WMS-III, technical manual. San Antonio: Psychological Corporation.
Weller, R. E., Cook, E. W., III, Avsar, K. B., & Cox, J. E. (2008). Obese women show greater delay discounting than healthy-weight women. Appetite, 51(3), 563–569.
Wilson, B., Alderman, N., Burgess, P., Emslie, H., & Evans, J. (1996). Behavioral assessment of the dysexecutive syndrome. Oxford: Thames Valley Test Company.
World Health Organisation (WHO) (2011) Global Database on Body Mass Index. Retrieved December 4, 2011, from http://apps.who.int/bmi/index.jsp
Zinzindohoue, F., Chevallier, J., Douard, R., Elian, N., Ferraz, J., Blanche, J., et al. (2003). Laparoscopic gastric banding: a minimally invasive surgical treatment for morbid obesity: prospective study of 500 consecutive patients. Annals of Surgery, 237(1), 1–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fitzpatrick, S., Gilbert, S. & Serpell, L. Systematic Review: Are Overweight and Obese Individuals Impaired on Behavioural Tasks of Executive Functioning?. Neuropsychol Rev 23, 138–156 (2013). https://doi.org/10.1007/s11065-013-9224-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-013-9224-7