
Abstract
This study aimed to determine the relation between methylene-tetrahydrofolate reductase (MTHFR) gene polymorphism and lung cancer risk and the frequency of this polymorphism. The study involved 64 lung cancer patients (the study group) with definitive diagnosis and 61 noncancerous subjects (the control group). MTHFR C677T and A1298C mutation analysis was made using DNA isolated from peripheric blood and multiplex PCR and reverse hybridization strip test. Eighty-four percent of the patients were male. The age, gender, and history of alcohol use of the patients and control group were statistically similar. While MTHFR 677T and 677C allele frequency was 0.33 and 0.67 in the patients respectively, it was 0.29 and 0.71 in the control group. The frequencies of MTHFR 1298C and 1298A were 0.33 and 0.67 in the patients, and it was 0.31 and 0.69 in the control group respectively. When MTHFR 677TT and 677CT genotypes were compared with 677CC genotype, lung cancer risk was 2.4 times higher in the 677TT genotype. When MTHFR 1298AC and 1298CC genotypes were compared with 1298AA genotype, lung cancer risk was 1.5 times higher in 1298CC genotype. According to the results, allele frequency of homozygote T and C was high in lung cancer patients. It was 3.05 and 1.29 times higher in smokers than in non-smokers, and 3.05 and 1.64 times higher in males than in females; 3.0 and 2.44 times higher in those with non-small cell lung cancer than in those with small-cell lung cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung Cancer (LC) has become the most common type of cancer worldwide with the increase in smoking habit [1]. It is responsible for 12.8% of the cancer cases and 17.8% of cancer related deaths worldwide [2]. Just in 2001, LC caused more than one million deaths [1, 3]. Although smoking is the primary risk factor for lung cancer, LC develops in less than 20% of people who smoke throughout their life [4]. This shows that genetic susceptibility and nutritional habits of an individual increase the risk of LC [5, 6]. The risk of lung cancer development is increased by active and passive smoking, carcinogens in polluted air, carcinogen activation by various occupational exposures as well as by individual genetic factors [7]. The genes coding some enzymes like polycyclic aromatic hydrocarbons and aromatic amines, which act in the detoxification and metabolic activation of pulmonary carcinogens in humans, are known to be polymorphic [8].
Numerous epidemiological studies have pointed out that low dietary folate intake is an important factor in development of cancer including lung, breast, colorectum, bladder and pancreas [9–13]. Folate is involved in DNA methylation, synthesis, and repair [14]. In all of these events, folate serves as one-carbon donor and its metabolic product provides methyl group for both synthesis of methionine and DNA methylation [15]. Folate deficiency may cause uracil misincorporation and subsequent DNA instability, retarded DNA repair capacity for oxidative or alkylating damage, and global and proto-oncogenic DNA hypomethylation [14].
MTHFR is an FAD-dependent enzyme, which catalyzes the irreversible conversion of 5,10 methylenetetrahydrofolate to 5-methyltetrahydrofolate. Five-Methyltetrahydrofolate in turn serves as a methyl donor in the remethylation of homocysteine (Hcy) to methionine. The enzyme, therefore, resides at an important metabolic branch point directing the folate pool towards Hcy remethylation and DNA methylation at the expense of DNA and RNA biosynthesis [16]. There are two well-described polymorphisms in the MTHFR gene: A1298C and C677T. The C677T polymorphism occurs in exon 4 and results in alanine to valine substitution at codon 222 [17]. It has been shown that individuals who have homozygous mutation at this codon lose MTHFR enzyme activity approximately by 70% [18]. A1298C polymorphism resides in exon 7 of MTHFR gene and results in glutamate-to-alanine substitution at codon 429 [19].
In this study, the relation between MTHFR Gene Polymorphism and LC risk and the frequency of this polymorphism were investigated in the population of Central Anatolia.
Study population
The study was approved by the Ethics Committee of Medical faculty of Cumhuriyet University, Sivas, Turkey, and written informed consent was obtained from all individuals or their legal guardians. This study involved 64 patients whose definitive diagnosis of LC was made in our thoracic diseases clinic between 2007 and 2009. The patients were genotyped and were compared histologically in terms of small-cell carcinoma (SCLC) and non-small cell carcinoma (NSCLC). A control group consisting of 61 people were formed. The age, gender, smoking habit, body mass index (BMI), alcohol consumption of the patient and control groups was recorded. The patients were divided into 3 groups according to their smoking habits as: none smokers (NS), who never smoked throughout their life, ex-smokers (ES) who smoked before but stopped smoking for at least the last one year, active smokers (AS) who started smoking before and continued smoking within the last one year. Active smokers (AS) and ex-smokers (ES) were included in the ever smoking group. Smoking period was calculated as pack-years of smoking. The patients were then allocated into two groups in terms of alcohol consumption habits: “ever drinkers” who used alcohol at least once a week for one year or more up until now and “never drinkers” as the rest of the patients.
Mutation analysis
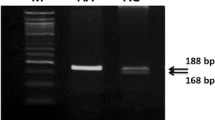
Total genomic DNA was extracted from the peripheral blood samples using DNA isolation kit according to manufacturer’s instruction (Invitek Invisorb Spin Blood Kit, Germany). Isolated DNA samples were screened for two MTHFR gene polymorphism (C677T and A1298C) using reverse hybridization strip assay (Vienna Lab, CVD Strip Assay, GMBH, Austria). Relevant gene sequences were simultaneously in vitro amplified and biotin labeled in a single (multiplex) amplification reaction. PCR conditions were as follows: pre-PCR, 2 min at 95°C; denaturation, 15 s at 95°C; annealing 30 s at 56°C; extension 30 s at 72°C, and final extension 3 min at 72°C. The amplification products were selectively hybridized to a test strip, which contains allele-specific (wild type and mutant) oligonucleotide probes immobilized as an array of parallel lines. Bound biotinylated sequences were detected using streptavidin-alkaline phosphatise and color substrates. Hybridization was performed in an automated incubator (Auto-LIPA, İnnogenetics).
Statistical analysis
Statistical analysis was performed using SPSS 14.0 program (SPSS Inc., Chicago, IL, USA). Student’s t test was performed for BMI, pack-year of smoking, and mean age. χ2 test was used to evaluate alcohol consumption, gender differences, allele and genotype frequency. The odds ratios (OR) for relation between genotypes and the risk in the formation of LC were calculated at 95% confidence interval, and P < 0.05 was considered statistically significant.
Results
The patient group consisted of 54 male (84%) and 10 female (16%) subjects. The mean age of the patients was 60.8 ± 9.0 years (Range: 32–77 years). The control group consisted of 52 male (85%) and 9 female (15%) subjects. The mean age of the control group subjects was 58.7 ± 8.7 years (Range: 28–75 years). No statistically significant differences were found between the age, gender, and alcohol intake of the patient and control groups. Pack-year of smoking of the patients (32.83 ± 13.5 year) was higher than that of the control group (24.3 ± 11.5 year) (P < 0.001). Body mass index (BMI) of the patients (23.1 ± 5.5) was lower than BMI of the control group (P < 0.001). The characteristics of the patients and the control group are shown in Table 1.
Distribution of MTHFR variant allele and genotypes in the patient and control groups is presented in Table 2. While MTHFR 677T and 677C allele frequencies were 0.33 and 0.67 in cancer patients respectively, they were 0.29 and 0.71 in the control group. Similarly, while MTHFR 1298C and 1298A frequencies were 0.33 and 0.67 in cancer patients, they were 0.31 and 0.69 in the control group respectively. There were no differences between the patient and control groups for these variant alleles (For C677T, P = 0.445 and for A1298C, P = 0.841). When 677TT genotype of MTHFR was compared to its 677CC genotype, a 2.4 times higher risk of LC was determined with 677TT genotype (Table 2). Similarly, when MTHFR homozygote mutant MTHFR 1298CC genotype was compared to wild type 1298AA genotype, there was a 1.5 times higher risk of LC (Table 2). When genotype frequencies were evaluated for genders and smoking status, 677TT genotype of MTHFR presented 3 times higher risk of LC in smokers, whereas the risk was 1.3 times in 1298CC genotype (Table 3). Similarly, while 677TT genotype MTHFR showed 3 times higher risk of LC in men, the risk was 1.6 times higher in 1298CC genotype (Table 3).
When genotype frequencies of NSCLC and SCLC histological types were evaluated, it was determined that MTHFR 677CT and 677TT genotypes were 2.1 and 3 times higher respectively in the NSCLC group compared to the SCLC group (Table 4). The frequencies of the 1298AC and 1298CC genotypes of MTHFR were 2.6 and 2.4 times higher in NSCLC group compared to the SCLC group (Table 4).
Discussion
To the best of our knowledge, this study, which evaluated the relation between MTHFR gene polymorphism and risk of LC development in 64 patients and 61 control subjects from Sivas, the Central Anatolia Region of Turkey, is the first of its kind in Turkey.
Enzyme activity has been shown to decrease in people with 677TT genotype [18]. MTHFR gene presents wide-spread polymorphism in two different regions. From the exon 4, 222nd codon belonging to the gene region, normally alanin aminoacid is synthesized, but during this process, missence mutation that develops in the form of leads to amionoacid synthesis rather than valin alanin synthesis. This leads to a reduction in the enzyme activity. Reduction in the MTHFR enzymatic activity may increase the risk of cancer development as a result of the change in the DNA methylation associated with reduced level of 5-methyltetrahydrofolate. In conformity with this hypothesis, in people with 677TT genotype, higher risk of breast and esophagus cancer has been reported [20–22]. Few studies have evaluated the relationship between MTHFR C677T polymorphism and LC risk. Siemianowicz et al. [23], in their case-control study on 146 patients and 44 controls, determined a significant relationship between 677TT genotype and LC risk. However, in the study by Shen et al. [24] on 550 patients and 554 controls, no significant relationship was determined between C677T polymorphism and LC risk. In another study with 59 patients and 232 controls, no relationship was found between 677TT genotype and LC risk (OR, 0.71; 95% CI, 0.39–1.30) [25]. In our study, in subjects with 677TT genotype, the risk of LC was 2.4 times higher than the risk in the control subjects. However, this increase was not statistically significant.
MTHFR A1298C polymorphism leads to the reduction of enzyme activity by replacement of glutamic acid with alanine in the 7th exon 429th codon [19]. In two earlier studies [23, 24], no significant relationship was found between 1289T and TT polymorphism and LC risk. Qiuling et al. [2] found no statistically significant relationships although MTHFR 1298C and CC genotypes had a higher risk of LC. In our study, MTHFR1298CC genotype presented lower rate of risk for LC than MTHFR 677TT genotype, but a higher rate of risk than MTHFR 1298AA genotype. The difference, however, was not statistically significant.
The degree of smoking-associated DNA damage in the tumor and adjacent tissues of females has been reported to be higher than that of both smoking and non-smoking males [28–30]. In one study, it was suggested that women tended to have less capacity for DNA repair than men [12]. These findings suggest that intake of food that enhance the capacity for DNA repair and synthesis may prove more beneficial for women than men. Qiuling et al. [26], in their case-controlled study, evaluated the relationship between gender and MTHFR polymorphism and found that 1289CC genotype showed a higher risk for LC (OR, 2.09; 95% CI, 1.32–3.29), whereas 677TT genotype had a lower risk for LC (OR, 0.60; 95% CI, 0.40–0.92). These rates were not statistically significant in males (for 1289CC: OR, 0.95; 95% CI, 0.62–1.45; for 677TT: OR, 1.09: 95% CI, 0.72–1.65). In the same study, there was a higher rate of 1298CC in smoking females (OR, 2.25; CI, 1.19–4.23), while it was lower in smoking males (OR;0.44: CI, 0.20–0.95). Suzuki et al. [27] determined no significant relationships between 1298CC and 677TT genotypes and LC risk in smoking individuals. In our study, although the rates of 1298CC and 677TT genotypes were higher in the male LC cases, the differences were not statistically significant (For 1298CC: OR, 3.05:CI, 0.52–10.68 and for 677CC: OR, 1.64: CI, 0.32–9.14). The rates of these two genotypes in females were the same, and the differences were not statistically significant (for both genotypes: OR, 0.95: CI, 0.03–35.77). However, this may have been due to the low number of female cases included in the study. In our study, the rates of 1298CC and 677TT genotypes were higher in smoking individuals and LC cases. However, the difference was not statistically significant.
Literature presents few studies that have evaluated the relationship between NSCLC and SCLC and MTHFR gene polymorphism. Siemianowicz et al. [23] determined a significant relationship between 677TT genotype and risk of NSCLC development. In another study [27], it was determined that those with MTHFR 677T and 1298C alleles had lower risk of squamous/small cell carcinoma (P = 0.029). In our study, the rates of 677T and 677TT alleles were 2.13 and 3 times higher in the NSCLC cases than in the SCLC cases. However, the differences were not statistically significant. Similarly, although the rates of 1298C and 1298CC genotypes were 2.6 and 2.4 times higher in the NSCLC group, the differences were not statistically significant.
The values of the present study for some parameters were either higher of different from those of the control group, but the differences were not statistically significant. This may have been associated with the limited number of patients. Another drawback of our study was the lack of reliable information provided by the patients on their nutritional habits and lack of sufficient diet analysis for folate intake. Studies with larger series are needed to confirm our findings for our country.
The distribution of alleles in 61 individuals with no cancer were as follows MTHFR 677CC genotype: 48%, CT genotype: 48%, and TT genotype: 5%. These rates have been reported to be as follows in different regions of the world: for Canada, 43, +6, and 11% respectively in a control group of 260 individuals [31]; for Texas: 44, 46, and 11% respectively in a control group of 1141 individuals [26]; for California: 45, 43, and 12% respectively in a control group of 1964 individuals [32]; and for Japan: 37, 46, and 17% respectively in a control group of 1030 individuals [27].
According to our results, the rates of TT genotypes were less than half those of the other reported series, while the rates for the other genotypes were similar to those reported in the literature. In our study, the distribution of MTHFR 1298AA, AC, and CC genotypes were 46, 48, and 75% respectively. In the study from Texas [26], these rates were found to be 49, 44, and 8%; from California (33), 47, 42, and 11%; from Japan [27], 63, 31, and 4%; from Italy [33], 49, 43, and 8%. The data collected in this study from the city of Sivas vicinity in the Mid-Anatolia region of Turkey were compatible with the literature.
In conclusion, the rates of 677TT and 1298CC alleles were higher in those with LC, and the rates for smokers were 3.05 and 1.29 times; for males, 3.05 and 1.64 times, and for those with NSCLC, 3.0 and 2.44 times higher. The distribution of the alleles was similar to those reported for different parts of the world. However, further studies with larger series of Turkish cases are needed to confirm our results.
References
Spiro SG, Porter JC (2002) Lung cancer—where are we today? Current advances in staging and nonsurgical treatment. Am J Respir Crit Care Med 166:1166–1196
Parkin GM, Pisani P, Ferlay J (1999) Global cancer statistics. CA Cancer J Clin 49:33–64
Postmus PE (1998) Epidemiology of lung cancer. In: Fishman AP, Elias JA, Fishman JA et al (eds) Fishman’s pulmonary diseases and disorders. McGraw Hill Companies, New York, pp 1707–1719
Shields PG (2002) Molecular epidemiology of smoking and lung cancer. Oncogene 21:6870–6876
Spitz MR, Wei Q, Dong Q, Amos CI, Wu X (2003) Genetic susceptibility to lung cancer: the role of DNA damage and repair. Cancer Epidemiol Biomarkers Prev 12:689–698
World Cancer Research Fund, American Institute for Cancer Research Expert Panel (Potter JD, chair) (1997) Food, nutrition and the prevention of cancer: a global perspective. American Institute for Cancer Research, Washington (DC)
Perera FP (1998) Molecular epidemiology of environmental carcinogenesis. Recent Results Cancer Res 154:39–46
Raunio H, Husgafvel-Pursiainen K, Anttila S, Hietanen E, Hirvonen A, Pelkonen O (1995) Diagnosis of polymorphisms in carcinogen activating and inactivating enzymes and cancer susceptibility. Gene 159:113–121
Shen H, Wei Q, Pillow PC, Amos CI, Hong WK, Spitz MR (2003) Dietary folate intake and lung cancer risk in former smokers: a case control analysis. Cancer Epidemiol Biomarkers Prev 12:980–986
Larsson SC, Håkansson N, Giovannucci E, Wolk A (2006) Folate intake and pancreatic cancer incidence: a prospective study of Swedish women and men. J Natl Cancer Inst 98(6):407–413
Schabath MB, Spitz MR, Lerner SP, Pillow PC, Hernandez LM, Delclos GL, Grossman HB, Wu X (2005) Case-control analysis of dietary folate and risk of bladder cancer. Nutr Cancer 53(2):144–151
Shrubsole MJ, Gao YT, Cai Q, Shu XO, Dai Q, Hébert JR, Jin F, Zheng W (2004) MTHFR polymorphisms, dietary folate intake, and breast cancer risk: results from the Shanghai breast cancer study. Cancer Epidemiol Biomarkers Prev 13:190–196
Choi SW, Mason JB (2002) Folate status: effects on pathways of colorectal carcinogenesis. J Nutr 132:2413–2418
Xu WH, Shrubsole MJ, Xiang YB, Cai Q, Zhao GM, Ruan ZX, Cheng JR, Zheng W, Shu XO (2007) Dietary folate intake, MTHFR genetic polymorphisms, and the risk of endometrial cancer among Chinese woman. Cancer Epidemiol Biomarkers Prev 16(2):281–287
Heijmans BT, Boer JMA, Suchiman HED, Cornelisse CJ, Westendorp RGJ, Kromhout D, Feskens EJM, Slagboom PE (2003) A common variant of the methylenetetrahydrofolate reductase gene (1p36) is associated with an increased risk of cancer. Cancer Res 63:1249–1253
Leclerc D, Sibani S, Rosen R (2005) Molecular biology of methylenetetrahydrofolate reductase (MTHFR) and overview of mutations/polymorphisms. In: Ueland PM, Rozen R (eds) MTHFR polymorphisms and disease. Landes Bioscience, Texas, USA, pp 1–20
Robien K, Ulrich CM (2003) 5, 10-Methylenetetrahydrofolate reductase polymorphisms and leukemia risk: a HuGE minireview. Am J Epidemiol 157:571–582
Frosst P, Blom HJ, Milos R, Goyette P, Sheppard CA, Matthews RG, Boers GJH, den Heijer M, Kluijtmans LAJ, van den Heuve LP, Rozen R (1995) A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet 10:111–113
Weisberg I, Tran P, Christensen B, Sibani S, Rozen R (1998) A second genetic polymorphism in methylenetetrahydrofolate reductase (MTHFR) associated with decreased enzyme activity. Mol Genet Metab 64:169–172
Ergul E, Sazci A, Utkan Z, Canturk NZ (2003) Polymorphisms in the MTHFR gene are associated with breast cancer. Tumour Biol 24:286–290
Stolzenberg-Solomon RZ, Qiao YL, Abnet CC, Ratnasinghe DL, Dawsey SM, Dong ZW, Taylor PR, Mark SD (2003) Esophageal and gastric cardia cancer risk and folate- and vitamin B (12)-related polymorphisms in Linxian, China. Cancer Epidemiol Biomarkers Prev 12:1222–1226
Song C, Xing D, Tan W, Wei Q, Lin D (2001) Methylenetetrahydrofolate reductase polymorphisms increase risk of esophageal squamous cell carcinoma in a Chinese population. Cancer Res 61:3272–3275
Siemianowicz K, Gminski J, Garczorz W, Slabiak N, Goss M, Machalski M, Magiera-Molendowska H (2003) Methylenetetrahydrofolate reductase gene C677T and A1298C polymorphisms in patients with small cell and non-small cell lung cancer. Oncol Rep 10:1341–1344
Shen H, Spitz MR, Wang LE, Hong WK, Wei Q (2001) Polymorphisms of methylene-tetrahydrofolate reductase and risk of lung cancer: a case-control study. Cancer Epidemiol Biomarkers Prev 10:397–401
Jeng YL, Wu MH, Huang HB, Lin WY, You SL, Chu TY, Chen CJ (2003) The methylenetetrahydrofolate reductase 677C → T polymorphism and lung cancer risk in a Chinese population. Anticancer Res 23:5149–5152
Shi Q, Zhang Z, Li G, Pillow PC, Hernandez LM, Spitz MR, Wei Q (2005) Sex differences in risk of lung cancer associated with methylene-tetrahydrofolate reductase polymorphisms. Cancer Epidemiol Biomarkers Prev 14(6):1477–1484
Suzuki T, Matsuo K, Hiraki A, Saito T, Sato S, Yatabe Y, Mitsudomi M, Hida T, Ueda R, Tajima K (2007) Impact of one-carbon metabolism-related gene polymorphisms on risk of lung cancer in Japan: a case–control study. Carcinogenesis 28(8):1718–1725
Ryberg D, Hewer A, Phillips DH, Haugen A (1994) Different susceptibility to smoking-induced DNA damage among male and female lung cancer atients. Cancer Res 54:5801–5803
Mollerup S, Ryberg D, Hewer A, Phillips DH, Haugen A (1999) Sex differences in lung CYP1A1 expression and DNA adduct levels among lung cancer patients. Cancer Res 59:3317–3320
Cheng YW, Hsieh LL, Lin PP, Chen CP, Chen CY, Lin TS, Su SM (2001) Gender difference in DNA adduct levels among nonsmoking lung cancer patients. Environ Mol Mutagen 37:304–310
Kelemen LE, Anand SS, Hegele RA, Stampferef MJ, Rosnerf B, Willettef WC, Montague PA (2004) Associations of plasma homocysteine and the methylenetetrahydrofolate reductase C677T polymorphism with carotid intima media thickness among South Asian, Chinese and European Canadians. Atherosclerosis 176:361–370
Curtin K, Bigler J, Slattery ML, Caan B, Potter JD, Ulrich CM (2004) MTHFR C677T and A1298C polymorphisms: diet, estrogen, and risk of colon cancer. Cancer Epidemiol Biomarkers Prev 13:285–292
Gemmati D, Ongaro A, Scapoli GL, Porta MD, Tognazzo S, Serino ML, Bona ED (2004) Common gene polymorphisms in the metabolic folate and methylation pathway and the risk of acute lymphoblastic leukemia and non Hodgkin’s lymphoma in adults. Cancer Epidemiol Biomarkers Prev 13:787–794
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arslan, S., Karadayi, S., Yildirim, M.E. et al. The association between methylene-tetrahydrofolate reductase gene polymorphism and lung cancer risk. Mol Biol Rep 38, 991–996 (2011). https://doi.org/10.1007/s11033-010-0194-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-010-0194-z