
Abstract
The interleukin (IL)-1β-511 C/T polymorphism has been shown to be functional and to contribute to the risk of gastric cancer. However, the relationship between the IL-1β-511 C/T polymorphism and gastric carcinogenesis remains inconclusive. A systematical electronic search was conducted of the MEDLINE, EMBASE, and CENTRAL databases. A random and a fixed effects model were exploited to estimate summary odds ratios and 95 % confidence intervals. Subgroup and sensitivity analyses were carried out with respect to ethnicity, quality assessment scores, control sources, genotyping methods, cancer histopathology and location, and Helicobacter pylori (H. pylori) infection. A total of 45 studies containing 9,066 cases of gastric cancer and 11,192 control subjects satisfied the inclusion criteria. The IL-1β-511 C/T polymorphism was found to enhance the risk of stomach cancer for overall and HWE-satisfying studies. Asians showed a positive relationship in both the overall and HWE-satisfying groups, whereas Caucasians did not. Based on subgroup analysis, H. pylori infection and genotype analysis using PCR–RFLP methods increase the association between IL-1β-511 T allele carrier and risk of stomach cancer. A positive relationship was found between the IL-1β-511 C/T SNP and stomach carcinoma susceptibility, and the results suggest that Asian ethnicity, H. pylori infection and methodologically, PCR–RFLP genotyping strengthen this relationship. Reflecting on prevalence of H. pylori in Asian countries, additional studies on the IL-1β-511 C/T SNP in the context of ethnicity and H. pylori infection may provide key insights into the mechanism underlying gastric cancer carcinogenesis. It was found PCR–RFLP is the most reliable genotyping method, and thus, it is recommendable to adopt it to determine the presence of the IL-1β-511 C/T SNP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Interleukin (IL)-1β initiates inflammatory reactions and amplifies immunologic responses against harmful stimuli [1]. Furthermore, in chronic inflammatory states, IL-1β generates COX-2 and iNOS, which inhibit apoptosis, induce DNA damage, and modulate cell adhesion [2]. In addition, the signaling cascade from IL-1β is the basis of the carcinogenesis. In addition to persistent inflammatory reaction caused by gastric injury, IL-1β suppresses acid secretion 6,000 times as effectively as H2 antagonist and 100 times more than proton pump inhibitor [3]. The expression of this cytokine creates a hypoacidic condition that favors the survival of Helicobacter pylori (H. pylori), and consequently leads to atrophy of stomach tissues or adenocarcinoma [4, 5], and overgrowth of H. pylori induces an assembly of neutrophils and lymphocytes, particularly Th1 and Th17 CD4+ cells, which induce IL-1β secretion [6, 7]. Three single-nucleotide polymorphisms (SNPs), namely −31 T/C, +3954 C/T, and −511 C/T have been discovered in the promoter region of chromosome 2q and are regarded to trigger the overexpression of IL-1β [8]. This study focuses on the IL-1β-511 C/T polymorphism because many studies have investigated it, whereas relatively few have examined the +3954 C/T polymorphism. In addition, the −31 T/C SNP has been reported to show linkage disequilibrium with −511 C/T [9].
However, previous studies, including meta-analyses, have produced mixed results [10–15], which may have been caused by dissimilar characteristics among studies, such as, sample sizes, ethnicities, cancer type, inconsistent inclusion criteria (e.g., involving premalignant lesions as a case group), and a lack of comprehensive subgroup analyses. In this regard, the present study provides a comprehensive and systematic review based on sophisticated subgroup analysis that excluded methodological discrepancies. In addition, overall susceptibility results were verified by sensitivity analysis based on considerations of Hardy–Weinberg equilibrium (HWE) as a crucial standard for determining the reliability of subject for case–control studies [16].
Materials and methods
Search strategy
A systematic search was conducted utilizing the MEDLINE, EMBASE, and CENTRAL databases (last search on February 05, 2013). The following terms were combined: “Interleukins,” “IL-1β,” “IL-1β-511,” “Interleukin-1,” “Interleukin-1β,” “Interleukin-1β-511,” “Interleukin-1beta,” “IL-1beta,” “Interleukin-1beta,” “polymorphisms,” “SNP,” “single nucleotide,” “mutation,” “stomach cancer,” “gastric adenocarcinoma,” and “gastric cancer.” Supplement S1 describes the detailed search strategy, which was reviewed by two independent investigators (M.J.P and M.H.H) and a third reviewer (S.S.P).
Study selection
The studies included: (i) described the relationship between the IL-1β-511 C/T SNP and stomach carcinoma; (ii) contained sufficient number of subjects to yield odds ratios (ORs) and 95 % confidence intervals (CIs); (iii) had a case–control design; (iv) included case samples consisting of gastric cancer (not premalignant lesions), and control samples free of any gastric disease, such as, gastritis or gastric ulcer; and (v) were written in English. A PRISMA checklist and a flow chart of the study inclusion procedure are presented in Supplements S2 and S3, respectively.
Methodological quality assessment
The methodologic quality of each study was assessed using the scale proposed by Thakkinstian et al. [7] and refined by Camargo et al. [12] and Xue et al. [13]. Any disagreement between evaluation results was resolved by the third reviewer (S.S. Park). Evaluations were conducted to determine the representativeness of cases and controls, to assess reliability of stomach carcinoma confirmation and genotyping tests, and to assess potential confounding factors, as shown in Supplement S4. Quality assessment scores ranged from 0 (lowest) to 9 (highest). We classified reports that scored <5.0 as “low to moderate quality” and those that scored ≥5.0 as “high quality.”
Data extraction
To enhance the reliability of data, two investigators (M.J. Park and M.H. Hyun) independently performed and verified data extraction. The following information was collected: authors’ names, subject ethnicity, sex ratio, origin of control samples, numbers of cases and controls, and the genotyping method. In addition, the genotype frequencies of each pathologic type of cancer, each anatomical classification of cancer, and of H. pylori-positive populations were determined when reports provided relevant information.
Statistical analysis
We utilized Review Manager 5.2 (Cochrane Collaboration, London, UK) to conduct the statistical analysis. ORs and 95 % CIs were calculated from extracted raw data, and strengths of association were estimated [17]. Meta-analysis was conducted using the following models: (1) T allele versus C allele (an allelic contrast model), (2) TT genotype versus CC genotype (a homozygote contrast model), (3) TT+TC genotype versus. CC genotype (a dominant contrast model), and (4) TT vs. TC+CC (a recessive contrast model).
Heterogeneities of included studies were calculated based on Q statistics using the Mantel–Haunszel weight and I 2 statistics. [18]. Heterogeneity between studies was confirmed when studies have a P value of <0.10 and an I 2 value >50 %. For studies with heterogeneity, a random effects model was employed based on the DerSimonian–Laird method [19]. Otherwise, a fixed effects model was employed based on the Mantel–Haenszel method [18].
We conducted Chi square analysis to assess the control group fit with the Hardy–Weinberg equilibrium (HWE). The groups deviating from the HWE have a P value of <0.05 [20]. Begg’s test and Egger’s funnel plot asymmetry test were used to evaluate publication bias [21, 22].
Results
Literature search, characteristics of included studies, and publication bias
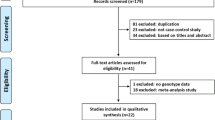
The overall flow of the searching procedure is shown in Fig. 1. First, a total of 824 studies were identified by systematic search after excluding duplicates. Screening of full texts for relevance and accessibility resulted in the exclusion of 482 irrelevant studies and 7 abstract-only articles. 290 of the remaining 335 studies were excluded for the following reasons: 93 for including premalignant lesions, not gastric cancer, 138 for including control populations with gastritis or dyspeptic disease, 44 for not having a case–control design, and 15 for being written in other than English. In addition, 2 studies included data from two different geographic areas [23, 24]. Persson et al. [25] recruited control subjects from two sources: hospitals and general population. Zhao et al. [26] considered three ethnic groups from the same area. In the present study, each geographic area, control source, and ethnicity were considered separate data sets. As a result, 45 studies (50 data sets) were included in this meta-analysis, reflecting 9,066 gastric cancer patients and 11,192 control subjects [8, 23–66]. Table 1 shows the characteristics of each study. Of the 45 studies, control groups deviated from the HWE in 10 [33, 34, 36, 39, 41, 42, 51, 59, 60, 63]. In addition, 14 studies involved Caucasian populations, 27 Asian populations, and 4 other ethnicities. Twenty-four studies employed the PCR–RFLP genotyping, and the remainder used other genotyping techniques, such as, RCP–SSCP and PCR–DHPLC. Twenty-nine studies were classified as high quality, and 16 as low to moderate quality. Supplement S5 summarizes quality assessment criteria. Finally, we used a funnel plot and Egger’s regression to assess the heterogeneity of studies and publication bias. Figure 2 presents the qualitative results for publication bias and shows a symmetrical distribution for the overall studies. Egger’s regression revealed no publication bias (P > 0.1).

Study flow chart

A funnel plot of publication bias
Overall results on the relationship between the IL-1β-511 C/T SNP and gastric cancer
Figure 3 summarizes the results of sensitivity analysis based on the HWE principle using the recessive model (TT vs. CC+CT). For overall studies, interleukin 1β-511 C/T SNP was found to be positively related to the risk of stomach carcinoma (OR = 1.15; 95 % CI 1.03–1.29). Studies satisfying the HWE supported this relationship with a similar odds ratio (OR = 1.15; 95 % CI 1.01–1.29), whereas those deviating from the HWE showed no association between the IL-1β-511 C/T SNP and the risk of stomach carcinoma (OR = 1.19; 95 % CI 0.84–1.69).

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) based on the Hardy–Weinberg equilibrium by publication year. The areas of the squares indicate the relative weights of the specific studies. Bars represent 95 % confidence intervals, and “GC,” gastric cancer
Comprehensive subgroup analysis for overall studies and HWE studies
Table 2 summarizes the outcomes of comprehensive subgroup analysis with respect to ethnicity, study quality, control sources, genotyping methods, anatomical locations of cancer, pathologies of cancer, and H. pylori infection. When stratified by ethnicity, a positive relationship was observed for Asian populations for both overall (OR = 1.14; 95 % CI 1.01–1.29) and HWE satisfying (OR = 1.16; 95 % CI 1.01–1.33) studies. However, no such association was observed for Caucasian populations for overall (OR = 1.15; 95 % CI 0.87–1.52) and HWE satisfying (OR = 1.10; 95 % CI 0.85–1.42) studies (Fig. 4). H. pylori-positivity group was related to the risk of stomach carcinoma in overall (OR = 1.70; 95 % CI 1.03–2.80) and HWE satisfying (OR = 2.04; 95 % CI 1.15–3.62) studies (Fig. 5). In addition, PCR–RFLP genotyping method is better at revealing susceptibility of IL-1β-511 T allele carrier to gastric cancer than other PCR methods, such as, PCR–DHPLC and PCR–SSCP for both overall (OR = 1.24; 95 % CI 1.05–1.47) and HWE satisfying (OR = 1.28; 95 % CI 1.05–1.56) studies (Fig. 6). In terms of study quality, high-quality studies showed a correlation between IL-1β-511 T carrier and risk of stomach carcinoma. (OR = 1.17; 95 % CI 1.00–1.36) (Fig. 7). Anatomical location of cancer does not affect to the relationship between IL-1β-511 C/T SNP and stomach cancer in either overall (cardia OR = 0.98; 95 % CI 0.46–2.08, noncardia OR = 1.25; 95 % CI 0.60–2.60) or HWE satisfying (cardia OR = 0.66; 95 % CI 0.35–1.24, noncardia OR = 0.91, 95 % CI 0.66–1.26) studies (Fig. 8).

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) by ethnicity subgroups based on the Hardy–Weinberg equilibrium. The areas of the squares indicate the relative weights of the specific studies. Bars represent 95 % confidence intervals, and “GC,” gastric cancer

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) in the H. pylori-positive subgroup based on the Hardy–Weinberg equilibrium. The areas of the squares indicate the relative weights of the specific studies Bars represent 95 % confidence intervals, and “GC,” gastric cancer

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) according to genotyping method based on the Hardy–Weinberg equilibrium. The areas of the squares indicate the relative weights of the specific studies. Bars represent 95 % confidence intervals. GC gastric cancer, PCR polymerase chain reaction, RFLP restriction fragment length polymorphism

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) according to the study quality subgroup based on the Hardy–Weinberg equilibrium. The areas of the squares indicate the relative weights of the specific studies. Bars represent 95 % confidence intervals, and “GC,” gastric cancer

A forest plot of the stomach carcinoma risk of relevance to the interleukin-1β-511 C/T polymorphism (TT vs. CC+CT) according to histology subgroups based on the Hardy–Weinberg equilibrium. The areas of the squares indicate the relative weights of the specific studies. Bars represent 95 % confidence intervals, and “GC,” gastric cancer
Discussion
Gastric cancer maintains its second place position amongst the causes of cancer-associated mortality, and therefore, researchers worldwide have concentrated on unearthing its etiology. H. pylori is a major causative agent in gastric cancer and produces oxidative radicals, which are harmful to DNA stability and stimulate the secretion of the proliferative factor gastrin [1, 67]. Interleukin 1β (IL-1β) amplifies this mechanism through hypochlorhydria, which is favorable to H. pylori [4]. Nevertheless, the fact that not every H. pylori carrier develops stomach carcinoma strongly suggests a relation between IL-1β polymorphisms and stomach carcinoma susceptibility. Many studies have investigated this potential relationship since El-Omar et al. [8] first described a positive correlation between the IL-1β-511 C/T SNP and risk of stomach carcinoma. However, such studies and even meta-analyses have produced mixed results. In this context, the present meta-analysis draws comprehensive analysis regarding the strength of the relationship between the IL-1β-511 C/T SNP and gastric cancer risk by in-depth analysis and the removal of presumed factors of heterogeneity from previous studies. A total of 45 recent studies with 50 population data sets were considered after eliminating selection bias from unrefined searches and systematically searching the MEDLINE, EMBASE, and CENTRAL databases. In addition, clear criteria for excluding and including studies were set. As a result, 12 new studies were added, and the homogeneity of control groups was elaborated by eliminating studies that included premalignant gastric patients as an eligible control group. In addition, HWE studies were analyzed because a deviation from the HWE implies that the study may exhibit selection bias or have suffered some erroneous event during genotyping [16, 20]. Consequently, consistency with the HWE is critical for guaranteeing the appropriateness of control subjects for a given case control study and for verifying the credibility of a genotyping procedure.
In this meta-analysis, we found that the IL-1β-511 C/T SNP confers susceptibility to stomach carcinoma, which is in accordance with the results of six of the seven previous meta-analyses. It is noteworthy that some of our subgroup analysis results are inconsistent with the findings of previous meta-analyses.
With respect to ethnicity, Asian populations were found to show a positive relation between the presence of the IL-1β-511 T allele and the risk of stomach carcinoma in overall and HWE satisfying studies, which is inconsistent with the findings of three previous meta-analyses [10, 12, 13] that found no such relation. In the present meta-analysis, ten recently published Asian studies were included and five Caucasian studies were excluded because healthy individuals and patients with premalignant lesions such as ulcer, MALToma, and gastritis were not differentiated in control populations. In this regard, the large size of Asian populations included in the present study and the process used for selecting control populations probably affected the results.
In subgroup analysis of H. pylori carriers, it was shown that H. pylori infection reinforces the relation between IL-1β-511 T allele with susceptibility to gastric cancer in both overall and HWE satisfying studies. It provides support for the mechanism that IL-1β contributes to chronic inflammation by producing hypochlorhydria. Close attention should be paid to the fact that East Asian populations have generally high H. pylori infection rate and that Asian exhibited the strongest relationship between the IL-1β-511 C/T SNP and gastric cancer in our study. As explained above, IL-1β-511 C/T SNP makes IL-1β to be overexpressed, which suppresses acid secretion and thus creates favorable conditions for H. pylori proliferation. These findings suggest that Asian populations, which are particularly vulnerable to H. pylori infection, would have a strong relationship between the IL-1β-511 C/T SNP and gastric cancer.
In addition, the relationship between stomach carcinoma and the IL-1β-511 C/T SNP was noteworthy in studies that employed PCR–RFLP genotyping methods. Of the various genotyping methods used, PCR–RFLP method was employed most frequently (25 of the 50 population data sets). The PCR–RFLP method was the first DNA-profiling technique which was used for genetic fingerprinting, evaluating the risk of genetic disorders, and analyzing samples from crime scenes. The large pool of cases analyzed in previous studies using PCR–RFLP supports the validity of the method. In addition, the sensitivity of PCR–RFLP has been verified in many studies. Accordingly, the reliability and validity of this method support the observed relation between IL-1β-511 T allele and risk of gastric cancer.
A subgroup analysis according to study quality scores showed a positive association between the IL-1β-511 T allele and the risk of stomach carcinoma. Quality analysis was carried out utilizing the scale proposed by Thakkinstian et al. [7] and refined by Camargo et al. [12] and Xue et al. [13]. High-score studies were elaborated by designating the source of control groups, confirming the representativeness of cases, using reliable methods to confirm the presence of stomach carcinoma and to conduct genotyping. Classifying studies by quality reduced study heterogeneity because it ensured the reliabilities of control sources and case populations.
In the present study, only recessive model (TT vs. CT+CC) results are presented, but recessive model results are consistent with those of other models. In the additive model (TT vs. CC), pooled ORs (95 % CI) were 1.20 (1.00–1.45) for overall studies and 1.24 (1.02–1.57) for HWE satisfying studies. In addition, the dominant model (TT+CT vs. TT) produced insignificant results for overall studies (OR = 1.10; 95 % CI 0.97–1.24), but the susceptibility of IL-1β-511 T carriers for HWE satisfying studies (OR = 1.14; 95 % CI 1.01–1.27) (data not shown). A similar pattern was observed for ethnicity analysis. Caucasian populations showed no relationship for any model: TT+CT versus CC (overall: OR = 1.13; 95 % CI 0.89–1.42; HWE: OR = 1.12; 95 % CI 0.87–1.44) and TT versus CC (overall: OR = 1.23; 95 % CI 0.86–1.75; HWE: OR = 1.18; 95 % CI 0.87–1.62), whereas Asian in HWE satisfying studies showed statistical significance in all models: TT+CT vs. CC (OR = 1.15; 95 % CI 1.00–1.34) and TT versus CC (OR = 1.26; 95 % CI 1.04–1.54).
This meta-analysis has several limitations that should be considered. Although we evaluated publication bias comprehensively using a funnel plot, Egger’s test, and Begg’s test, the tendency not to publish negative results may have produced this bias. In addition, future research should provide updated systematic analysis on the relationship between gastric cancer and haplotypes of the gene family cluster on chromosome 2q, IL-1β-31 C, IL-1β +3954, and IL1RN, because a polymorphism in one gene is often accompanied instability of a nearby gene.
In summary, the results of this refined and updated meta-analysis verify the relationship between the IL-1β-511 T allele carrier and stomach carcinoma susceptibility. It also confirms that Asian ethnicity strengthens this relationship. In addition, the coexistence of IL-1β-511 C/T SNP and H. pylori infection was found to increase susceptibility to stomach carcinoma. The most reliable genotyping technique appears to be PCR–RFLP, which suggests that it should be used to analyze the relationship between the IL-1β-511 C/T SNP and the risk of stomach carcinoma. Thorough screening of eligible studies and the adoption of a strict study selection procedure based on the elimination of selection bias for control groups may explain reported inconsistencies across ethnic subgroups.
References
Rozengurt E, Walsh JH (2001) Gastrin, CCK, signaling, and cancer. Annu Rev Physiol 63:49–76
Ambs S, Merriam WG, Ogunfusika MO, Bennett WP, Ishibe N et al (1998) p53 and vascular endothelial growth factor regulate tumor growth of NOS2-expressing human carcinoma cells. Nat Med 4:1371–1376
Oger P, Dessaux Y, Petit A, Gardan L, Manceau C et al (1998) Validity, sensitivity and resolution limit of the PCR–RFLP analysis of the rrs (16S rRNA gene) as a tool to identify soil-borne and plant-associated bacterial populations. Genet Sel Evol 30:1–22
Kuipers EJ, Uyterlinde AM, Pena AS, Roosendaal R, Pals G et al (1995) Long-term sequelae of Helicobacter pylori gastritis. Lancet 345:1525–1528
Shin A, Kim J, Park S (2011) Gastric cancer epidemiology in Korea. J Gastric Cancer 11:135–140
Logan RPH, Walker MM (2001) Epidemiology and diagnosis of Helicobacter pylori infection. BMJ 323:920–922
Thakkinstian A, McEvoy M, Minelli C, Gibson P, Hancox B et al (2005) Systematic review and meta-analysis of the association between {beta}2-adrenoceptor polymorphisms and asthma: a HuGE review. Am J Epidemiol 162:201–211
El-Omar EM, Carrington M, Chow WH, McColl KE, Bream JH et al (2000) Interleukin-1 polymorphisms associated with increased risk of gastric cancer. Nature 404:398–402
Cox A, Camp NJ, Nicklin MJ, di Giovine FS, Duff GW (1998) An analysis of linkage disequilibrium in the interleukin-1 gene cluster, using a novel grouping method for multiallelic markers. Am J Hum Genet 62:1180–1188
Vincenzi B, Patti G, Galluzzo S, Pantano F, Venditti O et al (2008) Interleukin 1beta-511 T gene (IL1beta) polymorphism is correlated with gastric cancer in the Caucasian population: results from a meta-analysis. Oncol Rep 20:1213–1220
Wang P, Xia HH, Zhang JY, Dai LP, Xu XQ et al (2007) Association of interleukin-1 gene polymorphisms with gastric cancer: a meta-analysis. Int J Cancer 120:552–562
Camargo MC, Mera R, Correa P, Peek RM Jr, Fontham ET et al (2006) Interleukin-1beta and interleukin-1 receptor antagonist gene polymorphisms and gastric cancer: a meta-analysis. Cancer Epidemiol Biomark Prev 15:1674–1687
Xue H, Lin B, Ni P, Xu H, Huang G (2010) Interleukin-1B and interleukin-1 RN polymorphisms and gastric carcinoma risk: a meta-analysis. J Gastroenterol Hepatol 25:1604–1617
Song H, Peng JS, Yang ZL, Xiang J (2010) Association of interleukin-1 gene polymorphisms with susceptibility of gastric cancer: a meta-analysis of chinese population. Chinese Journal of Cancer Prevention and Treatment 17:1705–1710
Kamangar F, Cheng C, Abnet CC, Rabkin CS (2006) Interleukin-1B polymorphisms and gastric cancer risk—a meta-analysis. Cancer Epidemiol Biomark Prev 15:1920–1928
Tiret L, Cambien F (1995) Departure from Hardy-Weinberg equilibrium should be systematically tested in studies of association between genetic markers and disease. Circulation 92:3364–3365
Thompson SG, Pocock SJ (1991) Can meta-analyses be trusted? Lancet 338:1127–1130
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719–748
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Gyorffy B, Kocsis I, Vasarhelyi B (2004) Biallelic genotype distributions in papers published in Gut between 1998 and 2003: altered conclusions after recalculating the Hardy–Weinberg equilibrium. Gut 53: 614–615; author reply 615-616
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Zeng ZR, Hu PJ, Hu S, Pang RP, Chen MH et al (2003) Association of interleukin 1B gene polymorphism and gastric cancers in high and low prevalence regions in China. Gut 52:1684–1689
Perri F, Piepoli A, Bonvicini C, Gentile A, Quitadamo M et al (2005) Cytokine gene polymorphisms in gastric cancer patients from two Italian areas at high and low cancer prevalence. Cytokine 30:293–302
Persson C, Engstrand L, Nyren O, Hansson LE, Enroth H et al (2009) Interleukin 1-beta gene polymorphisms and risk of gastric cancer in Sweden. Scand J Gastroenterol 44:339–345
Zhao JD, Geng PL, Li ZQ, Cui S, Zhao JH et al (2012) Associations between interleukin-1 polymorphisms and gastric cancers among three ethnicities. World J Gastroenterol 18:7093–7099
Burada F, Angelescu C, Mitrut P, Ciurea T, Cruce M et al (2012) Interleukin-4 receptor −3223T → C polymorphism is associated with increased gastric adenocarcinoma risk. Can J Gastroenterol 26:532–536
He BS, Pan YQ, Xu YF, Zhu C, Qu LL et al (2011) Polymorphisms in interleukin-1B (IL-1B) and interleukin 1 receptor antagonist (IL-1RN) genes associate with gastric cancer risk in the Chinese population. Dig Dis Sci 56:2017–2023
Wex T, Leodolter A, Bornschein J, Kuester D, Kahne T et al (2010) Interleukin 1 beta (IL1B) gene polymorphisms are not associated with gastric carcinogenesis in Germany. Anticancer Res 30:505–511
Yu J, Zeng Z, Wang S, Tian L, Wu J et al (2010) IL-1β-511 polymorphism is associated with increased risk of certain subtypes of gastric cancer in Chinese: a case-control study. Am J Gastroenterol 105:557–564
Melo Barbosa HP, Martins LC, Dos Santos SE, Demachki S, Assumpcao MB et al (2009) Interleukin-1 and TNF-alpha polymorphisms and Helicobacter pylori in a Brazilian Amazon population. World J Gastroenterol 15:1465–1471
Kumar S, Kumar A, Dixit VK (2009) Evidences showing association of interleukin-1B polymorphisms with increased risk of gastric cancer in an Indian population. Biochem Biophys Res Commun 387:456–460
Feng Y, Zhang J, Dai L, Zhang J, Wang P et al (2008) Inflammatory cytokine gene polymorphisms in gastric cancer cases’ and controls’ family members from Chinese areas at high cancer prevalence. Cancer Lett 270:250–259
Shin WG, Jang JS, Kim HS, Kim SJ, Kim KH et al (2008) Polymorphisms of interleukin-1 and interleukin-2 genes in patients with gastric cancer in Korea. J Gastroenterol Hepatol 23:1567–1573
Garcia-Gonzalez MA, Lanas A, Quintero E, Nicolas D, Parra-Blanco A et al (2007) Gastric cancer susceptibility is not linked to pro-and anti-inflammatory cytokine gene polymorphisms in whites: a Nationwide Multicenter Study in Spain. Am J Gastroenterol 102:1878–1892
Sun H, Wang Y, Ma X, Pei F, Sun H et al (2007) A method of oligochip for single nucleotide polymorphism genotyping in the promoter region of the interleukin-1 beta gene and its clinical application. Oligonucleotides 17:336–344
Sugimoto M, Furuta T, Shirai N, Nakamura A, Xiao F et al (2007) Different effects of polymorphisms of tumor necrosis factor-alpha and interleukin-1 beta on development of peptic ulcer and gastric cancer. J Gastroenterol Hepatol 22:51–59
Li C, Xia HH, Xie W, Hu Z, Ye M et al (2007) Association between interleukin-1 gene polymorphisms and Helicobacter pylori infection in gastric carcinogenesis in a Chinese population. J Gastroenterol Hepatol 22:234–239
Ito H, Kaneko K, Makino R, Konishi K, Kurahashi T et al (2007) Interleukin-1beta gene in esophageal, gastric and colorectal carcinomas. Oncol Rep 18:473–481
Zhang D, Zheng H, Zhou Y, Tang X, Yu B et al (2007) Association of IL-1beta gene polymorphism with cachexia from locally advanced gastric cancer. BMC Cancer 7:45
Kamangar F, Abnet CC, Hutchinson AA, Newschaffer CJ, Helzlsouer K et al (2006) Polymorphisms in inflammation-related genes and risk of gastric cancer (Finland). Cancer Causes Control 17:117–125
Kim N, Cho SI, Yim JY, Kim JM, Lee DH et al (2006) The effects of genetic polymorphisms of IL-1 and TNF-A on Helicobacter pylori-induced gastroduodenal diseases in Korea. Helicobacter 11:105–112
Shirai K, Ohmiya N, Taguchi A, Mabuchi N, Yatsuya H et al (2006) Interleukin-8 gene polymorphism associated with susceptibility to non-cardia gastric carcinoma with microsatellite instability. J Gastroenterol Hepatol 21:1129–1135
Ikehara SK, Ikehara Y, Matsuo K, Hirose K, Niwa T et al (2006) A polymorphism of C-to-T substitution at -31 IL1B is associated with the risk of advanced gastric adenocarcinoma in a Japanese population. J Hum Genet 51:927–933
Morgan DR, Dominguez RL, Keku TO, Heidt PE, Martin CF et al (2006) Gastric cancer and the high combination prevalence of host cytokine genotypes and Helicobacter pylori in Honduras. Clin Gastroenterol Hepatol 4:1103–1111
Alpizar-Alpizar W, Perez-Perez GI, Une C, Cuenca P, Sierra R (2005) Association of interleukin-1B and interleukin-1RN polymorphisms with gastric cancer in a high-risk population of Costa Rica. Clin Exp Med 5:169–176
Lu W, Pan K, Zhang L, Lin D, Miao X et al (2005) Genetic polymorphisms of interleukin (IL)-1B, IL-1RN, IL-8, IL-10 and tumor necrosis factor alpha and risk of gastric cancer in a Chinese population. Carcinogenesis 26:631–636
Taguchi A, Ohmiya N, Shirai K, Mabuchi N, Itoh A et al (2005) Interleukin-8 promoter polymorphism increases the risk of atrophic gastritis and gastric cancer in Japan. Cancer Epidemiol Biomark Prev 14:2487–2493
Muramatsu A, Azuma T, Okuda T, Satomi S, Ohtani M et al (2005) Association between interleukin-1beta-511 C/T polymorphism and reflux esophagitis in Japan. J Gastroenterol 40:873–877
Sakuma K, Uozaki H, Chong JM, Hironaka M, Sudo M et al (2005) Cancer risk to the gastric corpus in Japanese, its correlation with interleukin-1beta gene polymorphism (+3953*T) and Epstein-Barr virus infection. Int J Cancer 115:93–97
Chang YW, Jang JY, Kim NH, Lee JW, Lee HJ et al (2005) Interleukin-1B (IL-1B) polymorphisms and gastric mucosal levels of IL-1beta cytokine in Korean patients with gastric cancer. Int J Cancer 114:465–471
Ruzzo A, Graziano F, Pizzagalli F, Santini D, Battistelli V et al (2005) Interleukin 1B gene (IL-1B) and interleukin 1 receptor antagonist gene (IL-1RN) polymorphisms in Helicobacter pylori-negative gastric cancer of intestinal and diffuse histotype. Ann Oncol 16:887–892
Zhang WH, Wang XL, Zhou J, An LZ, Xie XD (2005) Association of interleukin-1B (IL-1B) gene polymorphisms with risk of gastric cancer in Chinese population. Cytokine 30:378–381
Yang J, Hu Z, Xu Y, Shen J, Niu J et al (2004) Interleukin-1B gene promoter variants are associated with an increased risk of gastric cancer in a Chinese population. Cancer Lett 215:191–198
Lee KA, Ki CS, Kim HJ, Sohn KM, Kim JW et al (2004) Novel interleukin 1beta polymorphism increased the risk of gastric cancer in a Korean population. J Gastroenterol 39:429–433
Glas J, Torok HP, Schneider A, Brunnler G, Kopp R et al (2004) Allele 2 of the interleukin-1 receptor antagonist gene is associated with early gastric cancer. J Clin Oncol 22:4746–4752
Chen A, Li CN, Hsu PI, Lai KH, Tseng HH et al (2004) Risks of interleukin-1 genetic polymorphisms and Helicobacter pylori infection in the development of gastric cancer. Aliment Pharmacol Ther 20:203–211
Kang WK, Park WS, Chin HM, Park CH (2004) The role of interleukin-1beta gene polymorphism in the gastric carcinogenesis. Korean J Gastroenterol 44:25–33
Hartland S, Newton JL, Griffin SM, Donaldson PT (2004) A functional polymorphism in the interleukin-1 receptor-1 gene is associated with increased risk of Helicobacter pylori infection but not with gastric cancer. Dig Dis Sci 49:1545–1550
Gatti LL, Burbano RR, de Assumpcao PP, Smith Mde A, Payao SL (2004) Interleukin-1beta polymorphisms, Helicobacter pylori infection in individuals from Northern Brazil with gastric adenocarcinoma. Clin Exp Med 4:93–98
Wu MS, Chen LT, Shun CT, Huang SP, Chiu HM et al (2004) Promoter polymorphisms of tumor necrosis factor-alpha are associated with risk of gastric mucosa-associated lymphoid tissue lymphoma. Int J Cancer 110:695–700
Machado JC, Figueiredo C, Canedo P, Pharoah P, Carvalho R et al (2003) A proinflammatory genetic profile increases the risk for chronic atrophic gastritis and gastric carcinoma. Gastroenterology 125:364–371
El-Omar EM, Rabkin CS, Gammon MD, Vaughan TL, Risch HA et al (2003) Increased risk of noncardia gastric cancer associated with proinflammatory cytokine gene polymorphisms. Gastroenterology 124:1193–1201
Wu MS, Wu CY, Chen CJ, Lin MT, Shun CT et al (2003) Interleukin-10 genotypes associate with the risk of gastric carcinoma in Taiwanese Chinese. Int J Cancer 104:617–623
zur Hausen A, Crusius JB, Murillo LS, Alizadeh BZ, Morre SA et al (2003) IL-1B promoter polymorphism and Epstein-Barr virus in Dutch patients with gastric carcinoma. Int J Cancer 107:866–867
Machado JC, Pharoah P, Sousa S, Carvalho R, Oliveira C et al (2001) Interleukin 1B and interleukin 1RN polymorphisms are associated with increased risk of gastric carcinoma. Gastroenterology 121:823–829
Johnson LR, Guthrie PD (1976) Stimulation of DNA synthesis by big and little gastrin (G-34 and G-17). Gastroenterology 71:599–602
Author information
Authors and Affiliations
Corresponding author
Additional information
Min-Jeong Park and Myung-Han Hyun contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Park, MJ., Hyun, MH., Yang, JP. et al. Effects of the interleukin-1β-511 C/T gene polymorphism on the risk of gastric cancer in the context of the relationship between race and H. pylori infection: a meta-analysis of 20,000 subjects. Mol Biol Rep 42, 119–134 (2015). https://doi.org/10.1007/s11033-014-3748-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-014-3748-7