
Abstract
The understanding of oxidative damage in different neurodegenerative diseases could enhance therapeutic strategies. Our objective was to quantify lipoperoxidation and other oxidative products as well as the activity of antioxidant enzymes and cofactors in cerebrospinal fluid (CSF) samples. We recorded data from all new patients with a diagnosis of either one of the four most frequent neurodegenerative diseases: Parkinson’s disease (PD), Alzheimer’s disease (AD), Huntington’s disease (HD) and lateral amyotrophic sclerosis (ALS). The sum of nitrites and nitrates as end products of nitric oxide (NO) were increased in the four degenerative diseases and fluorescent lipoperoxidation products in three (excepting ALS). A decreased Cu/Zn-dependent superoxide dismutase (SOD) activity characterized the four diseases. A significantly decreased ferroxidase activity was found in PD, HD and AD, agreeing with findings of iron deposition in these entities, while free copper was found to be increased in CSF and appeared to be a good biomarker of PD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Neurodegenerative diseases have various etiologic factors, biochemical and pathological changes and mechanisms in common, such as selective neuronal death, protein aggregation, glutamate-mediated excitotoxicity, mitochondrial failure and finally, an important role of transition metals and oxidative stress [1]. Neurons are highly susceptible to free radical-mediated injury due to their important oxidative metabolism and given that neuronal membranes are rich in polyunsaturated fatty acids [2]. When free radical oxidants generation by the neuron surpasses the ability of endogenous antioxidant defenses, proteins, lipids, DNA and other macromolecules become the main targets for oxidative modifications, which can lead to deterioration of cellular architecture and signaling and ultimately death [3]. Parkinson’s disease (PD) is the most frequent neurodegenerative disease in Mexico. In our institution alone, PD patients represent 5% of the total attendance (2,500 medical consultations for PD per year). Occasionally, patients with relatively advanced disease are referred untreated to our clinic, which is a particular interesting circumstance for the present study. Among the most important biochemical changes in PD, reduced glutathione, an important free radical scavenger, has been confirmed to be decreased in the substantia nigra (SN) in a PD animal model [4, 5]. Monoamine catabolism, via MAO enzymes, generates hydrogen peroxide (H2O2) and further free radical hydroxyl. This highly reactive oxygen species, derived from H2O2 in presence of reduced transition metals and/or in absence of glutathione peroxidase, contributes also to oxidative stress in PD [6]. Cell death in the SN in PD patients has been associated with increased iron levels related to decreased content of the iron-binding protein ferritin [7]. Alterations in other metallic compounds have also been observed; copper levels are reduced in both parkinsonian tissues derived from post mortem studies and PD animal models [7–9] while copper ion is increased in the cerebrospinal fluid (CSF) of PD patients [10, 11]. Huntington’s disease (HD) is a relentless progressive autosomal dominant disease responsible for a wide array of CNS abnormalities including movement disorders, mood and behavioral alterations as well as cognitive impairment. This condition is caused by the unstable expansion of the cytosine–adenine–guanine (CAG) trinucleotide repeat within the coding region of the IT15 gene on the short arm of chromosome 4, encoding the protein huntingtin [12]. Since 1994, our institution has been the main referral site for HD molecular diagnosis in Mexico. The most frequent neurodegenerative disease in several countries, Alzheimer’s disease (AD), is characterized by a gradual cognitive deficit generating behavioral disturbances and loss of independency. Surprisingly, only 40 of 600 new cases of dementia attended in our institution during the last 4 years have a diagnosis of probable AD, according to the NINCDS-ADRDA criteria [13]. Amyotrophic lateral sclerosis is a relatively frequent neurodegenerative disease that affects both upper and inferior motoneurons. Reduced glutamate (Glu) transporter, EAAT1, has been described in lateral amyotrophic sclerosis (ALS) tissues in 1995 [14], and recently demonstrated in aging and AD [15]. Looking for the effects of the excitatory aminoacid Glu on neurons, especially on the calcium mediated synthesis of nitric oxide (NO), we found that nitrites and nitrates, as end-products of NO, are measurable in the CSF [16]. To appreciate the magnitude of the oxidative generation of free radicals in the CNS and the consequent membrane damage, we found that lipid fluorescent products levels in the CSF can be a stable and representative marker of lipid peroxidation [17].
Superoxide dismutase (SOD) is the main antioxidant enzyme, as superoxide is implicated in the production of peroxide and other oxidative species. Two isoformes of this enzyme are copper dependent. Mutations in the cytosolic copper enzyme SOD1 result in the motor neuron degeneration of some forms of familial amyotrophic lateral sclerosis [18] and current evidence suggests a direct pathogenic role of copper in this process [19].
Copper is an essential trace metal which plays a fundamental role in the biochemistry of the human nervous system. Menkes disease and Wilson’s disease are inherited disorders of copper dependent ATPases and the dramatic neurodegenerative phenotypes of these two diseases underscore the essential nature of copper in nervous system development as well as the toxicity of this metal when neuronal copper homeostasis is altered [19].
Ceruloplasmin is an abundant alpha 2-serum glycoprotein that contains over 95% of the copper present in human plasma and consists of a ferroxidase enzyme (capable of transforming Fe2+ into Fe3+). Aceruloplasminemia is an autosomal recessive disorder caused by mutations in the ceruloplasmin gene expressed in the CNS [20]. It is characterized by a progressive neurodegeneration of the retina, basal ganglia, dentate nucleus and cerebral cortex in association with iron accumulation in these tissues. Since PD, HD and AD also present iron deposition in degenerated areas, we are particularly interested in the functional state of ceruloplasmin in these pathologies, as a biochemical marker of metal related neurodegenerative processes.
Experimental Procedure
Two hundred and forty ambulatory patients newly referred to the National Institute of Neurology and Neurosurgery (NINN) with suspected neurodegenerative disease were screened to participate in this study after thorough clinical examination and revision of laboratories and head MRI. Patients taking medications that could potentially modify our results (selegiline, levodopa, steroids and/or riluzole) were not included. Aged-pared control subjects were recruited applying the same criteria, but with no history of CNS degenerative disorder and an indication for a lumbar puncture; i.e., uninfected rhinorrea, myelographies, idiopathic intracranial hypertension and other causes of headache non tumoral in origin, and psychomotor agitation without evidence of encephalitis, during a 40-month-period.
Diagnostic Criteria and Clinimetrics
HD patients were studied at the Movement Disorders Clinic of the NINN. All subjects were clearly documented as HD-patients by clinical history, neurological examination and magnetic resonance imaging. Furthermore, the molecular diagnosis was provided by the genetic department [21]. The age of onset was defined as the age at which choreiform movements or mental disorders were first documented. The clinical disability was assessed by the UHDRS [22].
PD patients were asked to participate after the neurological examination, laboratories revision, and before to initiate the treatment.
Alzheimer disease patients were screen using the Mini-Mental State Examination [23] and AD criteria [13]. A Hachinski ischemic score (HIS) above six points was also considered to exclude vascular dementia [24]. Lumbar puncture was performed, after an informed consent form was signed and authorized by a family member. After inclusion of each patient, an array of neuropsychological tests and a further neurological revision corroborated the severity of the dementia.
ALS patients were diagnosed using the clinical and electromyographic El Escorial criteria [25] and scored in the ALS Functional Rating Scale [26].
Biological Assessment
All the lumbar punctures were practiced by two experienced neurologists (MCB and LMB). A first 2 ml collection in a glass tube was employed to observe the absence of traumatic puncture and sent to the clinical laboratory for cyto-chemical analysis. The second part collected for the present study in a 5 ml plastic tube protected by the light was rapidly aliquoted, coded and frozen at −80°C for further analyses.
-
(1)
Lipid peroxidation assay The presence of lipid fluorescent products in the CSF is a solid index of lipoperoxidation in the CNS. In our laboratory, we have adapted the technique previously described [17]; briefly: 500 μl of undiluted CSF were added with 4 ml of chloroform–methanol 2:1 mixture, in glass tubes protected from light exposure. After gently shaking the tubes for 2 min, followed by a centrifugation step at 10,000 rpm for 10 min, the superior aqueous phase was discharged and the intermediate skin was delicately moved to transfer 2.5 ml of organic phase (bottom layer) into clean tubes and add 1 ml of H2O. After gently shaking for one min, mixture was placed in ice for 15 min, then the upper phases were delicately pumped out and 1 ml of organic phase was transferred into a quartz cuvette and added with 100 μl of methanol. Fluorescence was measured in a Perkin-Elmer LS50B luminescence spectrophotometer at 370 nm of excitation and 430 nm of emission. The sensitivity of the spectrophotometer was adjusted to 140 fluorescence units (FU) with a 0.1 mg/l quinine standard solution in 0.05 M sulfuric acid solution. Results are expressed in FU/ml.
-
(2)
Nitrites + nitrates concentration was measured by high performance liquid chromatography as previously described [27].
-
(3)
Ceruloplasmin ferroxidase activity This measurement described in the 80s for sera was adapted and validated in our neurochemistry laboratory for CSF analysis [11]. The enzymatic reaction is based on the capability of CP to transform Fe2+ into Fe3+. In brief, 100 μl CSF samples were mixed with 200 μl acetate buffer (0.3 M, pH 6). After incubation at 30°C for 5 min, 100 μl freshly prepared 0.01 M ammonium ferrous sulfate solution were added. Samples were then incubated for five more minutes at the same temperature; the mixture reaction was stopped by addition of 200 μl 1.25 M perchloric acid. Samples were centrifuged at 10,000g for 3 min. Ferric iron produced by ferroxidase activity was determined by adding the same volume of 0.5 M ammonium thiocyanate solution to the incubation mixture. The red thiocyanate–Fe(III) complex was monitored at 450 nm in a Perkin-Elmer Lambda-20-double-beam spectrophotometer.
-
(4)
Cu/Zn–SOD activity in the CSF was measured in 50 μl aliquots of CSF, added to a mixture containing xanthine and cytochrome, subsequently added to a second solution with xanthine-oxidase as described in detail [27]. The inhibition capacity of xanthine-oxidase reflects the SOD activity in the CSF.
-
(5)
Total copper and free copper levels in the CSF were analyzed by graphite furnace atomic absorption. To obtain the free—low molecular weight copper—immediately after defrosting the samples, a 400 μl aliquot was placed in a Microcon YM-3 centrifugal device (Millipore Corporation) that uses Amicon’s low-binding, anisotropic, hydrophilic regenerated cellulose membrane able to separate a nominal molecular weight of 3000 Dalton. After a 70 min. centrifugation at 14,000g. in a 5417R Eppendorf centrifuge with fast cooling system, 300 μl of filtered CSF were obtained, in which the copper concentration was directly measured by atomic absorption spectrophotometry.
Statistical Analysis
Individual data collection forms were stored on a computerized database to be further analyzed with SPSS V.10.0 for Windows (SPSS Inc., Chicago, IL, USA). The distribution of each single variable was first analyzed descriptively. Relationships between clinical and biological variables were also checked by graphs and correlation matrix completed by multivariate logistic regression models taking as dependent variable the diagnosis of a single degenerative disease versus control and looking for the independent (biological) variable that could be a good predictor in that particular pathology. On the other hand, biological measurements were analyzed in the different patients groups and a multivariate post hoc analyze evaluated the impact of each marker in the different neurodegenerative disorders.
Results
Patients newly referred to the NINN during a 40-month period (n = 135) matched the criteria for entering the study. Fourteen cases were excluded from the final analysis given that the CSF cytochemical analysis showed abnormal cell number or elevated protein concentration; from these, 12 exhibited positive serology for neurocysticercosis in their CSF: one patient with PD and 11 potential controls. We finally report the study of 23 HD patients (all with positive molecular diagnosis), 22 PD patients untreated with levodopa, 27 sporadic ALS patients and 8 with probable Alzheimer disease according to the NINCDS-ADRDA criteria. Fluorescent lipid peroxidation products were found significantly elevated in the CSF in AD patients, followed by PD and HD. In contrast, patients with ALS registered CSF levels similar to controls (Fig. 1a). The sum of nitrates (abundant) and nitrites (mostly undetectable) was significantly higher in all four neurodegenerative disorders than in the control group, especially in ALS (Fig. 1b).

CSF markers of lipid peroxidation and nitric oxide production in the five groups of subjects. Bars represent means and error bars, SEM. (a) Fluorescent products ANOVA p < 0.001 followed by Tukey post hoc analysis shows no difference between ALS and control group (p = 1.000). In HD versus control, p = 0.05, in PD p = 0.043, in AD p = 0.001. (b) Nitrites + nitrates concentration in the CSF ANOVA p < 0.001 followed by Tukey analysis. Samples from patients with ALS, HD, PD and AD, versus control group, reached p values of 0.000, 0.024, 0.012 and 0.003, respectively
Cu/Zn–SOD activity was decreased in the four diseases (Fig. 2a) while ferroxidase activity, uncharged by ceruloplasmin, was significantly decreased in PD and HD, also decreased in the few samples from AD patients, and similar to controls in ALS (Fig. 2b).

Two antioxidant enzymatic activities in the CSF from the five groups of patients. Bars represent means and error bars, SEM. (a) Cu/Zn–SOD activity. ANOVA p = 0.001 followed by Tukey analysis. In ALS versus control, p = 0.009, in HD p = 0.007, in PD p = 0.021 and in AD p = 0.0432. (b) Ferroxidase (ceruloplasmine) activity. ANOVA p = 0.000 followed by Dunnett analysis: samples from patients with ALS, HD, PD and AD reached, versus control, p values of 1, 0.000, 0.012 and 0.605, respectively
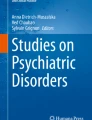
The measurement of free copper in CSF showed a statistically significant increase, only in the PD group (Fig. 3a). Some clinical–biological correlations need to be emphasized. We found a significant relationship between the clinical time of onset and lipoperoxidation in all the diseases with a global Pearson coefficient = 0.56, p < 0.001. Age also correlated with this biologic marker, both in the neurodegenerative group and in the control group, with the following Spearman’s rho coefficients 0.29; p = 0.008 and 0.33; p = 0.007 respectively. Lipid peroxidation in AD seems to have a strong relationship with the alteration in the MMSE Spearman’s rho coefficients = −0.98; p < 0.001. Cu/Zn–SOD activity (IU) in ALS correlated with the amplitude of motor potentials in both lunar nerves, thus providing a good marker on axonal degeneration (p = 0.002) [27], but no correlation was found with the ALS Functional Rating Scale (p = 0.105).

Measurement of free copper concentration in the CSF and ROC curve in PD patients versus controls. (a) Free copper concentration in the CSF in the five groups of patients. ANOVA p = 0.011 followed by Dunnett analysis shows versus controls no difference in ALS (p = 1), in HD p = 0.153, in AD p = 0.405, and PD p = 0.007. (b) Receiver operating characteristic curve analyze for free copper concentration. The area under the curve indicates that 84% of PD patients have a free copper concentration >3.2 μmol/l. Asymptotic 95% interval is 0.72–0.95
Ferroxidase activity was related to UHDRS motor scale, with a Spearman’s rho coefficient = −0.82, p = 0.003 in HD patients, as well as to the time of onset (months) in PD (p = 0.007) and AD patients (p < 0.001). Free copper in PD showed to be significantly correlated with the duration of the disease and UPDRS motor scores with the respective rho coefficient = 0.409, p < 0.05 and 0.399, p < 0.05. High levels in this variable seem to be specific of PD as the multivariate analysis showed the PD group to be the only significantly different from controls (Fig. 3a). Given this noticeable increase in free copper in CSF from patients suffering PD, we looked for the best cut-point to discriminate this finding from the control group. The free copper concentration value in CSF > 3.2 μg/l gave an 84% specificity and a 75% sensibility, despite sample size, while the receiver operating characteristic (ROC) curve illustrates the significant area under the curve (Fig. 3b). We did not find any difference related to gender in all five biomarkers.
Discussion
Fluorescent lipid peroxidation products (Schiff bases, conjugated dienes, oxidized proteins and aldehyde polymers), are stable indicators of membrane damage and the rate of CSF fluorescence with this technique, is a highly sensitive marker of oxidative stress [28]. Its correlation with age (not with gender) and disease progression indexes were significant as was expected. However, in ALS, there was no difference in its values compared with the control group. This result suggests that membranes probably are not damaged in ALS as in the other studied diseases or that these products in CSF are rapidly moved out while nitrates were significantly increased in all the four pathological groups reflecting a NO overproduction whereas Cu/Zn–SOD activity was decreased especially in sporadic ALS cases. Superoxide radical per se is not able to induce lipid peroxidation, but in presence of NO, the endogenous production of a powerful oxidant, the highly diffusible peroxynitrite (ONOO−), is sufficient to activate apoptosis in motor neurons by activating caspases [29]. The action of reactive nitrogen species (NO and ONOO−) is mostly important in mitochondria, especially by their interaction with cytochrome c oxidase, which is the copper dependent complex IV of the respiratory chain, modulating different pathways such as apoptosis and redox regulation of gene expression [30]. In PD models, tyrosine nitration has been especially implicated in α-synuclein aggregation, a major component of Lewy bodies [3].
Decreased ferroxidase activity was a common characteristic of all three diseases related with the increment of iron deposition in degenerated areas. This supports the neuroprotective and iron mobilization functions of brain ceruloplasmin.
Free copper was elevated in the same samples of CSF accompanying a diminution of copper–proteins [11]. Copper-dependent enzymes such as Cp and SOD may play an important role in copper retention, in addition to some other copper-binding proteins, like albumin and metallothionein. In the present study, mean total protein concentration in the CSF was found slightly decreased in all the four diseases, but without statistical significance, indicating that it is not a generalized effect on CSF protein content. On the other hand, metallothionein, using the silver saturation technique, showed a concentration in the CSF below the detection limit of the atomic absorption device (data not shown). An important result of the present work is that a level of free copper in the CSF > 3.2 μg/l could be considered as a good marker of idiopathic PD. In PD, HD and AD, free copper is also significantly related with the clinical stage and the duration of clinical manifestations. In a previous work in PD patients and controls, where we also included subjects under l-DOPA treatment, the free fraction of copper was measured indirectly through the ratio ceruloplasmin ferroxidase activity/total copper concentration in CSF. A decreased ratio was found only for untreated PD patients [11]. The measurement of copper ion by Pall et al. [10] by means of phenanthroline quelation reflects the metal unbound to SOD and ceruloplasmin but it probably also measures copper bound to albumin, histidine and dopamine molecules that loosely bound copper ion. Thus, our report is the first showing a direct measurement of free CSF copper in PD. We describe here an easy, rapid, reproducible and more specific technique to estimate total ionic copper. Free copper is also for the first time related to UPDRS motor scale. This finding, together with the decreased copper enzyme activities, and the decreased copper content in affected tissues, underlines the role of copper and copper-binding proteins in the establishment of neurodegeneration. The cause of sporadic ALS is not known, but excitotoxicity due to overactivation of glutamate receptors may mediate the motor neuron degeneration in the spinal cord, which is the hallmark of this disease [31]. As a consequence of glutamate receptors activation, production of NO through the Ca/Calmoduline dependent neuronal synthase of NO (nNOS), seems to play a major role in ALS programmed neuronal death [29], instead of necrosis and membrane destruction by free radicals derived from NO. The other neurodegenative pathologies in this study: HD, AD and PD, are characterized by an increased level of lipid peroxidation and a diminution of copper–proteins content in the CSF, in addition to the presence of increased concentration of free copper-ion, especially in PD. A German research team recently found the SN hyperechogenicity, an ultrasound marker of iron deposition, to be significantly associated with ceruloplasmin (Cp) gene variations [32]. Previously, the role of Cp in iron levels regulation and free radicals scavenging has been demonstrated in a Cp knock-out rodent model [33]. Cp deficiency also seems to be related to increased CSF free copper. Unfortunately, the reduced number of samples from AD patients avoided us to conclude in this disease, while an explanation is needed in HD subjects, where the most important iron depots are shown in their striatum by MRI, comparing with PD patients, while better Cp activity and lower free copper levels were measured in their CSF. Copper also acts as a potent oxidant depending on its oxidation state. Other studies have also implicated copper in the pathogenesis of neuronal injury in Alzheimer’s disease [34] and prion-mediated encephalopathies [35], suggesting that further elucidation of the mechanisms of copper transit and metabolism within the nervous system will be of direct relevance to our understanding of the pathophysiology of neurodegenerative diseases. Consequently, a therapeutic research line based on the induction of copper-dependent proteins is recommended.
References
Price DL (1999) New order from neurological disorders. Nature 399(suppl):A3–A5
Halliwell B (1992) Reactive oxygen species in the central nervous system. J Neurochem 59:1609–1623
Ischiropoulos H, Beckman JS (2003) Oxidative stress and nitration in neurodegeneration: cause, effect, or association? J Clin Invest 111:163–169
Jenner P, Schapira AH, Marsden CD (1992) New insights into the cause of Parkinson’s disease. Neurology 42:2241–2250
Schon EA, Manfredi G (2003) Neuronal degeneration and mitochondrial dysfunction. J Clin Invest 111:303–312
Youdim MBH, Ben Shachar D, Yehuda S, Riederer P (1990) The role of iron in the Basal Ganglion. Adv Neurol 53:155–162
Dexter DT, Jenner P, Schapira AHV, Marsden CD (1992) Alterations in levels of iron, ferritin, and other trace metals in neurodegenerative diseases affecting the basal ganglia. Ann Neurol 32:S94–S100
Rios C, Alvarez-Vega R, Rojas P (1995) Depletion of copper and manganese in brain after MPTP treatment of mice. Pharmacol Toxicol 76:348–352
Alcaraz-Zubeldia M, Rojas P, Boll C, Rios C (2001) Neuroprotective effect of acute and chronic administration of copper (II) sulfate against MPP+ neurotoxicity in mice. Neurochem Res 26:59–64
Pall HS, Williams AC, Blake DR et al (1987) Raised cerebrospinal-fluid copper concentration in Parkinson’s disease. Lancet 2:238–241
Boll MC, Sotelo J, Otero E, Alcaraz-Zubeldia M, Rios C (1999) Reduced ferroxidase activity in the CSF from patients with Parkinson’s disease. Neurosci Lett 265:155–158
Huntington’s Disease Collaborative Research Group (1993) A novel gene containing a trinucleotid repeat that is unstable on Huntington’s disease chromosomes. Cell 72:971–983
McKhann G, Drachman D, Folstein M et al (1994) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of the Department of Health and Human Services task force on Alzheimer’s disease. Neurology 34:939–944
Rothstein JD, Van Kammen M, Levey AI, Martin J, Kuncl JW (1995) Selective loss of glial glutamate transporter GTL1 in amyotrophic lateral sclerosis. Ann Neurol 38:73–84
Zoia C, Cogliati T, Tagliabue E et al (2004) Glutamate transporters in platelets: EAAT1 decrease in aging and in Alzheimer’s disease. Neurobiol Aging 25:149–157
Zecca L, Rosati M, Renella R et al (1998) Nitrite and nitrate levels in cerebrospinal fluid of normal subjects. J Neural Transm 105:627–633
Naidoo R, Knapp ML (1992) Studies of lipid peroxidation products in cerebrospinal fluid and serum in multiple sclerosis and other conditions. Clin Chem 38:2449–2454
Rosen DR, Siddique T, Patterson D et al (1993) Mutations in Cu/Zn superoxide dismutase are associated with familiar amyotrophic lateral sclerosis. Nature 362:59–62
Waggoner DJ, Bartnikas TB, Gitlin JD (1999) The role of copper in neurodegenerative diseases. Neurobiol Dis 6:221–230
Harris ZL, Takahashi Y, Miyajima H, Serizawa M, McGiliwray RTA, Gitlin JD (1995) Aceruloplasminemia: molecular characterization of this disorder of iron metabolism. Proc Natl Acad Sci USA 92:2539–2543
Alonso ME, Yescas P, Cisneros B et al (1997) Analysis of the (CAG)n repeat causing Huntington’s disease in a Mexican population. Clin Genet 51:225–230
Huntington Study Group (1996) Unified Huntington’s disease rating scale: reliability and consistency. Mov Disord 11:136–142
Folstein MF, Folstein SE, McHugh PR (1975) “Mini- mental state”: a practical method for grading the cognitive state of subjects for the clinician. J Psychiatr Res 12:189–198
Moroney JT, Bagiella E, Desmond DW et al (1997) Meta-analysis of the Hachinski Ischemic score in pathologically verified dementias. Neurology 49:1096–1105
Brooks BR (1994) El Escorial World Federation of Neurology criteria for the diagnosis of amyotrophic lateral sclerosis: subcommittee on motor neuron diseases/amyotrophic lateral sclerosis of the World Federation of Neurology research group on neuromuscular diseases and the El Escorial “clinical limits of amyotrophic lateral sclerosis” workshop contributors. J Neurol Sci 124(suppl):96–107
ALS CNTF Treatment Study Phase I-II Study Group (1996) The ALS functional rating scale: assessment of activities of daily living in patients with amyotrophic lateral sclerosis. Arch Neurol 53:141–147
Boll MC, Alcaraz-Zubeldia M, Montes S, Murillo-Bonilla LM, Rios C (2003) Raised nitrates level and low SOD activity in the CSF in sporadic ALS. Neurochem Res 28(5):699–703
Gutteridge JMC, Halliwell B (1990) The measurement and mechanism of lipid peroxidation in biological systems. TIBS 15:129–135
Estevez AG, Spear N, Manuel SM et al (1998) Role of endogenous nitric oxide and peroxynitrite formation in the survival and death of motor neurons in culture. Prog Brain Res 118:269–280
Brookes P, Levonen AL, Shiva S et al (2002) Mitochondria: regulators of signal transduction by reactive oxygen and nitrogen species. Free Rad Biol Med 33:755–764
Corona JC, Tovar-y-Romo LB, Tapia R (2007) Glutamate excitotoxicity and therapeutic targets for amyotrophic lateral sclerosis. Expert Opin Ther Targets 11:1415–1428
Hochstrasser H, Bauer P, Walter U et al (2004) Ceruloplasmin gene variations and substantia nigra hyperechogenicity in Parkinson disease. Neurology 63:1912–1917
Patel BN, Dunn RJ, Jeong SY et al (2002) Ceruloplasmin regulates iron levels in the CNS and prevents free radical injury. J Neurosci 2215:6578–6586
Bayer TA, Multhaup G (2005) Involvement of amyloid beta precursor protein (AbetaPP) modulated copper homeostasis in Alzheimer’s disease. J Alzheimers Dis 8:201–206
Brown DR (2001) Copper and prion disease. Brain Res Bull 55:165–173
Acknowledgments
The authors wish to thank all physicians and nurses involved in this study for their help and support, in particular Dr. Noffal from the clinical laboratory of the NINN. A doctoral grant No. 96086 from CONACyT also provided considerable support to this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boll, MC., Alcaraz-Zubeldia, M., Montes, S. et al. Free Copper, Ferroxidase and SOD1 Activities, Lipid Peroxidation and NO x Content in the CSF. A Different Marker Profile in Four Neurodegenerative Diseases. Neurochem Res 33, 1717–1723 (2008). https://doi.org/10.1007/s11064-008-9610-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11064-008-9610-3