
Abstract
Purpose Temozolomide (TMZ), given concurrently with radiotherapy (RT) and as adjuvant monotherapy afterwards, has led to improved survival in glioblastoma multiforme (GBM). However, it is unclear whether its primary mechanism of action is through enhancement of radiation response, independent cytotoxicity, or both. We sought to determine the relative contribution of concomitant temozolomide in patients treated by concurrent and adjuvant TMZ versus adjuvant TMZ alone in the setting of newly diagnosed GBM. Methods and Materials We identified patients diagnosed with GBM and treated with surgery, involved-field radiotherapy, and chemotherapy at MGH between 2002 and 2004. Eligible patients received either adjuvant temozolomide alone (group 1) or temozolomide concurrently with RT followed by adjuvant TMZ (group 2). The primary endpoint of this retrospective analysis was overall survival (OS). Results Forty-three patients (group 1, n = 21; group 2, n = 22) were included in this study. The median follow-up was 33.7 months for surviving patients. There were no significant differences in baseline characteristics between these two groups. On univariate analysis, patients who received concurrent and adjuvant temozolomide experienced a 2-year OS of 51% and median survival of 25.5 months, compared with a 2-year OS of 36% and median survival of 15.6 months for group 1 patients (P < 0.05). On multivariable analysis, the hazard ratio (HR) favoring concurrent TMZ trended towards significance (HR = 0.51, P = 0.08) despite modest patient numbers. Conclusions Concurrent and adjuvant TMZ was associated with improved survival compared to adjuvant TMZ alone, highlighting the potentiation of radiation effect by temozolomide in the clinical setting.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Glioblastoma (GBM), despite aggressive surgery and radiotherapy, is almost a uniformly fatal disease. Trials of systemic chemotherapy provided mixed results but overall were disappointing [1, 2]. However, the introduction of temozolomide (TMZ) in the setting of newly diagnosed GBM has made a substantial impact in the treatment of this disease. The EORTC recently reported the results of a phase III randomized trial that showed significantly improved overall and progression-free survival in patients who received temozolomide compared to those who were managed with radiation alone [3]. Patients in the TMZ arm of the trial received concurrent low-dose temozolomide during radiotherapy and then monthly adjuvant temozolomide for 6 months or until treatment failure, resulting in an absolute 16.1% increase in survival at 2 years [3].
Despite these findings, it is unclear whether the primary benefit of temozolomide is mediated through its concurrent or adjuvant delivery. Pre-clinical evidence suggests that temozolomide acts as a radiation enhancing agent [4–6]. Therefore, it is possible that the observed survival benefit is a function of improved local control from radiation potentiation. Although temozolomide is well-tolerated, it is important to isolate the mechanism through which it exerts its effect. Thus far no clinical studies have compared the different modes of delivery of temozolomide in an attempt to distinguish this mechanism.
Glioblastoma patients at the Massachusetts General Hospital have been managed with temozolomide since 2001. Prior to 2004, temozolomide was commonly prescribed as adjuvant treatment only after the end of radiotherapy, but after the results of the phase III EORTC trial were reported, patients were treated with concurrent temozolomide as well. Since radiotherapy dose and technique were stable over this time, our experience is a natural comparison of the difference in survival between patients who receive concurrent and adjuvant TMZ (i.e., Stupp protocol [3]) versus adjuvant drug alone. We report the survival outcomes in a cohort of patients who were treated with either the Stupp protocol or adjuvant temozolomide alone.
Methods and materials
Study design
This study is a retrospective chart and radiology analysis. Data were abstracted from the electronic medical record and imaging computing system. This study was approved by the Massachusetts General Hospital (MGH) Investigational Review Board (IRB). The MGH Cancer Registry compiles a database of all patients diagnosed with a malignancy at its hospital, and the patients in this registry formed the basis of this study cohort.
Patient eligibility
Patient eligibility was strictly defined by the following characteristics. All patients had a diagnosis of glioblastoma (GBM) at MGH between 1/1/02 and 12/31/04. This time frame was selected to ensure adequate follow-up. All patients underwent surgery (and/or biopsy) at MGH, and the radiotherapy (RT) was delivered at MGH. Patients were excluded if they received less than 56 Gy of RT. Patients were required to have at least one documented post-RT follow-up visit at MGH in which the adjuvant therapy was specified.
Many patients were enrolled in a variety of clinical protocols over this time, many of which included temozolomide. Patients who received an experimental treatment in addition to TMZ were excluded, although patients who received concurrent celecoxib or rofecoxib were included. Patients who underwent RT without concurrent TMZ were assigned to the adjuvant TMZ-only arm if they received adjuvant TMZ alone after RT (group 1). Patients were assigned to the concurrent temozolomide arm (group 2) if they received daily, low-dose TMZ (75 mg/m2) with radiotherapy and then adjuvant TMZ (typically 200 mg/m2 for 5 days, repeated every 28 days). Patients who clinically progressed during radiation where treatment had to be interrupted or was incomplete were not included in this study.
Radiation treatment
All patients were treated with involved-field radiotherapy (IFRT), either in 1.8 or 2 Gy fractions using 3-dimensional conformal treatment planning, with a planned total dose of 60 Gy. Dose was in part determined by critical structure tolerance. Patients who received a stereotactic radiosurgery (SRS) or stereotactic radiotherapy (SRT) boost were excluded. One patient received a total of 61.5 Gy, in which 54 Gy was delivered to the involved field, and 7.5 Gy was given using SRT in 2.5 Gy fractions in order to meet normal tissue constraints.
Temozolomide treatment
When taken during radiotherapy, temozolomide was initially prescribed at a dose of 75 mg/m2. The majority of patients received adjuvant TMZ at a dose of 150–200 mg/m2 for 5 days every 4 weeks, but 10 patients in group 2 continued to receive daily low-dose TMZ as adjuvant therapy at 75 mg/m2 per day. For the latter group, the number of cycles was approximated by the number of months the patients were receiving the drug. The standard treatment duration at MGH was determined by the individual neuro-oncologist. In general, clinicians did not follow the Stupp protocol of 6 months of adjuvant treatment, and instead prescribed TMZ until disease progression. Toxicity during treatment was defined by the NCI Common Toxicity Criteria version 3.0.
Radiology review
Each patient’s serial MR images were reviewed by a neuroradiologist (JH) who was blinded to temozolomide status. The MRI scan closest to the start of radiation treatment was used as the baseline study. In some patients, the post-operative MRI was used as the baseline scan. Progression was defined using an adaptation of the RECIST criteria [7]. Progression was defined as an increase by 20% of the largest dimension of the tumor; measurements could be taken in the axial, sagittal or coronal planes. Non-measureable tumors were defined as masses whose largest cross-sectional dimension was less than 10 mm. Patients with no measureable disease were defined to have progressed once their tumor grew larger than 10 mm (or a satellite lesion of that size or larger developed). The appearance of new (measureable) lesions was also considered evidence of progression. Death without radiologic failure was a censoring event.
Statistical methods
The primary endpoint for this study was overall survival (OS), defined as the time between the date of resection (or biopsy, if no resection was performed) and death from any cause. The secondary endpoint for this study was progression-free survival (PFS), defined as the time between date of surgery (or biopsy) and the MRI scan indicating progression.
Baseline and treatment characteristics between group 1 and group 2 were compared using Fisher’s exact test. Differences in toxicity between the two groups were also assessed using Fisher’s exact test. Continuous variables were tested for normality, and normally distributed characteristics were compared using a t-test. Non-normal variables were compared using a Wilcoxon rank sum test.
Univariate predictors of overall survival and progression-free survival were tested using the log-rank statistic. The variable representing Karnofsky performance status (KPS) was dichotomized due to inadequate sample size in each strata.
A bivariable Cox regression model was used to evaluate OS and PFS after adjustment for RPA class, since that variable incorporates several clinical factors which are prognostic for survival. Only two covariates were included in this model due to the small number of events, and this parsimony was an attempt to avoid overfitting.
In order to address selection bias, an additional model was prepared. All patients who received concurrent temozolomide (but no other concurrent or non-TMZ adjuvant chemotherapy) were assigned to the concurrent group (group 2), whether or not they progressed during radiation treatment, irrespective of whether they received adjuvant TMZ. Group 1 was composed of all patients who did not receive concurrent temozolomide but received adjuvant TMZ, as well as all patients who did not receive concurrent or adjuvant chemotherapy (including TMZ), whether or not they progressed during radiotherapy.
SAS software (Raleigh, NC) was used for all analyses.
Results
Patient selection and follow-up
Between January 1, 2002 and December 31, 2004, a total of 107 patients were treated with surgical resection and radiotherapy at MGH for GBM and had at least 1 follow-up visit which clearly specified the delivered adjuvant therapy (as well as any concurrent chemotherapy during RT). Nineteen patients received no concurrent or adjuvant chemotherapy, 10 received concurrent TMZ only, 22 patients were given non-TMZ concurrent and/or adjuvant chemotherapy, and 12 patients received a stereotactic boost (above 60 Gy) and were, hence, excluded. One patient who was prescribed concurrent and adjuvant TMZ received 54 Gy and was excluded.
Thus, a total of 43 patients form the final study cohort. Twenty-one patients received adjuvant TMZ only (group 1), and 22 patients were treated with concurrent and adjuvant temozolomide (group 2). Ten patients in group 2 received daily adjuvant temozolomide instead of higher-dose monthly TMZ. The median follow-up time for surviving patients was 33.7 months (interquartile range 28.4–36 months).
Clinical and treatment characteristics
Baseline clinical characteristics are listed in Table 1. Although there was a trend for more favorable KPS and RPA class in group 2, these differences were not statistically significant.
Treatment characteristics are described in Table 2. Treatment variables were well distributed between these two groups, with no significant differences between them. There was a trend towards more cycles of temozolomide in group 2, but this difference was not statistically significant. Among patients who received monthly adjuvant temozolomide, the dose (mg/m2) was not significantly different (group 1 median 176 mg/m2 versus group 2 median 193 mg/m2, Wilcoxon P = 0.22). The median interval between the end of IFRT and start of adjuvant TMZ was significantly longer (Wilcoxon P = 0.004) in group 1 (30 days, IQ range 16–42 days) than group 2 (15 days, IQ range 0–21 days). This difference occurred because 6 patients receiving daily TMZ never stopped taking the medication after completing RT.
There was no significant difference between the two arms of the likelihood of undergoing salvage local or systemic therapies, although group 2 patients appeared to be more likely to undergo non-nitrosourea containing protocols.
Univariate survival analyses
Before excluding any patients from the analysis, the median survival (i.e., for all patients, n = 107) was 14.1 months, with a 2-year overall survival of 30%. After excluding patients who received no adjuvant or concurrent therapy (n = 89), the median survival was 15.4 months, with a 2-year overall survival of 35%. After restricting the analysis to patients eligible for this study (n = 43), the median survival was 21.7 months, with a 2-year overall survival of 44%.
Univariate survival analyses for the study cohort are reported in Table 3. Treatment with concurrent temozolomide was associated with a significant survival benefit (MST 25.5 months vs. 15.6 months, P < 0.05). Figure 1 displays a Kaplan-Meier graph comparing these two regimens. There was no difference in survival between patients who received daily or monthly adjuvant TMZ (log rank P = 0.4).

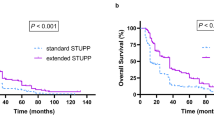
Kaplan–Meier graph of overall survival, stratified by protocol. Solid line = adjuvant temozolomide only (group 1). Dashed line = concurrent and adjuvant temozolomide (group 2). The difference between these curves was statistically significant (log-rank P < 0.05)
Younger age and non-biopsy resection status were also associated with improved survival. There was a trend for improved survival with higher KPS dichotomized at 70, but this relationship was not statistically significant.
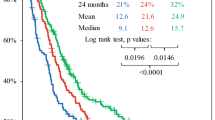
There was no significant difference in progression-free survival (group 1 MST 8.6 months vs. group 2 MST 9.7 months, P = 0.22), although there was a trend for improved progression-free survival at 2 years in the concurrent TMZ group (group 1 2-year PFS 18% vs. group 2 2-year PFS 32%). The Kaplan–Meier curves are shown in Fig. 2.

Kaplan-Meier graph of progression-free survival, stratified by protocol. Solid line = adjuvant temozolomide only (group 1). Dashed line = concurrent and adjuvant temozolomide (group 2). The difference between these curves was not statistically significant (log-rank p = 0.22)
Multivariate survival analyses
Due to the small number of events, a bivariable Cox proportional hazards model was designed to adjust for RPA class. Treatment with concurrent temozolomide was associated with a hazard ratio of 0.51 (95% CI 0.24–1.1) compared to adjuvant TMZ alone. There was a trend towards significance (P = 0.08). RPA class was associated with a hazard ratio of 2.0 (95% CI 1.3–3.1, P = 0.002). There was no significant relationship between radiographic progression and temozolomide status (HR 0.68, 95% CI 0.34–1.4, P = 0.28).
Alternate model to address selection bias
The alternate model compared patients who received any concurrent temozolomide (including patients on concurrent TMZ who progressed on treatment) with patients who did not receive concurrent TMZ and either (a) received adjuvant temozolomide alone or (b) did not receive any adjuvant temozolomide, irrespective of whether they progressed during RT. Almost all of the latter patients (16/19) did not receive adjuvant treatment because they failed during RT. On univariable analysis, concurrent temozolomide was associated with a significant improvement in overall survival (MST 21.7 months vs. 8.7 months, P = 0.02, Table 3). After adjusting for RPA class, the survival benefit associated with concurrent TMZ persisted (HR 0.45, P = 0.04).
Toxicity
Temozolomide was generally well tolerated in both groups, and toxicities are described in Table 4. There was significantly more thrombocytopenia and a non-significant increase in neutropenia in group 1. One potential explanation for the decreased toxicity in the concurrent arm (group 2) could be the administration of daily adjuvant TMZ in 10 group 2 patients, since no patient receiving that regimen experienced greater than a grade 1 toxicity. In total, there was no significant difference in the number of patients with grade 2 or higher toxicities (P = 0.54, Fisher’s exact test).
Discussion
In this highly selected cohort, we have shown that treatment with concurrent and adjuvant temozolomide was associated with a significant increase in overall survival compared to adjuvant temozolomide alone on univariate analysis. After adjustment for RPA class, this relationship maintained borderline significance. With additional follow-up, it is possible that concurrent treatment will again regain significance, as the survival curves are continuing to diverge.
These findings are consistent with pre-clinical and in vitro data which suggest that temozolomide acts as a radiation sensitizer. For example, Chakravarti et al. showed that glioma cell lines which do not express O(6)-methylguanine-DNA methyltransferase (MGMT) are significantly more susceptible to killing by radiation when the drug is given concurrent with the irradiation versus after irradiation [4]. The authors found that temozolomide enhances double-stranded DNA breaks and apoptosis after radiation, both of which could enhance radiosensitization.
It is worth noting that these clinical findings suggest but do not confirm radiosensitization. Perhaps earlier treatment with active therapy (i.e., TMZ) may delay progression and preserve performance status such that additional adjuvant treatment is more feasible. A second possibility is that TMZ and RT have independent cytotoxicities, which results in an additive versus synergistic effect. Another potential hypothesis is that 6 weeks of daily temozolomide depletes MGMT prior to adjuvant therapy, such that subsequent temozolomide is more effective. Only a randomized clinical trial can truly serve to answer this question.
Our data also bring up several other issues in the management of this disease. First, overall survival for GBM may be improving, although additional prospective studies are needed to validate this assertion. Patients who only received adjuvant temozolomide experienced a median survival of 15.5 months, which is on par with the median survival from the experimental arm of the EORTC trial [3]. The survival for patients who received TMZ according to the Stupp protocol fared extremely well, with a 2-year overall survival of 51%. Perhaps a more realistic estimate is obtained by including all patients who started on concurrent TMZ, and these patients had a 2-year overall survival of 36%. In addition, traditional prognostic factors were confirmed in our results, as low RPA class, young age and non-biopsy resection status were all favorable characteristics.
One of the strengths of this study is the relative standardization of treatment. All patients underwent surgical treatment at MGH, and the radiotherapy was planned and delivered in one department. Surviving patients have been followed for over two years, so it is unlikely that these results are due to inadequate follow-up. Since our neuro-oncologists generally started using concurrent temozolomide only after the preliminary results of the EORTC trial were released, the decision to use the drug during radiotherapy was more a function of the year of diagnosis and not patient characteristics. This natural experiment tends to reduce the influence of unmeasured confounders.
That said, this study has several limitations. First, it is a retrospective analysis and subject to the limitations of that study design. One critical issue is selection bias, as patients who were more fit were more likely to receive concurrent temozolomide; this confounding factor is seen in the bias towards slightly better RPA classes for group 2. Furthermore, selection bias likely enriched both groups for patients with more favorable disease, in part because patients were excluded if they progressed through radiation treatment and, hence, did not receive all of the planned treatment. In comparison, the EORTC randomized trial reported intention-to-treat results, including 22% of patients who never started adjuvant temozolomide. The retrospective nature of this study essentially precludes a similar intention-to-treat analysis. However, we did perform a secondary analysis which attempted to emulate an intention-to-treat analysis. The concurrent arm included all patients who started treatment with concurrent TMZ, whether or not they received adjuvant TMZ, and the adjuvant arm included all patients who received RT without concurrent TMZ, whether or not they received adjuvant TMZ. The results from this analysis were similar to the original comparison and were in fact statistically significant.
Finally, it has been shown that O(6)-methylguanine-DNA methyltransferase (MGMT) promoter methylation predicts response to temozolomide and is prognostic for survival [8, 9]. Therefore, an imbalance in MGMT methylation between the two groups could explain the apparent benefit of concurrent TMZ. Unfortunately, our institution does not test for MGMT methylation outside of prospective studies, so we could not control for that marker. However, since treatment decisions were made without knowing MGMT status, there is no a priori reason to assume there was a significant different in MGMT methylation.
In addition, patients in both groups were eligible for many other experimental protocols. Thus patients who received adjuvant temozolomide alone were either not candidates for the other protocols or chose not to enroll, which could have selected that cohort for patients with worse prognoses. However, the same argument could be made for patients in group 2, so it is unclear the extent to which selection bias could account for these results. Finally, ten patients were treated with daily adjuvant TMZ, which is not standard treatment and results in a higher overall dose intensity than monthly administration. Nevertheless their survival outcomes were not improved.
The absence of a significant relationship between treatment regimen and progression-free survival is somewhat surprising, although the general trend of improved PFS with concurrent temozolomide was consistent with the overall results. One potential explanation is the challenge of assessing radiographic progression. Necrosis and post-operative stroke can be confused with progressive disease, and the clinical picture may not be consistent with worsening disease [10].
In summary, our results are consistent with the evolving paradigm of combined-modality therapy and generally concordant with the experience from other disease sites [11–14]. It will be important to determine temozolomide’s mechanism of action, since future approaches to GBM treatment should build upon the success of this agent. If the drug primarily acts through radiosensitization, then the use of additional non-TMZ adjuvant chemotherapy should be actively investigated.
References
Fine HA, Dear KB, Loeffler JS, Black PM, Canellos GP (1993) Meta-analysis of radiation therapy with and without adjuvant chemotherapy for malignant gliomas in adults. Cancer 71:2585–2597
Medical Research Council Brain Tumor Working Party (2001) Randomized trial of procarbazine, lomustine, and vincristine in the adjuvant treatment of high-grade astrocytoma: a Medical Research Council trial. J Clin Oncol 19:509–518
Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New Engl J Med 352:987–996
Chakravarti A, Erkkinen MG, Nestler U, Stupp R, Mehta M, Aldape K, Gilbert MR, Black PM, Loeffler JS (2006) Temozolomide-mediated radiation enhancement in glioblastoma: a report on underlying mechanisms. Clin Cancer Res 12:4738–4746
Wedge SR, Porteous JK, Glaser MG, Marcus K, Newlands ES (1997) In vitro evaluation of temozolomide combined with X-irradiation. Anti-Cancer Drugs 8:92–97
van Rijn J, Heimans JJ, van den Berg J, van der Valk P, Slotman BJ (2000) Survival of human glioma cells treated with various combination of temozolomide and X-rays. Int J Radiat Oncol Biol Phys 47:779–784
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, Gwyther SG (2000) New guidelines to evaluate the response to treatment in solid tumors. European organization for research and treatment of cancer, national cancer institute of the United States, national cancer institute of Canada. J Nat Cancer Inst 92:205–216
Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, Kros JM, Hainfellner JA, Mason W, Mariani L, Bromberg JE, Hau P, Mirimanoff RO, Cairncross JG, Janzer RC, Stupp R (2005) MGMT gene silencing and benefit from temozolomide in glioblastoma. New Engl J Med 352:997–1003
Krex D, Klink B, Hartmann C, von Deimling A, Pietsch T, Simon M, Sabel M, Steinbach JP, Heese O, Reifenberger G, Weller M, Schackert G (2007) Long-term survival with glioblastoma multiforme. Brain 130:2596–2606
Ulmer S, Braga TA, Barker FG 2nd, Lev MH, Gonzalez RG, Henson JW (2006) Clinical and radiographic features of peritumoral infarction following resection of glioblastoma. Neurology 67:1668–1670
Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, Kish JA, Kim HE, Cmelak AJ, Rotman M, Machtay M, Ensley JF, Chao KS, Schultz CJ, Lee N, Fu KK (2004) Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. New Engl J Med 350:1937–1944
Dillman RO, Seagren SL, Propert KJ, Guerra J, Eaton WL, Perry MC, Carey RW, Frei EF 3rd, Green MR (1990) A randomized trial of induction chemotherapy plus high-dose radiation versus radiation alone in stage III non-small-cell lung cancer. New Engl J Med 323: 940–945
Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA (2001) Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. New Engl J Med 345:725–730
Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, Rotman M, Gershenson DM, Mutch DG (1999) Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. New Engl J Med 340:1137–1143
Acknowledgements
We gratefully acknowledge the statistical support of Alona Muzikansky and Gregory DiRienzo, PhD.
Author information
Authors and Affiliations
Corresponding author
Additional information
Statement of originality: This work is completely original and has not been published or presented elsewhere.
John W. Henson and Bindu Avutu contributed equally to this publication.
Rights and permissions
About this article
Cite this article
Sher, D.J., Henson, J.W., Avutu, B. et al. The added value of concurrently administered temozolomide versus adjuvant temozolomide alone in newly diagnosed glioblastoma. J Neurooncol 88, 43–50 (2008). https://doi.org/10.1007/s11060-008-9530-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-008-9530-8