
Abstract
The literature on medulloblastoma in adults is generally limited to case reports and retrospective series, and there is no accepted standard of care. The Cooperative Trials Group for Neuro-Oncology (COGNO) sought to determine the range and consistency of clinicians’ approaches to management as a basis for future trials. We aimed to identify current treatment strategies for adult medulloblastoma through an online survey launched at the 2012 Society of Neuro-Oncology meeting and by email invitation. Clinicians who had treated at least one adult patient with medulloblastoma, primitive neuroectodermal tumor (PNET), or pineoblastoma in the preceding year were asked about their most recent patient and invited to discuss their approach to a typical clinical scenario. Between November 2012 and January 2013, 45 clinicians (11 medical oncologists, 8 radiation oncologists, 5 pediatric oncologists, and 21 others) from Australia (24), United States (3), Europe (4) and other countries (14) completed the survey. Responding clinicians had treated 54 cases in the past 12 months. The most common histological type was medulloblastoma (64 %), then PNET (20 %). Most patients were male (68 %), and had high-risk disease (65 %). Complete surgical resection in 56 and 32 % had molecular testing. Radiotherapy was predominantly cranio-spinal (92 %) and given mostly post-resection (80 %). Combination chemotherapy was more common than single-agent chemotherapy. The choice of chemotherapy varied considerably. There is substantial variation in the treatment of adult medulloblastoma, most pronounced in the choice of chemotherapeutic agents, highlighting the need for further collaborative research to guide evidence-based treatment strategies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Medulloblastoma is a highly cellular, fast-growing, high-grade malignant embryonal neoplasm [1]. By definition, medulloblastoma arises in the posterior fossa, usually from the cerebellar vermis in the roof of the fourth ventricle. Types of medulloblastoma include classic medulloblastoma, desmoplastic nodular medulloblastoma, large-cell or anaplastic medulloblastoma, and other rare variants. PNET is a name used for tumors that are morphologically identical to medulloblastoma, but occur primarily in the cerebrum. PNET is also used sometimes to refer to rare tumors such as pineoblastoma. PNET and medulloblastoma have a marked propensity to seed within the cerebrospinal fluid (CSF) pathways, with evidence of such metastatic spread occurring in up to 35 % of cases at diagnosis [2].
Medulloblastoma accounts for 4–6 % of primary intracranial malignancies [3]. In contrast with the pediatric disease, where it is the most common malignant central nervous system (CNS) tumor, adult medulloblastoma is rare [1, 4]. The European annual incidence (world-standardized) is about 1.1 per million in men and 0.8 per million in women [5]. Adult medulloblastoma typically presents in the third or fourth decade, with a survival of 78 % at 1 year, 61 % at 3 years and 52 % at 5 years, with no gender differences [6, 7].
Current knowledge has identified a few differences between pediatric and adult medulloblastoma. These include cell of origin, tumor cell differentiation, pathologic features, localization, and responses to therapy [4, 8]. While desmoplastic histology is most frequently identified in infant and adult tumors, it is less frequent in children [9]. Also, sonic hedgehog pathway activation constitutes a feature of about 30 % of this histological subtype [4, 10].
Additionally, adult medulloblastoma has a higher incidence of late relapse, with 30 % of cases detected more than 5 years after treatment [11]. Recently, the transcriptome of adult medulloblastoma was found to differ considerably from that of pediatric counterparts, both in terms of tumor biology and prognostic impact [9].
Despite these differences, approaches to treatment are based on the pediatric experience. Studies concerning the treatment of these tumors are mostly case reports and retrospective studies, and no treatment is universally accepted.
The aim of this study was to gain insight into current views and practice regarding clinical management of adult medulloblastoma patients and explore the variations in clinical treatment of this rare tumor.
Materials and methods
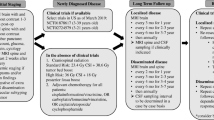
We designed an online web-based survey aimed at clinicians treating adult medulloblastoma. Respondents were asked to identify their country of residence, institution of practice, and specialty. Those who had treated one or more adult patients with medulloblastoma, PNET or pineoblastoma in the preceding year were asked to provide details of their most recent patient (Table 1).
Clinicians were also invited to discuss their management approach to a typical hypothetical clinical case scenario for a high-risk patient (Box 1). Responding clinicians could provide comments about this rare disease and feedback on the survey, with the choice of making their comments publicly available or privately noted. Cumulated results were instantly accessible by the respondents at the conclusion of the survey.
This survey was launched internationally in November 2012, promoted at the Society of Neuro-Oncology meeting and sent to 180 clinicians worldwide. It was closed on January 30 2013.
Results
Of the 180 clinicians emailed, 64 (36 %) responded. The majority were Australian (72 %), with respondents also from New Zealand (2 %), United States (6 %), United Kingdom (2 %), Denmark (3 %), Switzerland (2 %), Sweden (2 %), Argentina (2 %) and Lebanon (2 %) and 7 % from other countries.
Forty-five respondents identified their medical specialties: 11 medical oncologists (34 %), 8 radiation oncologists (21 %), 5 pediatric oncologists (19 %), 1 neurologist, and others, including 1 neurosurgeon (21 %).
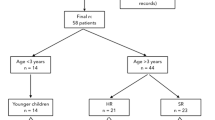
Twenty-five respondents reported on the most recent patient treated: 17 (68 %) were male, 7 female, and 1 unknown sex, and 17 (68 %) were classified as having high-risk disease. Most of the recent patients were aged 17 years or over (72 %) and had a histological diagnosis of medulloblastoma (59 %). The other histological subtypes, including PNET (27 %), pineoblastoma (6 %), and atypical histology (8 %), were less common. Interestingly, 38 % had undergone molecular testing.
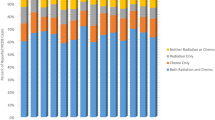
Complete surgical resection was achieved in 56 % of cases. 22 (88 %) patients received adjuvant radiotherapy, 10 (40 %) of them receiving it concurrently with chemotherapy. Standard-dose radiotherapy was more common (88 %) than hyper-fractionated dosing (12 %). Craniospinal radiotherapy was given to 23 (92 %) patients and only 2 (8 %) had cranial radiotherapy. A boost into the posterior fossa was given to 14 (56 %) patients. One of the novel treatments used was proton-beam therapy for 2 (8 %) patients.
Chemotherapy was given to all but 1 of the 25 most recent patients. Two (8 %) patients received neoadjuvant chemotherapy, 11 (44 %) received only adjuvant chemotherapy, and an additional 4 (16 %) continued with adjuvant chemotherapy after concurrent chemotherapy and radiotherapy. One (4 %) patient had maintenance or adjuvant chemotherapy following radiotherapy. Regimens used varied considerably. Vincristine, platinum, and cyclophosphamide was the most commonly used chemotherapy regimen (Table 2).
There were eight responses to the case scenario (Table 3). All 8 recommended craniospinal radiotherapy and the 3 who specified the dose delivered used around 36 Gy. Four plans were provided, which included an upfront treatment (2 recommended surgery; 1 suggested 3 cycles of ifosfamide, carboplatin and etoposide (ICE); 1, stem-cell harvesting; 1, possible stem-cell collection but noting the potential delay in radiotherapy). Adjuvant chemotherapy was recommended in six responses (2 recommended carboplatin and etoposide; 2 recommended a vincristine–based regimen; 2 did not specify the regimen).
Discussion
There are limitations inherent in a survey based research approach such as recall bias but considering the rarity of medulloblastoma in adults this survey sheds light on the approach to treating this condition. The results of our survey showed a substantial variation in the approaches adopted in managing adult medulloblastoma. Many of the strategies used are closely modelled on the pediatric literature. A major hurdle in extrapolating from pediatric data is that toxicity profiles vary greatly between children and adults, leading to dose-limiting toxicity in most adults treated on pediatric protocols. There were major variations in radiotherapy, its dose fractionation, and its mode and timing of delivery, and even more so in the choice of chemotherapy regimens, with over 10 different regimens used.
Despite the small number of responses to the case scenario, it is clear there is heterogeneity in treatment practices.
Craniospinal radiotherapy formed the backbone of any treatment regimen in PNET, followed by chemotherapy (with variation in regimen). There was some potential use of stem cell support.
Post-operative radiotherapy is usually given to the whole brain and spinal column [craniospinal radiotherapy (CSI)]. The highest radiation dose is given to the posterior fossa of the brain where the tumour originates, but a lower dose is given to the remaining brain and spinal cord tissues because of the potential risk of relapse in these regions due to tumor seeding on neural surfaces via the CSF.
There were major variations in radiotherapy, its dose fractionation, and its mode and timing of delivery, and even more so in the choice of chemotherapy regimens, with over 10 different regimens used.
Despite the small number of responses to the case scenario, it is clear there is heterogeneity in treatment. Management of patients with medulloblastoma requires a multidisciplinary approach combining the contributions of neurosurgery, neuroradiology, pediatric oncology, neuro-oncology, neurology and radiotherapy teams. The aim of treatment is, on one hand, to improve the survival rates and, and on the other hand, to avoid late side effects.
The data collected on patients and their disease characteristics were consistent with the published literature, including male-to-female predominance, the relative incidence of different histological subtypes, risk status and tumor resectability. The existing evidence for management of medulloblastoma in the adult population is based mostly on retrospective studies and case reports. A prospective phase II trial initiated in 1991 and reported in 2012 treated adult medulloblastoma patients postoperatively with 3 cycles of cisplatin and etoposide followed by craniospinal radiotherapy. After a median follow-up of 14.9 years, among a total of 28 adults with medulloblastoma, the progression-free survival and overall survival rates at 5 years were 58 % and 80 %, respectively. The median overall survival was 11.3 years. The observed toxicity was mainly hematologic, including leukopenia and thrombocytopenia (16 % were grades 3 or 4). This small series could not clarify the role of chemotherapy started before the initiation of radiotherapy in reducing recurrences, particularly distant recurrences, or increasing overall survival [12]. There are a number of other reported relevant studies in the literature but none of them can clearly provide the much-needed evidence to guide clinical practice [13–16]. There are also ongoing efforts on molecular treatment strategies in recurrent medulloblastoma with novel agents including hedgehog pathway inhibitors such as GDC-0449 (vismodegib) and LDE-225.
Due to the rarity of this disease, the populations studied have been small, and the various treatments given span decades, during which diagnostic procedures, neurosurgical skills, and radiotherapy techniques have changed. In addition, a few studies have reported risk-adapted therapeutic strategies for medulloblastoma. Despite risk-tailored treatments, 20–30 % of patients experience recurrence. Although patients could respond to second line treatments, the prognosis of patients whose disease recurs remains dismal.
Our study is the first of its kind to be conducted internationally and included respondents from five continents, shedding light on clinical practice in different parts of the world. It brings to the forefront the fact that we have no robust evidence to guide management of this rare but important disease. However, it does not take into account local guidelines and local limitations imposed by the availability and accessibility of certain diagnostic techniques and therapeutic options, including different radiotherapy technologies and chemotherapy drugs.
In feedback to the survey, comments included: “I think it is time we looked at adults differently to children and developed our own protocols, potentially with the aid of molecular testing”, “Radiation therapy to spine can limit dose intensity of subsequent chemotherapy” and “This is an uncommon problem, for which there is no clear data. A nationwide combine trial would be helpful.” These indicate the potential value of a collaborative trial for this patient group. The dilemma faced by clinicians making decisions on the management of this disease in the adult population points to the need for international collaboration to provide evidence-based management strategies and establish a standard of care for the management of these patients worldwide.
An important challenge for the future will be the biologic characterization of medulloblastoma, and the identification of specific genetic patterns carrying a better or worse prognosis. This may also lead to better treatment options by revealing potential biologic targets.
Conclusion
This study has shown substantial variation in the treatment of adult medulloblastoma, most pronounced in the choice of chemotherapeutic agents. It also provides an update on the various therapeutic approaches and outcomes based on clinicians’ experience, which could provide the cornerstone for further studies in this area.
References
Louis DN, Ohgaki H, Wiestler OD et al (2007) The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114(2):97–109
Gandhi R, Babu R, Cummings TJ, Adamson C (2013) Adult primitive neuroectodermal tumors: the prognostic value of supratentorial location. J Neuro-Oncol 114(1):141–148
Polkinghorn WR, Tarbell NJ (2007) Medulloblastoma: tumorigenesis, current clinical paradigm, and efforts to improve risk stratification. Nat Clin Pract Oncol 4(5):295–304
Korshunov A, Remke M, Werft W et al (2010) Adult and pediatric medulloblastomas are genetically distinct and require different algorithms for molecular risk stratification. J Clin Oncol 28(18):3054–3060
Parkin D, Whelan S, Ferlay J, Teppo L, Thomas D (2002) Cancer incidence in five continents. Vol. VIII. IARC Scient. Publ Lyon: International Agency for Research on Cancer, Lyon, p 155
Wong SF, Mak G, Rosenthal MA, Cher L, Gan HK (2013) Local perspective on a rare brain tumour: adult medulloblastoma. Intern Med J 43(5):567–572
Lai R (2008) Survival of patients with adult medulloblastoma: a population-based study. Cancer 112(7):1568–1574
Ang C, Hauerstock D, Guiot MÄ et al (2008) Characteristics and outcomes of medulloblastoma in adults. Ped Blood Cancer 51(5):603–607
Remke M, Hielscher T, Northcott PA et al (2011) Adult medulloblastoma comprises three major molecular variants. J Clin Oncol 29(19):2717–2723
Pfister S, Remke M, Benner A et al (2009) Outcome prediction in pediatric medulloblastoma based on DNA copy-number aberrations of chromosomes 6q and 17q and the MYC and MYCN loci. J Clin Oncol 27(10):1627–1636
Chan AW, Tarbell NJ, Black PM et al (2000) Adult medulloblastoma: prognostic factors and patterns of relapse. Neurosurgery 47(3):623–631
Silvani A, Gaviani P, Lamperti E et al (2012) Adult medulloblastoma: multiagent chemotherapy with cisplatinum and etoposide: a single institutional experience. J Neuro-Oncol 106(3):595–600
Brandes A, Franceschi E, Tosoni A et al (2009) Adult neuroectodermal tumors of posterior fossa (medulloblastoma) and of supratentorial sites (stPNET). Crit Rev Oncol Hematol 71(2):165–179
Brandes A, Franceschi E, Tosoni A et al (2007) Long-term results of a prospective study on the treatment of medulloblastoma in adults. Cancer 110(9):2035–2041
Call JA, Naik M, Rodriguez FJ et al (2014) Long-term outcomes and role of chemotherapy in adults with newly diagnosed medulloblastoma. Am J Clin Oncol 37(1):1–7
Friedrich C, von Bueren AO, von Hoff K et al (2013) Treatment of adult nonmetastatic medulloblastoma patients according to the paediatric HIT 2000 protocol: a prospective observational multicentre study. Eur J Cancer 49(4):893–903
Acknowledgments
This study was conducted under the auspices of the Cooperative Trials Group for Neuro-Oncology (COGNO), coordinated at the National Health and Medical Research Council (NHMRC) Clinical Trials Centre, University of Sydney. Special thanks to COGNO staff for coordinating the survey. This study was partly funded by the ‘Support for Cancer Clinical Trials 2013-2016’ Cancer Australia grant to the Cooperative Trials Group for Neuro-oncology (COGNO).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cosman, R., Brown, C.S.B., DeBraganca, K.C. et al. Patterns of care in adult medulloblastoma: results of an international online survey. J Neurooncol 120, 125–129 (2014). https://doi.org/10.1007/s11060-014-1525-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-014-1525-z