
Abstract
We report a case of primary cutaneous mucormycosis caused by Mucor irregularis. A 52-year-old male farmer was presented to our hospital with a history of progressive nodule and plaque with ulceration on the face for two and a half years. Broad, aseptate hyphae were seen in direct KOH examination and biopsy. Fungal culture showed light yellow filamentous colonies. The rRNA sequencing revealed M. irregularis was the responsible fungus. Amphotericin B in gradually increasing dose and itraconazole were administered. When the cumulative dose of amphotericin B was 1500 mg, the skin lesion improved significantly with remaining scars on the face. Then, the patient received sequential oral itraconazole treatment for 8 months. There was no recurrence up to now through follow-ups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mucor irregularis infection is a rare disease mainly described in Asia which usually presents progressive skin lesions without systemic involvement [1]. Although the prognosis is usually good, it can leave severe cosmetic damage [2]. In this article, we report a case of disfiguring skin infection caused by M. irregularis that was cured by amphotericin B and itraconazole and share our treatment experience.
Case Report
A 52-year-old farmer was presented to our clinic on May 15, 2018, with the history of progressive nodule and plaque with ulceration on the face for two and a half years. Two and a half years ago, a peanut-sized red nodule appeared on the bridge of the nose with no apparent cause and enlarged gradually. The patient had symptoms of nasal congestion, runny nose, headache and fatigue. The palate perforated 2 years ago. The skin pathology from the local hospital showed fungal infection. Itraconazole capsules were given orally, and the lesion improved partially. Later, the plaque continued to progress and ulcerate. The patient was in good health with no diabetes before. His grandfather and cousin had history of cutaneous tuberculosis which had been cured.
On physical examination, a red, symmetrical plaque was seen on the patient’s face, covered by oyster-like thick scales with relatively clear boundary. There was a little purulent exudation on the surface of the plaque. The nasal tip, alar, septum and uvula were absent (Fig. 1a–c). There was a perforation on the palate.

A red, symmetrical plaque covered by oyster-like thick scales and a little purulent excretion, with relatively clear boundary. The nasal tip, alar and septum were absent (a full face, b right face, c left face)
Diagnosis and Treatment
The blood routine, liver and kidney function and immune function were normal. Sinus computed tomography imaging showed sinusitis in all sinuses.
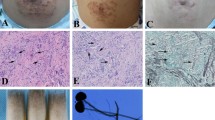
Direct KOH examination and fluorescence stain showed linear, aseptate hyphae with right-angled branching (Fig. 2a). Histopathologic examination [hematoxylin–eosin (HE) (Fig. 2b) and periodic acid–Schiff (PAS) stain (Fig. 2c)] revealed aseptate hyphae in the dermis, surrounded by mixed granulomatous infiltrates. Immunohistochemistry examination showed that the hyphae were bound to anti-Rhizopus arrhizus antibody but not to anti-Aspergillus antibody (Fig. 2d, e), which could distinguish from Aspergillus. Fungal culture of the tissue revealed light yellow filamentous colonies after 2 weeks of incubation in Sabouraud dextrose agar (SDA) at 28 °C (Fig. 2f). Microscopy observations showed abundant rhizoids, branched sporangiophores and ruptured sporangia with unequal-sized sporangiospores (Fig. 2g). The ITS regions of ribosomal DNA of the strain were sequenced. A BLAST search of the NCBI GenBank database showed that the isolated pathogen had 100% homology with that of R. variabilis (M. irregularis) (GenBank Accession No. EF583637.1).

a Direct KOH examination showed linear, aseptate hyphae with right-angled branching (KOH, fluorescence stain, × 400). b Histopathologic examination showed mixed granulomatous infiltrates (hematoxylin and eosin (HE) stain, × 100) and c ribbon-like, hyaline and aseptate hyphae in the dermis (periodic acid–Schiff (PAS) stain, × 400). d Immunohistochemistry examination showed that the hyphae could bound to anti-Rhizopus arrhizus antibody e but not to anti-Aspergillus antibody. f Light yellow filamentous colony grown on Sabouraud dextrose agar (SDA) after 2 weeks at 28 °C. g Microscopy observations showed abundant rhizoids, branched sporangiophores and ruptured sporangia with unequal-sized sporangiospores (× 200)
According to the clinical manifestation, morphological features and molecular identification, the patient was diagnosed as primary cutaneous mucormycosis caused by M. irregularis. Intravenous amphotericin B of gradually increasing dose was given. The initial dose was 1 mg/day, and the maximum dose was 25 mg/day. When the dose increased at 15 mg/day, central venous infusion was used to reduce the adverse drug effects on blood vessels. The examinations of blood routine, liver and kidney functions, electrolytes and electrocardiogram were performed per week. The adverse drug reactions during treatment were as follows: (1) hypokalemia: the lowest serum potassium level was 3.17 mmol/L, and it was corrected by taking potassium chloride sustained-release tablets 1.5 g/day combined with potassium citrate 60 ml/day; and (2) phlebitis: on the third day of central venous infusion, the patient presented with pain at the catheterization site, where a cordlike erythema extending proximally was seen, and it was alleviated by the use of mucopolysaccharide polysulfate cream. No other adverse drug reactions occurred. After 2 weeks of treatment, the plaque became smooth and dark, and the atrophic scar formed, causing lower eyelid ectrophia (Fig. 3a, b). The patient was discharged then. Intravenous amphotericin B was continued in the local hospital, and itraconazole 400 mg/day was taken orally meanwhile. The cumulative dose of amphotericin B was 1500 mg. The infection was in complete remission, and there was no recurrence for 8 months through telephone follow-ups.

Amphotericin B accumulated to 1500 mg, the plaque became smooth and dark. The atrophic scar formed, causing lower eyelid ectrophia (a right face, b left face)
Besides, we treated another four patients with M. irregular infections before. Including the case we report here, three of the five patients had sinus involvement. All patients were treated with intravenous amphotericin B combined with oral itraconazole. The adverse drug reactions during treatments included hypokalemia, anemia, abnormal liver and renal function, phlebitis, etc. They were alleviated by symptomatic management or withdrawal of antifungal agents. All the five patients were cured and had no recurrence during follow-ups. The treatment, adverse drug reactions and prognosis details of the five patients are shown in Table 1.
Discussion
M. irregularis infection is an opportunistic fungal infection which often occurs on farmers and workers, sometimes with the history of injury or surgery [3]. The distribution of M. irregularis infections is regional. Most cases caused by M. irregularis were reported in Asia, of which most were in China and several in Japan and India [1,2,3,4,5,6,7,8]. As this type of fungal infection is acquired from the environment, it may be related to the specific geographical conditions. The face is most commonly affected among all the parts of the body [3]. Patients with facial involvement near the nose often have sinus involvement, sometimes extending to the palate. The lesions usually infiltrate into the surrounding area gradually after the onset; the system damage is rare [1]. Most patients caused by M. irregularis are immunocompetent; however, Wang et al. [4] found the M. irregularis skin infection is related to CARD 9 deficiency recently. The patient in our case had a severe cosmetic damage; it could be related to the lack of timely effective treatment, so the treatment experience is very important.
Unlike other pathogenic fungi, M. irregularis is insensitive to most conventional antifungal agents. Drug susceptibility tests showed that M. irregularis was sensitive to amphotericin B [2, 6, 8,9,10], while the MIC value of itraconazole varied greatly, between 0.5 and > 16 μg/ml [2, 8, 9]. Clinical practice has proved that amphotericin B or its liposome is effective [3, 6, 10] and itraconazole is also effective in high-dose long-term therapy (400 mg/day) [1, 7,8,9]. Kang et al. [3] summarized 23 cases of M. irregularis infection and found that amphotericin B or its liposome had a cure rate of 70.59% (12/17, 3 lost to follow-up), while azoles tend to have a higher recurrence rate. We applied intravenous amphotericin B combined with oral itraconazole to treat M. irregularis infections in clinical practice, and the effect was remarkable. For patients with sinus involvement, amphotericin B should be applied to a cumulative dose of 1500 mg. Itraconazole 200–400 mg/day can be taken sequentially for 6–12 months; hence, the infection can be completely cured. For skin infections without sinus involvement, the total amount of amphotericin B can be reduced to about 500 mg, followed by itraconazole 200–400 mg/day for 1–10 months (the patient with CARD9 deficiency seems to need long-period therapy [4]); hence, the infection can be completely cured.
Surgical excision combined with antifungal agents can be used in patients with localized lesions and cannot adhere to antifungal therapy [2, 5]. Liang et al. [5] reported a case of M. irregularis infection that was treated by surgical resection without antifungal drugs and did not relapse for 2 years. Yamaguchi et al. [2] found that even if no fungal cells were found in the resected tissue, recurrence still occurred, so amphotericin B or its derivatives should be added after resection to prevent recurrence. Topical treatment such as amphotericin B wet compress is also helpful.
Adverse reactions of amphotericin B include arrhythmia, hypokalemia, abnormal liver and renal function, leukopenia, phlebitis, etc. [3, 6], most of which can be tolerated after symptomatic treatment. Weekly monitoring of blood routine, liver and renal function, electrolytes and electrocardiogram is needed. Slow infusion, sufficient hydration and central venous infusion can reduce the occurrence of phlebitis. In the patients we treated, amphotericin B can be discontinued after temporary renal impairment and continued after renal function recovery. For older patients, application of amphotericin B every two days can reduce the adverse reactions.
In summary, M. irregularis infection often presents as primary cutaneous infection without systemic involvement, but can leave severe cosmetic damage. Patients with nose involvement are prone to have sinus involvement. Amphotericin B intermittent intravenous infusion combined with itraconazole oral treatment has remarkable effect. Amphotericin B should reach 1500 mg in sinus affected patients, and the dose can be reduced in those without sinus involvement. Sequential itraconazole treatment can be added, with a total course of 6–12 months generally.
References
Matsudate Y, Murao K, Urano Y, et al. Primary cutaneous mucormycosis caused by Mucor irregularis in an immunocompetent patient. J Dermatol. 2015;42(3):267–8.
Yamaguchi S, Okubo Y, Katano A, et al. Primary cutaneous mucormycosis caused by Mucor irregularis in an elderly person. J Dermatol. 2015;42(2):210–4.
Kang D, Jiang X, Wan H, et al. Mucor irregularis infection around the inner canthus cured by amphotericin B: a case report and review of published literatures. Mycopathologia. 2014;178(1–2):129–33.
Wang X, Wang A, Wang X, et al. Cutaneous mucormycosis caused by Mucor irregularis in a patient with CARD9 deficiency. Br J Dermatol. 2019;180(1):213–4.
Liang GZ, Xu WQ, Zheng XL, et al. Successful treatment by surgery of a primary cutaneous mucormycosis caused by Mucor irregularis. Mycopathologia. 2018;183(2):445–9.
Xia ZK, Liu C, Cong L, et al. Mucormycosis caused by Mucor irregularis, a retrospective review of 20 cases. J Pract Dermatol. 2014;3:161–5.
Xia XJ, Shen H, Liu ZH. Primary cutaneous mucormycosis caused by Mucor irregularis. Clin Exp Dermatol. 2015;40(8):875–8.
Chander J, Kaur M, Bhalla M, et al. Changing epidemiology of mucoralean fungi: chronic cutaneous infection caused by Mucor irregularis. Mycopathologia. 2015;180(3–4):181–6.
Zhao Y, Zhang Q, Li L, et al. Primary cutaneous mucormycosis caused by Rhizomucor variabilis in an immunocompetent patient. Mycopathologia. 2009;168:243–7.
Martinez-Mugica C, Alba SR, Boga JA, et al. Cutaneous infection due to Mucor irregularis (Rhizomucor variabilis) in a immunocompetent traveller. Enferm Infecc Microbiol Clin. 2017;35(1):56–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Informed Consent
Informed consent for case report and image report was obtained from the patient.
Additional information
Handling editor: Cunwei Cao.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wei, Lw., Wang, H., Song, Yg. et al. Disfiguring Mucor irregularis Infection Cured by Amphotericin B and Itraconazole: A Case Report and Treatment Experience. Mycopathologia 184, 677–682 (2019). https://doi.org/10.1007/s11046-019-00380-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11046-019-00380-5