
Abstract
Background To analyze retrospectively the results of treatments for patients with brain metastases from breast cancer. Materials and Methods The records of 65 breast cancer patients with brain metastases who were treated between 1985 and 2005 were reviewed. For brain metastases, 11 patients (17%) were treated with surgical resection followed by radiotherapy, and the remaining 54 patients were treated with radiotherapy alone. Systemic chemotherapy was also administered to 11 patients after brain radiotherapy. Results The overall median survival for all patients was 6.1 months (range, 0.4–82.2 months). In univariate analysis, treatment modality, Karnofsky performance status (KPS), administration of systemic chemotherapy, extracranial disease status and total radiation dose each had significant impact on overall survival, and in multivariate analysis, treatment modality, KPS and administration of systemic chemotherapy were significant prognostic factors. Eight patients survived for more than 2 years after the diagnosis of brain metastases, and all these patients were treated with surgical resection and/or systemic chemotherapy in addition to radiotherapy. For the 45 patients treated with palliative radiotherapy (without systemic chemotherapy), the improvements in neurological symptoms were observed in 35 patients (78%), with the median duration of improvement of 3.1 months (range, 1.5–4.4 months). Conclusions The prognoses for patients with brain metastases from breast cancer were generally poor, although selected patients may survive longer with intensive brain tumor treatment, such as surgical resection and/or systemic chemotherapy in addition to brain radiotherapy. For patients with unfavorable prognoses, palliative radiotherapy was effective in improving the quality of the remaining lifetime.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Brain metastases represent an important cause of morbidity and mortality, and are the most common intracranial tumors in adults [1]. Despite numerous studies designed to improve treatment outcome, a median survival of 3–6 months has been reported [2, 3]. The risk of developing brain metastases varies according to primary tumor type, with breast cancer accounting for approximately 10–20% of all brain metastases, making breast cancer the second most common source of brain metastases [4–6].
Recently, advances in neuroimaging, such as computed tomography (CT) scans and magnetic resonance imaging (MRI) have allowed careful monitoring of cancer patients. This fact, along with the increased survival of patients, has led to more frequent and earlier detection of brain metastases, and number of published clinical reports on treatment of brain metastases has gradually increased. However, most of the large studies have been dominated by cases of brain metastases from lung cancer [7, 8], and the optimal management for brain metastases from breast cancer has not yet been fully investigated. Identification of subgroups of patients with substantially different outcomes is, thus, mandatory to enable tailoring of optimal therapy and to influence the stratification of future clinical trials. In the current study, we retrospectively analyzed the results of treatment for brain metastases from breast cancer, and identify the factors that influence the prognosis of these patients.
Materials and methods
Patient population
A retrospective review of medical records identified 65 patients with documented brain metastases from breast cancer between 1985 and 2005. In all patients, brain metastases were diagnosed by contrast-enhanced CT scans or, more recently, CT scans and/or MRI. In addition, 11 patients (17%) had histologic confirmation of their diagnosis after undergoing surgical resection of the brain lesion. All patients underwent a primary medical evaluation including a detailed history, review of symptoms, and physical examination before a treatment plan was formulated, and follow-up information was obtained from the patients’ records or from communications with patients or their physicians.
Treatment for brain metastases
For brain metastases, 11 patients (17%) were treated with surgical resection followed by radiotherapy (S + RT), and the remaining 54 patients were treated with radiotherapy alone (RT).
Radiotherapy was administered by a 4-MV, 6-MV, or 10-MV linear accelerator, and daily fraction sizes of 2–3 grays (Gy) 5 days per week were used. Stereotactic radiosurgery was not applied. Four patients received localized field radiotherapy alone (median 40 Gy, dose range 30–60 Gy), 57 patients received whole brain radiotherapy (WBRT) alone (median, 30 Gy; dose range, 3–50 Gy), and the remaining 4 patients received WBRT (40 Gy in 20 fractions) followed by a local boost using the appropriate technique (median, 53 Gy, dose range, 49–60 Gy). The median doses were 40 Gy (range, 24–60 Gy) for the S + RT group and 30 Gy (range, 3–60 Gy) for the RT group. Corticosteroids in individualized doses were given during radiotherapy.
After brain tumor treatment (S + RT group: 2 patients; RT group: 9 patients), 11 patients received systemic chemotherapy. Chemotherapy consisted of 4-week courses of cyclophosphamide, methotrexate, and 5-fluorouracil (CMF) in 1 patient, 3–4-week course of cyclophosphamide, doxorubicin, and 5-fluorouracil (CAF) in 5 patients, one-week courses of cisplatin (CDDP) in 1 patient, 3-week courses of paclitaxel/docetaxcel (TXN) in 3 patients and combination of TXN, cyclophosphamide and adriamycin (CA) in 1 patient. Table 1 indicates the administered chemotherapy regimens before and after the diagnosis of brain metastases in 11 patients.
Statistical analysis
In this study, the following potential prognostic factors affecting survival were analyzed: age (<50 years or ≥50 years), Karnofsky performance status (KPS; ≥70% or <70%), extracranial disease status (active or inactive), number of brain metastases (single or multiple), greatest dimension of brain metastases (≤3 cm or >3 cm), interval between diagnosis of primary and brain metastases (≤2 years or >2 years), treatment modality for brain metastases (S + RT or RT), total radiation dose (<50 Gy or ≥50 Gy), and use of systemic chemotherapy after radiotherapy (yes or no). Patients were considered to be without evidence of active extracranial disease if there were no metastases outside the brain and the primary tumor was controlled.
In 1997, Gasper et al. published a recursive partitioning analysis (RPA) of three Radiation Therapy Oncology Group (RTOG) studies: Class 1: patients with a KPS ≥ 70, age < 65 years with controlled primary disease and no evidence of extracranial metastases; Class 3: patients with a KPS < 70; and Class 2; all remaining patients who did not fit into Class 1 or 3 [9]. To ascertain whether this scoring system also may be applicable for patients with brain metastases from breast cancers, the patients were grouped into these three classes and analyzed.
All data were updated to March 2007. Overall survival rate was calculated actuarially according to the Kaplan–Meier method [10] and were measured from the date of diagnosis of brain metastases until the date of last follow-up or until death. Differences between groups were estimated using the log-rank test [11]. Multivariate analysis was performed using the Cox regression model [12]. A probability level of 0.05 was chosen for statistical significance. Statistical analysis was performed using the SPSS software package (version 11.0; SPSS, Inc., Chicago, IL).
Results
Patient characteristics
At the time of initial diagnosis of breast cancer, the median patient age was 45 years (range, 31–73 years). All patients had histologic confirmation of their primary lesion. At the time of initial primary treatment, 44 patients had pathological T1-T2 stage tumors, and 21 patients had pathological T3-T4 stage tumors. Concerning nodal involvement, 21 patients had axillary node-negative disease, and 44 patients had axillary node-positive diseases.
At the time brain metastases appeared, the median age was 50 years (range, 32–75 years), and the median KPS was 60% (range, 30–100%). The presented signs and symptoms were headache in 30 patients (46%), motor weakness in 25 patients (38%), nausea and vomiting in 6 patients (9%), gait disturbance in 3 patient (5%), disorientation in 3 patients (5%), seizures in 3 patients (5%) and speech disturbance in 2 patients (3%). All patients underwent chest radiographs, chest CT scans and abdominal CT scans. About 61 of 65 patients (94%) underwent radionucleotide bone scans. Extracranial disease status was active in 53 patients (82%; 2 patients with chest wall recurrence, 2 patients with lymph node recurrence, 11 patients with bone metastases, 7 patients with lung/pleura metastases, and 31 patients with multiple site metastases). The median interval between the diagnoses of primary tumor and brain metastases was 26 months (range, 0–98 months). A total of 13 patients (20%) had an single brain metastases, and 11 patients (17%) had brain metastases with a greater dimension > 4 cm.
Survival and prognostic factors
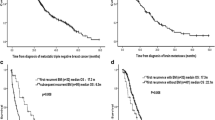
The overall median survival was 6.1 months (range, 0.4–82.2 months). The actuarial survival rates at 12 months and 24 months were 28% and 12%, respectively (Fig. 1). With respect to treatment modality, the median survival was 19.3 months (range, 4.8–82.2 months) for patients in the S + RT group and 4.8 months (range, 0.4–50.3 months) for patients in the RT group. In univaraiate analysis, treatment modality, KPS, extracranial disease status, number of brain metastases, systemic chemotherapy and total radiation dose each had a statistically significant impact on overall survival (Table 2). In multivariate analysis, treatment modality, KPS and administration of systemic chemotherapy were significant prognostic factors for overall survival. No significant differences in survival were seen with respect to other factors.

Actuarial overall survival curves for 65 patients with brain metastases from breast cancer
With regard to brain metastases-progression/recurrence-free survival, treatment modality, KPS, extracranial disease status, number of brain metastases, systemic chemotherapy and total radiation dose each had a statistically significant impact on overall survival in univariate analysis, and treatment modality, KPS and administration of systemic chemotherapy were significant prognostic factors in multivariate analysis (Table 2).
Cause of death according to treatment modality
For the assessment of the cause of death by treatment modality, patients were grouped according to treatment modality: patients undergoing S + RT group (n = 11, including 2 patients treated with systemic chemotherapy); patients undergoing RT with systemic chemotherapy (n = 9); and patients undergoing RT without systemic chemotherapy (n = 45). Table 3 indicates the incidences and causes of death according to treatment modality. Patients treated with S + RT or RT with systemic chemotherapy usually died of recurrent/regrowth progressive brain metastases, while more than half of the patients treated with RT without systemic chemotherapy usually died of active systemic diseases.
Long-term survivors
About 8 patients survived for more than 2 years after the diagnosis of brain metastases (median 32.8 months, range: 27–82.2 months). Seven of eight patients (88%) had a KPS of 0–1 and all 8 patients were treated with surgical resection (4 patients) or systemic chemotherapy (4 patients) in addition to 30–50 Gy brain radiotherapy (median, 50 Gy).
Analysis of RTOG RPA Class
When grouped according to RTOG RPA classification, as proposed by Gasper et al. [9], the median survival was 25.5 months for patients in RPA class I, 10.6 months for patients in RPA class II and 3.3 months for patients in RPA class III. About seven of 65 patients fell into RPA class I, 23 patients fell into RPA class II and 35 patients fell into RPA class III. There was a statistically significant difference in survival among these groups (P < 0.001). Compared with the results of RTOG reports, the median survival for patients with RPA Class I (3 of 7 patients were treated with S + RT) was superior to the median survival for patients in the S + RT study reported by Agboola et al. [13] (median survival for patients in RPA Class I, 14.8 months). The median survival for patients in RPA Class II (3 of 23 patients was treated with S + RT) was superior to the median survival of patients in the RT study by Gasper et al. [9, 14] (median survival of patients in RPA Class II, 3.8–4.2 months). On the other hand, the median survival for patients in RPA Class Class III (5 of 35 patients was treated with S + RT) was comparable to the median survival of patients in the RT study by Gasper et al [9, 14] (median survival of patients in RPA Class III, 2.3 months).
Improvement and duration of neurological symptoms after brain tumor treatment
For the assessment of the improvements of neurological symptoms by treatments, patients were grouped according to treatment modality: patients undergoing S + RT (n = 11, including 2 patients treated with systemic chemotherapy); patients undergoing RT with systemic chemotherapy (n = 9); and patients undergoing RT without systemic chemotherapy (n = 45). For 11 patients treated with S + RT, the improvements in neurological symptoms, including headache, motor weakness, seizures and cerebellar dysfunction, were observed in 11 patients (100%) with the median duration of improvement was 13.2 months (range, 3.5–82.2 months). For 9 patients treated with RT and systemic chemotherapy, the improvements in neurological symptoms were observed in 8 patients (89%) with the median duration of improvement was 12 months (range, 2.5–50.3 months). For the 45 patients treated with RT without systemic chemotherapy, the improvements in neurological symptoms were observed in 35 of patients (78%) with the median duration of improvement was 3.7 months (range, 0.4–11.8 months).
Discussion
Brain metastases have been a major detrimental event in the natural history of most malignancies. In the majority of patients, the treatment of brain metastases is a palliative measure, because the primary disease is sometimes advanced, and the general condition of the patients often is poor. Concerning patients with brain metastases from breast cancer, a median survival of 3–6 months has been reported [5, 15, 16]. In the current study, the median survival of 6.1 months was comparable to the results of the previous reports. Therefore, our results as well as previous reports indicated that the prognoses of patients with brain metastases from breast cancer were generally poor.
Concerning prognostic factors, our results indicated that treatment modality was an independent prognostic factor. It has now been established clearly that achieving local control in the brain improves the survival of selected patients [17]. Two randomized trials that excluded patients with multiple brain metastases showed that surgical resection plus radiotherapy was significantly better than radiotherapy alone [7, 18]. Stereotactic radiosurgery also has provided local control equivalent to those from surgical series and has facilitated the treatment of patients with surgically inaccessible or multiple lesions [19, 20]. In our study, the prognosis of the patients treated with S + RT was significantly better than those treated with RT. Saito et al. also indicated that surgery followed by whole brain radiotherapy yielded better survival rates than whole brain radiotherapy alone [21]. These results indicated that intensive brain tumor treatment, such as S + RT, may provide better results for patients with brain metastases from breast cancers.
Our results also suggest that patients have significant benefits from systemic chemotherapy after brain radiotherapy in terms of brain-progression/recurrence-free survival. Previously it was generally considered that systemic chemotherapy could not be effective against central nervous system tumors, because the blood–brain barrier would preclude significant penetration of antineoplastic drugs into brain tumor tissue. However, based on a number of profound studies, it now is generally agreed that the integrity of the blood–brain barrier varies widely in different regions of malignant brain tumors, resulting in an impaired or absent barrier function in large areas of the tumor vasculature [22–24]. This suggests that the effects of chemotherapy on brain tumors may be more dependent on the chemosensitivity of the tumor than on the ability of the drugs to cross an intact blood–brain barrier. Supporting this hypothesis are the results of a clinical study in patients with breast cancer with brain metastases showing an effective response of systemic and neurologic disease to systemic chemotherapy, with a neurologic response in 50% of the patients and an overall median survival time of 5.5 months [25].
Regarding overall survival, our results indicated that the administration of systemic chemotherapy after radiotherapy was an independent prognostic factor. Bartsh et al. [26] also indicated that systemic chemotherapy significantly prolonged not only cerebral time to progression but also overall survival. Brain metastases from breast cancer are usually associated with active extracranial diseases, and the fact that approximately 50% of patients with brain metastases die of active extracranial deisease illustartes the need for improved therapy for all metastatic diseases, as well as for brain metastases [5]. A possible explanation of the favorable results seen in the patients treated with systemic chemotherapy may be that systemic chemotherapy was active against to not only the brain metastases from breast cancer but also to active extracranial diseases [27]. Several reports indicated that most of the patients with an unfavorable prognosis died of extracranial disease, whereas a substantial subgroup with a favorable prognosis usually died of brain metastases, which determined the length of survival [28–30]. In the current study, most of the patients treated with systemic chemotherapy died from brain metastases (75%) while greater than half of the patients treated with palliative radiotherapy alone died front extracranial diseases (56%) (Table 2). Further studies are required to determine whether systematic chemotherapy could be effective in prolonging the time to progression of not only brain metastases but also extracranial diseases.
The other prognostic factors that affect survival outcomes have been identified in patients with brain metastases, including age, KPS, number of brain metastases, tumor size, performance status and the presence of extracranial metastases [31]. Our results indicated that KPS was an independent prognostic factor in overall survival. Several other authors also indicated that KPS was a significant prognostic factor for survival in patients with brain metastases from breast cancer [16, 21, 26, 31–34]. Furthermore, most of the long-term survivors have been reported to have a KPS of 0–1 [16, 32, 33, 35]. On the other hand, our results found no significant differences in overall survival with respect to extracranial disease status. An explanation for the insignificant difference regarding extracranial disease status may be that systemic chemotherapy after radiotherapy prolonged survival in some patients with active systemic diseases. Additional studies with a larger number of patients are required to determine whether these factors would be prognostic factors.
We have experienced 8 patients who survived for more than 2 years after the diagnosis of brain metastases. About seven of the 8 patients (88%) had a KPS of 0–1 and all 8 patients were treated with surgical resection (4 patients) or systemic chemotherapy (4 patients) in addition to 30–50 Gy brain radiotherapy (median, 50 Gy). With respect to the RPA Class, the median survival for patients in RPA Class I (who were treated with S + RT) was 25.5 months, which was superior to that of the previous S + RT study (median survival, 14.8 months) [13]. In selected patients who may profit from effective local tumor control in the brain, such multimodal treatments may provide better results for patients with brain metastases from breast cancers.
Our results indicated that for patients with unfavorable prognoses, palliative radiotherapy was effective in improving the quality of the remaining lifetime as well as those frequently seen from other primaries. It has been well-established that whole brain radiotherapy is effective in the palliation of symptoms resulting from intracranial metastases [36]. The results of the first two RTOG metastatic brain studies, which mainly incorporated patients with metatatic lung and breast cancer, suggested that the administration of whole brain radiotherapy could improve neurologic function in 50% of patients; 70–80% of patients spent their remaining lifetime in an improved or stable neurologic state [3]. Yamada et al. [15] analyzed 39 patients with brain metastases from breast cancer and the relief of specific neurologic symptoms was observed in 80%. In the current study, for the 43 patients treated with radiotherapy without systemic chemotherapy, the improvements of neurological symptoms were observed in 34 of patients (79%) with the median duration of improvement was 3.7 months (range, 0.4–11.8 months). These results indicated that for breast cancer patients with unfavorable prognosis, palliative whole brain radiotherapy was effective in improving the quality of the remaining lifetime as well as those frequently seen from other primaries
In conclusion, our results indicated that the prognoses for patients with brain metastases from breast cancer were generally poor, although selected patients may survive longer with intensive brain tumor treatment and/or systemic chemotherapy. Our results also indicated that for patients with unfavorable prognoses, palliative radiotherapy was effective in improving the quality of the remaining lifetime. However, this study was a retrospective study comprising a relatively small number of patients, and further prospective studies with a larger number of patients are necessary to confirm our results.
References
Loeffler JS, Patchell RA, Sawata R (1997) Metastatic brain tumor. In: Devita VT Jr, Hellman S, Rosenberg SA (eds) Cancer: principles and practice of oncology, 5th edn. Lippincott-Raven, Philadelphia, pp 2523–2536
Phillips TL, Scott CB, Leibel SA et al (1995) Results of a randomized comparison of radiotherapy and bromodeoxyuridine with radiotherapy alone for brain metastases: report of RTOG trial 89–05. Int J Radiat Oncol Biol Phys 33:339–348
Borgelt B, Gelber R, Kramer S et al (1980) The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 6:1–9
Lee YT (1983) Breast carcinoma: pattern of metastasis at autopsy. J Surg Oncol 23:175–180
DiStefano A, Yong Yap Y, Hortobagyi GN et al (1979) The natural history of breast cancer patients with brain metastases. Cancer 44:1913–1918
Chang EL, Lo S (2003) Diagnosis and management of central nervous system metastases from breast cancer. Oncologist 8:398–410
Patchell RA, Tibbs PA, Walsh JW et al (1990) A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 322:494–500
Zimm S, Wampler GL, Stablein D et al (1981) Intracerebral metastases in solid-tumor patients: natural history and results of treatment. Cancer 48:384–394
Gaspar L, Scott C, Rotman M et al (1997) Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 37:745–751
Kaplan EL, Meier P (1985) Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457–481
Mantel N (1966) Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 50:163–170
Cox DR (1972) Regression models and life tables. J R Stat Soc 34:187–220
Agboola O, Benoit B, Cross P et al (1998) Prognostic factors derived from recursive partition analysis (RPA) of Radiation Therapy Oncology Group (RTOG) brain metastases trials applied to surgically resected and irradiated brain metastatic cases. Int J Radiat Oncol Biol Phys 42:155–159
Gaspar LE, Scott C, Murray K et al (2000) Validation of the RTOG recursive partitioning analysis (RPA) classification for brain metastases. Int J Radiat Oncol Biol Phys 47:1001–1006
Yamada K, Murakami M, Kuroda Y (1997) Treatment results of brain metastases from breast cancer: course of the disease and radiation therapy. Nippon Igaku Hoshasen Gakkai Zasshi 57:34–40 (in Japanese)
Boogerd W (1996) Central nervous system metastases in breast cancer. Radiother Oncol 40:5–22
Wronski M, Arbit E, McCormick B (1997) Surgical treatment of 70 patients with brain metastases from breast carcinoma. Cancer 80:1746–1754
Vecht CJ, Haaxma-Reiche H, Noordijk EM et al (1993) Treatment of single brain metastasis: radiotherapy alone or combined with neurosurgery? Ann Neurol 33:583–590
Breneman JC, Warnick RE, Albright RE et al (1997) Stereotactic ardiosurgery for the treatment of brain metastases. Results of a single institution series. Cancer 79:551–557
Adler JR, Cox RS, Kaplan I et al (1992) Stereotactic radiosurgical treatment of brain metastases. J Neurosurg 76:444–449
Saito EY, Viani GA, Ferrigno R et al (2006) Whole brain radiation therapy in management of brain metastasis: results and prognostic factors. Radiat Oncol 1:20
Workman P (1986) The pharmacology of brain tumour chemotherapy. In: Bleehen NM (ed) Tumours of the brain. Springer-Verlag, Berlin, pp 183–200
Greig NH (1989) Brain tumors and the blood-brain barrier. In: Neuwelt EA (ed) Implications of the blood–brain barrier and its manipulation, Vol 2. Plenum, New York, pp 77–106
Fortin D, Gendron C, Boudrias M et al (2007) Enhanced chemotherapy delivery by intraarterial infusion and blood–brain barrier disruption in the treatment of cerebral metastasis. Cancer 109:751–760
Rosner D, Nemoto T, Lane WW (1986) Chemotherapy induces regression of brain metastases in breast carcinoma. Cancer 58:832–839
Bartsch R, Fromm S, Rudas M et al (2006) Intensified local treatment and systemic therapy significantly increase survival in patients with brain metastases from advanced breast cancer-a retrospective analysis. Radiother Oncol 80:313–317
Boogerd W, Dalesio O, Bais EM et al (1992) Response of brain metastases from breast cancer to systemic chemotherapy. Cancer 69:972–980
Boogerd W, Vos VW, Hart AAM et al (1993) Brain metastases in breast cancer; natural history, prognostic factors and outcome. J Neurooncol 15:165–174
Colleoni M, Graiff C, Nelli P et al (1997) Activity of combination chemotherapy in brain metastases from breast and lung adenocarcinoma. Am J Clin Oncol 20:303–307
Snee MP, Rodger A, Kerr GR (1985) Brain metastases from carcinoma of breast: a review of 90 cases. Clin Radiol 36:365–367
Ogura M, Mitsumori M, Okumura S et al (2003) Radiation therapy for brain metastases from breast cancer. Breast Cancer 10:349–355
Lentzsch S, Reichardt P, Weber F et al (1999) Brain metastases in breast cancer: prognostic factors and management. Eur J Cancer 35:580–585
Mahmoud-Ahmed AS, Suh JH, Lee SY et al (2002) Results of whole brain radiotherapy in patients with brain metastases from breast cancer: a retrospective study. Int J Radiat Oncol Biol Phys 54:810–817
Le Scodan R, Massard C, Mouret-Fourme E et al (2007) Brain metastases from breast carcinoma: validation of the Radiation Therapy Oncology Group recursive partitioning analysis classification and proposition of a new prognostic score. Int J Radiat Oncol Biol Phys doi: 10.1016/j.irobp.2007.04.024
Kocher M, Muller RP, Staar S et al (1995) Long-term survival after brain metastases in breast cancer. Strahlenther Onkol 171:290–295
Kurtz JM, Gelber R, Brady LW et al (1981) The palliation of brain metastases in a favorable patient population: a randomized clinical trial by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 7:891–895
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ogawa, K., Yoshii, Y., Nishimaki, T. et al. Treatment and prognosis of brain metastases from breast cancer. J Neurooncol 86, 231–238 (2008). https://doi.org/10.1007/s11060-007-9469-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-007-9469-1