
Abstract
Purpose
Germ cell tumors (GCT) in the central nervous system (CNS) are rare tumors that occur with highest frequency in males, Asian populations, and children less than age 20 years. Due to the rarity of these tumors, their patterns of incidence are not well-described. The aim of this study is to provide the most up-to-date data on incidence and survival patterns for CNS GCT by sex, race, and age at diagnosis.
Methods
The Central Brain Tumor Registry of the United States (CBTRUS) is the largest aggregation of population-based incidence data on primary brain and other CNS tumors in the United States, containing incidence data from 51 central cancer registries and representing 100% of the US population. The current study used the CBTRUS analytic file to examine incidence (IR) of CNS GCT from 2006 to 2015, as well as registry data from the Surveillance, Epidemiology, and End Results (SEER) program to examine survival.
Results
Males had greater IR than females in all CNS GCT histologies examined. Asian and Pacific Islanders had a significantly greater IR of CNS GCT than the other race categories. We confirmed that CNS GCT IR was greatest for those age 10–14 years and male. Overall survival rates were high for malignant CNS GCT, germinoma, mixed GCT, and malignant teratoma.
Conclusions
There is significant variation in CNS GCT incidence by sex, race, and age at diagnosis. Ascertaining accurate incidence and survival rates of CNS GCT provides vital information usable in real time for clinicians, public health planners, patients, and their families.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Germ cell tumors (GCT) in the central nervous system (CNS) are rare, presenting at an overall incidence rate (IR) of 0.10 per 100,000 person-years in the United States (US) [1,2,3,4,5]. Additionally, CNS GCT represent less than 5% of all CNS tumors and 3–11% of all pediatric brain tumors [1,2,3,4, 6, 7]. Common sites for CNS GCT include the pineal and suprasellar regions [6,7,8,9,10]. These tumors can cause a wide range of symptoms, including increased intracranial pressure, visual tract involvement, and endocrine abnormalities [1, 8]. Males are more than twice as likely to be diagnosed with CNS GCT compared to females (IR for males = 0.13 per 100,000, IR for females = 0.06 per 100,000), and it has been reported that males have a 15-fold increased incidence of GCT in the pineal region compared to females [1, 2, 5, 11, 12]. Approximately two-thirds of CNS GCT are germinomas (synonymous with dysgerminoma and seminoma), while the remaining one-third are classified as non-germinomatous germ cell tumors (NGGCT), which include teratoma (mature—benign or immature—malignant), embryonal carcinoma, yolk sac tumor, or choriocarcinoma, either occurring singly or, more commonly, admixed with or without a germinoma component (mixed malignant germ cell tumors) [1,2,3,4, 6, 8,9,10,11]. Germinomas are extremely sensitive to radiation therapy, with 5-year survival rates reported to exceed 90% with radiation therapy alone [3, 8, 9, 11, 13]. Patients with NGGCT, on the other hand, have very poor outcomes when treated with radiation therapy alone (5-year survival rates less than 15–20%), with improvements now reported as high as 76% 5-year survival after treatment with radiation therapy and chemotherapy in adults, and as high as 93% after treatment with combined neoadjuvant chemotherapy and radiation in children [3, 8, 10, 11, 13, 14]. Due to the rarity of these tumors, their patterns of incidence are not well-described. The objective of this report is to provide the most up-to-date data on incidence and survival patterns for CNS GCT by sex, race, and age at diagnosis for the US.
Materials and methods
Data collection
This study was approved as an exempt study by the University Hospitals Cleveland Medical Center Institutional Review Board. The Central Brain Tumor Registry of the United States (CBTRUS) data were provided through an agreement with the Centers for Disease Control and Prevention (CDC), National Program of Cancer Registries (NPCR) and from the research data file of the National Cancer Institute’s (NCI) Survival, Epidemiology, and Ends Results (SEER) program. The CBTRUS is the largest aggregation of population-based incidence data on primary brain and other central nervous system tumors in the US, containing incidence data from 51 central cancer registries (CCR) (46 NPCR and 5 SEER) and representing 100% of the US population [15]. The current study used the CBTRUS analytic file to examine incidence (IR) of primary CNS GCT from 2006 to 2015, as well as registry data from the NCI SEER program for 18 registries. Unless noted, incidence analyses are from the CBTRUS dataset, while the SEER data were used for survival analyses. All IR were adjusted to the 2000 US standard population. Population estimates for 2006–2015 were provided by the US Census American Community Survey (ACS) Demographic and Housing Estimates to determine IR of specified Asian subpopulations. Our analysis included histologically or radiologically confirmed newly diagnosed primary malignant and non-malignant germ cell tumors with the following International Classification of Diseases for Oncology, Third Edition (ICD-O-3) histology codes: 9060/3, 9061/3, 9064/3 (germinoma), 9065/3, 9085/3 (mixed germ cell tumor), 9080/0 (teratoma, benign), 9080/3, 9081/3, 9082/3, 9084/3 (teratoma, malignant), 9080/1 (teratoma, NOS), 9071/3 (yolk sac tumor), 9070/3 (embryonal carcinoma, NOS), and 9100/3 (choriocarcinoma). The following ICD-O-3 site codes were included: C70.0–C70.9, C71.0–C71.9, C72.0–C72.5, C72.8–C72.9, C75.1–C75.3, and C30.0 (ICD-O-3 histology codes 9522–9523 only).
Statistical analyses
SEER*Stat statistical software was used to calculate the age-adjusted IR per 100,000 population with corresponding 95% confidence intervals (95% CIs) for CNS GCT overall and by histology; these IRs were also examined by sex and race [16]. IR were considered to be significantly different between groups if the 95% CIs had no overlap. Proportions of Asian subpopulations by age interval for 2006–2015 were obtained from the American Community Survey (ACS) [17, 18]. These were used to create age-adjusted IR per 100,000 for specified Asian subpopulations using the dsrTest R package and the US 2000 Standard Populations [19]. Asian subpopulations were defined as: East Asia (Chinese, Japanese, Koreans), Southeast Asia (Filipinos, Vietnamese), Polynesia (Hawaiians, Samoans, Pacific Islanders NOS), South Asia (Indians), and Other Asian. In addition, the distribution of primary site for the most common CNS GCT histology, germinoma, was determined. Survival was assessed by Kaplan–Meier and multivariable Cox proportional hazards regression and included age at diagnosis, sex, race, and radiation status for selected malignant histologies. Survival analyses were conducted using R version 3.1.5. Statistics were suppressed when counts were fewer than 16 within a cell but included in totals except when data were suppressed from only one cell within a category to prevent identification of the number in the suppressed cell.
Results
Patient demographics
For the years of diagnosis 2006–2015, there were 2240 patients diagnosed in the United States with a CNS germ cell tumor (GCT) (Table 1). The majority of CNS GCT were germinomas (67.3%). The majority of cases occurred in males (75.4%) and White persons (78.7%). The average age at diagnosis was 18 years, while the median age at diagnosis was 16 years. Almost one-fourth (24.6%) of the patients were diagnosed in the 10–14 years age group (551 patients), with another 23.3% diagnosed in the 15–19 years age group (521 patients). Most GCT occurred in the pineal gland (949 patients; 42.4%). There were 1369 histologically confirmed (i.e. diagnosis confirmed at minimum by biopsy) germinomas (90.8%) and 637 NGGCT (86.9%), with the remaining cases having been diagnosed by radiography. In the subset from the SEER data, there were 695 patients diagnosed in the US with a CNS GCT, of whom 66.6% were diagnosed with germinoma in the decade 2006–2015. The SEER patient characteristics were similar to those of patients in the CBTRUS set. Over half of the patients in the SEER dataset (55.4%) underwent surgery (385 patients), while in another 42.3% of the patients (294 patients), did not receive surgery as it was not recommended. See Table 1 for a complete listing of patient demographics.
Age-adjusted incidence rates by sex in CBTRUS
Males had greater IR than females in all CNS GCT histologies examined (Fig. 1). Overall, males had an IR of 0.111 per 100,000 population (95% CI 0.105, 0.116), while females had an IR of 0.038 per 100,000 population (95% CI 0.035, 0.041), which is statistically significant. The largest difference in IR was observed in mixed germ cell tumors, with males having an IR of 0.012 per 100,000 population (95% CI 0.011, 0.014) and females having an IR of 0.003 per 100,000 population (95% CI 0.002, 0.004). For germinoma, males had an IR of 0.078 per 100,000 population (95% CI 0.074, 0.083) compared to females who had an IR of 0.022 per 100,000 population (95% CI 0.019, 0.024). For malignant teratoma, males had an IR of 0.006 per 100,000 population (95% CI 0.005, 0.008) compared to females who had an IR of 0.003 per 100,000 population (95% CI 0.002, 0.004). However, the difference margin became narrower for benign teratoma, with males having an IR of 0.008 per 100,000 population (95% CI 0.007, 0.010) and females having an IR of 0.007 per 100,000 population (95% CI 0.006, 0.008).

Age-adjusted incidence rates and 95% confidence intervals by sex for CNS germ cell tumors (CBTRUS, 2006–2015)
Age-adjusted incidence rates by race in CBTRUS
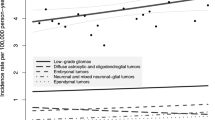
Asian and Pacific Islanders (API) had a significantly greater incidence of CNS GCT than the other race categories, with an IR of 0.136 per 100,000 population (95% CI 0.119, 0.155) (Fig. 2a–d). API IR was followed by Whites, with an IR of 0.078 per 100,000 population (95% CI 0.074, 0.081), Blacks, with an IR of 0.049 per 100,000 population (95% CI 0.041, 0.054), and American Indians/Alaska Natives (AIAN), with an IR of 0.026 per 100,000 population (95% CI 0.014, 0.047). API had a greater incidence of germinoma (IR = 0.093 per 100,000 population; 95% CI 0.079, 0.109) compared to Whites (IR = 0.052 per 100,000 population; 95% CI 0.059, 0.055), which in turn had a significantly greater IR than Blacks (IR = 0.032 per 100,000 population; 95% CI 0.027, 0.038) and AIAN (IR = 0.016 per 100,000 population; 95% CI 0.007, 0.034). Blacks had a significantly lower incidence of mixed germ cell tumors (IR = 0.004 per 100,000 population; 95% CI 0.003, 0.007) than Whites (IR = 0.008 per 100,000 population; 95% CI 0.007, 0.010) and API (IR = 0.016 per 100,000 population; 95% CI 0.010, 0.023). Incidence of benign teratoma did not vary significantly by race.

Age-adjusted incidence rates and 95% confidence intervals by race and Asian subpopulation for CNS germ cell tumors (age-adjusted for a–d) (CBTRUS 2006–2015 for panels a–d; SEER 2006–2015 for panel e)
Age-adjusted incidence rates by Asian subpopulation in SEER
Using the SEER dataset for the decade 2006–2015, the API race category was further broken down by region in Asia. These included East Asia, Southeast Asia, Polynesia, South Asia, and Other Asian. Some Asian subpopulations were excluded due to having a count of zero for the time period analyzed. Asian subpopulations included in SEER but not in by the ACS were also excluded. The excluded races are as follows: Laotian, Hmong, Kampuchean, Thai, and Pakistani. Polynesians had the highest incidence (IR = 2.246 per 100,000;95% CI 1.120, 3.758), followed by Other Asian category (IR = 1.478 per 100,000, 95% CI 0.996–2.053), Southeast Asians (IR = 0. 837 per 100,000, 95% CI 0.580, 1.142), East Asians (IR = 0.702 per 100,000, 95% CI 0.499, 0.939), and South Asians (IR = 0.111 per 100,000, 95% CI 0.023, 0.268) (Fig. 2e). However, some of the counts were small, so caution should be used while interpreting these results.
Frequencies by age at diagnosis in CBTRUS
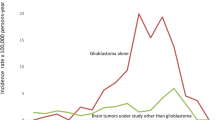
Overall, CNS GCT frequency was greatest for those age 10–14 years (24.6%) (Table 1, Fig. 3), which was followed closely by those age 15–19 years (23.3%). There was a continuous drop in frequency following 19 years of age. For germinoma, the frequency also peaked at 10–14 (28.9%) and 15–19 years of age (28.7%), with a continuous drop in frequency after 19 years of age. For mixed germ cell tumors, the frequency peaked at 10–14 years of age (35.2%), with the vast majority of patients being diagnosed between 5 and 19 years of age (73.5%). For benign teratoma, the frequencies were fairly consistent between the ages of 0 and 24 years, with a sharp drop in frequency following 24 years of age. Over half of the patients with benign teratoma were diagnosed prior to age 25 years (55.3%).

CNS germ cell tumor frequencies by age at diagnosis (CBTRUS, 2006–2015)
Primary site distribution for germinoma in CBTRUS
Because germinomas comprised the largest proportion of CNS GCT, the primary site distribution was assessed for these tumors (Supplemental Figure 1). The most common site was the pineal gland (C75.3; 42.4%), followed by other brain (C71.8–C71.9; 23.3%), the pituitary and craniopharyngeal duct (C75.1–C75.2; 7.5%), ventricles (C71.5; 6.8%)., and cerebrum (C71.0; 5.9%).
Survival using SEER
Adjusting for age at diagnosis, sex (p = 0.848) and race (p > 0.418) were not found to be significant predictors of survival of malignant GCT. However, radiation therapy status was shown to be a significant predictor of death, even after adjusting for age at diagnosis, with radiation therapy decreasing the hazard of death by 54.9% (HR = 0.451, 95% CI 0.283–0.718, p = 0.001), when compared to those with no radiation or unknown radiation status. Chemotherapy was also found to be statistically significant among all histological types. Adjusting for age at diagnosis, those who received chemotherapy were 43.1% less likely to die at any given point in time (HR = 0.569, 95% CI 0.346–0.934, p = 0.026) when compared to those with no chemotherapy or unknown chemotherapy status. There were also significant differences by histology, when controlling for age at diagnosis. Within germinoma, receiving radiation therapy decreased the hazard of death by 60.2% (HR = 0.398, 95% CI 0.173–0.913, p = 0.030), while sex and race were not significant predictors of death, controlling for age at diagnosis. However, radiation therapy was not a significant predictor of death within mixed germ cell tumors (p = 0.246) or within malignant teratoma (p = 0.777). Overall survival rates were high for malignant CNS GCT, germinoma, mixed germ cell tumors, and malignant teratoma. Median survival rates could not be obtained for these histologies since survival did not drop below the 50% rate. However, when stratifying by sex, median survival for females with malignant teratoma was found to be 52 months (95% CI 8, N/A), though this sample was fairly small (malignant teratoma n = 48; female n = 16) which may account for the survival rate this specific subgroup dropping beneath 50%. See Table 2 for all survival results.
Discussion
Our analysis presents up-to-date data on incidence and survival rates by sex, race, and age at diagnosis on CNS GCT. Because CBTRUS data include NPCR and SEER CCR data, it represents an up-to-date approximation of 100% of all CNS tumors diagnosed in the US by histology, sex, race and age at diagnosis. Therefore, the data analyzed in this study are population-based, specific, and current. CBTRUS, its major contributor NPCR, and SEER provide essential central data resources for monitoring population-level patterns of cancer. The NPCR central registries which provide data to CBTRUS, go to great lengths to only report cases for residents of their specific state, thereby eliminating the possibility of duplicate data for patients who may have traveled between states for their treatment [7]. SEER contains accurate data for survival analyses since it has been funded to collect follow-up on the cases in its dataset [7].
Germinomas comprised the largest proportion of CNS GCT in both SEER and CBTRUS data, with frequencies of 66.6% and 67.3%, respectively. These frequencies support findings from other databases reporting that germinomas account for 61–77% of all CNS GCT cases [5, 11, 20, 21].
Much like other studies, our analyses demonstrated increased incidence rates for CNS GCT in males (IR: 0.111 per 100,000) compared to females (IR: 0.038 per 100,000). A male predominance has been previously published, with reported incidence rate ratios ranging from 1.4 to 1.8 per 100,000 for all CNS GCT, and as high as 3.1 per 100.000 in malignant germinomas [1, 5, 11].
Analyses of our data sources revealed that 42.4% (CBTRUS) and 43.2% (SEER) of CNS GCT were present in the pineal region. These frequencies were similar to past data collected from SEER registries (~ 46%) and the Brain Tumor Registry of Japan (46.5%) [1, 11], although a report using the American College of Surgeons Commission on Cancer National Cancer Data Base (NCDB) data found a frequency of 78.7% of all CNS GCT being located in the pineal gland. Unlike our analysis, this hospital-based report found a frequency that was 14.4 times higher in males than in females in the pineal region but demonstrated little difference in the non-pineal regions [1]. One unfortunate aspect of the analysis of tumor location from SEER and CBTRUS registries is the outdated terminology still employed; the sellar and suprasellar/hypothalamic regions are the second most prevalent location of CNS GCT after the pineal region, but most of these, other than those ascribed to the craniopharyngeal duct location, are “lost” within the “Other” category. It is commonly impossible to separate primary tumor site within this region anterior to the third ventricle, and GCT arising in this region should be assigned to a single location.
It has been reported that incidence of GCT is highest among those with East Asian ancestry, both continentally and in the US [1, 20, 21]. Incidence rates, found in both CBTRUS and SEER databases, were highest for API followed by Whites, with incidence (CBTRUS) for API to be 0.136 per 100,000 and 0.078 per 100,000 for Whites. While it is known that incidence is highest among this demographic, there has been no previous systematic analysis done on incidence among specific Asian subpopulations within the US. Our analyses of specific Asian subpopulations found CNS GCT incidence highest among Polynesians (IR = 2.25 per 100,000, 95% CI 1.12, 3.76), followed by Other Asians, Southeast Asians, East Asians and South Asians. These specific rates exclude subpopulations not provided by the ACS, and use data provided in the SEER data, and therefore cannot be directly compared to the overall API incidence rate calculated using all of CBTRUS. Also, these excluded subpopulations are primarily present in the South and Southeast Asian regions, potentially reducing the generalizability of this results.
Analysis of CBTRUS and SEER data found that peak ages at diagnosis were age 10–14 years with frequency percentages of 24.6% and 23.6% respectively, and age 15–19 years with frequency percentages of 23.3% and 24.9% respectively. These results resembled trends found in past reports conducted on CNS GCT, which found that peak age at diagnosis occurred between ages 10 and 14 years, and then decreased over time [3, 5, 11, 17, 18].
Survival analysis using SEER data concluded that those who receive radiation and chemotherapy have better survival outcomes. Radiation treatment is highly effective in increasing survival rates for patients with germinomas, though it is less effective for those with NGGCT [3, 8, 9, 11, 13]. Unfortunately, SEER does not distinguish between receiving no radiation and missing information, as is the case with chemotherapy, so it is possible that individuals who received radiation or chemotherapy but were not documented in SEER are represented in the No/Unknown category, which is a limitation to this study. The abundance of germinomas present in the dataset is likely responsible for the significant survival advantage in receiving radiation for all GCT (HR = 0.451, 95% CI 0.283–0.718), as radiation therapy for NGGCT such as mixed germ cell tumor (HR = 0.461, 95% CI 0.124–1.707) and malignant teratoma (HR = 1.196, 95% CI 0.348–4.115) was not statistically significant.
Although the results presented here are valuable, there are some limitations. SEER collects information from 28% of the US population, thus making it difficult to extrapolate survival results to the entirety of the US. Cancer registries use multiple sources of information to identify cancer cases, including pathology and radiology used in this study. Two-thirds of CNS GCT are germinomas, which are non-secreting, require a biopsy for diagnosis [1]. Other limitations include biases from regional influences, examples of which include diagnostic practices, case definitions, or reporting patterns. Furthermore, there was no central pathology review in place for registry procedures, meaning that each case had been classified at the diagnosing institution with no central confirmation of histology at the state or national levels. The large data resources used in these analyses are also restricted by rules and regulations guiding cancer collection, some of which can change over time, and therefore can inadvertently influence trends in data.
Conclusion
CNS GCTs are rare tumors that occur with highest frequency in males, Asian populations, and children 10–14 years old at diagnosis. There is significant variation in incidence by sex, race, and age at diagnosis. Further studies will be needed to evaluate potential explanations for these differences and may lead to clues into the etiology of these rare tumors. Nonetheless, ascertaining accurate incidence and survival rates of CNS GCT at the granular level of sex, race, and age at diagnosis provides vital information usable in real time for clinicians, public health planners, patients, and their families.
References
Echevarría ME, Fangusaro J, Goldman S (2008) Pediatric central nervous system germ cell tumors: a review. Oncologist 13(6):690–699
Wong K, Opimo AB, Olch AJ, All S, Waxer JF, Clark D et al (2016) Re-irradiation of recurrent pineal germ cell tumors with radiosurgery: report of two cases and review of literature. Cureus 8(4):e585
Modak S, Gardner S, Dunkel IJ, Balmaceda C, Rosenblum MK, Miller DC et al (2004) Thiotepa-based high-dose chemotherapy with autologous stem-cell rescue in patients with recurrent or progressive CNS germ cell tumors. J Clin Oncol 22(10):1934–1943
Kim A, Ji L, Balmaceda C, Diez B, Kellie SJ, Dunkel IJ et al (2008) The prognostic value of tumor markers in newly diagnosed patients with primary central nervous system germ cell tumors. Pediatr Blood Cancer 51(6):768–773
McCarthy BJ, Shibui S, Kayama T, Miyaoka E, Narita Y, Murakami M et al (2012) Primary CNS germ cell tumors in Japan and the United States: an analysis of 4 tumor registries. Neuro Oncol 14(9):1194–1200
Khatua S, Dhall G, O’Neil S, Jubran R, Villablanca JG, Marachelian A et al (2010) Treatment of primary CNS germinomatous germ cell tumors with chemotherapy prior to reduced dose whole ventricular and local boost irradiation. Pediatr Blood Cancer 55(1):42–46
Sands SA, Kellie SJ, Davidow AL, Diez B, Villablanca J, Weiner HL et al (2001) Long-term quality of life and neuropsychologic functioning for patients with CNS germ-cell tumors: from the first international CNS germ-cell tumor study. Neuro Oncol 3(3):174–183
Jubran RF, Finlay J (2005) Central nervous system germ cell tumors: controversies in diagnosis and treatment. Oncology (Williston Park) 19(6):705–711 (discussion 711–712, 715–717, 721)
Souweidane MM, Krieger MD, Weiner HL, Finlay JL (2010) Surgical management of primary central nervous system germ cell tumors: proceedings from the second international symposium on central nervous system germ cell tumors. J Neurosurg Pediatr 6(2):125–130
Kellie SJ, Boyce H, Dunkel IJ, Diez B, Rosenblum M, Brualdi L, Finlay JL (2004) Primary chemotherapy for intracranial nongerminomatous germ cell tumors: results of the second international CNS germ cell study group protocol. J Clin Oncol 22(5):846–853
Villano JL, Virk IY, Ramirez V, Propp JM, Engelhard HH, McCarthy BJ (2010) Descriptive epidemiology of central nervous system germ cell tumors: nonpineal analysis. Neuro Oncol 12(3):257–264
Packer RJ, Cohen BH, Cooney K (2000) Intracranial germ cell tumors. Oncologist 5(4):312–320
da Silva NS, Cappellano AM, Diez B, Cavalheiro S, Gardner S, Wisoff J et al (2010) Primary chemotherapy for intracranial germ cell tumors: results of the third international CNS germ cell tumor study. Pediatr Blood Cancer 54(3):377–383
Goldman S, Bouffet E, Fisher PG, Allen JC, Robertson PL, Chuba PJ et al (2015) Phase II trial assessing the ability of neoadjuvant chemotherapy with or without second-look surgery to eliminate measurable disease for nongerminomatous germ cell tumors: a children’s oncology group study. J Clin Oncol 33(22):2464–2471
Ostrom QT, Gittleman H, Truitt G, Boscia A, Kruchko C, Barnholtz-Sloan JS (2018) CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2011–2015. Neuro Oncol 20(suppl_4):v1–v86
Surveillance Epidemiology and End Results (SEER) Program (2018) SEER*Stat software version 8.3.5. National Cancer Institute, DCCPS, Surveillance Research Program. www.seer.cancer.gov/seerstat. Accessed 18 Jan 2019
United States Census Bureau; American Community Survey, 2006–2010 American Community Survey 5-year estimates, table DP05; generated using American FactFinder. http://factfinder2.census.gov. Accessed 18 Jan 2019
United States Census Bureau; American Community Survey, 2011–2015 American Community Survey 5-year estimates, table DP05; generated using American FactFinder. http://factfinder2.census.gov. Accessed 18 Jan 2019
Nelson M(2013) dsrTest: tests and Confidence intervals on directly standardized rates for several methods. R package version 0.2.1
Goodwin TL, Sainani K, Fisher PG (2009) Incidence patterns of central nervous system germ cell tumors. J Pediatr Oncol/Hematol 31(8):541–544
Kang J, Ha J, Hong EK, Ju H, Park BK, Shin S et al (2018) A nationwide, population-based epidemiologic study of childhood brain tumors in Korea, 2005–2014: a comparison with United States data. Cancer Epidemiol Biomark Prev 28:409–416
Funding
Funding for CBTRUS was provided by the Centers for Disease Control and Prevention (CDC) under Contract No. 2016-M-9030, the American Brain Tumor Association, The Sontag Foundation, Novocure, Abbvie, the Musella Foundation, National Brain Tumor Society, the National Cancer Institute (NCI) under Contract No. HHSN261201800176P, the Zelda Dorin Tetenbaum Memorial Fund, as well as private and in kind donations. QTO is supported by a Research Training Grant from the Cancer Prevention and Research Institute of Texas (CPRIT; RP160097T). Contents are solely the responsibility of the authors and do not necessarily reflect the official views of the CDC or of the NCI.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. This study was approved as an exempt study by the University Hospitals Cleveland Medical Center Institutional Review Board.
Informed consent
This was a retrospective study using de-identified national cancer registries. Thus, formal consent was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gittleman, H., Cioffi, G., Vecchione-Koval, T. et al. Descriptive epidemiology of germ cell tumors of the central nervous system diagnosed in the United States from 2006 to 2015. J Neurooncol 143, 251–260 (2019). https://doi.org/10.1007/s11060-019-03173-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03173-4