
Abstract
Over the past 5 years, Diffusion Tensor Imaging (DTI) has begun to provide new evidence about the effects of prenatal alcohol exposure on white matter development. DTI, which examines microstructural tissue integrity, is sensitive to more subtle white matter abnormalities than traditional volumetric MRI methods. Thus far, the available DTI data suggest that white matter microstructural abnormalities fall on a continuum of severity in Fetal Alcohol Spectrum Disorder (FASD). Abnormalities are prominent in the corpus callosum, but also evident in major anterior-posterior fiber bundles, corticospinal tracts, and cerebellum. These subtle abnormalities are correlated with neurocognitive deficits, especially in processing speed, non-verbal ability, and executive functioning. Future studies using larger samples, increasingly sophisticated DTI methods, and additional functional MRI connectivity measures will better characterize the full range of abnormalities in FASD. Ultimately, these measures may serve as indices of change in future longitudinal studies and in studies of interventions for FASD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the past 5 years, a series of brain imaging studies using Diffusion Tensor Imaging (DTI) has broadened our understanding of the neurodevelopmental effects of prenatal alcohol exposure. It has been known for some time that prenatal alcohol exposure is associated with serious cognitive consequences including low IQ, attention and executive functioning deficits, memory impairments, visual-spatial abnormalities, and fine motor deficits among others (Mattson and Riley 1998) (also see review in this same edition). Earlier neuroimaging studies demonstrated that gross structural brain anomalies were common in Fetal Alcohol Syndrome (FAS), a diagnosis with an incidence of about 1 in 1,000 (Abel 1995) that is made on the basis of heavy prenatal alcohol exposure, growth deficiency, dysmorphic facial features, and significant cognitive impairment. DTI may be uniquely suited to the study of a broader range of effects due to prenatal alcohol exposure known as Fetal Alcohol Spectrum Disorder (FASD) (incidence ≈ 1 in 100) (Sampson et al. 1997) because it is non-invasive, it is sensitive to normal brain development, and it provides measures of tissue organization and integrity at a microscopic level not achievable with conventional volumetric MRI methods.
Thus far, despite differences in populations and methodologies across studies, DTI studies have provided relatively consistent results in major white matter tracts, including the corpus callosum, in FASD. The findings demonstrate that subtle white matter disruption may be an important neurodevelopmental component of FASD and highlight the need for a more complete understanding of the cognitive consequences of white matter disturbance during brain development.
A Brief Overview of DTI Methods
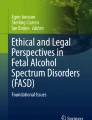
DTI is a Magnetic Resonance Imaging (MRI) technique that measures the diffusion of water molecules in tissue (Le Bihan 1995; Stejskal and Tanner 1965). Molecules that are unrestricted by tissue structure diffuse via Brownian motion in an isotropic manner—equally in all planes (see Fig. 1). In tissue, the orientation of the diffusion is often differentially restricted, such as by cell membranes, fibers, and myelin (Moseley et al. 1990). For example, in white matter, the diffusion occurs more readily parallel to the axons rather than perpendicular to the axons. This orientation-specific diffusion is called anisotropic (Beaulieu 2002).

The panel on the left illustrates isotropic diffusion which is equal in all orientations. Diffusion is more isotropic in tissue that contains few or no restrictions. The panel on the right illustrates anisotropic diffusion which is orientation-specific. Diffusion is more anisotropic in structured tissue such as white matter fiber bundles (illustrated)
DTI measures the orientation and magnitude of diffusion in three dimensions and subsequently reconstructs the data into a three-dimensional volume, (Basser et al. 1994b), allowing for mapping of white matter structure as well as measurement of tissue “integrity” on a voxel-by-voxel level. The tensor in DTI simply refers to a mathematical construct for representing the magnitude of water diffusion in three-dimensional space (Basser and Pierpaoli 1996).
Following data acquisition, a diffusion tensor matrix is constructed and matrix diagonalization is used to compute three eigenvectors (Basser and Pierpaoli 1998). Scalar measures are derived from the eigenvectors. The sum total of the three eigenvalues (λ1 + λ2 + λ3) is the defined as the trace of the diffusion tensor. The average of the three eigenvalues is the mean diffusivity (MD). In white matter, the first and largest of the eigenvalues, λ1, represents diffusivity parallel to the axons and is referred to as the axial diffusivity (Basser 1995) or parallel diffusivity. Similarly, the second and third eigenvalues, λ2 and λ3, represent diffusivity in the planes orthogonal to the axons and are usually averaged (λ2 + λ3)/2, resulting in a measure of radial diffusivity or perpendicular diffusivity. The most commonly reported measure, fractional anisotropy (FA), represents the fraction tensor’s magnitude that is due to anisotropic diffusion (Basser et al. 1994a; Masutani et al. 2003). Abnormal brain development or acquired brain damage typically contributes to lower FA and higher MD values in affected white matter compared with normal white matter (Neil et al. 2002). Fig. 2. contains examples of fractional anisotropy maps, color-coded to show the orientation of major white matter fiber bundles.

The first column illustrates raw diffusion-weighted images with diffusion weighting applied in “X” (left-right), “Y”(anterior-posterior), and “Z” (superior-inferior) planes. Signal attenuation (dark regions) is the result of water diffusion in the plane of the diffusion encoding gradient. The second column shows fractional anisotropy (FA) maps at the same slices. The third column shows diffusion encoded color maps, where red indicates diffusion in “X”, green indicates diffusion in “Y”, blue indicates diffusion in “Z”, and combinations of the colors indicates diffusion in combinations of “X”, “Y”, and/or “Z”. Yellow boxes highlight structures within each image to illustrate signal attenuation in the diffusion images and the corresponding color encoding in the diffusion encoded color maps
Currently, the physiological meaning of DTI measures such as FA and MD is not yet fully understood (for a review, see (Beaulieu 2009)). With the recent publication of numerous DTI studies, it has now become clear that DTI does not measure a single characteristic of white matter development or integrity. Rather, DTI reflects underlying aspects of tissue organization at numerous levels (Neil, et al. 2002). Although DTI is often thought to predominantly reflect myelin status, it is clear that DTI is sensitive to several aspects of axonal integrity as well as the general organization and alignment of groups of axons and fibers in white matter tissue (Beaulieu 2002; Neil, et al. 2002). Thus, although DTI is sensitive to the type of damage caused by prenatal alcohol exposure, it seems unlikely that DTI by itself will be able to substantially increase our understanding of the actual physiological mechanisms of alcohol damage in the brain.
In addition, as a further caveat in understanding the strengths and limitations of DTI, a detailed example illustrating the scale of the measurements is worthwhile (Wozniak et al. 2008): Free water molecules diffuse an average of 10 μm during a typical diffusion encoding sequence (Le Bihan 2003; Mori and Zhang 2006). Axons in the corpus callosum have a median diameter of about 1 μm with a range of 0.2 to 10 μm (Aboitiz et al. 1992). The actual spatial resolution of the DTI image is many orders of magnitude larger than the scale of the individual axon. For example, a common DTI voxel (a single three-dimensional ‘volume pixel’ in the image) is 2.5 × 2.5 × 2.5 mm, or 2500 μm per side and 6.25 million square microns in cross-section. Thus, the measured diffusion in a single corpus callosum voxel is the result of millions of axons that pass through that single voxel. Even at 1.0 × 1.0 × 1.0 mm, there are still approximately one million axons passing through the voxel. Therefore, despite the impressive images that DTI produces and the fact that it measures aspects of microstructural integrity, DTI remains a relatively blunt tool in our investigation of the brain.
Lastly, despite the proliferation of DTI papers and software tools, DTI remains a highly technically challenging methodology with many opportunities for errors and biases along the complex path from data acquisition to processing to final analysis. For a comprehensive discussion of these issues, the interested reader is referred to an excellent paper on the many potential pitfalls inherent to DTI methods (Jones and Cercignani 2010).
Nonetheless, with a clear understanding of the limitations of the technique, it remains evident that DTI is a promising tool that has now become a staple in the investigation of a wide range of neurodevelopmental conditions (Alkonyi et al. 2010; Cykowski et al. 2010; Filippi et al. 2003; Groen et al. 2010; Kao et al. 2010; Kumar et al. 2010; Mullen et al. 2010; Radua et al. 2010; Shukla et al. 2010; Utsunomiya 2010; Wozniak et al. 2011b; Yoshida et al. 2010). Ultimately, DTI’s primary advantage lies in its sensitivity: to neurodevelopmental abnormalities, to normal developmental changes (reviewed below), to changes in disease status including progression and recovery (Teipel et al. 2010; Wu et al. 2010), and to the effects of both biological and behavioral treatments (Fox et al. 2010; Keller and Just 2009; Schweder et al. 2010; Trivedi et al. 2008). As we move into the era of new interventions for FASD, including micronutrient supplementation and others, the availability of sensitive, non-invasive measures of brain status—like DTI—will become increasingly important.
The Role of White Matter in the Brain: Context for DTI Studies of FASD
Cerebral white matter is made up of three major types of fibers: commissural fibers (including the corpus callosum, anterior and posterior commissures, and hippocampal commissure) that connect corresponding regions in the right and left hemispheres; association fibers that connect regions within the same hemisphere, locally across long distances; and projection fibers that connect cortex to deep gray matter structures. White matter’s appearance is largely due to myelin, the fatty layer that surrounds axons. Myelination of axons is essential for efficient neural transmission. Myelination unfolds as part of an orderly developmental sequence: posterior regions are myelinated prior to anterior regions (Barkovich et al. 1988; Hayakawa et al. 1991; Kinney et al. 1988). In the cerebrum, myelination occurs rapidly and broadly during the prenatal period and into the second year of life; it continues more slowly into adolescence and young adulthood (Holland et al. 1986). Long fibers, including those that bridge the two hemispheres, are myelinated first, followed by the shorter inter-cortical associational neurons (Yakolev and Lecours 1967). The final stages of myelination occur in the frontal lobes during adolescence, accompanied by significant cognitive growth, especially in executive functioning.
Although historically white matter has been thought to be primarily important for motor and sensory functioning, more recent conceptualizations suggest that white matter’s principal role may be to serve as the infrastructure of the brain’s neural networks. Thus, white matter is critical for complex high-level cognitive processes involving attention, executive functioning, non-verbal/visual-spatial processing, and speed (Filley 1998; Geschwind 1965). Data from numerous studies of white matter diseases including Multiple Sclerosis (Rao 1995), toxic leukoencephalopathy (Filley and Kleinschmidt-DeMasters 2001), cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), and others (Pantoni and Garcia 1995) provide direct evidence that intact white matter is necessary for normal executive function, attention, processing speed, and motor skill (Sullivan and Pfefferbaum 2011). White matter integrity, as measured by DTI, has also been shown to be associated with working memory, processing speed, and attention in adults with alcoholism (Chanraud et al. 2010; Pfefferbaum et al. 2000). Processing speed deficits have also been associated with DTI abnormalities in children with shear-damaged white matter as a result of traumatic brain injury (TBI) (Wilde et al. 2006). Similarly, Wozniak et al. (2007) showed associations between DTI measures of white matter damage and both attention and executive functioning deficits in children with TBI. Thus, DTI appears to be sensitive to the kind of underlying brain damage that is known to contribute to the types of cognitive deficits frequently observed in FASD.
White Matter Macrostructure in FASD
Before the advent of DTI, a number of studies using macrostructural methods demonstrated white matter abnormalities in FASD. Riley et al. (1995) showed smaller corpus callosum area in prenatally-exposed individuals, even after correcting for smaller brain size. Archibald et al. (2001) reported white matter hypoplasia, especially in the parietal region, in subjects with histories of prenatal alcohol exposure. In a study using voxel-based morphometry, Sowell et al. reported lower white matter density in left posterior temporo-parietal cortex, a region that is connected inter-hemispherically by posterior callosal fibers (Sowell, Thompson, et al. 2001). In another study, Sowell et al. did not observe lower callosal area after adjusting for brain size, but did report highly significant alterations in callosal shape in prenatally-exposed subjects (Sowell, Mattson, et al. 2001). Specifically, they reported displacement of the callosum, primarily in the posterior regions (isthmus and splenium). Moderate correlations were observed between callosal shape abnormalities and performance on cognitive measures, including a verbal learning measure. Callosal shape abnormalities have also been reported in FAS and Fetal Alcohol Effects (FAE) in a series of studies (Bookstein et al. 2002a; b; Bookstein et al. 2001. Bookstein et al. (2002a; b) also demonstrated relationships between callosal shape disruption and cognition. Specifically, they reported that higher callosal thickness was associated with executive functioning deficits whereas lower callosal thickness was associated with motor abnormalities. A significant relationship between callosal volume and performance on a finger localization task (which is dependent on callosal transfer) has also been shown in FASD (Roebuck et al. 2002). Slower inter-hemispheric transfer of information was associated with lower callosal volume. Overall, the evidence for macrostructural abnormalities in FASD, especially in the more severe forms such as FAS, led to the search for more subtle microstructural abnormalities across the full spectrum using methods such as DTI.
DTI Findings in Fetal Alcohol Spectrum Disorders: The First 5 Years
The first DTI study of FASD (Ma et al. 2005) examined adults (ages 18–25) with FAS. The study involved measurements of fractional anisotropy (FA) and apparent diffusion coefficient (ADC) (also called Mean Diffusivity (MD)) from hand-drawn regions of interest (ROIs) in the genu and splenium of the corpus callosum at the mid-sagittal slice. Lower FA and higher MD were found in both ROIs for the FAS group compared with controls, suggesting microstructural abnormalities in the alcohol-exposed brains. No correlations between DTI measures and facial dysmorphia were observed. Although higher FA in the genu was correlated with faster processing speed in controls, there was no significant correlation in the FASD group. The correlations between FA measures and full-scale IQ were not significant in either group.
Wozniak et al. (2006) examined children with mild to moderate severity FASD (none had FAS), ages 10 to 13, using DTI and found predominantly posterior corpus callosum abnormalities among six midline ROIs that were examined (Fig. 3). Specifically, higher MD was seen in the isthmus region for children with FASD compared with control subjects. None of the DTI metrics was found to be associated with the degree of facial dysmorphology.

Locations of six regions of interest (ROIs) placed in corpus callosum illustrated on a T1-weighted anatomical image (reprinted from Wozniak et al. 2006 with permission)
Using a voxel-wise approach, Sowell et al. (2008) found lower FA in children with FASD (ages 7 to 15). Lower FA was seen in several regions including the right and left lateral aspects of the splenium, although not at the midline (primarily in superior parietal regions). In that study, lower FA in the lateral splenium was associated with lower performance on a measure of visuomotor skill among the children with FASD. Other regions in which the FASD group showed lower FA included bilateral posterior cingulate, right temporal lobe (inferior longitudinal fasciculus and inferior fronto-occipital fasciculus), right internal capsule, and brainstem. No significant relationship between reading ability and white matter status was observed.
Lebel et al. (2008) used a semi-automated DTI tractography method in children with FASD (ages 5 to 12). Compared with controls, the FASD group had lower FA in the splenium tract and lower MD for the tract involving the genu. The finding of lower MD in the genu among those with FASD is noteworthy because lower MD is thought to reflect a higher degree of fiber coherence/organization and this finding contrasted the Ma et al. (2005) study. Group differences in DTI measures were also seen in a number of other white matter and grey matter regions including bilateral inferior and superior longitudinal fasciculi, right cingulum, bilateral globus pallidus, and left thalamus. In this study, no significant correlations were observed between the DTI metrics and measures of executive functioning, working memory, reading, vocabulary, or mathematical ability.
Fryer et al. (2009) examined white matter in a group of children (ages 8 to 18) with heavy prenatal alcohol exposure compared with controls using Tract-Based Spatial Statistics (TBSS) (Smith et al. 2006), a voxel-wise method that focuses on central white matter voxels in order to minimize the effects of inter-subject registration problems. They reported lower FA in a significant number of white matter tracts including right superior longitudinal, uncinate, and fronto-occipital fasciculi, bilateral anterior/superior corona radiata, bilateral posterior corona radiata, and bilateral forceps major. The abnormalities were most prominent in the medial regions of frontal and occipital lobes. They also observed low FA in the body of the corpus callosum. Although FA in each of these white matter regions distinguished the FASD group from controls, only FA in the body of the callosum distinguished those with FAS from those with prenatal exposure to alcohol (PEA). Thus, DTI measures in midline structures, such as the corpus callosum, may reflect severity and, perhaps the extent of the alcohol exposure. Despite a preponderance of regions that showed lower FA in subjects with alcohol exposure relative to control subjects, there were some regions—including the right cingulum and right posterior limb of the internal capsule—in which the opposite (higher FA) was observed in the alcohol-exposed group. These somewhat counterintuitive findings and those of Lebel cited above should be evaluated in the context of evidence that higher than normal FA and lower than normal MD could be indicative of pathology such as damage to regions of crossed fibers (which normally have very low FA and high MD) for example. Alternatively, such findings could be related to other developmental insults that commonly co-occur with FASD. For example, high FA and low MD have been seen in samples of individuals with prenatal exposure to tobacco and other drugs, as discussed in detail in a section below.
In another study employing a TBSS examination of the corpus callosum among adults with FASD (ages 19 to 27), Li et al. (2009) reported lower FA, higher MD, and higher radial diffusivity (RD) in the isthmus for individuals with dysmorphic facial features compared with controls. Significant group differences in FA were also seen in the splenium. These abnormalities were at the midline but they also extended into the lateral callosal fibers (see Fig. 4). There were no statistically significant differences between the FASD group without dysmorphic facial features and controls, but the FA, MD, and radial diffusivity (RD) values fell between the other two groups, suggesting a continuum of effects. Correlations between the DTI measures and full-scale IQ as well as facial dysmorphia ratings were non-significant.

The results of TBSS analysis among the CONT, DYSM and ETOH groups. (a) The schematic of the positions of the selected volume shown in (b); the yellow arrow shows the order of the axial slices starting from upper left corner of (b); (b) FA difference maps (red) superimposed on the mean FA skeletons (green, thresholded at FA > 0.3) of the 82 subjects between CONT and DYSM group pair. The isthmus and the lateral branches of the isthmus part of the corpus callosum in DYSM group showed significantly lower FA values than these of the control group (cluster-wise, pFWE <0.05); (c) 3D rendering of the FA difference maps (red) superimposed on the mean FA skeletons (green, thresholded at FA > 0.3) (cluster-wise pFWE < 0.05) (reprinted with permission from Li et al. 2009)
In a study utilizing DTI tractography, Wozniak et al. (2009) examined the integrity of corpus callosum tracts at the midline and extending into the cerebral hemispheres in children with FASD (ages 10 to 17) (see Fig. 5). FA in the inter-hemispheric fibers of the posterior midbody, isthmus, and splenium of the corpus callosum was significantly lower in the FASD group compared with controls. No significant correlation was found between the DTI measures of white matter integrity and facial dysmorphology. In the FASD group, a significant correlation was observed between the Wechsler Working Memory Index and FA in the genu but not FA in the splenium. Similarly, significant correlations were seen between MD in the splenium and both the Working Memory and Perceptual Organizational indices. There were no associations between Perceptual Organization and the DTI measures in the genu. Although the findings do not represent a double dissociation, they do indicate a degree of regional specificity.

Six inter-hemispheric connectivity distribution masks (tracts) generated by tractography: (anterior to posterior) 1. genu; 2. rostral body; 3. anterior mid-body; 4. posterior mid-body; 5. isthmus; 6. Splenium (reprinted from Wozniak et al. 2009) with permission)
Most recently, Lebel et al. (2010) used a voxel-wise approach to examine relationships between white matter DTI measures and math ability in a sample of children with FASD (ages 5 to 13). They observed significant associations between FA and math ability in the left cerebellum, left parietal lobe, and bilateral brainstem after controlling for age. Fiber tracking revealed that the significant parietal clusters were part of the superior longitudinal fasciculus, a tract known to be related to overall cognitive functioning and to math ability in particular.
As an illustration of the relative consistency of DTI evidence of white matter abnormalities in individuals with FASD thus far, Table 1 provides a summary of findings specifically highlighting the corpus callosum. For purposes of comparison, we computed Cohen’s d effect sizes for the studies that used defined ROIs. Variability in findings across studies may be related to differences in age, diagnosis, severity, sample size, and DTI methodology. As would be expected, the largest group effect sizes come from the study of the most severely affected population, those with FAS and mean IQ = 58 (Ma, et al. 2005), but moderate effects are also evident in less severely affected individuals on the FASD spectrum. Looking across studies, it is apparent that microstructural abnormalities occur throughout the corpus callosum (as well as elsewhere in the brain) but are most consistently seen in the posterior regions of the callosum – especially in the isthmus and splenium. In evaluating the various methods of data analysis used in these studies, it is apparent that ROI-based methods have significant power to discriminate groups, voxel-wise analyses are useful for characterizing the extent of the effects across the whole brain, and tractography methods are essential in moving forward to better understand the specific functional implications of these structural effects. Overall, these studies consistently demonstrate that DTI is sensitive to white matter abnormalities in FASD, including those who do not meet full criteria for FAS.
Importantly, the consistent findings of specific abnormalities in the posterior portion of the corpus callosum highlight the fact that white matter tracts such as the corpus callosum are complex and heterogeneous. Corpus callosum projections are known to be regionally specific (Innocenti 1986). Anterior portions of the callosum, including the genu and rostrum, project mostly to caudal, orbital, and inferior prefrontal regions. Anterior midbody regions project to pre-motor and motor regions, while posterior midbody regions, including the isthmus, project to posterior parietal and superior temporal regions. The splenium projects widely to inferior temporal, occipital, superior temporal and posterior parietal cortices. In addition, the microstructure of the corpus callosum also varies significantly, with proportionally more high density, small-diameter fibers in the genu and more large-diameter fibers in the midbody, as seen by light microscopy (Aboitiz, et al. 1992). Figure 6 dramatically illustrates the regionally-specific corpus callosum abnormalities in a child with FASD compared with a same-age control. The fiber tracking suggests significant abnormalities in tracts that would normally project through the posterior midbody and isthmus regions into parietal and temporal cortices. Interestingly, although the callosum is clearly malformed in the posterior region, the splenium is present and its fibers clearly project to the occipital cortex.

Inter-hemispheric fiber tracking through the corpus callosum in a 12 year-old boy with partial FAS and gross structural abnormalities including partial agenesis of the corpus callosum (left panel) compared with a non-exposed 12 year-old male control subject (right panel). The top panels are DTI tractography images overlaid on fractional anisotropy maps. The bottom panels are T1-weighted anatomical images. Tractography images were generated using the Diffusion Toolkit (http://trackvis.org/dtk)
Ultimately, as research moves forward in FASD, it will be important to begin to understand the relationships between the initial effects of alcohol on white matter tissue, the interaction of specific exposure timing and an unfolding developmental process, and the differential sensitivity of the measures at various points in bran development. It is likely that large DTI datasets will be necessary to explore these specific issues in FASD at the necessary level of detail.
Context: DTI in the Developing Brain
The majority of DTI studies of FASD thus far have been done in childhood—a period during which the brain is changing in ways that are reflected in the DTI measures themselves. Fortunately, in FASD (and in many other neurodevelopmental disorders), DTI measures are proving to be very sensitive to underlying abnormalities in tissue integrity despite the “moving target” of predictable changes that occur with normal development (Gao et al. 2008; Hasan et al. 2008; Hermoye et al. 2006; Huang et al. 2006; Qiu et al. 2008). Understanding normative white matter development is essential in gaining further insight into abnormalities that occur in FASD. Characterizing the maturational processes fully, especially using tools such as DTI, will ultimately guide future studies of FASD. Over the last few years, the application of DTI to the study of normal brain development has steadily increased, with over 30 published reports at present. Here, we will briefly highlight the literature that has thus far characterized the development of white matter in healthy children and adolescents using DTI. For a more detailed report, Schmithorst and Yuan (2009) have compiled a thoughtful review of the literature on DTI and adolescent brain development.
Of particular relevance to FASD, some studies of development have explicitly examined the development of the corpus callosum using both region of interest (ROI) and fiber tractography analyses (Bonekamp et al. 2007; Hasan et al. 2009; Hasan, et al. 2008; Lebel et al. 2008; Muetzel et al. 2008). Other studies have reported DTI associations with age in the callosum using whole-brain voxel-wise analyses (Barnea-Goraly et al. 2005; Giorgio et al. 2010; Giorgio et al. 2008). In general, these studies have shown regionally-dependent associations between age and DTI metrics. Specifically, there is evidence indicating that mid-callosal and posterior callosal regions (e.g., the body and splenium) mature later in life compared with anterior regions (e.g., the genu). Just as the cortex follows a particular spatial pattern of development, these data suggest the callosum may follow an anterior-to-posterior gradient in terms of maturation. As described earlier in this review, depending on the diffusion metric used, these data could potentially reflect the differences in myelin, axonal caliber and packing, or other processes (Beaulieu 2009; Paus 2009). Some studies have also reported within-subject, regional differences in diffusion metrics in the callosum and its inter-hemispheric connections. For example, there is evidence suggesting that posterior regions have significantly higher FA compared with anterior regions (Hasan, et al. 2009). The normative data presented in these published studies have the potential to assist future FASD studies by allowing for adjustment for developmental trends and other region-specific variability.
Because FASD is associated with midline physical dysmorphia, neurocognitive impairment, and gross structural midline brain anomalies (e.g., callosal agenesis), the corpus callosum has been the subject of the majority of DTI reports on FASD. However, it is clear that there are abnormalities in other brain regions in individuals with FASD. In healthy individuals, studies examining large fiber bundles using DTI tractography—including the cingulum bundle, cortico-spinal tract, inferior longitudinal fasciculus, superior longitudinal fasciculus, and the uncinate fasciculus—have demonstrated continued maturation throughout the brain (Eluvathingal et al. 2007; Giorgio et al. 2010; Lebel, Rasmussen, et al. 2008). As in the callosum, the developmental timing of white matter maturity throughout the brain has been shown to be regionally dependent. For example, the fornix appears to be fully developed by age 5, whereas the inferior longitudinal fasciculus attains 90% of its maximum FA value by age 11 (Lebel, Rasmussen, et al. 2008). Some structures, including the fronto-temporal connections of the uncinate fasiculus and the cingulum bundle, do not reach this plateau until after age 25 (Lebel, Rasmussen, et al. 2008). Because both linear and nonlinear associations between DTI white matter measures and age have been described, it remains critical to consider the age range of the sample and the handling of age as a matching variable/co-variate when evaluating the results of DTI studies in FASD.
Context: DTI in Other Prenatal Exposures
Many individuals who have been exposed to alcohol prenatally were also exposed to other drugs of abuse (Della Grotta et al. 2010; Perham-Hester and Gessner 1997). The DTI literature examining individuals with prenatal exposure to substances other than alcohol is still in its infancy. Although the underlying mechanisms contributing to disruptions in white matter development following prenatal exposure to other substances are likely to be distinct from the mechanisms of damage caused by prenatal alcohol exposure, the careful characterization of these deficits using DTI is relevant to the understanding of alcohol effects in the case of FASD. In one study of non-exposed controls (ages 8-to-14) and children whose mothers were polysubstance abusers (primarily opiates), Walhovd et al. (2010) used DTI with a whole-brain voxel-wise approach. They reported significantly lower FA in the exposed children in central, inferior and posterior white matter (i.e., occipital and temporal lobes). These effects remained significant, even after controlling for age and sex. It was found that most of the difference in FA between groups was driven by higher radial diffusion in the exposed children. In terms of associations between white matter microstructure and cognition, the authors reported a positive correlation between Freedom from Distractibility (a measure of working memory) and FA in the temporal lobe, indicating better performance is associated with higher FA. As part of a prospective longitudinal study, Warner and colleagues (2006) used DTI to study children (ages 10 to 12) with prenatal cocaine exposure and compared them with well-matched non-exposed controls. Neurocognitive assessments focusing on executive functioning were also administered. The study found higher MD in frontal ROIs among exposed children compared with non-exposed controls. One of the ROIs consisted of inter-hemispheric projections of the corpus callosum. Interestingly, only MD was found to be different between groups; FA was not significantly different. The authors also reported an interaction between cocaine exposure and marijuana exposure, such that children exposed prenatally to both substances had the highest MD values in frontal white matter. Task performance on the Stroop and Trail Making Task (both measures of executive functioning) correlated with FA in frontal white matter—with better performance corresponding to higher FA.
As described previously, lower FA and higher MD are suggestive of underlying pathology. However, some studies have reported the opposite effect in prenatal substance exposure. Jacobsen et al. (2007) examined the following four groups of children (ages 10 to 18): 1) prenatal exposure to tobacco smoke and current smoker; 2) prenatal exposure to tobacco smoke and current non-smoker; 3) no prenatal exposure and current smoker; and 4) no prenatal exposure and current non-smoker. They used a voxel-wise approach and found higher FA in the genu of the corpus callosum and in frontal white matter in those individuals exposed to tobacco prenatally, compared with the un-exposed. Current smoking exacerbated these effects in exposed children with additional regions showing abnormalities, including the corpus callosum and associated inter-hemispheric fibers, frontal white matter, and internal capsule. Interestingly, the number of weeks of exposure to tobacco prenatally was not significantly related to FA, however amount of exposure during adolescence was—especially in the genu of the corpus callosum (those who smoked had higher FA). They also examined tasks assessing auditory attention and motor speed and found a significant positive correlation between reaction time on an auditory attention task and FA in the internal capsule, but only in the group of current smokers. This effect was not modulated by prenatal exposure, meaning only current smoking status contributed to the model. There were no significant correlations between motor ability and DTI measures. As another example, Cloak et al. (2009) evaluated young children, ages 3 to 4 years, with prenatal methamphetamine exposure. The study used an ROI analysis of DTI data and found lower ADC in multiple regions, particularly frontal and parietal lobes, among the exposed children. The authors also reported higher FA (at a trend-level) in frontal white matter of the exposed group. These results were contrary to the author’s hypotheses given the expected trends in DTI data with pathology and the findings reported in cocaine exposed children (Warner, et al. 2006).
Taken together, these data indicate that not all abnormalities measured by DTI methods are specific to prenatal alcohol exposure. Rather, DTI abnormalities likely reflect a wide range of negative effects during prenatal brain development. Because many children exposed to alcohol have also been exposed to tobacco and other substances during prenatal development, studies should account for these factors as much as possible in the sample description and in the data analysis. Despite the caveats raised by these potential confounding factors, it remains clear that the DTI effects seen in FASD are not due solely to the effects of confounding variables. Perhaps some of the most convincing evidence along these lines comes from emerging DTI data from controlled animal studies which clearly do show that alcohol exposure by itself is highly disruptive to the development of white matter (see O’Leary-Moore et al. (2011) in this edition).
Context: DTI Findings in ADHD
Another potential confound in studies of children with FASD is the frequent co-morbid diagnosis of attention-deficit/hyperactivity disorder (ADHD), a condition that is known to be associated with its own underlying neurodevelopmental abnormalities. The DTI literature on ADHD provides additional context in which to interpret DTI studies of FASD. Ashtari et al. (2005) examined children with ADHD and healthy controls (ages 7 to 11), using a voxel-wise analysis of DTI data. They reported lower FA in children with ADHD in the internal capsule, cerebral peduncle, cerebellar peduncle, and the pre-motor area. The effect of medication on DTI measures was also examined, and no relationship was observed. Ratings of inattention severity were negatively correlated with FA values in the cerebellum, where lower FA was associated with more severe inattention. Using an ROI approach, Hamilton et al. (2008) found lower FA in the corticospinal tract and the superior longitudinal fasciculus in male subjects (mean age = 12) with ADHD compared with controls. The study did not find a relationship between hyperactivity scores or medication status and FA. In another study of all boys (ages 11 to 16), Cao et al. (2010) conducted an ROI analysis of the corpus callosum. The authors found significantly lower FA in the isthmus of the corpus callosum in children with ADHD (a number of these boys also had co-morbid Oppositional Defiant Disorder and/or Conduct Disorder). In another study that examined all boys, Kobel et al. (2010) found lower FA in children with ADHD (ages 9 to 13) in the anterior corona radiata and middle cerebellar peduncle. Mean FA in left temporal-occipital white matter was actually found to be higher in children with ADHD. Finally, Davenport et al. (2010) studied children and young adults (ages 10 to 20) with ADHD and healthy controls. Contrary to other reports, the authors found higher FA in the anterior corona radiata in the ADHD group, compared with both healthy controls and another sub-sample of children with psychosis. However, children with ADHD did show lower FA in the fornix, when compared with healthy controls.
Managing the confound of co-morbid ADHD in studies of FASD is a significant challenge because the rates of ADHD among children with FASD are so high—reportedly as high as 41% to 94% (Bhatara et al. 2006; Fryer et al. 2007; Streissguth et al. 1994). It is worth noting that none of the DTI studies of ADHD cited above included any screening for potential pre-natal alcohol exposure (either through history or facial evaluation). Given the high incidence of pre-natal alcohol exposure in the general population and the presumed higher incidence in clinical populations, it seems possible and even likely that some children with unidentified prenatal alcohol exposure may be represented in these studies of ADHD.
Studies of other neurodevelopmental disorders further highlight the non-specific nature of the white matter abnormalities observed in FASD. In individuals with autism, similar corpus callosum abnormalities have been observed (Barnea-Goraly et al. 2004) and have been found to be associated with poor processing speed (Alexander et al. 2007). Children with developmental disabilities have been found to have lower FA and higher MD in the genu and splenium (Filippi, et al. 2003). Clearly, the interpretation of small studies of clinical populations (ADHD, autism-spectrum, FASD, other drug exposure, etc.) will continued to be hampered by confounding variables that can only be fully addressed by large-scale studies that incorporate comprehensive measures of potential confounds.
Future Directions: Incorporating New Measures of Functional Connectivity
DTI has provided us with a unique window into the fine details of structural connectivity in the brain—during development and also following insults to the developmental process such as those resulting from prenatal alcohol exposure. The next logical step is to incorporate measures of functional connectivity into future investigations. Modern functional connectivity studies take the approach of measuring brain activity with functional MRI across multiple brain regions during an awake period of rest/inactivity and then use correlational techniques to “map” networks in the brain based on levels of synchronized activity over time (Biswal et al. 1995). Using methods such as these, Raichle et al. (2001) and others have described a “default mode network” that is essentially a collection of brain regions that are “pulled together” as a functional circuit during periods of rest. The default mode network is specifically active during an eyes-closed, at-rest state and then shows decreased activity when the brain engages in an activity (Raichle and Snyder 2007). The examination of these types of networks using resting-state fMRI is thought to provide a measure of “intrinsic” brain activity—brain activity that is distinct from the brain response that occurs to extrinsic stimuli, such as during a task-based fMRI study. Brain activity during the resting state may reflect ongoing integration of information, consolidation of memories, maintenance of salient connections, and even preparation for action. The patterns of functional connectivity that are seen during rest are also a reflection of the underlying structural connectivity in the brain. For example, a loss of inter-hemispheric functional connectivity has been shown in cases of surgical severing of the corpus callosum (Johnston et al. 2008) and studies are now beginning to demonstrate strong relationships between resting functional connectivity measures and anatomical connectivity as defined by DTI maps (Skudlarski et al. 2008). For an extensive review of the effects of disrupted connectivity, the reader is referred to a special issue of Neuropsychology Review (Sullivan 2010).
Functional connectivity methods will likely prove very relevant to the study of developmental disorders including FASD. As the brain matures structurally, it’s ability to coordinate itself in real-time in the form of functional networks follows a developmental trajectory—as evidenced by stronger functional connectivity with increasing age in children (Fair et al. 2008). Functional connectivity studies are already beginning to shed light on developmental conditions such as autism and ADHD (Broyd et al. 2008; Greicius 2008; Uddin et al. 2008). Recently, Wozniak et al. (2011a) have demonstrated the applicability of functional connectivity measures to FASD and related these measures to the commonly observed microstructural abnormalities in posterior callosal regions. Using functional MRI (fMRI) during a resting state, they demonstrated abnormalities in inter-hemispheric functional connectivity, specifically in those cortical regions that are connected by posterior callosal fibers. Functional connectivity was lowest in the FASD group compared with controls (12.7% lower) for the right and left para-central regions. These regions are highly interconnected by posterior-midbody and isthmus callosal fibers—the same posterior callosal regions that have been found to be abnormal in a number of the published DTI studies (see Table 1). Across patients and controls, a trend-level association was seen between para-central functional connectivity and white matter integrity (MD) of the isthmus tract as measured by DTI. Future studies of FASD will be able to examine whole brain connectivity in greater detail, combining structural connectivity measures from DTI with functional connectivity measures from resting-state fMRI to better characterize the extent of the abnormalities in this population.
Conclusions
Although the existing body of work using DTI in the study of FASD is small, the available data clearly indicate that the method is sensitive to the underlying brain abnormalities in this condition. Furthermore, the data suggest that the microstructural abnormalities that can be detected are functionally significant—as indicated by correlation with neurocognitive functioning and with measures of functional connectivity. Although these small studies have thus far provided important insights into the effects of prenatal alcohol exposure on white matter development, it is clear that much larger studies will be needed in order to address the variability in results due to heterogeneity of the population, significant co-morbidity, and the need to understand differential effects across development. The availability of a normative DTI database, such in the form of a developmental white matter “atlas”, would go a long way toward advancing our understanding of DTI results in neurodevelopmental disorders such as FASD. The application of an atlas-based technique to individual children with cerebral palsy has recently been demonstrated (Faria et al. 2010). Ultimately, multi-center studies and other data-sharing arrangements involving data from large numbers of individuals with FASD will significantly advance our understanding of this condition.
References
Abel, E. L. (1995). An update on incidence of FAS: FAS is not an equal opportunity birth defect. Neurotoxicology and Teratology, 17(4), 437–443.
Aboitiz, F., Scheibel, A. B., Fisher, R. S., & Zaidel, E. (1992). Fiber composition of the human corpus callosum. Brain Research, 598(1–2), 143–153.
Alexander, A. L., Lee, J. E., Lazar, M., Boudos, R., DuBray, M. B., Oakes, T. R., et al. (2007). Diffusion tensor imaging of the corpus callosum in Autism. Neuroimage, 34(1), 61–73.
Alkonyi, B., Govindan, R. M., Chugani, H. T., Behen, M. E., Jeong, J. W., & Juhasz, C. (2010). Focal white matter abnormalities related to neurocognitive dysfunction: An objective diffusion tensor imaging study of children with Sturge-Weber syndrome. Pediatric Research.
Archibald, S. L., Fennema-Notestine, C., Gamst, A., Riley, E. P., Mattson, S. N., & Jernigan, T. L. (2001). Brain dysmorphology in individuals with severe prenatal alcohol exposure. Developmental Medicine and Child Neurology, 43(3), 148–154.
Ashtari, M., Kumra, S., Bhaskar, S. L., Clarke, T., Thaden, E., Cervellione, K. L., et al. (2005). Attention-deficit/hyperactivity disorder: a preliminary diffusion tensor imaging study. Biological Psychiatry, 57(5), 448–455.
Barkovich, A. J., Kjos, B. O., Jackson, D. E., Jr., & Norman, D. (1988). Normal maturation of the neonatal and infant brain: MR imaging at 1.5 T. Radiology, 166(1 Pt 1), 180–173.
Barnea-Goraly, N., Kwon, H., Menon, V., Eliez, S., Lotspeich, L., & Reiss, A. L. (2004). White matter structure in autism: preliminary evidence from diffusion tensor imaging. Biological Psychiatry, 55(3), 323–326.
Barnea-Goraly, N., Menon, V., Eckert, M., Tamm, L., Bammer, R., Karchemskiy, A., et al. (2005). White matter development during childhood and adolescence: a cross-sectional diffusion tensor imaging study. Cerebral Cortex, 15(12), 1848–1854.
Basser, P. J. (1995). Inferring microstructural features and the physiological state of tissues from diffusion-weighted images. NMR in Biomedicine, 8(7–8), 333–344.
Basser, P. J., Mattiello, J., & LeBihan, D. (1994a). Estimation of the effective self-diffusion tensor from the NMR spin echo. Journal of Magnetic Resonance. Series B, 103(3), 247–254.
Basser, P. J., Mattiello, J., & LeBihan, D. (1994b). MR diffusion tensor spectroscopy and imaging. Biophysical Journal, 66(1), 259–267.
Basser, P. J., & Pierpaoli, C. (1996). Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. Journal of Magnetic Resonance. Series B, 111(3), 209–219.
Basser, P. J., & Pierpaoli, C. (1998). A simplified method to measure the diffusion tensor from seven MR images. Magnetic Resonance in Medicine, 39(6), 928–934.
Beaulieu, C. (2002). The basis of anisotropic water diffusion in the nervous system—a technical review. NMR in Biomedicine, 15(7–8), 435–455.
Beaulieu, C. (2009). The biological basis of diffusion anisotropy. In H. B. Johansen-Berg & T. E. J. Behrens (Eds.), From quantitative measurement to in-vivo neuroanatomy. London: Academic.
Bhatara, V., Loudenberg, R., & Ellis, R. (2006). Association of attention deficit hyperactivity disorder and gestational alcohol exposure: an exploratory study. Journal of Attention Disorders, 9(3), 515–522.
Biswal, B., Yetkin, F. Z., Haughton, V. M., & Hyde, J. S. (1995). Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magnetic Resonance in Medicine, 34(4), 537–541.
Bonekamp, D., Nagae, L. M., Degaonkar, M., Matson, M., Abdalla, W. M., Barker, P. B., et al. (2007). Diffusion tensor imaging in children and adolescents: reproducibility, hemispheric, and age-related differences. Neuroimage, 34(2), 733–742.
Bookstein, F. L., Sampson, P. D., Connor, P. D., & Streissguth, A. P. (2002). Midline corpus callosum is a neuroanatomical focus of fetal alcohol damage. The Anatomical Record, 269(3), 162–174.
Bookstein, F. L., Sampson, P. D., Streissguth, A. P., & Connor, P. D. (2001). Geometric morphometrics of corpus callosum and subcortical structures in the fetal-alcohol-affected brain. Teratology, 64(1), 4–32.
Bookstein, F. L., Streissguth, A. P., Sampson, P. D., Connor, P. D., & Barr, H. M. (2002). Corpus callosum shape and neuropsychological deficits in adult males with heavy fetal alcohol exposure. Neuroimage, 15(1), 233–251.
Broyd, S. J., Demanuele, C., Debener, S., Helps, S. K., James, C. J., & Sonuga-Barke, E. J. (2008). Default-mode brain dysfunction in mental disorders: a systematic review. Neuroscience and Biobehavioral Reviews, 33(3), 279–296.
Cao, Q., Sun, L., Gong, G., Lv, Y., Cao, X., Shuai, L., et al. (2010). The macrostructural and microstructural abnormalities of corpus callosum in children with attention deficit/hyperactivity disorder: a combined morphometric and diffusion tensor MRI study. Brain Research, 1310, 172–180.
Chanraud, S., Zahr, N., Sullivan, E. V., & Pfefferbaum, A. (2010). MR diffusion tensor imaging: a window into white matter integrity of the working brain. Neuropsychology Review, 20(2), 209–225.
Cloak, C. C., Ernst, T., Fujii, L., Hedemark, B., & Chang, L. (2009). Lower diffusion in white matter of children with prenatal methamphetamine exposure. Neurology, 72(24), 2068–2075.
Cykowski, M. D., Fox, P. T., Ingham, R. J., Ingham, J. C., & Robin, D. A. (2010). A study of the reproducibility and etiology of diffusion anisotropy differences in developmental stuttering: a potential role for impaired myelination. Neuroimage, 52(4), 1495–1504.
Davenport, N. D., Karatekin, C., White, T., & Lim, K. O. (2010). Differential fractional anisotropy abnormalities in adolescents with ADHD or schizophrenia. Psychiatry Research, 181(3), 193–198.
Della Grotta, S., LaGasse, L. L., Arria, A. M., Derauf, C., Grant, P., Smith, L. M., et al. (2010). Patterns of methamphetamine use during pregnancy: results from the Infant Development, Environment, and Lifestyle (IDEAL) Study. Maternal and Child Health Journal, 14(4), 519–527.
Eluvathingal, T. J., Hasan, K. M., Kramer, L., Fletcher, J. M., & Ewing-Cobbs, L. (2007). Quantitative diffusion tensor tractography of association and projection fibers in normally developing children and adolescents. Cerebral Cortex, 17(12), 2760–2768.
Fair, D. A., Cohen, A. L., Dosenbach, N. U., Church, J. A., Miezin, F. M., Barch, D. M., et al. (2008). The maturing architecture of the brain's default network. Proceedings of the National Academy of Sciences of the United States of America, 105(10), 4028–4032.
Faria, A. V., Hoon, A., Stashinko, E., Li, X., Jiang, H., Mashayekh, A., et al. (2010). Quantitative analysis of brain pathology based on MRI and brain atlases-Applications for cerebral palsy. Neuroimage.
Filippi, C. G., Lin, D. D., Tsiouris, A. J., Watts, R., Packard, A. M., Heier, L. A., et al. (2003). Diffusion-tensor MR imaging in children with developmental delay: preliminary findings. Radiology, 229(1), 44–50.
Filley, C. M. (1998). The behavioral neurology of cerebral white matter. Neurology, 50(6), 1535–1540.
Filley, C. M., & Kleinschmidt-DeMasters, B. K. (2001). Toxic leukoencephalopathy. The New England Journal of Medicine, 345(6), 425–432.
Fox, R. J., Cronin, T., Lin, J., Wang, X., Sakaie, K., Ontaneda, D., et al. (2010). Measuring Myelin Repair and Axonal Loss with Diffusion Tensor Imaging. AJNR. American Journal of Neuroradiology.
Fryer, S. L., McGee, C. L., Matt, G. E., Riley, E. P., & Mattson, S. N. (2007). Evaluation of psychopathological conditions in children with heavy prenatal alcohol exposure. Pediatrics, 119(3), e733–741.
Fryer, S. L., Schweinsburg, B. C., Bjorkquist, O. A., Frank, L. R., Mattson, S. N., Spadoni, A. D., et al. (2009). Characterization of white matter microstructure in fetal alcohol spectrum disorders. Alcoholism, Clinical and Experimental Research, 33(3), 1–8.
Gao, W., Lin, W., Chen, Y., Gerig, G., Smith, J. K., Jewells, V., et al. (2008). Temporal and spatial development of axonal maturation and myelination of white matter in the developing brain. AJNR. American Journal of Neuroradiology, 30(2), 290–296.
Geschwind, N. (1965). Disconnexion syndromes in animals and man. I. Brain, 88(2), 237–294.
Giorgio, A., Watkins, K. E., Chadwick, M., James, S., Winmill, L., Douaud, G., et al. (2010). Longitudinal changes in grey and white matter during adolescence. Neuroimage, 49(1), 94–103.
Giorgio, A., Watkins, K. E., Douaud, G., James, A. C., James, S., De Stefano, N., et al. (2008). Changes in white matter microstructure during adolescence. Neuroimage, 39(1), 52–61.
Greicius, M. (2008). Resting-state functional connectivity in neuropsychiatric disorders. Current Opinion in Neurology, 21(4), 424–430.
Groen, W. B., Buitelaar, J. K., van der Gaag, R. J., & Zwiers, M. P. (2010). Pervasive microstructural abnormalities in autism: a DTI study. Journal of Psychiatry and Neuroscience.
Hamilton, L. S., Levitt, J. G., O'Neill, J., Alger, J. R., Luders, E., Phillips, O. R., et al. (2008). Reduced white matter integrity in attention-deficit hyperactivity disorder. NeuroReport, 19(17), 1705–1708.
Hasan, K. M., Kamali, A., Iftikhar, A., Kramer, L. A., Papanicolaou, A. C., Fletcher, J. M., et al. (2009). Diffusion tensor tractography quantification of the human corpus callosum fiber pathways across the lifespan. Brain Research, 1249, 91–100.
Hasan, K. M., Kamali, A., Kramer, L. A., Papnicolaou, A. C., Fletcher, J. M., & Ewing-Cobbs, L. (2008). Diffusion tensor quantification of the human midsagittal corpus callosum subdivisions across the lifespan. Brain Research, 1227, 52–67.
Hayakawa, K., Konishi, Y., Kuriyama, M., Konishi, K., & Matsuda, T. (1991). Normal brain maturation in MRI. European Journal of Radiology, 12(3), 208–215.
Hermoye, L., Saint-Martin, C., Cosnard, G., Lee, S. K., Kim, J., Nassogne, M. C., et al. (2006). Pediatric diffusion tensor imaging: normal database and observation of the white matter maturation in early childhood. Neuroimage, 29(2), 493–504.
Holland, B. A., Haas, D. K., Norman, D., Brant-Zawadzki, M., & Newton, T. H. (1986). MRI of normal brain maturation. AJNR. American Journal of Neuroradiology, 7(2), 201–208.
Huang, H., Zhang, J., Wakana, S., Zhang, W., Ren, T., Richards, L. J., et al. (2006). White and gray matter development in human fetal, newborn and pediatric brains. Neuroimage, 33(1), 27–38.
Innocenti, G. M. (1986). General ogranization of callosal connections in cerebral cortex. In E. G. Jones (Ed.), Cerebral cortex (pp. 291–354). New York: Plenum.
Jacobsen, L. K., Picciotto, M. R., Heath, C. J., Frost, S. J., Tsou, K. A., Dwan, R. A., et al. (2007). Prenatal and adolescent exposure to tobacco smoke modulates the development of white matter microstructure. The Journal of Neuroscience, 27(49), 13491–13498.
Johnston, J. M., Vaishnavi, S. N., Smyth, M. D., Zhang, D., He, B. J., Zempel, J. M., et al. (2008). Loss of resting interhemispheric functional connectivity after complete section of the corpus callosum. The Journal of Neuroscience, 28(25), 6453–6458.
Jones, D. K., & Cercignani, M. (2010). Twenty-five pitfalls in the analysis of diffusion MRI data. NMR in Biomedicine, 23(7), 803–820.
Kao, Y. C., Peng, S. S., Weng, W. C., Lin, M. I., & Lee, W. T. (2010). Evaluation of White Matter Changes in Agyria-Pachygyria Complex Using Diffusion Tensor Imaging. Journal of Child Neurology.
Keller, T. A., & Just, M. A. (2009). Altering cortical connectivity: remediation-induced changes in the white matter of poor readers. Neuron, 64(5), 624–631.
Kinney, H. C., Brody, B. A., Kloman, A. S., & Gilles, F. H. (1988). Sequence of central nervous system myelination in human infancy. II. Patterns of myelination in autopsied infants. Journal of Neuropathology and Experimental Neurology, 47(3), 217–234.
Kobel, M., Bechtel, N., Specht, K., Klarhofer, M., Weber, P., Scheffler, K., et al. (2010). Structural and functional imaging approaches in attention deficit/hyperactivity disorder: does the temporal lobe play a key role? Psychiatry Research, 183(3), 230–236.
Kumar, M., Srivastava, A., Agarwal, S., Behari, S., Malik, G. K., Rathore, R. K., et al. (2010). Cognitive functions correlate with diffusion tensor imaging metrics in patients with spina bifida cystica. Childs Nervous System.
Le Bihan, D. (1995). Molecular diffusion, tissue microdynamics and microstructure. NMR in Biomedicine, 8(7–8), 375–386.
Le Bihan, D. (2003). Looking into the functional architecture of the brain with diffusion MRI. Nature Reviews. Neuroscience, 4(6), 469–480.
Lebel, C., Rasmussen, C., Wyper, K., Andrew, G., & Beaulieu, C. (2010). Brain microstructure is related to math ability in children with fetal alcohol spectrum disorder. Alcoholism, Clinical and Experimental Research, 34(2), 354–363.
Lebel, C., Rasmussen, C., Wyper, K., Walker, L., Andrew, G., Yager, J., et al. (2008). Brain diffusion abnormalities in children with fetal alcohol spectrum disorder. Alcoholism, Clinical and Experimental Research, 23(10), 1732–1740.
Lebel, C., Walker, L., Leemans, A., Phillips, L., & Beaulieu, C. (2008). Microstructural maturation of the human brain from childhood to adulthood. Neuroimage, 40(3), 1044–1055.
Li, L., Coles, C. D., Lynch, M. E., & Hu, X. (2009). Voxelwise and skeleton-based region of interest analysis of fetal alcohol syndrome and fetal alcohol spectrum disorders in young adults. Human Brain Mapping, 30(10), 3265–3274.
Ma, X., Coles, C. D., Lynch, M. E., Laconte, S. M., Zurkiya, O., Wang, D., et al. (2005). Evaluation of corpus callosum anisotropy in young adults with fetal alcohol syndrome according to diffusion tensor imaging. Alcoholism, Clinical and Experimental Research, 29(7), 1214–1222.
Masutani, Y., Aoki, S., Abe, O., Hayashi, N., & Otomo, K. (2003). MR diffusion tensor imaging: recent advance and new techniques for diffusion tensor visualization. European Journal of Radiology, 46(1), 53–66.
Mattson, S. N., & Riley, E. P. (1998). A review of the neurobehavioral deficits in children with fetal alcohol syndrome or prenatal exposure to alcohol. Alcoholism, Clinical and Experimental Research, 22(2), 279–294.
Mori, S., & Zhang, J. (2006). Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron, 51(5), 527–539.
Moseley, M. E., Cohen, Y., Kucharczyk, J., Mintorovitch, J., Asgari, H. S., Wendland, M. F., et al. (1990). Diffusion-weighted MR imaging of anisotropic water diffusion in cat central nervous system. Radiology, 176(2), 439–445.
Muetzel, R. L., Collins, P. F., Mueller, B. A., Schissel, A. M., Lim, K. O., & Luciana, M. (2008). The development of corpus callosum microstructure and associations with bimanual task performance in healthy adolescents. Neuroimage, 39(4), 1918–1925.
Mullen, K. M., Vohr, B. R., Katz, K. H., Schneider, K. C., Lacadie, C., Hampson, M., et al. (2010). Preterm birth results in alterations in neural connectivity at age 16 years. Neuroimage.
Neil, J., Miller, J., Mukherjee, P., & Huppi, P. S. (2002). Diffusion tensor imaging of normal and injured developing human brain—a technical review. NMR in Biomedicine, 15(7–8), 543–552.
O’Leary-Moore, S., Parnell, S. E., Lipinski, R. J., & Sulik, K. K. (2011). Magnetic resonance-based imaging in animal models of fetal alcohol spectrum disorders. Neuropsychology Review, 21(2), in press.
Pantoni, L., & Garcia, J. H. (1995). The significance of cerebral white matter abnormalities 100 years after Binswanger’s report. A review. Stroke, 26(7), 1293–1301.
Paus, T. (2009). Growth of white matter in the adolescent brain: Myelin or axon? Brain Cogn.
Perham-Hester, K. A., & Gessner, B. D. (1997). Correlates of drinking during the third trimester of pregnancy in Alaska. Maternal and Child Health Journal, 1(3), 165–172.
Pfefferbaum, A., Sullivan, E. V., Hedehus, M., Adalsteinsson, E., Lim, K. O., & Moseley, M. (2000). In vivo detection and functional correlates of white matter microstructural disruption in chronic alcoholism. Alcoholism, Clinical and Experimental Research, 24(8), 1214–1221.
Qiu, D., Tan, L. H., Zhou, K., & Khong, P. L. (2008). Diffusion tensor imaging of normal white matter maturation from late childhood to young adulthood: voxel-wise evaluation of mean diffusivity, fractional anisotropy, radial and axial diffusivities, and correlation with reading development. Neuroimage, 41(2), 223–232.
Radua, J., Via, E., Catani, M., & Mataix-Cols, D. (2010). Voxel-based meta-analysis of regional white-matter volume differences in autism spectrum disorder versus healthy controls. Psychological Medicine, 1–12.
Raichle, M. E., MacLeod, A. M., Snyder, A. Z., Powers, W. J., Gusnard, D. A., & Shulman, G. L. (2001). A default mode of brain function. Proceedings of the National Academy of Sciences of the United States of America, 98(2), 676–682.
Raichle, M. E., & Snyder, A. Z. (2007). A default mode of brain function: a brief history of an evolving idea. Neuroimage, 37(4), 1083–1090. discussion 1097–1089.
Rao, S. M. (1995). Neuropsychology of multiple sclerosis. Current Opinion in Neurology, 8(3), 216–220.
Riley, E. P., Mattson, S. N., Sowell, E. R., Jernigan, T. L., Sobel, D. F., & Jones, K. L. (1995). Abnormalities of the corpus callosum in children prenatally exposed to alcohol. Alcoholism, Clinical and Experimental Research, 19(5), 1198–1202.
Roebuck, T. M., Mattson, S. N., & Riley, E. P. (2002). Interhemispheric transfer in children with heavy prenatal alcohol exposure. Alcoholism, Clinical and Experimental Research, 26(12), 1863–1871.
Sampson, P. D., Streissguth, A. P., Bookstein, F. L., Little, R. E., Clarren, S. K., Dehaene, P., et al. (1997). Incidence of fetal alcohol syndrome and prevalence of alcohol-related neurodevelopmental disorder. Teratology, 56(5), 317–326.
Schmithorst, V. J., & Yuan, W. (2009). White matter development during adolescence as shown by diffusion MRI. Brain Cogn.
Schweder, P. M., Joint, C., Hansen, P. C., Green, A. L., Quaghebeur, G., & Aziz, T. Z. (2010). Chronic pedunculopontine nucleus stimulation restores functional connectivity. NeuroReport, 21(17), 1065–1068.
Shukla, D. K., Keehn, B., & Muller, R. A. (2010). Tract-specific analyses of diffusion tensor imaging show widespread white matter compromise in autism spectrum disorder. Journal of Child Psychology and Psychiatry and Allied Disciplines.
Skudlarski, P., Jagannathan, K., Calhoun, V. D., Hampson, M., Skudlarska, B. A., & Pearlson, G. (2008). Measuring brain connectivity: diffusion tensor imaging validates resting state temporal correlations. Neuroimage, 43(3), 554–561.
Smith, S. M., Jenkinson, M., Johansen-Berg, H., Rueckert, D., Nichols, T. E., Mackay, C. E., et al. (2006). Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage, 31(4), 1487–1505.
Sowell, E. R., Johnson, A., Kan, E., Lu, L. H., Van Horn, J. D., Toga, A. W., et al. (2008). Mapping white matter integrity and neurobehavioral correlates in children with fetal alcohol spectrum disorders. The Journal of Neuroscience, 28(6), 1313–1319.
Sowell, E. R., Mattson, S. N., Thompson, P. M., Jernigan, T. L., Riley, E. P., & Toga, A. W. (2001). Mapping callosal morphology and cognitive correlates: effects of heavy prenatal alcohol exposure. Neurology, 57(2), 235–244.
Sowell, E. R., Thompson, P. M., Mattson, S. N., Tessner, K. D., Jernigan, T. L., Riley, E. P., et al. (2001). Voxel-based morphometric analyses of the brain in children and adolescents prenatally exposed to alcohol. NeuroReport, 12(3), 515–523.
Stejskal, E. O., & Tanner, J. E. (1965). Spin diffusion measurements: spin echos in the presence of time-dependent field gradient. The Journal of Chemical Physics, 42, 288–292.
Streissguth, A. P., Sampson, P. D., Olson, H. C., Bookstein, F. L., Barr, H. M., Scott, M., et al. (1994). Maternal drinking during pregnancy: attention and short-term memory in 14-year-old offspring–a longitudinal prospective study. Alcoholism, Clinical and Experimental Research, 18(1), 202–218.
Sullivan, E. V. (Ed.). (2010). Historical feature on disconnexion syndrome in animals and man by Norman Geschwind [Special Issue]. Neuropsychology Review (Vol. 20(2)).
Sullivan, E. V., & Pfefferbaum, A. (2011). Diffusion tensor imaging in aging and age-related disorders. In D. K. Jones (Ed.), Diffusion MRI: Theory, methods, and applications (pp. 624–643). Oxford: Oxford University Press.
Teipel, S. J., Meindl, T., Wagner, M., Stieltjes, B., Reuter, S., Hauenstein, K. H., et al. (2010). Longitudinal changes in fiber tract integrity in healthy aging and mild cognitive impairment: A DTI follow-up study. Journal of Alzheimer's Disease, 22(2), 507–522.
Trivedi, R., Gupta, R. K., Shah, V., Tripathi, M., Rathore, R. K., Kumar, M., et al. (2008). Treatment-induced plasticity in cerebral palsy: a diffusion tensor imaging study. Pediatric Neurology, 39(5), 341–349.
Uddin, L. Q., Kelly, A. M., Biswal, B. B., Margulies, D. S., Shehzad, Z., Shaw, D., et al. (2008). Network homogeneity reveals decreased integrity of default-mode network in ADHD. J Neurosci Methods, 169(1), 249–254.
Utsunomiya, H. (2010). Diffusion MRI abnormalities in pediatric neurological disorders. Brain and Development.
Walhovd, K. B., Westlye, L. T., Moe, V., Slinning, K., Due-Tonnessen, P., Bjornerud, A., et al. (2010). White matter characteristics and cognition in prenatally opiate- and polysubstance-exposed children: a diffusion tensor imaging study. AJNR. American Journal of Neuroradiology, 31(5), 894–900.
Warner, T. D., Behnke, M., Eyler, F. D., Padgett, K., Leonard, C., Hou, W., et al. (2006). Diffusion tensor imaging of frontal white matter and executive functioning in cocaine-exposed children. Pediatrics, 118(5), 2014–2024.
Wilde, E. A., Chu, Z., Bigler, E. D., Hunter, J. V., Fearing, M. A., Hanten, G., et al. (2006). Diffusion tensor imaging in the corpus callosum in children after moderate to severe traumatic brain injury. Journal of Neurotrauma, 23(10), 1412–1426.
Wozniak, J. R., Krach, L., Ward, E., Mueller, B. A., Muetzel, R., Schnoebelen, S., et al. (2007). Neurocognitive and neuroimaging correlates of pediatric traumatic brain injury: a diffusion tensor imaging (DTI) study. Archives of Clinical Neuropsychology, 22(5), 555–568.
Wozniak, J. R., Mueller, B. A., Chang, P., Muetzel, R. L., Caros, L., & Lim, K. O. (2006). Diffusion tensor imaging in children with fetal alcohol spectrum disorders. Alcoholism, Clinical and Experimental Research, 30(10), 1799–1806.
Wozniak, J. R., Mueller, B. A., & Lim, K. O. (2008). Diffusion tensor imaging. In C. A. Nelson & M. Luciana (Eds.), Handbook of developmental cognitive neuroscience (2nd ed., pp. 301–310). Cambridge: MIT.
Wozniak, J. R., Mueller, B. A., Muetzel, R. L., Bell, C. J., Hoecker, H. L., Nelson, M. L., et al. (2011). Inter-hemispheric functional connectivity disruption in children with prenatal alcohol exposure. Alcoholism, Clinical and Experimental Research.
Wozniak, J. R., Mueller, B. A., Ward, E. E., Lim, K. O., & Day, J. W. (2011). White matter abnormalities and neurocognitive correlates in children and adolescents with myotonic dystrophy type 1: A Diffusion Tensor Imaging study. Neuromuscular Disorders.
Wozniak, J. R., Muetzel, R. L., Mueller, B. A., McGee, C. L., Freerks, M. A., Ward, E. E., et al. (2009). Microstructural corpus callosum anomalies in children with prenatal alcohol exposure: an extension of previous diffusion tensor imaging findings. Alcoholism, Clinical and Experimental Research, 33(10), 1825–1835.
Wu, T. C., Wilde, E. A., Bigler, E. D., Li, X., Merkley, T. L., Yallampalli, R., et al. (2010). Longitudinal Changes in the Corpus Callosum following Pediatric Traumatic Brain Injury. Developmental Neuroscience.
Yakolev, P. I., & Lecours, A. R. (1967). The myelogenic cycles of regional maturation of the brain. In A. Minkowski (Ed.), Regional development of the brain in early life (pp. 3–70). Blackwell: Oxford.
Yoshida, S., Hayakawa, K., Yamamoto, A., Okano, S., Kanda, T., Yamori, Y., et al. (2010). Quantitative diffusion tensor tractography of the motor and sensory tract in children with cerebral palsy. Developmental Medicine and Child Neurology.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wozniak, J.R., Muetzel, R.L. What Does Diffusion Tensor Imaging Reveal About the Brain and Cognition in Fetal Alcohol Spectrum Disorders?. Neuropsychol Rev 21, 133–147 (2011). https://doi.org/10.1007/s11065-011-9162-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-011-9162-1