
Abstract
To report health-related quality of life (HRQOL) in glioblastoma (GBM) patients treated on a phase II trial of hypofractionated intensity-modulated radiotherapy (hypo-IMRT) with temozolomide (TMZ). GBM patients received postoperative hypo-IMRT to 60 Gy in 10 fractions with TMZ. HRQOL was assessed using the EORTC quality of life questionnaire core-30 and the EORTC brain cancer module, performed at baseline, RT completion, 1 mo post-RT, and every 3 mos thereafter. Changes from baseline were calculated for each specific HRQOL scale. A ≥ 10 point change in any HRQOL scale from the mean baseline score was significant. 24 patients were treated. Compliance with HRQOL assessments at baseline, RT completion, and 1, 3, 6, 9, and 12 mos post-RT was 100, 96, 92, 79, 70, 68 and 53 %, respectively. Up to 12 mos post-RT, no significant changes were seen in global health status, physical functioning, role functioning, emotional functioning, fatigue, nausea, vision, headache or seizure. Significant improvement was seen in insomnia, future uncertainty, motor dysfunction and drowsiness. Significant worsening was observed in cognitive functioning, social functioning, appetite loss and communication deficit. 60 Gy hypo-IMRT in 6-Gy fractions with TMZ does not appear to negatively impact overall HRQOL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Initial presenting symptoms, treatment-associated effects and the eventual recurrence/progression that characterizes the natural disease course for the majority of glioblastoma (GBM) patients all have significant implications for health-related quality of life (HRQOL). Quality of life in GBM is influenced by numerous factors, including neurocognitive [1, 2], social, and emotional status [2]; deterioration in quality of life has even been correlated with overall survival (OS) [3]. Understandably, patient quality of life and performance status are always important considerations guiding management decisions in GBM patients.
As the current standard treatment for GBM, surgical resection followed by radiotherapy with concurrent and adjuvant temozolomide (TMZ), is associated with a 5-year OS of only 10 %, new treatments continue to be sought. In light of the dismal prognosis for most patients with GBM, any new therapeutic strategy should be evaluated not only by its ability to prolong OS, but also to preserve quality of life [4].
We have previously reported on a phase II trial of hypo-IMRT to 60 Gy in 6-Gy fractions over 2 weeks with concurrent and adjuvant TMZ, which appeared feasible with acceptable acute and late toxicity in patients with newly-diagnosed GBM [5]. In this paper, we report on the HRQOL of patients enrolled on this trial, which was a secondary endpoint of this prospective study.
Methods and materials
Patient eligibility and treatment
The trial was a prospective phase II study approved by our institutional review board and registered with ClinicalTrials.gov (NCT00792012). Enrolled patients were ≥18 years old with histopathologically confirmed GBM, with a Karnofsky performance status (KPS) ≥60 and a maximal diameter of ≤ 6cm for the surgical cavity plus the T1-weighted enhancing residual tumor on MRI. All patients signed an institutional review board-approved study-specific informed consent. Details regarding treatment planning, study conduct and clinical outcomes have been previously reported [5]. Briefly, Planning target volume 1 (PTV1) was defined as the contrast-enhancing residual tumor on T1-weighted pre-RT brain MRI plus the entire surgical cavity with a 5-mm margin; PTV2 was defined as the abnormality on T2-weighted brain MRI with a 5-mm margin. Hypo-IMRT was prescribed to a total dose of 60 Gy in 6-Gy fractions to PTV1 and 30 Gy in 3-Gy fractions to PTV2 (10 total fractions delivered over 2 weeks). All patients were to receive concurrent TMZ with hypo-IMRT and adjuvant TMZ after hypo-IMRT. TMZ was administered orally, once daily, at 75 mg/m2, starting on the first day of hypo-IMRT and continuing for 28 consecutive days. Adjuvant TMZ was administered at 150–200 mg/m2 orally, once daily, for 5 consecutive days every 28 days, for a minimum of 6 cycles, and longer at the discretion of the treating neuro-oncologist. Patients were evaluated weekly during concurrent hypo-IMRT and TMZ, monthly during adjuvant TMZ chemotherapy, and once every 3 months thereafter.
Quality of life assessment
HRQOL was assessed using two validated, patient-reported measures which have been widely utilized in prospective clinical trials, the EORTC quality of life questionnaire core-30 version 3.0 (QLQ-C30) [6, 7] and the EORTC brain cancer module (QLQ-BN20) [8]. The QLQ-C30 is used to evaluate quality of life in cancer patients across disease sites; it employs a modular approach to gather information regarding patient-rated global health status/quality of life, physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning, as well as specific symptoms. QLQ-C30 symptom scales evaluated in our study included: fatigue, nausea/vomiting, pain, dyspnea, insomnia, and appetite loss. QLQ-BN20 was designed specifically for use in patients with brain malignancies, with scores reflecting differences in neurologic status [8]; specific QLQ-BN20 symptom scales assessed in our study included: future uncertainty, visual disorder, motor dysfunction, communication deficit, headaches, seizures, and drowsiness. Patients completed the QLQ-C30 and QLQ-BN20 prior to RT initiation and at RT completion, as well as 1 month post-RT and every 3 months thereafter, until disease progression. At follow-up visits, the questionnaires were typically administered by the study clinical research coordinator prior to physician visit, in a standardized manner. Recommended, published EORTC scoring procedures were utilized, which convert raw patient responses to scale scores ranging from 0 to 100 [9]. Higher scale scores represent favorable responses for global health status/quality of life and functional scales (i.e., role functioning), but unfavorable responses for individual symptoms (i.e., headache). If any of the items contributing to a specific scale were not completed, then the scale score was not calculated for that timepoint. At each timepoint, a ≥ 10 point change in the mean value of any HRQOL scale compared to the mean baseline score was defined as significant.
Results
Patients and compliance with HRQOL
Between January 2008 and January 2010, 24 patients were treated on the trial. Patient characteristics are listed in Table 1. All 24 received hypo-IMRT and concurrent TMZ per protocol, except for two patients who received only 14 days of TMZ; 23 patients received adjuvant TMZ with a median of 6.5 cycles (range 0–14). At a median follow-up time for all patients of 14.8 months (range 2.7–39.5), the median OS was 16.6 months (range 4.1–41.3). At the time of data analysis, four patients were still alive with OS ranging from 26.8 to 41.3 months.
Compliance with HRQOL testing (defined as number of patients completing questionnaires divided by number of eligible, surviving patients) decreased steadily post RT completion. Compliance with HRQOL assessments at baseline, RT completion, and 1, 3, 6, 9, 12, 15, 18, and 21 mos post-RT was 100 % (24/24), 96 % (23/24), 92 % (22/24), 79 % (19/24), 70 % (16/23), 68 % (15/22), 53 % (9/17), 14 % (2/14), 18 % (2/11), and 25 % (1/4), respectively. Given the dramatic drop in HRQOL compliance following the fifth follow-up visit, analyses were restricted to the first 12 months following radiotherapy.
Global health status and functional scales following hypo-IMRT
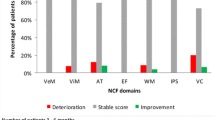
Table 2 depicts the mean baseline scale scores for all 24 patients for HRQOL functional and symptom scales. Figure 1 illustrates the changes in the mean scores for each of the functional (a) and symptom scale scores (b) over time.


Changes in the HRQOL mean scores for each of the functional a and symptom scale scores b over time
No significant change was demonstrated in the global health/quality of life score, from a mean of 75.7 (SD 15.5) prior to RT initiation to 67.7 (SD 15.7) at 12 months. The largest difference in global health from baseline was seen at the first follow-up visit at 1 month post-RT (mean score 66.3, SD 18.0, −9.4 change from baseline). The mean global health score subsequently increased to 74.1 (SD 15.1) by the second follow-up visit. No significant changes were also observed post-RT for physical functioning (largest change from baseline of −5.9 at 12 months), role functioning (largest change from baseline of −5.0 at 9 months) or emotional functioning (largest change from baseline of +6.3 at RT completion; largest drop from baseline of 2.0 at 12 months). Cognitive functioning demonstrated a significant deterioration at the fourth follow-up visit (mean score of 68.9, SD 30.1, change from baseline of −12.4). With a change in the number of respondents/surviving patients from 15/22 to 9/17, the mean cognitive functioning score at the next follow-up visit was improved by 7.0–75.9. Interestingly, social functioning was noted to be significantly improved at 6 months (mean score of 89.6, SD 18.1, change from baseline of +11.1), significantly worsened at 9 months (mean score of 67.8, SD 29.9, change from baseline of −10.7), and subsequently improved at 12 months (mean 72.9, SD 29.5, change from baseline of −5.6).
With respect to specific symptom scales, no significant change from baseline was observed for: fatigue (largest change from baseline of −5.6 at 6 months), nausea/vomiting (largest change of +7.7 at RT completion, with subsequent improvement), pain (largest change of −7.3 at 6 months), visual disorder (largest change of +5.2 at 9 months), headache (largest change of +9.3 at 9 months, improved to +4.9 at next follow-up), or seizure (largest change of +9.7 at 6 months, improved to +1.7 by 9 months). Significant improvement from pre-RT status was found for insomnia (−20.1 at third follow-up), future uncertainty (−11.7 at 3 months and −11.4 at 6 months), motor dysfunction (−11.3 at second follow-up) and drowsiness (−14.6 at 6 months). Symptoms demonstrating significant worsening included: appetite loss (+12.1 at RT completion and +11.6 at 1 month follow-up, with gradual continued improvement to −8.7 by 9 months) and communication deficit (+16.7 at 9 months and +17.9 at 12 months).
Discussion
We have previously shown that hypofractionated IMRT to 60 Gy in 6-Gy fractions over 2 weeks with concurrent and adjuvant TMZ was well tolerated without grade 3 or 4 toxicity in select GBM patients. Hypofractionated IMRT for GBM allows us to increase the biologically effective dose of the radiotherapy regimen, while holding the total radiation dose constant. The efficacy of this approach in a phase II trial with 24 patients appeared comparable to that of current standard of care therapy. Efficacy of hypofractionated RT in GBM treatment, if confirmed in future, randomized studies, may suggest a lower than expected α/β ratio for glioma cells. It might also suggest that larger fractional doses are able to make a larger therapeutic impact on glioma stem cells or tumor stromal cells/endothelium. Assessment of any new therapeutic approach for GBM, however, must take into account its impact on quality of life. In our present work, we report that our hypo-IMRT regimen does not appear to negatively impact overall HRQOL.
Taphoorn et al. [10] has reported on the HRQOL for GBM patients treated with the current standard of care (6-week) RT regimen with or without concurrent TMZ in a randomized phase III trial, utilizing the same assessment tools (EORTC QLQ-C30 and EORTC QLQ-BN20). Patients in our study appeared to have more favorable baseline scores for global health/overall QOL (mean score of 75.7 in our study versus 61.9 in the radiotherapy + TMZ group, as reported by Taphoorn), social functioning (78.5 vs. 67.4), emotional functioning (78.8 vs. 69.3), future uncertainty (27.5 vs. 39.0), and communication deficit (9.3 vs. 17.9). Other aspects of HRQOL were similar pre-treatment, including fatigue (35.2 vs. 35.2) and insomnia (30.6 vs. 27.4). As in our trial, compliance in the Taphoorn study declined post-RT, from 84 % at baseline (in the RT + TMZ group) to 69 % at fourth follow-up. Taphoorn et al. concluded from their trial that 60 Gy RT in standard fractionation with TMZ did not have a detrimental effect on HRQOL in the first year of follow-up.
The impact of radiotherapy dose escalation with standard fractionation in RTOG 98-03 on HRQOL has been reported by Corn et al. [11]. In this phase I-II study, GBM patients received RT to an initial field to 46 Gy in 2-Gy fractions, followed by a subsequent boost, up to a total dose of 66, 72, 78 or 84 Gy; concurrent and adjuvant BCNU was administered. No correlation between dose escalation and HRQOL or neurocognitive status was seen in this study.
The impact of selection bias and survivorship on serial HRQOL measurements and their close relationship with compliance must be considered when interpreting our results. Other studies evaluating HRQOL in glioma patients have shown that compliant patients have a higher likelihood of survival compared to non-compliant patients [10, 12], suggesting that “drop-out” of individuals with declining overall performance can lead to improved HRQOL average scores over time. Indeed, Taphoorn et al. found that patients with higher initial performance status remained on study longer. In our trial, patients were taken off study (and therefore no longer completed HRQOL questionnaires) at the time of disease progression. While this declining number of “more favorable” respondents likely accounts for the stable HRQOL scores observed at later timepoints, it should be noted that this phenomenon also obviously magnifies the effect of individual patient scores on the overall group average. This underscores the importance of caution when drawing conclusions regarding specific HRQOL domains.
Hypofractionated RT for GBM has been associated with increased rates of radionecrosis, which can potentially impact HRQOL. In the present study, 7/24 patients underwent repeat surgery at a median of 10.4 months post hypo-IMRT (range 1.3–37.4), with necrosis found in 50–100 % of each of the resected specimens (and ≥80 % necrosis in 5). Notably, none of these seven patients in our study were experiencing significant worsening of HRQOL prior to re-operation, and five of the seven were clinically stable. The two others were experiencing new neurologic symptoms, specifically a new visual field deficit which resolved on steroids in one case, and increased word finding difficulty along with a visual field deficit in the other. Second surgery in these patients was most often performed for diagnostic considerations (to help distinguish between radionecrosis vs. recurrent tumor). The absence of a significant clinical effect of radionecrosis on quality of life in these patients may reflect the fact that these patients often experienced a gradual increase in radiographic changes over time (ultimately prompting resection). It is reasonable to expect that more rapid progression of radionecrosis would be more likely to be accompanied by a detriment to quality of life. Furthermore, the specific location of radionecrosis is likely to contribute to the likelihood of accompanying symptoms.
One approach to the management of cerebral radionecrosis is the use of bevacizumab, an anti-VEGF antibody which has been shown to have radiographic and symptomatic benefit. Interestingly, bevacizumab has also been found to promote improved HRQOL and neurocognitive function in the setting of recurrent GBM. We are currently accruing newly-diagnosed GBM patients to a phase II trial of concurrent and adjuvant bevacizumab and TMZ along with the hypo-IMRT regimen as in the current study. Evaluation of HRQOL and neurocognitive function of enrolled patients will be performed in the same manner as the current study. Although outside the context of a randomized trial, comparison between patients enrolled on these two phase II trials may offer some insight into the effects of bevacizumab on HRQOL and neurocognitive status in GBM patients treated with hypo-IMRT in the upfront setting. Our future plans include designing a multi-institutional phase III trial randomizing patients between the hypo-IMRT regimen used in the current study and conventionally-fractionated RT concurrent with TMZ, which will include rigorous assessment of QOL and neurocognitive functioning.
Conclusion
In select GBM patients receiving hypofractionated IMRT to 60 Gy in 6-Gy fractions with concurrent and adjuvant TMZ, HRQOL appears to be maintained at a reasonable level, comparable to pre-treatment state, through 1-year follow-up.
References
Giovagnoli AR, Silvani A, Colombo E et al (2005) Facets and determinants of quality of life in patients with recurrent high grade glioma. J Neurol Neurosurg Psychiatry 76:562–568
Li J, Bentzen SM, Renschler M et al (2008) Relationship between neurocognitive function and quality of life after whole-brain radiotherapy in patients with brain metastasis. Int J Radiat Oncol Biol Phys 71:64–70
Jakola AS, Gulati S, Weber C et al (2011) Postoperative deterioration in health related quality of life as predictor for survival in patients with glioblastoma: a prospective study. PLoS ONE 6(12):e28592
Henriksson R, Asklund T, Poulsen HS (2011) Impact of therapy on quality of life, neurocognitive function and their correlates in glioblastoma multiforme: a review. J Neurooncol 104:639–646
Reddy K, Damek D, Gaspar LE et al (2012) Phase II trial of hypofractionated IMRT with temozolomide for patients with newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys 84(3):655–660
Fayers P, Bottomley A (2002) Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer 38(4):S125–S133
Aaronson NK, Ahmedzai S, Bergman B et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376
Osoba D, Aaronson NK, Muller M et al (1996) The development and psychometric validation of a brain cancer quality-of-life questionnaire for use in combination with general cancer-specific questionnaires. Qual Life Res 5:139–150
Fayers P, Aaronson N, Bjordal K et al (2001) EORTC QLQ-C30 scoring manual, 3rd edn. EORTC, Brussels
Taphoorn MJ, Stupp R, Coens C et al (2005) Health-related quality of life in patients with glioblastoma: a randomised controlled trial. Lancet Oncol 6:937–944
Corn BW, Wang M, Fox S et al (2009) Health related quality of life and cognitive status in patients with glioblastoma multiforme receiving escalating doses of conformal three dimensional radiation on RTOG 98–03. J Neurooncol 95:247–257
Walker M, Brown J, Brown K et al (2003) Practical problems with the collection and interpretation of serial quality of life assessments in patients with malignant glioma. J Neurooncol 63:179–186
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reddy, K., Gaspar, L.E., Kavanagh, B.D. et al. Prospective evaluation of health-related quality of life in patients with glioblastoma multiforme treated on a phase II trial of hypofractionated IMRT with temozolomide. J Neurooncol 114, 111–116 (2013). https://doi.org/10.1007/s11060-013-1159-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-013-1159-6