
Abstract
Published data on the association between TGFBR1*6A/9A polymorphism and cancer risk are inconclusive. To derive a more precise estimation of the relationship, a meta-analysis was performed. A total of 32 studies including 13,662 cases and 14,147 controls were involved in this meta-analysis. Overall, significantly elevated cancer risks were associated with TGFBR1*6A in all genetic models (for allelic effect: OR = 1.11; 95% CI = 1.03–1.21; for 6A/6A vs. 9A/9A: OR = 1.30; 95% CI = 1.01–1.69; for 9A/6A vs. 9A/9A: OR = 1.08; 95% CI = 1.01–1.15; for dominant model: OR = 1.08; 95% CI = 1.02–1.15; for recessive model: OR = 1.29; 95% CI = 1.00–1.68). In the subgroup analysis by cancer types, significant associations were found in breast cancer (for allelic effect: OR = 1.16; 95% CI = 1.01–1.34) and ovarian cancer (for allelic effect: OR = 1.24; 95% CI = 1.00–1.54; for 6A/6A vs. 9A/9A: OR = 2.34; 95% CI = 1.03–5.33). However, no significant associations were found in colorectal cancer, bladder cancer, prostate cancer and lung cancer for all genetic models. In summary, this meta-analysis suggests that the TGFBR1*6A/9A polymorphism is associated with cancer susceptibility, increasing the risk of breast and ovarian cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer remains one of the leading causes of mortality worldwide in the twenty-first century. It is predicted that by 2020, the number of new cases of cancer in the world will increase to more than 15 million, with deaths increasing to 12 million.
Therefore, the effective measures for cancer prevention and management are urgently needed. Recent studies have suggested that improved cancer survival can be achieved by earlier detection, better access to care and improved treatment [1, 2]. Finding new gene markers for screening high-risk populations is an important way to achieve earlier detection of cancer. However, the mechanism of carcinogenesis is still not fully understood. It has been suggested that low-penetrance susceptibility genes combining with environmental factors may be important in the development of cancer [3]. In recent years, several common low-penetrant genes have been identified as potential cancer susceptibility genes. An important one is transforming growth factor beta receptor type I (TGFBR1), which plays an important role in the TGFB singling pathway [4]. A functional single nucleotide polymorphism in exon 1, with a 9A to 6A change, has been proven to decrease TGFB growth inhibitory singling activity and contribute to the development of cancer [5, 6]. A number of studies have reported the role of TGFBR1*6A/9A polymorphism and cancer risk [5–27], but the results are inconclusive, partially because of the possible small effect of the polymorphism on cancer risk and the relatively small sample size in each of published studies. Therefore, we performed a meta-analysis to derive a more precise estimation of this association.
Materials and methods
Publication search
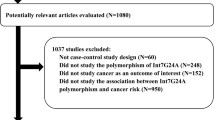
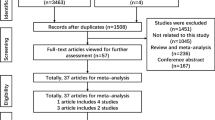
Systematic computerized searches of the PubMed and Medline databases (up to Jan 28, 2009) were performed using the following search terms: “transforming growth factor”, “transforming growth factor receptor”, “Type I TGF-beta receptor”, “TbR-I(6A)”, “TbetaR-I(6A)”, “TGFBR1*6A”, “mutation”, ”susceptibility allele”, “cancer”, and “tumor”. The search was limited to human studies. All eligible studies were retrieved, and their bibliographies were checked for other relevant publications. When the same patient population was used in several publications, only the most recent, largest or complete study was included in this meta-analysis.
Inclusion criteria
The following criteria were used for the study selection: (1) evaluate the association between TGFBR1*6A/9A polymorphism and cancer risk, (2) case–control studies, (3) sufficient data about genotype frequency.
Data extraction
Information was carefully extracted from all eligible publications independently by two of the authors according to the inclusion criteria listed above. Disagreement was resolved by discussion between the two authors. If these two authors could not reach a consensus, another author was consulted to resolve the dispute and a final decision was made by the majority of the votes. The following data were collected form each study: first author’s name, publication date, country, cancer types, total numbers of cases and controls, and numbers of every genotype, respectively. When studies included subjects of more than one cancer types, genotype data were extracted separately according to cancer types for subgroup analyses. To achieve enough statistical power, we only conducted the meta-analysis on cancer types with more than two studies.
Statistical methods
Allele frequencies of each study were determined by the allele-counting method. A chi-square test was used to determine if the distributions of genotypes among controls conformed to Hardy–Weinberg equilibrium (HWE). The strength of the association between TGFBR1*6A/9A polymorphism and cancer risk was measured by odds ratios (ORs) with 95% confidence intervals (CIs). The pooled ORs were estimated for allelic effect (6A vs. 9A), codominant model (6A/6A vs. 9A/9A; 9A/6A vs. 9A/9A), dominant model (6A/6A+9A/6A vs. 9A/9A) and recessive model (6A/6A vs. 9A/6A+9A/9A), respectively. Subgroup analyses were conducted by cancer types. Chi-square-based Q test was used to check heterogeneity among studies [28]. A P < 0.10 indicates a heterogeneity existing among studies, so the random-effects model (the DerSimonian and Laird method) was used [29]. Otherwise, the fixed-effects model (the Mantel–Haenszel method) was used [30]. One-way sensitivity analyses were performed to assess the stability of the results, namely, a single study in the meta-analysis was deleted each time to reflect the influence of the individual data-set to the pooled OR [31]. An estimate of potential publication bias was carried out by the funnel plot, in which the standard error of log (OR) of each study was plotted against its log (OR). An asymmetric plot suggests a possible publication bias. Funnel plot asymmetry was assessed by the method of Egger’s linear regression test, a linear regression approach to measure funnel plot asymmetry on the natural logarithm scale of the OR. The significance of the intercept was determined by the t-test suggested by Egger (P < 0.05 was considered representative of statistically significant publication bias) [32]. All of the statistical tests used in our meta-analysis were performed by STATA version 10.0 (Stata Corporation, College Station, TX).
Results
Studies included in the meta-analysis
Based on our search criteria, a total of 23 publications were identified [5–27]. Among them, one publication [13] included five separate unpublished studies and five publications [5, 6, 10, 14, 26] presented two separate case–control studies, respectively. Each study in one publication was considered separately for pooling analysis. Hence, 23 publications including 32 studies were included in the final meta-analysis. Table 1 lists the main characteristics of these studies. In total, these studies included 13,662 cases and 14,147 controls. Sample sizes ranged from 59 to 2,860. There were 15 studies for breast cancer, 9 for colorectal cancer, 5 for the bladder cancer, 4 for ovarian cancer, and 3 for prostate cancer. All controls in theses studies conformed to HWE.
Table 1 also listed the distribution of genotypes for each study. The frequency of the 9A/9A genotype in the controls ranged from 73 to 90% (median, 83.5%); the frequency of the 9A/6A genotype ranged from 10 to 26% (median, 15.7%); the frequency of the 6A/6A genotype ranged from 0 to 1.6% (median, 0.7%). The frequency of the 9A/9A genotype in the cases ranged from 75 to 92% (median, 82.3%); the frequency of the 9A/6A genotype ranged from 7 to 23% (median, 17.1%); the frequency of the 6A/6A genotype ranged from 0 to 3% (median, 0.9%).
Meta-analysis results
Table 2 lists the main results of this meta-analysis. When all 32 studies were pooled into the meta-analysis, significantly elevated cancer risk was associated with TGFBR1*6A in all genetic models (for allelic effect: OR = 1.11; 95% CI = 1.03–1.21; for 6A/6A vs. 9A/9A: OR = 1.30; 95% CI = 1.01–1.69; for 9A/6A vs. 9A/9A: OR = 1.08; 95% CI = 1.01–1.15; for dominant model: OR = 1.08; 95% CI = 1.02–1.15; for recessive model: OR = 1.29; 95% CI = 1.00–1.68). When subgroup analysis by cancer types, significant association was found in breast cancer (for allelic effect: OR = 1.16; 95% CI = 1.01–1.34) and ovarian cancer (for allelic effect: OR = 1.24; 95% CI = 1.00–1.54; for 6A/6A vs. 9A/9A: OR = 2.34; 95% CI = 1.03–5.33).
Sensitivity analyses
A single study involved in the meta-analysis was deleted each time to reflect the influence of the individual data-set to the pooled ORs, and the corresponding pooled ORs were not materially altered (data not shown).
Publication bias
The shapes of the funnel plots did not reveal any evidence of obvious asymmetry (figures not shown). Also, the results of Egger’s test still did not suggest any evidence of publication bias (P = 0.38 for 6A vs. 9A, P = 0.05 for 6A/6A vs. 9A/9A, P = 0.63 for 9A/6A vs. 9A/9A, P = 0.51 for dominant model and P = 0.06 for recessive model, respectively).
Discussion
The present meta-analysis, including 13,662 cases and 14,147 controls from 32 published studies, explored the association between TGFBR1*6A/9A polymorphism and cancer risk. Our results indicated that the TGFBR1*6A allele is a low-penetrant risk factor for developing cancer in all genetic models. This finding is biologically plausible. TGFBR1*6A is caused by deletion of three GCG triplets coding for alanine within a nine alanine (*9A) repeat sequence of exon 1. It has been proven that TGFBR1*6A is an impaired mediator of TGFB antiproliferative signals compared with intact TGFBR1 [5, 6]. Because of the role that TGFB playing in carcinogenesis and cancer progression [33, 34, 35], the functional polymorphism in TGFBR1 may have an impact on cancer susceptibility attributable to the decreased TGFB growth inhibitory singling activity [35].
In the subgroup analyses by cancer types, significant associations were found in breast cancer (for allelic effect: OR = 1.16; 95% CI = 1.01–1.34) and ovarian cancer (for allelic effect: OR = 1.24; 95% CI = 1.00–1.54; for 6A/6A vs. 9A/9A: OR = 2.34; 95% CI = 1.03–5.33) but not in colorectal cancer, bladder cancer, and prostate cancer. One factor that would contribute to the discrepancy is that TGFBR1 polymorphism might play a different role in different kinds of cancer. It might be an increased risk factor for some kinds of cancer but not for others. In addition, considering the possible small effect size of TGFBR1 polymorphism to cancer and the relatively small sample size in some studies, the discrepancy may due to chance because some of these studies may not have enough power to detect a small but real association or give a fluctuated estimation.
Our studies had several limitations that need to be taken into consideration when interpreting the findings. First, in the subgroup analyses, the number of studies and the number of subjects included in ovarian cancer subgroup or prostate cancer subgroup are relatively small. Second, lacking of the original data limited our further evaluation of potential interactions among gene–gene and gene–environment. Third, our result was based on unadjusted estimates, while a more precise analysis should be conducted if more detailed individual data were available, which would allow for the adjustment by other covariates including age, ethnicity, lifestyle and environmental factors.
Despite its limitations, our meta-analysis also had some advantages. First, it provides pooled data on a substantial number of cases and controls and increased statistical power of the analysis. Second, sensitivity analyses were conducted using the method as previously described [31], all the results were not materially altered and did not draw different conclusions, indicating that our results were robust. Third, Begg’s and Egger’s tests did not detect any publication bias indicating that our results should be unbiased.
In summary, this meta-analysis suggests that the TGFBR1*9A/6A polymorphism is associated with cancer susceptibility, increasing the risk of breast and ovarian cancer. However, TGFBR1*9A/6A polymorphism is not only one of the common variants in TGFB signaling pathway. Other variant such as TGFB1 T29C [36, 37] and Int7G24A [11, 18] were also identified as important cancer risk factors. These variants may have a functional interaction with respect to cancer risk. Therefore, further studies may need to identify patterns of these variants to further increase the predictive value of cancer risk. Moreover, gene–environment interaction should also be considered in the analysis. Such studies taking these factors into account may eventually lead to better, comprehensive understanding of the association between the TGFBR1*9A/6A polymorphism and cancer risk.
References
Soerjomataram I, Louwman MW, Ribot JG, Roukema JA, Coebergh JW (2008) An overview of prognostic factors for long-term survivors of breast cancer. Breast Cancer Res Treat 107:309–330
Karim-Kos HE, De Vries E, Soerjomataram I, Lemmens V, Siesling S, Coebergh JW (2008) Recent trends of cancer in Europe: a combined approach of incidence, survival and mortality for 17 cancer sites since the 1990s. Eur J Cancer 44:1345–1389
Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M (2000) Environmental and heritable factors in the causation of cancer—analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med 343:78–85
Ebner R, Chen RH, Shum L, Lawler S, Zioncheck TF, Lee A (1993) Cloning of a type I TGF-β receptor and its effect on TGF-β binding to the type II receptor. Science 260:1344–1348
Pasche B, Kolachana P, Nafa K, Satagopan J, Chen YG, Lo RS (1999) TbetaR-I (6A) is a candidate tumor susceptibility allele. Cancer Res 59:5678–5682
Chen T, de Vries EG, Hollema H, Yegen HA, Vellucci VF, Strickler HD (1999) Structural alterations of transforming growth factor-beta receptor genes in human cervical carcinoma. Int J Cancer 82:43–51
van Tilborg AA, de Vries A, Zwarthoff EC (2001) The chromosome 9q genes TGFBR1, TSC1, and ZNF189 are rarely mutated in bladder cancer. J Pathol 194:76–80
Stefanovska AM, Efremov GD, Dimovski AJ, Jasar D, Zografski G, Josifovski T (2001) TbetaR-I(6A) polymorphism is not a tumor susceptibility allele in Macedonian colorectal cancer patients. Correspondence re: B. Pasche et al. Type I TbetaR-I (6A) Is a candidate tumor susceptibility allele. Cancer Res., 58:2727–2732, 1998. Cancer Res 61:8351–8352
Samowitz WS, Curtin K, Leppert MF, Slattery ML (2001) Uncommon TGFBRI allele is not associated with increased susceptibility to colon cancer. Genes Chromosom Cancer 32:381–383
Baxter SW, Choong DY, Eccles DM, Campbell IG (2002) Transforming growth factor beta receptor 1 polyalanine polymorphism and exon 5 mutation analysis in breast and ovarian cancer. Cancer Epidemiol Biomarkers Prev 11:211–214
Chen T, Jackson C, Costello B, Singer N, Colligan B, Douglass L (2004) An intronic variant of the TGFBR1 gene is associated with carcinomas of the kidney and bladder. Int J Cancer 112:420–425
Kaklamani V, Baddi L, Rosman D, Liu J, Ellis N, Oddoux C (2004) No major association between TGFBR1*6A and prostate cancer. BMC Genet 5:28
Pasche B, Kaklamani VG, Hou N, Young T, Rademaker A, Peterlongo P (2004) TGFBR1*6A and cancer: a meta-analysis of 12 case–control studies. J Clin Oncol 22:756–758
Jin Q, Hemminki K, Grzybowska E, Klaes R, Söderberg M, Zientek H (2004) Polymorphisms and haplotype structures in genes for transforming growth factor beta1 and its receptors in familial and unselected breast cancers. Int J Cancer 112:94–99
Suarez BK, Pal P, Jin CH, Kaushal R, Sun G, Jin L (2005) TGFBR1*6A is not associated with prostate cancer in men of European ancestry. Prostate Cancer Prostatic Dis 8:50–53
Spillman MA, Schildkraut JM, Halabi S, Moorman P, Calingaert B, Bentley RC (2005) Transforming growth factor beta receptor I polyalanine repeat polymorphism does not increase ovarian cancer risk. Gynecol Oncol 97:543–549
Kaklamani VG, Baddi L, Liu J, Rosman D, Phukan S, Bradley C (2005) Combined genetic assessment of transforming growth factor-beta signaling pathway variants may predict breast cancer risk. Cancer Res 65:3454–3461
Chen T, Jackson CR, Link A, Markey MP, Colligan BM, Douglass LE (2006) Int7G24A variant of transforming growth factor-beta receptor type I is associated with invasive breast cancer. Clin Cancer Res 12:392–397
Feigelson HS, Patel AV, Diver WR, Stevens VL, Thun MJ, Calle EE (2006) Transforming growth factor beta receptor type I and transforming growth factor beta1 polymorphisms are not associated with postmenopausal breast cancer. Cancer Epidemiol Biomarkers Prev 15:1236–1237
You W, Liu Z, Zhao J, Zheng M, Zheng SY, Liu X (2007) No association between TGFBR1*6A and lung cancer. J Thorac Oncol 2:657–659
Cox DG, Penney K, Guo Q, Hankinson SE, Hunter DJ (2007) TGFB1 and TGFBR1 polymorphisms and breast cancer risk in the Nurses’ Health Study. BMC Cancer 7:175
Song B, Margolin S, Skoglund J, Zhou X, Rantala J, Picelli S (2007) TGFBR1*6A and Int7G24A variants of transforming growth factor-beta receptor 1 in Swedish familial and sporadic breast cancer. Br J Cancer 97:1175–1179
Skoglund J, Song B, Dalén J, Dedorson S, Edler D, Hjern F (2007) Lack of an association between the TGFBR1*6A variant and colorectal cancer risk. Clin Cancer Res 13:3748–3752
Skoglund Lundin J, Vandrovcova J, Song B, Zhou X, Zelada-Hedman M, Werelius B (2009) TGFBR1 variants TGFBR1*6A and Int7G24A are not associated with an increased familial colorectal cancer risk. Br J Cancer 100:1674–1679
Castillejo A, Rothman N, Murta-Nascimento C, Malats N, García-Closas M, Gómez-Martínez A (2009) TGFB1 and TGFBR1 polymorphic variants in relationship to bladder cancer risk and prognosis. Int J Cancer 124:608–613
Jakubowska A, Gronwald J, Menkiszak J, Górski B, Huzarski T, Byrski T (2009) BRCA1-associated breast and ovarian cancer risks in Poland: no association with commonly studied polymorphisms. Breast Cancer Res Treat
Colleran G, McInerney N, Rowan A, Barclay E, Jones AM, Curran C (2009) The TGFBR1*6A/9A polymorphism is not associated with differential risk of breast cancer. Breast Cancer Res Treat
Cochran WG (1954) The combination of estimates from different experiments. Biometrics 10:101–129
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719–748
Tobias A (1999) Assessing the influence of a single study in the meta-analysis estimate. Stata Tech Bull 8:15–17
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Siegel PM, Massague J (2003) Cytostatic and apoptotic actions of TGF-beta in homeostasis and cancer. Nat Rev Cancer 3:807–820
Jakowlew SB (2006) Transforming growth factor-b in cancer metastasis. Cancer Metastasis Rev 25:435–457
Bian Y, Kaklamani V, Reich J, Pasche B (2003) TGF-beta signaling alterations in cancer. Cancer Treat Res 115:73–94
Ziv E, Cauley J, Morin PA, Saiz R, Browner WS (2001) Association between the T29-->C polymorphism in the transforming growth factor beta1 gene and breast cancer among elderly white women: the study of osteoporotic fractures. JAMA 285:2859–2863
Marchand LL, Haiman CA, van den Berg D, Wilkens LR, Kolonel LN, Henderson BE (2004) T29C polymorphism in the transforming growth factor h1 gene and postmenopausal breast cancer risk: the Multiethnic Cohort Study. Cancer Epidemiol Biomarkers Prev 13:412–415
Author information
Authors and Affiliations
Corresponding author
Additional information
Ru-Yan Liao, Chen Mao and Li-Xin Qiu contributed equally to this work and should be considered as co-first authors.
Rights and permissions
About this article
Cite this article
Liao, RY., Mao, C., Qiu, LX. et al. TGFBR1*6A/9A polymorphism and cancer risk: a meta-analysis of 13,662 cases and 14,147 controls. Mol Biol Rep 37, 3227–3232 (2010). https://doi.org/10.1007/s11033-009-9906-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-009-9906-7