
Abstract
Plasma matrix metalloproteinase (MMP)-9 is a predictor of cardiovascular mortality, and MMP-9 polymorphisms affect plasma MMP-9 levels. However, no study examined whether MMP-9 haplotypes affect MMP-9 levels in obese adults. We examined whether MMP-9 polymorphisms and haplotypes are associated with obesity, and whether they affect MMP-9 levels in obese subjects. We examined the plasma levels of MMP-9 and tissue inhibitor of metalloproteinase (TIMP)-1 in 105 subjects with normal weight (controls), 100 obese subjects, and 156 obese subjects with ≥3 metabolic risk factors (MRFs). We determined genotypes for three polymorphisms: C-1562T (rs3918242), Q279R (A>G, rs17576), and R668Q (G>A, rs17577). MMP-9 levels and activity (MMP-9/TIMP-1 ratio) were higher in obese subjects than in controls (P < 0.05). However, MMP-9 levels were higher in obese subjects with ≥3 MRFs than in obese subjects (P < 0.05). Obese subjects with ≥3 MRFs carrying the GA+AA genotypes for R668Q (G>A) polymorphism had higher MMP-9 levels than subjects carrying the AA genotype (P < 0.05). The “T, G, A” haplotype was more common in both groups of obese subjects than in controls (OR 3.95 and 4.39, respectively; P < 0.01). Notably, obese subjects with ≥3 MRFs carrying the “T, G, A” haplotype had higher MMP-9 levels than subjects carrying the “C, A, G” reference haplotype (P < 0.05). The “T, G, A” haplotype was associated with an increased risk of obesity and affected MMP-9 levels in obese subjects with ≥3 MRFs. Our findings suggest that plasma MMP-9 levels and MMP-9 haplotypes may help to discriminate obese subjects at an increased cardiovascular risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Matrix metalloproteinase (MMP)-9 is an endopeptidase capable of degrading components of extracellular matrix, and tissue inhibitor of matrix metalloproteinase (TIMP)-1 is a major MMP-9 inhibitor [1]. Plasma MMP-9 concentration was identified as a predictor of mortality in patients with coronary artery disease [2]. Notably, MMP-9 was found to be the highest upregulated gene in metabolically unhealthy compared to metabolically healthy obese subjects [3]. Moreover, MMP-9 expression was significantly higher in obese subjects and in obese patients with type 2 diabetes than in subjects with normal weight [4]. Obesity is a key factor in the development of the metabolic syndrome [5], and obese subjects may have an increased risk of developing cardiovascular diseases [6–8].
MMP-9 gene polymorphisms modify plasma MMP-9 levels and prognosis of patients with cardiovascular diseases [2, 9, 10]. We have shown that MMP-9 polymorphisms and haplotypes (combinations of genetic markers) affect plasma MMP-9 levels in obese children and adolescents [11]. However, no study has tested the hypothesis that MMP-9 haplotypes are associated with obesity and affect plasma MMP-9 levels in obese adults. It is possible that obese subjects carrying specific MMP-9 genotypes or haplotypes may have different plasma MMP-9 levels. We focused here on three functional polymorphisms in the MMP-9 gene: C-1562T (rs3918242), Q279R (A>G, rs17576) and R668Q (G>A, rs17577), which modify MMP-9 expression or activity [10, 12, 13] and have been associated with cardiovascular diseases [2, 9, 14].
In the present study, we aimed at comparing the plasma levels of MMP-9 and TIMP-1, as well as the MMP-9/TIMP-1 ratios, in subjects with normal weight with those found in obese subjects and in obese subjects with ≥3 metabolic risk factors (MRFs). We then examined whether the MMP-9 polymorphisms and haplotypes are associated with the susceptibility to obesity, and whether they affect plasma MMP-9 levels in obese subjects.
Materials and methods
Subjects
This study was approved by the Institutional Review Board at the Santa Casa de Belo Horizonte, Brazil, and subjects gave written informed consent. Subjects with obesity were recruited from the Department of Obesity, Center of Medical Specialties of Minas Gerais, Belo Horizonte, Brazil, and the control group consisted of 105 subjects recruited from the local community. Subjects with body mass index ≥18.5–24.9 kg/m2 were considered as having normal weight, and obese subjects were defined as having body mass index ≥30 kg/m2 [15]. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured at least three times from all subjects with the use of an automatic BP device. The individuals were considered hypertensive if their SBP or DBP was >140 or >90 mmHg, respectively, or were on antihypertensive therapy.
To determine metabolic risk factors in obese subjects, we followed the diagnostic criteria for metabolic syndrome defined according to the American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement [16], which included the following factors: (1) elevated waist circumference (WC ≥120 cm in men and ≥88 cm in women); (2) elevated triglycerides (TG, ≥150 mg/dL or drug treatment for elevated triglycerides); (3) reduced high-density lipoprotein (HDL) cholesterol (HDL-C, <40 mg/dL in men and <50 mg/dL in women or drug treatment for reduced HDL-C); (4) elevated blood pressure (≥130 mm Hg for SBP or ≥85 mm Hg for DBP) or drug treatment for elevated blood pressure; (5) elevated fasting glucose ≥100 mg/dL or drug treatment for elevated glucose [16].
At the time of clinical attendance, venous blood samples were collected after overnight fasting, immediately centrifuged at 3000g for 10 min at room temperature, and plasma samples were stored at −80 °C until analyzed. Genomic DNA was extracted from the cellular component of 1 mL of whole blood by a salting-out method and stored at −20 °C until analyzed.
Enzyme immunoassays of MMP-9 and TIMP-1 levels and biochemical analyses
Plasma levels of MMP-9 and TIMP-1 were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions. Glucose concentrations and lipid parameters were determined with routine enzymatic methods using commercial kits (Katal Biotechnology Industry and Trade Ltd., Belo Horizonte, Minas Gerais, Brazil).
Genotype determination
Genotypes for C-1562T (rs3918242) polymorphism in the promoter region of MMP-9 gene were determined by polymerase chain reaction-restriction fragment length polymorphism (PCR–RFLP), as described in detail elsewhere [17]. Briefly, amplified products obtained from PCR were digested with SphI restriction enzyme, and fragments were separated by electrophoresis in 12 % polyacrylamide gels and visualized by silver staining [17].
Genotypes for Q279R (rs17576, A>G; Assay ID: C__11655953_10) and R668Q (rs17577, G>A; Assay ID: C__11655948_1_) polymorphisms in the exon 6 and exon 12 of MMP-9 gene were determined by the respective Taqman allele discrimination assays (Applied Biosystems, Carlsbad, CA, USA). Fluorescence from PCR amplification was detected using Eco Real-Time PCR System (Illumina, San Diego, CA, USA) and analyzed with the manufacturer’s software.
Haplotype analysis
Haplotype frequencies were estimated using the Haplo.stats package version 1.6.11 (http://cran.r-project.org/web/packages/haplo.stats/index.html), as described in detail elsewhere [14, 18]. To further confirm the haplotype frequencies, we used the Bayesian statistical based program Phase version 2.1 (http://www.stat.washington.edu/stephens/software.html) [19]. Only four haplotypes “C, A, G”, “C, G, G”, “C, G, A” and “T, G, A” had frequencies >5 % in at least one of the study groups and were considered in the statistical analysis. However, we considered a value of Pc < 0.00625 (0.05/8, the total number of possible haplotypes) for the differences in haplotype frequencies among the groups tested using χ 2 tests, to correct for the number of comparisons made (Bonferroni’s correction). Linkage disequilibrium (LD) among MMP-9 polymorphisms for the study groups were characterized by calculating D′ and log of the likelihood odds ratio (LOD, a measure of confidence in the value of D′) using the Haploview software (version 4.2; http://www.broad.mit.edu/mpg/haploview/).
To further examine the effects of MMP-9 haplotypes on plasma MMP-9 levels, we compared the haplotype distributions in two extreme groups of subjects: the lower quartile and the upper quartile groups, which included subjects in the lower and in the upper quartiles of plasma MMP-9 distribution, respectively. We hypothesized that the haplotype associated with the higher MMP-9 levels would be more commonly found in the upper quartile group.
Statistical analysis
The clinical and biochemical characteristics among groups and the effects of genotypes and haplotypes on MMP-9 levels were compared by ANOVA followed by Tukey test (normally distributed variables) or Kruskall-Wallis test followed by Dunn’s multiple comparison test (not normally distributed variables). The categorical variables were compared between groups by χ 2 tests. The distribution of genotypes for each polymorphism was assessed for deviation from the Hardy–Weinberg equilibrium, and differences in genotype and allele frequencies between groups were assessed using χ 2 tests. A value of P < 0.05 was considered significant. Multivariate linear regression analysis was performed by using the JMP software 5.0.1a (SAS Institute, Cary, NC, USA). Age, gender, body mass index (BMI), and systolic blood pressure (SBP) were considered as independent variables.
Power calculations were performed using the PGA Matlab software (http://dceg.cancer.gov/tools/analysis/pga) [20]. Given the sample size of this study, we obtained a power of 80 % with an alpha level of 0.05 to detect an odds ratio of 2.0, based on the prevalence of obesity as 30 % [8], the disease allele frequency as 6 % for C-1562T polymorphism (Supplementary Table S1) and the “T, G, A” haplotype frequency as 8.9 % (Table 2).
Results
The clinical characteristics, anthropometric parameters and biochemical data of subjects included in this study are shown in Table 1. There were significant differences in all factors studied when both groups of obese subjects were compared with subjects with normal weight (P < 0.05), except for SBP and DBP (vs. obese subjects; P > 0.05). Obese subjects had a slightly lower average age. Importantly, the group of obese subjects with ≥3 MRFs had higher body mass index, waist circumference, SBP, DBP, triglycerides and fasting glucose than the group of obese subjects (P < 0.05; Table 1).
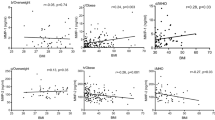
We found higher plasma MMP-9 levels and MMP-9/TIMP-1 ratios when both groups of obese subjects were compared with subjects with normal weight (P < 0.05; Fig. 1a, c, respectively). However, we found no differences in TIMP-1 levels among the groups (P > 0.05; Fig. 1b). Notably, obese subjects with ≥3 MRFs had higher MMP-9 levels than obese subjects (P < 0.05; Fig. 1a). We examined the association between plasma MMP-9 levels, BMI and the MRFs in the study groups using linear regression adjusting for age and gender (Table 2). We found that both BMI and SBP were positively correlated with plasma MMP-9 levels in obese subjects with ≥3 MRFs (P < 0.05; Table 2).

Plasma MMP-9 levels (a), TIMP-1 levels (b) and MMP-9/TIMP-1 ratios (c) in subjects with normal weight (n = 105), obese subjects (n = 100) and obese subjects with ≥3 metabolic risk factors (MRFs) (n = 156). The box and whiskers plots show range and quartiles. The boxes extend from the 25th to the 75th percentile, with a line at the median. The whiskers show the highest and the lowest values. *P < 0.05 versus subjects with normal weight. # P < 0.05 versus obese subjects
Genotypes and allele frequency distributions for the MMP-9 polymorphisms are shown in Supplementary Table S1. The distributions of genotypes for each polymorphism showed no deviation from Hardy–Weinberg equilibrium. The CT+TT genotypes (OR 2.49; P = 0.009) and the C allele (OR 2.49; P = 0.006) for the C-1562T polymorphism were found at higher frequency in obese subjects with ≥3 MRFs than in subjects with normal weight (Supplementary Table S1). The CT+TT genotypes were combined for the analysis because there were few subjects with the TT genotype in the study groups. Conversely, we found no differences for the Q279R (A>G) and R668Q (G>A) polymorphisms when the study groups were compared (P > 0.05; Supplementary Table S1).
We then examined the effects of MMP-9 genotypes on plasma MMP-9 levels. We found no effects of the C-1562T and Q279R (A>G) polymorphisms on MMP-9 levels (Fig. 2a, b, respectively; P > 0.05). However, we found that obese subjects with ≥3 MRFs carrying the GA+AA genotypes had higher MMP-9 levels than subjects carrying the AA genotype for the R668Q (G>A) polymorphism (P < 0.05; Fig. 2c). We also examined the effects of MMP-9 genotypes on MMP-9 levels using multiple linear regression adjusting for age, gender, BMI and SBP. We found that the GG genotype for the R668Q (G>A) polymorphism was negatively associated with MMP-9 levels in obese subjects with ≥3 MRFs (P = 0.069; Supplementary Table S2), which is in agreement with Fig. 2C.

Plasma MMP-9 levels in subjects with normal weight (n = 105), obese subjects (n = 100) and obese subjects with ≥3 metabolic risk factors (MRFs) (n = 156), grouped according to different genotypes for the MMP-9 polymorphisms (a–c). The box and whiskers plots show range and quartiles. The boxes extend from the 25th to the 75th percentile, with a line at the median. The whiskers show the highest and the lowest values. *P < 0.05 versus the GG genotype in obese subjects with ≥3 MRFs
Haplotype frequencies are shown in Table 3. The “C, G, A” haplotype was found at higher frequency in subjects with normal weight than in both groups of obese subjects (both P < 0.00625; Table 3). Conversely, the “T, G, A” haplotype was found at higher frequency in both groups of obese subjects than in subjects with normal weight (both P < 0.00625; Table 3).
Importantly, we examined the effects of different MMP-9 haplotypes on plasma MMP-9 levels. We found no effects on MMP-9 levels when the haplotypes were compared in subjects with normal weight and in obese subjects (P > 0.05; Fig. 3). The “C, G, A” haplotype was not considered for obese subjects, because there were too few subjects to conduct haplotype analysis in this group. Notably, obese subjects with ≥3 MRFs carrying the “T, G, A” haplotype had higher MMP-9 levels than subjects carrying the “C, A, G” reference haplotype (P < 0.05; Fig. 3). We also examined the effects of MMP-9 haplotypes on MMP-9 levels using multiple linear regression adjusting for age, gender, BMI and SBP. We found that the “T, G, A” haplotype was positively associated with MMP-9 levels in obese subjects with ≥3 MRFs (P = 0.070; Supplementary Table S3), which is in agreement with Fig. 3.

Plasma MMP-9 levels in the study subjects, grouped according to the different MMP-9 haplotypes. The box and whiskers plots show range and quartiles. The boxes extend from the 25th to the 75th percentile, with a line at the median. The whiskers show the highest and the lowest values. *P < 0.05 versus the “C, A, G” reference haplotype
We compared the LD among the MMP-9 polymorphisms and we found higher LD values in obese subjects with ≥3 MRFs (Fig. 4). The C-1562T polymorphism (rs3918242) is in high LD with the rs17576 and rs17577 polymorphisms in the exon 6 (D′ = 0.912, LOD = 11.68) and exon 12 (D′ = 0.789, LOD = 18.11), respectively, which form a haplotype block in obese subjects with ≥3 MRFs (Fig. 4).

Linkage disequilibrium (LD) among the MMP-9 polymorphisms for the study groups. The polymorphisms are identified by their reference SNP ID number (“rs#”). Numbers within squares indicate the D′ value expressed as a percentile. Black squares indicate pairs in strong LD with LOD scores for LD ≥2, gray squares D′ <1 with LOD ≥2, and white squares D′ <1.0 and LOD <2
We performed a further analysis and compared the haplotype frequencies for the subjects in the lower and in the upper quartiles of plasma MMP-9 levels distribution within each study group. No significant differences were found in subjects with normal weight and in obese subjects (data not shown). Notably, the “T, G, A” haplotype was more frequent in the upper than in the lower quartile group in obese subjects with ≥3 MRFs (OR 5.09; P = 0.009; Supplementary Table S4).
Discussion
The main novel findings of this study are that plasma MMP-9 levels were significantly higher in obese subjects with ≥3 MRFs compared to obese subjects. In addition, obese subjects with ≥3 MRFs carrying the GA+AA genotypes for R668Q (G>A) polymorphism or the “T, G, A” haplotype of the MMP-9 gene had higher plasma MMP-9 levels. Furthermore, we found that the “T, G, A” haplotype was associated with an increased risk of obesity.
Both groups of obese subjects had higher plasma MMP-9 levels than subjects with normal weight. Consistently, higher MMP-9 levels were found in obese women than lean women [21, 22], and in obese patients than controls [23]. Notably, the MMP-9/TIMP-1 ratios were significantly higher in both groups of obese subjects than subjects with normal weight. The ratio was used to assess net MMP-9 activity because TIMP-1 is a major MMP-9 inhibitor [1]. Therefore, the MMP-9/TIMP-1 ratio might provide a better index of net MMP-9 activity as compared with the simple assessment of MMP-9 levels [11].
Notably, plasma MMP-9 levels were significantly higher in obese subjects with ≥3 MRFs. Indeed, MMP-9 is one of the matrix metalloproteinases most associated with metabolic syndrome [24, 25]. Increased concentrations of pro-MMP-9 were associated with increased concentrations of pro-inflammatory mediators in patients with metabolic syndrome [26]. Moreover, elevated expression of pro-inflammatory genes, including MMP-9, decreased significantly after weight loss in obese women [27]. In addition, dysregulated production or secretion of adipokines owing to adipose tissue dysfunction can contribute to the development of cardiovascular diseases related to obesity [28–30]. Therefore, an increased pro-inflammatory state could explain the highest MMP-9 levels in obese subjects with ≥3 MRFs. However, further studies are needed to prove this hypothesis.
Interestingly, the higher plasma MMP-9 levels in obese subjects with ≥3 MRFs carrying the GA+AA genotypes of R668Q (G>A) polymorphism can be explained by its functional role on MMP-9 expression. The microRNA miR-4783-3p preferentially inhibits the G allele and reduce the MMP-9 protein, but have little effect on the A allele [13], which is in line with the higher MMP-9 levels in subjects carrying the genotypes containing the A allele of this polymorphism. Conversely, the C-1562T polymorphism had no effects on MMP-9 levels, which is in agreement with a previous finding [31]. However, the T allele of this polymorphism is associated with increased MMP-9 expression as a result of the loss of a nuclear repressor protein binding site when the T allele is present in the promoter region of the MMP-9 gene [10].
We provide the first evidence that MMP-9 haplotypes may be associated with the susceptibility to obesity in adults. Particularly, the “T, G, A” haplotype may be associated with an increased risk of obesity. Importantly, while we have shown that MMP-9 haplotypes affect plasma MMP-9 levels in obese children and adolescents [11], this is the first study to examine the effects of MMP-9 haplotypes on plasma MMP-9 levels in obese adults. Higher plasma MMP-9 levels were found in obese subjects with ≥3 MRFs carrying the “T, G, A” haplotype, which was confirmed to be associated with the group of subjects in the upper quartile of MMP-9 levels distribution in this group. Our findings suggest that the “T, G, A” haplotype not only is associated with an increased risk of obesity, but also to higher plasma MMP-9 levels in obese subjects with ≥3 MRFs.
The C-1562T polymorphism in the promoter region had no effect in the present study, but it could be in LD with another functional polymorphism of MMP-9 gene. Although there are differences in LD structure between different populations, MMP-9 polymorphisms were also found to be in strong LD in patients with coronary artery disease [9], including the C-1562T (rs3918242) and Q279R (rs17576) polymorphisms studied here. Indeed, we found high LD between rs3918242 and R668Q (rs17577) polymorphisms, which were found to be associated with the obese subjects with ≥3 MRFs and to affect plasma MMP-9 levels in this group, respectively.
This study has some limitations. Despite the relatively small number of subjects, we found associations of MMP-9 gene polymorphisms and haplotypes that remained significant after Bonferroni’s correction. Moreover, we have not studied the polymorphism −90(CA)14–24 in the promoter of the MMP-9 gene, which is known to modify MMP-9 expression [32], and to affect plasma MMP-9 levels in healthy subjects [17] and in obese children and adolescents [11].
In conclusion, we found evidence indicating that obese subjects with ≥3 MRFs carrying the GA+AA genotypes for R668Q (G>A) polymorphism or the “T, G, A” haplotype of the MMP-9 gene had higher plasma MMP-9 levels. Moreover, we found that the “T, G, A” haplotype is associated with an increased risk of obesity. Our findings suggest that plasma MMP-9 levels and MMP-9 gene haplotypes may help to discriminate obese subjects at an increased cardiovascular risk.
References
Van den Steen PE, Dubois B, Nelissen I, Rudd PM, Dwek RA, Opdenakker G (2002) Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9). Crit Rev Biochem Mol Biol 37(6):375–536. doi:10.1080/10409230290771546
Blankenberg S, Rupprecht HJ, Poirier O, Bickel C, Smieja M, Hafner G, Meyer J, Cambien F, Tiret L, AtheroGene I (2003) Plasma concentrations and genetic variation of matrix metalloproteinase 9 and prognosis of patients with cardiovascular disease. Circulation 107(12):1579–1585. doi:10.1161/01.CIR.0000058700.41738.12
Das SK, Ma L, Sharma NK (2015) Adipose tissue gene expression and metabolic health of obese adults. Int J Obes (Lond) 39(5):869–873. doi:10.1038/ijo.2014.210
Dandona P, Ghanim H, Monte SV, Caruana JA, Green K, Abuaysheh S, Lohano T, Schentag J, Dhindsa S, Chaudhuri A (2014) Increase in the mediators of asthma in obesity and obesity with type 2 diabetes: reduction with weight loss. Obesity (Silver Spring) 22(2):356–362. doi:10.1002/oby.20524
Phillips CM, Tierney AC, Perez-Martinez P, Defoort C, Blaak EE, Gjelstad IM, Lopez-Miranda J, Kiec-Klimczak M, Malczewska-Malec M, Drevon CA, Hall W, Lovegrove JA, Karlstrom B, Riserus U, Roche HM (2013) Obesity and body fat classification in the metabolic syndrome: impact on cardiometabolic risk metabotype. Obesity (Silver Spring) 21(1):E154–E161. doi:10.1002/oby.20263
Ahima RS, Lazar MA (2013) Physiology. The health risk of obesity—better metrics imperative. Science. doi:10.1126/science.1241244
Despres JP (2012) Body fat distribution and risk of cardiovascular disease: an update. Circulation 126(10):1301–1313. doi:10.1161/CIRCULATIONAHA.111.067264
Yang W, Kelly T, He J (2007) Genetic epidemiology of obesity. Epidemiol Rev 29:49–61. doi:10.1093/epirev/mxm004
Morgan AR, Zhang B, Tapper W, Collins A, Ye S (2003) Haplotypic analysis of the MMP-9 gene in relation to coronary artery disease. J Mol Med (Berl) 81(5):321–326. doi:10.1007/s00109-003-0441-z
Zhang B, Ye S, Herrmann SM, Eriksson P, de Maat M, Evans A, Arveiler D, Luc G, Cambien F, Hamsten A, Watkins H, Henney AM (1999) Functional polymorphism in the regulatory region of gelatinase B gene in relation to severity of coronary atherosclerosis. Circulation 99(14):1788–1794
Belo VA, Souza-Costa DC, Luizon MR, Lanna CM, Carneiro PC, Izidoro-Toledo TC, Ferraz KC, Tanus-Santos JE (2012) Matrix metalloproteinase-9 genetic variations affect MMP-9 levels in obese children. Int J Obes (Lond) 36(1):69–75. doi:10.1038/ijo.2011.169
Allan JA, Docherty AJ, Barker PJ, Huskisson NS, Reynolds JJ, Murphy G (1995) Binding of gelatinases A and B to type-I collagen and other matrix components. Biochem J 309(Pt 1):299–306
Duellman T, Warren C, Yang J (2014) Single nucleotide polymorphism-specific regulation of matrix metalloproteinase-9 by multiple miRNAs targeting the coding exon. Nucleic Acids Res 42(9):5518–5531. doi:10.1093/nar/gku197
Lacchini R, Jacob-Ferreira AL, Luizon MR, Coeli FB, Izidoro-Toledo TC, Gasparini S, Ferreira-Sae MC, Schreiber R, Nadruz W Jr, Tanus-Santos JE (2010) Matrix metalloproteinase 9 gene haplotypes affect left ventricular hypertrophy in hypertensive patients. Clin Chim Acta 411(23–24):1940–1944. doi:10.1016/j.cca.2010.08.008
Flegal KM, Kit BK, Orpana H, Graubard BI (2013) Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA 309(1):71–82. doi:10.1001/jama.2012.113905
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F, American Heart A, National Heart L, Blood I (2005) Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
Metzger IF, Luizon MR, Lacchini R, Tanus-Santos JE (2012) Genetic variants in matrix metalloproteinase-9 gene modify metalloproteinase-9 levels in black subjects. DNA Cell Biol 31(4):504–510. doi:10.1089/dna.2011.1388
Schaid DJ, Rowland CM, Tines DE, Jacobson RM, Poland GA (2002) Score tests for association between traits and haplotypes when linkage phase is ambiguous. Am J Hum Genet 70(2):425–434. doi:10.1086/338688
Stephens M, Smith NJ, Donnelly P (2001) A new statistical method for haplotype reconstruction from population data. Am J Hum Genet 68(4):978–989. doi:10.1086/319501
Menashe I, Rosenberg PS, Chen BE (2008) PGA: power calculator for case-control genetic association analyses. BMC Genet 9:36. doi:10.1186/1471-2156-9-36
Andrade VL, Petruceli E, Belo VA, Andrade-Fernandes CM, Caetano Russi CV, Bosco AA, Tanus-Santos JE, Sandrim VC (2012) Evaluation of plasmatic MMP-8, MMP-9, TIMP-1 and MPO levels in obese and lean women. Clin Biochem 45(6):412–415. doi:10.1016/j.clinbiochem.2012.01.008
Kosmala W, Plaksej R, Przewlocka-Kosmala M, Kuliczkowska-Plaksej J, Bednarek-Tupikowska G, Mazurek W (2008) Matrix metalloproteinases 2 and 9 and their tissue inhibitors 1 and 2 in premenopausal obese women: relationship to cardiac function. Int J Obes (Lond) 32(5):763–771. doi:10.1038/sj.ijo.0803794
Derosa G, Ferrari I, D’Angelo A, Tinelli C, Salvadeo SA, Ciccarelli L, Piccinni MN, Gravina A, Ramondetti F, Maffioli P, Cicero AF (2008) Matrix metalloproteinase-2 and -9 levels in obese patients. Endothelium 15(4):219–224. doi:10.1080/10623320802228815
Berg G, Miksztowicz V, Schreier L (2011) Metalloproteinases in metabolic syndrome. Clin Chim Acta 412(19–20):1731–1739. doi:10.1016/j.cca.2011.06.013
Berg G, Schreier L, Miksztowicz V (2014) Circulating and adipose tissue matrix metalloproteinases in cardiometabolic risk environments: pathophysiological aspects. Horm Mol Biol Clin Investig 17(2):79–87. doi:10.1515/hmbci-2013-0069
Goncalves FM, Jacob-Ferreira AL, Gomes VA, Casella-Filho A, Chagas AC, Marcaccini AM, Gerlach RF, Tanus-Santos JE (2009) Increased circulating levels of matrix metalloproteinase (MMP)-8, MMP-9, and pro-inflammatory markers in patients with metabolic syndrome. Clin Chim Acta 403(1–2):173–177. doi:10.1016/j.cca.2009.02.013
Sheu WH, Chang TM, Lee WJ, Ou HC, Wu CM, Tseng LN, Lang HF, Wu CS, Wan CJ, Lee IT (2008) Effect of weight loss on proinflammatory state of mononuclear cells in obese women. Obesity (Silver Spring) 16(5):1033–1038. doi:10.1038/oby.2008.37
Jung UJ, Choi MS (2014) Obesity and its metabolic complications: the role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int J Mol Sci 15(4):6184–6223. doi:10.3390/ijms15046184
Ouchi N, Parker JL, Lugus JJ, Walsh K (2011) Adipokines in inflammation and metabolic disease. Nat Rev Immunol 11(2):85–97. doi:10.1038/nri2921
Van Gaal LF, Mertens IL, De Block CE (2006) Mechanisms linking obesity with cardiovascular disease. Nature 444(7121):875–880. doi:10.1038/nature05487
Andrade VL, Fernandes KS, Bosco AA, Tanus-Santos JE, Sandrim VC (2012) Functional polymorphism located in MMP-9 gene promoter is strongly associated with obesity. DNA Cell Biol 31(6):1054–1057. doi:10.1089/dna.2011.1526
Peters DG, Kassam A, St Jean PL, Yonas H, Ferrell RE (1999) Functional polymorphism in the matrix metalloproteinase-9 promoter as a potential risk factor for intracranial aneurysm. Stroke 30(12):2612–2616
Acknowledgments
This study was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnologico (CNPq-Brazil), and by Fundacao de Amparo a Pesquisa do Estado de Minas Gerais (FAPEMIG-Brazil). MRL is a Young Talent Attraction fellow from CNPq-Brazil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Luizon, M.R., Belo, V.A., Fernandes, K.S. et al. Plasma matrix metalloproteinase-9 levels, MMP-9 gene haplotypes, and cardiovascular risk in obese subjects. Mol Biol Rep 43, 463–471 (2016). https://doi.org/10.1007/s11033-016-3993-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-016-3993-z