
Abstract
Social avoidance goals have been linked to negative social outcomes and may contribute to the social impairment experienced by socially anxious individuals. In this study, we examined whether engaging in acts of kindness, a technique designed to increase happiness, decreases social avoidance goals in socially anxious participants and whether social anxiety reduction and hedonic enhancement (i.e., increased positive affect) mediate this effect. Socially anxious undergraduates were randomly assigned to three conditions: performing acts of kindness (AK; N = 38); exposure only (EO; N = 41); and recording life details (LD; N = 36), a neutral control condition. Participants engaged in these activities for 4 weeks. AK resulted in the greatest decrease in social avoidance goals by post-intervention. EO also reduced avoidance goals over time relative to LD. The effect of task condition on avoidance goals over time was fully mediated by social anxiety reduction over time. Neither AK nor EO increased positive affect. Implications for social anxiety treatment are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Social relationships are a source of valuable rewards (e.g., support, intimacy) and notable threats (e.g., rejection, conflict; Gable and Gosnell 2013). Individuals differ in the extent to which they are motivated to approach social rewards and avoid social punishment. This affects the goals that they pursue (Gable 2006). Whereas focusing on approach goals in social situations is generally adaptive, focusing on avoidance goals has been linked to negative social outcomes (e.g., Elliot et al. 2006; Gable 2006). A case in point is provided by individuals with social anxiety. Although strongly motivated to avoid negative social outcomes, socially anxious individuals are more likely to experience them, in part because their self-protective behaviors impair their social interactions (e.g., Alden and Bieling 1998). Reducing avoidance goals may help to correct this paradoxical, self-defeating pattern. A recent study found that engaging in acts of kindness decreased social avoidance goals in socially anxious individuals (Alden and Trew 2013). In this study, we examined whether this effect is robust (i.e., replicable) and, if so, whether social anxiety reduction and hedonic enhancement mediate change in social avoidance goals.
The costs of social avoidance goals
Social goals translate general motivational tendencies (i.e., the desire to approach rewards or avoid threats) into more specific guidelines for behavior in social situations (Elliot et al. 2006; Elliot 2006; Gable 2006). Approach goals focus on attaining positive outcomes such as intimacy and are generally adaptive, predicting more positive relationships with others, more positive and fewer negative social events, decreased loneliness, greater satisfaction with social bonds, positive social attitudes, and better social adjustment (Elliot et al. 2006; Gable 2006; Ryan and Shim 2006). Avoidance goals, on the other hand, focus on avoiding negative outcomes such as rejection and have been linked to more negative and fewer positive social events, higher reactivity to negative events, loneliness, negative social attitudes, relationship insecurity, social worry, decreased relationship satisfaction, anxious solitary behavior, and lower perceived popularity (Elliot et al. 2006; Gable 2006; Ryan and Shim 2006, 2008). Compounding matters, the interpersonal problems associated with pursuing social avoidance goals predict lower satisfaction of approach goals (Holtforth et al. 2006).
Social anxiety has been linked to high avoidance motivation (Levinson et al. 2011; Nikitin and Freund 2010) and self-protective social goals (Alden and Bieling 1998; Meleshko and Alden 1993). It has also been indirectly linked to social avoidance goals through its relationship to low positive affect (Trew and Alden 2012). Further, social anxiety results in significant social impairment. Socially anxious individuals have lower educational and professional achievement (see Fink et al. 2009 for a review), fewer friends (Rodebaugh 2009), less satisfying social interactions (Heerey and Kring 2007), less emotional intimacy in close relationships (Davila and Beck 2002; Sparrevohn and Rapee 2009), and general social disruption (Aderka et al. 2012). Social avoidance goals may contribute to this social impairment by promoting overt and subtle avoidance behaviors (i.e., safety behaviors; Clark and Wells 1995; Rapee and Heimberg 1997), which have been shown to adversely affect social outcomes (e.g., Taylor and Alden 2011). Reducing social avoidance goals may help to reduce this impairment.
Reducing social avoidance goals
One technique that may decrease social avoidance goals involves engaging in acts of kindness. This technique was originally developed as a happiness intervention and has been shown to increase well-being (Buchanan and Bardi 2010; Lyubomirsky et al. 2005). Acts of kindness are acts that benefit others or make others happy, typically at some cost to oneself (Lyubomirsky et al. 2005). The prosocial intent behind acts of kindness makes them distinct from other social encounters. Although people may focus on approaching positive outcomes during other social interactions, acts of kindness focus on promoting positive outcomes for others rather than for oneself. Thus, acts of kindness may help to strengthen social relationships, increase social engagement, and broaden social networks (Kurtz and Lyubomirsky 2008; Otake et al. 2006). In addition, by promoting positive outcomes for others, acts of kindness may increase the likelihood of positive interactions, helping to counter negative social expectations (e.g., of rejection), reduce perceptions of threat, and decrease the perceived need for avoidance.
Consistent with this, in a recent study by Alden and Trew (2013), socially anxious participants who engaged in acts of kindness for 4 weeks showed a greater decrease in social avoidance goals relative to participants in a neutral control condition (i.e., recording daily events). Moreover, this relatively simple manipulation led to a marginally larger decrease in avoidance goals relative to a comparison condition that involved conducting behavioral experiments where participants observed the effects of safety behaviors on their social interactions. This supports the notion that engaging in acts of kindness decreases social avoidance goals. However, the mechanisms driving this effect remain unclear. Although acts of kindness increased positive affect (PA) relative to the other two conditions, change in PA was independent of change in avoidance goals (Alden and Trew 2013).
Decreased state-level social anxiety may help to account for the effectiveness of the kindness intervention. Socially anxious individuals view many social situations as threatening, triggering state-level (i.e., temporary) anxiety (e.g., Clark and Wells 1995). Negative affective states, including anxiety, are thought to promote avoidance goals and behavior (Bjornebekk 2008). Consistent with this, Bjornebekk (2007, as cited by Bjornebekk 2009) found that negative affect was related to the adoption of avoidance goals. If individuals experience less anxiety in social situations, they may perceive less need for avoidance and have fewer avoidance goals. Although research has not examined whether kindness interventions affect social anxiety, acts of kindness may encourage more positive perceptions of the social world (Lyubomirsky and Della Porta 2010) and decrease perceptions of threat as individuals recognize that others are unlikely to respond negatively to kindness. This may reduce anxiety in social situations which, in turn, may reduce social avoidance goals.
Present study
In this study we examined whether social anxiety reduction mediated the effect of acts of kindness on social avoidance goals over time in a socially anxious sample. Given that the acts of kindness intervention was originally developed as a happiness intervention (Lyubomirsky et al. 2005), we also examined PA as a potential mediator, as PA has been linked to fewer social avoidance goals (Trew and Alden 2012) and hedonic enhancement may broaden anxious individuals’ perspectives, allowing them to consider goals other than self-protection (Fredrickson 1998). Although earlier work found that change in PA was independent of change in social avoidance goals (Alden and Trew 2013), it is important to rule out hedonic enhancement as a competing mechanism of change.
In order to evaluate whether the prosocial nature of kindness offers unique advantages over simply increasing the frequency of social contact, we compared acts of kindness to an “exposure only” condition that involved engaging in social interactions that participants would typically avoid. Although exposure may gradually reduce social avoidance goals by countering avoidance tendencies, engaging in unstructured social interactions can be quite threatening for socially anxious individuals. The prosocial nature of kindness may make it easier for anxious individuals to engage in kind acts relative to exposure as they may anticipate more positive reactions from others. This may lead to higher engagement and, consequently, an earlier reduction in social avoidance goals. Consistent with this, Alden and Trew (2013) found that acts of kindness led to improvements in mood after just 1 week, suggesting that engaging in acts of kindness promotes rapid change in relevant outcomes. Demonstrating that acts of kindness lead to a greater (or earlier) reduction in social avoidance goals relative to exposure alone would help to establish the utility and specific benefits of this prosocial intervention. These two active conditions were compared to a neutral control condition (i.e., recording life details).
We hypothesized that engaging in acts of kindness would lead to a greater overall decrease in social avoidance goals at post-intervention relative to both comparison conditions, with differences between acts of kindness and exposure only expected to be particularly apparent in the early stages of the intervention. Some reduction in social avoidance goals over time is also expected to occur in response to exposure only. In addition, we hypothesized that engaging in acts of kindness would decrease state-level social anxiety relative to the control condition. Exposure only was also expected to reduce social anxiety relative to the control condition based on clinical research demonstrating that social exposure decreases social anxiety (Feske and Chambless 1995; Gould et al. 1997). Change in social anxiety over time is expected to mediate any observed changes in social avoidance goals over time. Lastly, we hypothesized that acts of kindness would increase PA relative to both comparison conditions. However, based on Alden and Trew’s (2013) findings, change in PA was not expected to mediate change in avoidance goals.
Methods
Participants
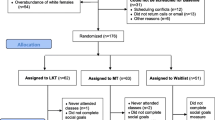
Undergraduates (N = 1662) completed the Social Interaction Anxiety Scale-Straightforward (SIAS-S), a measure of social anxiety, as part of a screening questionnaire. Those scoring 25 or above were invited to participate. In a large archival dataset, this was the lowest SIAS-S score corresponding to the commonly used clinical cut-off of 34 on the full Social Interaction Anxiety Scale (SIAS; Heimberg et al. 1992; Rodebaugh et al. 2006). Of 437 eligible participants, 146 participated (73.97 % female; mean age = 20.47, SD = 3.66; mean years of university completed = 2.11, SD = 1.60). Fifty-five were of European descent, 67 were of Asian descent, and 24 were of “other” descent. All participants had spoken English for at least 10 years.
SIAS scores from the initial intervention session were also examined to confirm that participants were high in social anxiety. This allowed us to use a formal clinical cut-off for the second screening process (a formal cut-off is not available for the SIAS-S; Rodebaugh et al. 2006) and directly compare our sample to Alden and Trew’s (2013) sample. Participants scoring 29 or higher on the SIAS were included in the analyses. This lower cut-off was based on research suggesting that the standard cut-off may be overly conservative in analogue samples (Rodebaugh et al. 2006). This second screening process resulted in the exclusion of 23 participants. One additional participant was excluded due to low task compliance.
Measures
Social Interaction Anxiety Scale (Mattick and Clarke 1998)
The SIAS includes 20 items assessing cognitive (e.g., “I worry about expressing myself in case I appear awkward”), affective (e.g., “I am nervous mixing with people I don’t know well”), and behavioral (e.g., “I have difficulty making eye-contact with others”) aspects of social interaction anxiety using a five-point scale (0 = not at all characteristic or true of me, 4 = extremely characteristic or true of me). It has high internal consistency, test–retest reliability, and convergent and discriminant validity as a measure of social anxiety (Mattick and Clarke 1998). The SIAS-S (Rodebaugh et al. 2007) is an adaptation of the SIAS that excludes the reverse scored items based on research suggesting that the 17 straightforwardly worded items are more valid indicators of social interaction anxiety (Rodebaugh et al. 2007). The SIAS-S has comparable psychometric properties and convergent validity to the SIAS (Rodebaugh et al. 2007). Cronbach’s alphas for the SIAS-S in this study ranged from .80 to .94. Cronbach’s alpha for the SIAS (used for screening purposes after the initial intervention session) was .89.
Social Goals Questionnaire (SGQ; Meleshko and Alden 1993)
The SGQ includes five items assessing social approach goals (e.g., “Get to know the person I was talking to”) and five assessing social avoidance goals (e.g., “Not appear foolish”). The SGQ was selected over an idiographic measure (i.e., having participants nominate their own social goals) to ensure that all participants responded to the same goals on each occasion, providing a consistent metric for the analyses. Participants were asked to “please rate the extent to which you had the following goals when interacting with other people in the last month” using a seven-point scale (1 = Not at all, 7 = Very much). The SGQ has acceptable reliability, with higher internal consistency in the avoidance subscale (Alden and Trew 2013). Cronbach’s alphas in this study ranged from .66 to .71 for approach and from .69 to .84 for avoidance at pre- and post-intervention.Footnote 1
Daily Social Anxiety (DSA; Kashdan and Steger 2006)
The DSA includes seven items assessing state-level social anxiety experienced during the past few days (e.g., “I worried about what other people thought of me”, “I felt uncomfortable and embarrassed when I was the center of attention”). In contrast to the SIAS-S which measures dispositional (i.e., longstanding) social anxiety, the DSA assesses the level of social anxiety recently experienced by participants. Responses are made using a five-point scale (1 = Very slightly/not at all, 5 = Extremely). The DSA was selected as the primary measure of social anxiety as state-level social anxiety is more likely to demonstrate change over a short-term intervention than dispositional social anxiety.Footnote 2 The DSA has high reliability and convergent validity (Kashdan and Steger 2006). Cronbach’s alphas in this study ranged from .84 to .91 at pre- and post-intervention.
International Positive and Negative Affect Schedule-Short Form (I-PANAS-SF; Thompson 2007)
The I-PANAS-SF includes 10 items from the Positive and Negative Affect Schedule (PANAS; Watson et al. 1988), a widely used measure of affect. Five items assess activated forms of PA (e.g., alert, determined) and five assess activated forms of negative affect (NA; e.g., nervous, ashamed) using a five-point scale (1 = Never, 5 = Always). The I-PANAS-SF was designed to comprehensively reflect the content of the PANAS and has adequate internal consistency, temporal stability, and convergent validity (Thompson 2007). Cronbach’s alphas in this study ranged from .75 to .81 for PA and from .78 to .80 for NA at pre- and post-intervention.
Online forms
Online forms were developed to assess compliance, social goals (via the SGQ), social anxiety (via the DSA), and affect (via the I-PANAS-SF) over the course of the study. Participants were emailed links to these forms twice weekly throughout the 4-week intervention beginning 3 days after the initial intervention session. Participants indicated whether they completed their assigned activity over the past few days, on which days, and whether they completed three repetitions each day. Participants completed the SGQ, DSA, and I-PANAS-SF with the time frame modified to assess goals, social anxiety, and affect over “the past few days.” Task instructions and items were otherwise identical to the SGQ, DSA, and I-PANAS-SF described above. Cronbach’s alphas ranged from .53 to .82 for SGQ-approach, .74–.87 for SGQ-avoidance, .89–.92 for DSA, .72–.85 for PA, and .77–.81 for NA. Although SGQ-approach had somewhat low internal consistency in the online forms, it is important to note that only two Cronbach’s alphas fell below .70 (i.e., .53 at time one and .63 at time two), the mean value was above .70 (M = .72, SD = .09), and, importantly, SGQ-approach is not a primary outcome or mediator variable. All time points were included in the analyses. As the correlations between the two online forms administered each week were consistently high for all measures, responses to each week’s forms were averaged prior to conducting the analyses to maximize reliability and minimize missing data.Footnote 3 When participants were missing data on one of the two forms, their responses to the other form were used in place of the averaged value.
Procedure
The institution’s Research Ethics Board approved this study. Participants were recruited from undergraduate psychology classes. Recruitment materials did not allude to any potential treatment benefits. Following informed consent, all participants completed the SIAS-S as part of a larger online questionnaire in exchange for partial course credit (see Fig. 1 for procedural timeline). Eligible participants were invited to attend the initial intervention session. During this session, participants completed all study measures (i.e., the pre-intervention measures) and were randomly assigned to one of three task conditions. Instructions included a plausible rationale explaining how each activity may be helpful in the treatment of anxiety. Task instructions were scripted and audio recorded to monitor experimenter adherence to the protocol. Participants received a booklet including task instructions, examples of activities they could complete/record, and worksheets for recording their participation (i.e., the activities they completed/recorded). They were emailed links to the online forms twice weekly and were contacted by telephone 2 weeks after the initial intervention session to ensure that they were able to complete their assigned task and understood the instructions. Participants returned to the laboratory after 4 weeks to complete a second questionnaire battery (i.e., the post-intervention measures), receiving partial course credit and entry into a prize draw in exchange for their participation. Five female experimenters tested an approximately equal number of participants in each condition.

Procedural timeline
Task conditions
Acts of kindness (AK)
In the AK condition, the nature of kind acts was explained and participants (N = 38) were informed that acts of kindness may reduce anxiety by affecting mood and social interactions. Acts of kindness were defined as acts that benefit others or make others happy, typically at some cost to oneself (Lyubomirsky et al. 2005). Based on findings by Lyubomirsky et al. (2005), participants were asked to engage in 3 acts of kindness a day on 2 days each week over 4 weeks. Examples of acts of kindness completed by the participants include doing a roommate’s dishes, mowing a neighbour’s lawn, and donating to a charity.
Exposure only (EO)
As noted above, the EO condition was included to control for a potential increase in social contact as a result of the AK intervention. Participants in this condition (N = 41) were given a brief description of exposure (i.e., going into social situations that they would usually avoid and staying until their anxiety decreases) and how it can be useful in countering avoidance and reducing anxiety. They were then asked to identify relevant social interactions, rank these interactions from easiest to most difficult, and engage in 3 interactions a day on 2 days each week over 4 weeks. This frequency was matched to that of the AK intervention. Participants were encouraged to start with easier interactions, gradually moving up to more difficult ones. They were also introduced to a deep breathing technique that they could use prior to entering social situations. This technique was included to control for the fact that participants in the AK condition have an additional task to complete during social encounters (i.e., the kind act) which may reduce their anxiety (e.g., Johnstone and Page 2004). Adding deep breathing to exposure makes this a particularly strong comparison condition as deep (i.e., slowed) breathing has been shown to decrease anxiety in its own right (e.g., Eisen et al. 1990). Examples of exposure exercises completed by the participants included asking a stranger for the time, talking with a neighbor, and asking someone to lunch.
Life details (LD)
LD is an affectively neutral control condition used by several research groups (e.g., Bhullar et al. 2011). Participants (N = 36) were informed that anxious individuals often have difficulty paying attention to events that occur throughout the day and that recording daily events may counteract this, increasing their level of awareness. They were then asked to record at least 3 events that occurred each day on 2 days each week over 4 weeks, with this frequency matched to that of the AK condition. Examples of life details recorded by participants included attending class, cooking, and shopping.
Results
Participant characteristics
The participants who attended the initial intervention session did not differ on the SIAS-S (M = 35.40, SD = 8.08) from those who were eligible but did not participate (M = 35.79, SD = 8.08), t(435) = −0.48, p = .63, d = 0.05. The mean SIAS in the final sample (N = 115, M = 43.39, SD = 9.39) exceeded the standard clinical cut-off of 34 and was significantly higher than the pre-screening mean reported by Alden and Trew (2013), M = 39.65, SD = 8.29, t(262) = 3.44, p < .001, d = 0.42. The task conditions did not significantly differ in gender distribution, χ 2(2, n = 115) = 2.28, p = .32, cultural background, χ 2 (4, n = 115) = 2.83, p = .59, age, F(2, 111) = 0.57, p = .57, or years of university completed, F(2, 111) = 1.42, p = .25, in the final sample.
Missing data
Several participants were missing responses to one or more items from a given scale. When <20 % of a participant’s responses were absent for a specific scale, missing items were replaced using individual mean substitution. This leads to accurate results in most missing data scenarios when the proportion of missing data is small (Hawthorne and Elliott 2005; Shrive et al. 2006). If more than 20 % of the responses for a given scale were absent, the scale score was treated as missing for that participant. Missing scale scores were not imputed. On average, participants received 0.71 imputed values across all measures (SD = 1.15). The rate of imputation did not differ across conditions, χ 2(10, N = 115) = 8.49, p = .58, w = 0.27.
After item-level imputation, the rate of missing data was very low at pre- and post-intervention, with one participant (0.87 %) missing pre-intervention SGQ-approach. All other pre- and post-intervention data was available. Although the rate of missing data was higher for the individual online forms (5.22–35.65 %), this rate did not differ across conditions at any time point, χ 2(2, N = 115) = 0.02–4.76, p = .09–.99, w = 0.01–0.20, and was considerably lower after computing the weekly average scores (0.87–15.65 %). In total, 4.73 % of the data was missing across the full dataset. The ns for each measure at each time point, by condition, are included in Tables 1 and 2.
Protocol adherence
Audio recordings were available for 101 initial intervention sessions. The remainder were unavailable due to technical difficulties. Research assistants transcribed these recordings. A review of these transcripts by the first author revealed no incidents where information specific to one condition was presented to participants in another condition. The first author identified key points (i.e., important concepts and information) in each script and determined adherence by coding whether each point had been accurately conveyed, assigning a score of 1 when points were fully conveyed, 0.5 when part of a point was missing or altered, and 0 when a point was missing or had been substantially altered. Protocol adherence (as a percentage) was high, M = 98.53 %, SD = 3.10, and did not differ across groups, F(2, 98) = 0.37, p = .69, Cohen’s f = 0.09.
Participant compliance
Seven participants did not complete the study (two AK, four EO, one LD).Footnote 4 These participants did not differ from study completers on pre-screening SIAS-S or any initial session variable (all ps > .05) with the exception of the DSA, t(10.83) = 4.04, p = .002, d = 0.76 (equal variances not assumed, Levene’s test: F(1, 120) = 4.67, p = .03). Completers were higher in pre-intervention DSA (M = 15.47, SD = 5.64) relative to non-completers (M = 11.29, SD = 2.36). The rate of non-completion did not differ across groups, χ2(2, N = 7) = 2.00, p = .37, w = 0.53.
Task compliance was examined using participants’ written records and online forms. The written records served as the primary source of compliance data as they could be used to determine the exact number of times a participant completed the activity. Written records were available for 104 participants (34 AK, 35 EO, 35 LD). The rate of non-return did not differ across groups, χ 2(2, N = 11) = 3.45, p = .18, w = 0.56. Task compliance was calculated as a percentage. Online forms were used to determine task compliance for the 11 remaining participants by calculating the percentage of days that they reported completing the activity, multiplying number of days reported on a form by 0.5 when they indicated partial compliance and coding missing online forms as non-compliance. Average self-reported compliance was 94.55 % (SD = 13.01). There were no group differences in task compliance (AK: M = 95.56 %, SD = 11.44; EO: M = 91.77 %, SD = 16.63; LD: M = 96.64 %, SD = 9.06), F (2, 112) = 1.53, p = .22, Cohen’s f = 0.17. As Levene’s test indicated heterogeneity of variance, F(2, 112) = 5.72, p = .004, this analysis was repeated using Alexander and Govern’s (1994) approach, confirming the absence of group differences, χ 2(2) = 2.55, p = .28. As noted above, one participant was excluded due to low task compliance (i.e., <50 %). All others were included to more closely approximate real-world compliance, providing a more conservative test of the effects of interest.
Manipulation check
To determine whether participants engaged in their assigned tasks, responses to the written record sheets were coded by the first author and two research assistants who were blind to task condition and the study hypotheses for whether they reflected acts of kindness and/or social activities (i.e., two separate ratings). As above, acts of kindness were defined as acts that benefit others or make others happy, typically at some cost to oneself. Social activities were defined as acts that involve interacting with others or engaging in shared activities where social interaction is likely (e.g., going to a movie). Coders received written instructions, examples, and 1 h of training that involved coding 5 % of the available data. The order of participants’ responses was randomized across all participants prior to coding. Fleiss’ Kappas of .89 and .81 were obtained for the kindness and social interaction ratings, respectively.
Group differences were found on the kindness ratings, χ 2(2, n = 2690) = 1916.64, p < .001, with a higher proportion of kind acts in AK (M = .93, SD = 0.06) relative to EO (M = .07, SD = 0.16), χ 2(1, n = 1629) = 1218.52, p < .001, and LD (M = .07, SD = 0.05), χ 2(1, n = 1893) = 1404.13, p < .001, which did not differ, χ 2(1, n = 1858) = 0.01, p = .91. Group differences were also found on the social activity ratings, χ 2(2, n = 2693) = 838.95, p < .001, with more social activities in EO (M = .96, SD = 0.07) relative to AK (M = .77, SD = 0.12), χ 2(1, n = 837) = 108.47, p < .001, and LD (M = .33, SD = 0.13), χ 2(1, n = 1856) = 714.77, p < .001. AK also had a higher proportion of social activities relative to LD, χ 2(1, n = 1898) = 359.41, p < .001.Footnote 5 This supports the notion that participants engaged in their assigned tasks.
Analytic overview
To determine whether change in DSA and PA mediate the effect of task condition on SGQ-avoidance, we first examined whether there were group differences in these variables at post-intervention. Significant group differences would establish an effect of task condition on the mediator (i.e., the a paths in traditional mediation) and outcome (i.e., the c path) variables. If task condition does not affect the mediator(s), mediation cannot occur.
We also examined group differences in these variables over time using latent growth models. Mediation was directly examined using a parallel process growth curve strategy, described in greater detail below. This approach allowed us to directly examine whether task condition affects change in the mediator(s), whether change in the mediator(s) predicts change in SGQ-avoidance, and the significance of the indirect effects.
Examining group differences at post-intervention
Analyses of Covariance (ANCOVAs) were used to investigate whether the three task conditions differentially affected the outcome (i.e., SGQ-avoidance) and mediator (i.e., DSA, PA) variables at post-intervention. Significant effects would provide support for additional mediation analyses. Each ANCOVA included the relevant pre-intervention measure as a covariate to control for group differences at pre-intervention and provide more precise estimates of the intervention effects (West et al. 2004). Post-intervention values served as dependent variables. As there were only three groups, significant omnibus effects were followed up with pairwise comparisons using Fisher’s Least Significant Difference (additional alpha correction is not required, see Seaman et al. 1991).
No univariate outliers (i.e., values ≥three SD from the mean) were identified, there were no notable departures from normality, and examination of the bivariate scatterplots between the measures supported linear relationships between the variables. There were no significant group differences on any of the pre-intervention variables (all ps > .05). Levene’s test supported homogeneity of variance for all variables (all ps ≥ .08). Means and standard deviations for the pre- and post-intervention measures, by group, appear in Table 1 along with post-intervention means and standard deviations adjusted for the relevant pre-intervention values from the ANCOVAs. Pearson correlations between all study variables at all time points appear in Table 2.
Significant group differences were observed for SGQ-avoidance, F(2, 111) = 3.44, p = .04, Cohen’s f = 0.25. As predicted, the AK group endorsed significantly fewer avoidance goals at post-intervention than both the EO, t(111) = −2.29, p = .02, d = 0.52, and LD groups, t(111) = −2.27, p = .03, d = 0.53, which did not differ, t(111) = −0.03, p = .97, d = 0.01. Group differences were also observed for the DSA, F(2, 111) = 4.20, p = .02, Cohen’s f = 0.28. The AK, t(111) = −2.17, p = .03, d = 0.50, and EO groups, t(111) = −2.77, p = .01, d = 0.63, scored lower at post-intervention than the LD group, but did not differ from one another, t(111) = 0.57, p = .57, d = 0.13. There were no group differences in PA at post-intervention, F(2, 111) = 0.44, p = .64, Cohen’s f = 0.09, suggesting that change in PA cannot mediate change in SGQ-avoidance.Footnote 6 , Footnote 7
Mediation
Potential mediation was evaluated using a parallel process latent growth curve strategy (Cheong et al. 2003). By combining latent variable and growth curve modeling with random effects, this approach allowed us to directly explore whether task condition affected change in the mediators (i.e., DSA and PA) over time and whether change in the mediators, in turn, predicted change in the outcome (i.e., SGQ-avoidance). This is accomplished by adding structural pathways linking task condition and the random effects (i.e., slopes) from latent growth models for the mediator and outcome variables (Muthén and Curran 1997).
This approach was implemented in several steps. First, separate latent growth models were estimated for each variable to examine patterns of change over time and whether the growth trajectories (i.e., intercepts and slopes) of the outcome (SGQ-avoidance) and mediator (DSA, PA) variables differed by task condition. Task condition was dummy-coded, grand mean centered, and included as a time-invariant predictor. It was recoded to provide all pairwise comparisons. This allowed the latent growth models to fully reproduce the ANCOVA findings while providing additional information about the nature of the observed changes over time. Each model included time-specific residuals and correlated random growth factors (i.e., an intercept, centered at week one, and a linear slope). The relevant pre-intervention measure, grand-mean centered, was included as a time-invariant covariate of the random growth factors. Consequently, the dependent variable becomes a residualized gain score, the intercept reflects initial gains between pre-intervention and week one, and the slope indicates whether these gains are maintained over time (West et al. 2004).
All models were evaluated using EQS 6.1 (Bentler 2004). Full information maximum likelihood estimation was used to account for missing data. The model Chi-squared value, Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA) were considered in evaluating model fit. Non-significant Chi-squared values, CFI values >.95, and RMSEA values <.06 support good model fit (Hu and Bentler 1999). RMSEA values are reported with 90 % confidence intervals.
After estimating the univariate latent growth models, bivariate parallel process latent growth curve models were estimated for the mediator(s) demonstrating significant group differences in change over time to examine potential mediation. Pre-intervention values of the mediator and outcome were allowed to covary, as were the dummy codes for task condition. Significant structural paths linking task condition to the slope of the mediator (the a paths) and the slope of the mediator to the slope of the outcome (the b path) support mediation. Lastly, the cross-products of the a and b paths were calculated and evaluated using bootstrapped percentile confidence intervals to assess the significance of the indirect effects (Biesanz et al. 2010). Significant indirect effects have confidence intervals that do not include zero.
Univariate latent growth models
There were no notable departures from normality for SGQ-avoidance, DSA, or PA from the online forms at any time point. One univariate outlier was detected for PA in the eighth online form. As omitting this observation did not affect the pattern of results, this participant was retained. The covariance matrices for the SGQ-avoidance and PA analyses were invariant across gender, Box’s M = 25.16, F(15, 7710.37) = 1.53, p = .09 and Box’s M = 26.19, F(15, 7710.37) = 1.60, p = .07, respectively. Although gender affected the covariance matrix for the DSA analysis, Box’s M = 27.98, F(15, 7752.08) = 1.70, p = .04, constraining all means and loadings in the DSA model to be equal for men and women did not reduce model fit, χ 2 difference (11) = 6.84, p = .81, suggesting that gender did not affect the findings of interest. Means and standard deviations for SGQ-avoidance, DSA, and PA, by group, are presented in Table 3. Unstandardized coefficients, standard errors, and t tests for the fixed effects from the univariate latent growth models appear in Table 4, along with the relevant fit indices.
As multivariate kurtosis was within acceptable limits (Mardia’s coefficient = −0.68), standard maximum likelihood estimation was used to calculate test statistics and standard errors in the SGQ-avoidance analysis. The linear growth model for SGQ-avoidance provided a good fit to the data, χ 2(13) = 14.68, p = .33, CFI = 1.00, RMSEA = .03 (.00, .10). The results of this analysis provide additional insight into the ANCOVA findings. The significant paths linking task condition to the intercept term indicated that AK and LD showed lower SGQ-avoidance by week one relative to EO, with SGQ-avoidance staying relatively constant in the EO group. The paths linking task condition to the slope (i.e., the c paths in the mediation model; see Table 4) indicated that both AK and EO showed a greater reduction in SGQ-avoidance over time relative to LD. AK and EO did not differ in their rate of change in SGQ-avoidance over time.
Multivariate kurtosis was also within acceptable limits in the DSA analysis (Mardia’s coefficient = 1.85). The linear growth model for DSA provided a good fit to the data, χ 2(13) = 8.85, p = .78, CFI = 1.00, RMSEA = .00 (.00, .06). The paths linking task condition to the intercept indicated that task condition did not affect the initial response to the intervention. The paths linking task condition to the slope indicated that AK and EO showed a greater decrease in social anxiety over time relative to LD, but did not differ from one another.
Lastly, multivariate kurtosis was acceptable in the PA analysis (Mardia’s coefficient = −0.98). The linear growth model for PA did not provide an adequate fit to the data, χ 2(13) = 41.03, p < .001, CFI = .91, RMSEA = .14 (.09, .19). Examination of the means suggested that the data did not follow a strictly linear trend, as PA decreased over the first 3 weeks and increased during the last week of the intervention in two groups. Freely estimating the final slope loading improved model fit, χ 2 difference (1) = 20.67, p = .000005. The revised model provided an adequate fit to the data, χ 2(12) = 20.36, p = .06, CFI = .98, RMSEA = .08 (.00, .13). Consistent with the ANCOVA findings, the groups did not differ in initial response or rate of change in PA over time, confirming that change in PA cannot mediate the effect of task condition on SGQ-avoidance.
Parallel process growth curve analysis
Given that task condition predicted change in SGQ-avoidance and DSA over time but did not predict change in PA, we examined whether change in DSA alone mediated the effect of task condition on SGQ-avoidance. The covariance matrix used for this analysis was invariant across gender, Box’s M = 75.05, F(55, 6476.70) = 1.13, p = .24. As multivariate kurtosis was high (Mardia’s coefficient = 3.85), Yuan and Bentler’s (2000) robust methodology was used to calculate test statistics and standard errors. The model evaluated in this analysis, including standardized loadings, is presented in Fig. 2.Footnote 8 Consistent with the univariate model for DSA, AK and EO showed a greater decrease in DSA over time relative to LD but did not differ from one another (i.e., the a paths). Change in DSA over time significantly predicted change in SGQ-avoidance over time (i.e., the b path).

Full parallel process latent growth curve model used to test mediation with standardized loadings. Note Condition is represented by two correlated dummy codes, recoded to provide all pairwise comparisons. Mediation paths are in bold. Significance is not indicated for the factor loadings for weeks 1–4 as these values are fixed in the unstandardized model. *p < .05
The 95 % bootstrapped percentile confidence intervals for the unstandardized a × b paths indicated that the indirect effects were significant for the paths comparing AK and LD, a × b = −0.71 (−1.37, −0.08), and EO and LD, a × b = −0.69 (−1.35, −0.02), but not for the path comparing EO and AK, a × b = −0.21 (−0.56, 0.61). This supports an indirect effect of task condition on change in SGQ-avoidance through change in DSA. After accounting for this effect, the effects of AK and EO on the slope of SGQ-avoidance, relative to LD (i.e., the c′ paths), became non-significant (see Fig. 2), supporting full mediation.
Discussion
Engaging in acts of kindness led to a greater overall reduction in social avoidance goals in these socially anxious participants relative to both comparison conditions, a finding that is consistent with previous research (Alden and Trew 2013). This effect appears to be attributable to a faster initial decrease in social avoidance goals in the acts of kindness group relative to exposure only. Both the acts of kindness and exposure only groups showed a greater reduction in social avoidance goals over time relative to the neutral control condition. This effect was fully mediated by a corresponding decrease in state-level social anxiety in these groups. Acts of kindness and exposure alone did not increase PA relative to the control condition, ruling out hedonic enhancement as a competing mechanism of change in social avoidance goals. These findings support the value of acts of kindness as an avoidance reduction strategy that decreases social avoidance goals by reducing state-level social anxiety and that does so faster than exposure alone.
The benefits of kindness
The faster initial decrease in social avoidance goals in the acts of kindness group suggests that the prosocial nature of acts of kindness may be particularly beneficial during the early stages of the intervention. Consistent with current theoretical accounts of kindness (Lyubomirsky and Della Porta 2010), acts of kindness may help to counter negative social expectations by promoting more positive perceptions (and expectations) of the social environment. This is likely to occur early in the intervention as participants anticipate positive reactions from others in response to their kindness, decreasing the perceived need to avoid negative social outcomes. As suggested above, positive social expectations may also make it easier to implement the intervention relative to social exposure, potentially enhancing participant engagement and leading to more rapid change in social avoidance goals.
In contrast, participants in the exposure only condition may have had more negative social expectations (e.g., anticipating rejection or criticism) as there is no guarantee that a particular social encounter will go smoothly. This may be particularly true during the early stages of the intervention when participants have had little opportunity to disconfirm their social fears. Later on, successful social encounters may help to modify these negative expectations, leading to a reduction in social avoidance goals over time. However, this reduction was not sufficient to “catch up” with acts of kindness by the end of the 4 week intervention. By facilitating an earlier reduction in social avoidance goals, the acts of kindness intervention may promote more positive social outcomes early on relative to exposure alone, giving this prosocial intervention an advantage over simply increasing the frequency of social contact.
Potential mechanisms of change
As predicted, both acts of kindness and exposure alone led to a significant decrease in state-level social anxiety by the end of the 4-week intervention relative to the neutral control condition. This is consistent with the argument that acts of kindness alter negative perceptions of others (Lyubomirsky and Dickerhoof 2010) which would be expected to reduce associated distress. This is also consistent with clinical research indicating that social exposure decreases social anxiety (Feske and Chambless 1995; Gould et al. 1997). This is the first study to demonstrate that engaging in acts of kindness reduces social anxiety. The fact that acts of kindness and exposure only decreased social anxiety to a similar extent is noteworthy given that social exposure is commonly included in cognitive behavioral therapy protocols for social anxiety (e.g., Feske and Chambless 1995) and the exposure condition used here included deep breathing which has also been shown to decrease anxiety (Eisen et al. 1990). As expected, decreases in state-level social anxiety over time fully mediated the reduction in social avoidance goals over time associated with acts of kindness and exposure only. This is consistent with previous findings suggesting that negative emotional states promote the adoption of avoidance goals (Bjornebekk 2007, as cited by Bjornebekk 2009) and suggests that anxiety reduction is an important mechanism of change in acts of kindness and social exposure.
Counter to expectations, acts of kindness did not significantly increase PA. The pattern of means suggests that power limitations did not affect our ability to detect PA enhancement in this study. If anything, PA appeared to decline slightly in the two active conditions. This is inconsistent with previous findings linking acts of kindness to improvements in PA (Alden and Trew 2013) and well-being (Buchanan and Bardi 2010; Lyubomirsky et al. 2005). However, it is important to note that acts of kindness do not uniformly increase PA. Although studies demonstrating an effect of kindness on PA generally report medium effect sizes, Sin and Lyubomirsky’s (2009) meta-analysis of positive psychology interventions identified two unpublished studies finding that acts of kindness had a negligible effect on well-being. It is also important to acknowledge that kindness may not uniformly lead to positive social interactions, potentially limiting hedonic benefits. In addition, several studies have suggested that acts of kindness may be detrimental in certain interpersonal contexts, particularly if they are not responsive to recipients’ needs, if they occur in the context of serious relationship difficulties (see McNulty and Fincham 2012 for a review), or if individuals focus exclusively on others’ needs, leading to self-neglect (i.e., unmitigated communion; Helgeson and Palladino 2012).
Given that task condition did not affect PA, increased PA cannot account for the effect of the acts of kindness and exposure only interventions on social avoidance goals. This is consistent with previous findings suggesting that change in PA is independent of change in social avoidance goals (Alden and Trew 2013) and effectively rules out hedonic enhancement as a competing mechanism of change. Ultimately, it appears that hedonic enhancement is not required for a reduction in social avoidance goals to occur.
Implications
The significantly larger overall reduction and faster initial decrease in avoidance goals in the acts of kindness condition relative to exposure alone suggests that engaging in acts of kindness is not reducible to an increase in the frequency of social contact, particularly during the early stages of the intervention. These findings suggest that engaging in acts of kindness may be beneficial for socially anxious individuals, reducing their state-level social anxiety and, in turn, their social avoidance goals. Over time, decreased state-level social anxiety associated with acts of kindness (and the more positive social outcomes associated with a reduction in social avoidance goals) may translate into more enduring changes in dispositional social anxiety. Exposure alone also appears to be beneficial, but may take longer to produce a noticeable decrease in social avoidance goals. Reducing social avoidance goals may improve the quality of social encounters and reduce the social difficulties experienced by socially anxious individuals, ultimately decreasing their overall level of social impairment.
Caveats and future directions
Notable strengths of this study include the use of random assignment, stringent participant selection to identify participants high in social anxiety, and the examination of multiple potential mediators to help clarify mechanisms of change in social avoidance goals. In addition, established multi-item measures were used to assess social goals, state-level social anxiety, and state affect, helping to clarify patterns of change in these variables over time. The acts of kindness intervention was compared to exposure only, helping to establish the specific benefits of kindness relative to simply increasing the frequency of social contact. Lastly, mediation was examined using modern and appropriate statistical techniques.
This study also has several limitations. First, the low response rate during participant recruitment suggests the potential for bias in our sample, although it is important to note that the recruitment materials did not allude to potential treatment benefits and the participants did not differ in their level of social anxiety from those who were eligible but did not participate. In addition, we did not examine the perceived credibility of the interventions or the time required to complete each task, factors that may have affected our findings. Further, this study relied exclusively on self-report measures. It would be beneficial to examine whether social goals affect observable behavior, physiological outcomes, and affective responses during social interactions. Future research should also examine whether these findings can be replicated in other social contexts (e.g., public speaking). In addition, perceptions of threat were not assessed in this study. Given the arguments presented above suggesting that acts of kindness may reduce social anxiety and avoidance goals by decreasing perceptions of threat, this may be an important mechanism of change to examine in future studies. Future research may also wish to examine whether a similar pattern of findings can be obtained when participants’ idiographic (i.e., self-nominated) social goals are examined.
From a statistical standpoint, the social goals measure had somewhat low internal consistency, particularly in the online forms. This may have affected our ability to detect change in social goals. It would be advantageous to replicate these findings using a different measure of social goals and a larger participant sample. Lastly, we used a parallel process growth curve model to evaluate mediation. This model assesses change in the mediator and outcome variables concurrently. As a result, we cannot draw causal conclusions from the mediation analyses. Although this approach has been used in other studies and is appropriate given the relatively short time frame of this study, assessing change in the mediator and outcome variables sequentially would establish temporal precedence and provide support for causal relationships between the variables (Selig and Preacher 2009).
Conclusions
In conclusion, engaging in acts of kindness is an effective way to reduce state-level social anxiety and, in turn, decrease social avoidance goals. This suggests that the acts of kindness intervention may be helpful for socially anxious individuals, providing unique benefits relative to exposure alone by promoting a more rapid initial reduction in social avoidance goals. This study represents a novel step in identifying interventions that change social avoidance goals and understanding the mechanisms that drive these changes. By using a range of interventions to alleviate distress, reduce social avoidance goals, and improve social outcomes, it may be possible to help socially anxious individuals overcome social avoidance and lead more satisfying and engaging lives.
Notes
Although Alden and Trew (2013) found that acts of kindness did not affect social approach goals or negative affect and no significant effects were anticipated, these variables were assessed by the SGQ and the I-PANAS-SF and were examined to confirm a lack of group differences. These results are briefly described in a footnote below.
Consistent with this, an ANCOVA revealed no significant group differences in the SIAS-S at post-intervention, controlling for pre-intervention SIAS-S, F(2, 111) = 2.45, p = .09, Cohen’s f = 0.21.
Correlations between the two online forms administered each week ranged from .60 to .89 across the full set of measures (M = .72, SD = 0.09).
The pattern of results was identical when these participants were included in the analyses (i.e., carrying their initial session scores over to the return session for the ANCOVAs). One participant was excluded from the latent trajectory and mediation analyses as they had completed no online forms.
There were no significant gender differences in kindness ratings in the AK, χ 2(1, n = 832) = 0.13, p = .71, or LD groups, χ 2(1, n = 1061) = 0.21, p = .64. Men (M = .13, SD = 0.28) reported more kind acts relative to women (M = .04, SD = 0.05) in the EO group, χ 2(1, n = 797) = 24.57, p < .001. There were also no significant gender differences in social activity ratings in the AK group, χ 2(1, n = 837) = 2.60, p = .11. Women reported a higher proportion of social activities in the EO (M = .97, SD = 0.05), χ 2(1, n = 795) = 15.95, p < .001, and LD (M = .35, SD = 0.13), χ 2(1, n = 1061) = 5.72, p = .02, groups relative to men (M = .92, SD = 0.10 and M = .28, SD = 0.33, respectively).
Consistent with Alden and Trew (2013), no significant group differences were observed in the ANCOVAs for SGQ-approach or NA. Similarly no group differences were observed on initial response or rate of change over time in SGQ-approach or NA in the latent trajectory analyses. Full results available upon request.
When gender was added to each model, gender did not affect SGQ-avoidance, F(1, 108) = 1.62, p = .21, DSA, F(1, 108) = 1.02, p = .32, or PA, F(1, 108) = 0.06, p = .81, nor did it interact with task condition in the models for SGQ-avoidance, F(2, 108) = 1.00, p = .37, DSA, F(2, 108) = 0.30, p = .74, or PA, F(2, 108) = 1.28, p = .28.
Residual correlations were added between the error terms for DSA and SGQ-avoidance at week 2 and at week 3 to improve model fit. These correlations likely reflect shared method variance and are not included in Fig. 2.
References
Aderka, I. M., Hofmann, S. G., Nickerson, A., Hermesh, H., Gilboa-Schechtman, E., & Marom, S. (2012). Functional impairment in social anxiety disorder. Journal of Anxiety Disorders, 26, 393–400. doi:10.1016/j.janxdis.2012.01.003.
Alden, L. E., & Bieling, P. (1998). Interpersonal consequences of the pursuit of safety. Behaviour Research and Therapy, 36, 53–64. doi:10.1016/S0005-7967(97)00072-7.
Alden, L. E., & Trew, J. L. (2013). If it makes you happy: Engaging in kind acts increases positive affect in socially anxious individuals. Emotion, 13, 64–75. doi:10.1037/a0027761.
Alexander, R. A., & Govern, D. M. (1994). A new and simpler approximation for ANOVA under variance heterogeneity. Journal of Educational and Behavioral Statistics, 19, 91–101. doi:10.3102/10769986019002091.
Bentler, P. M. (2004). EQS structural equations program manual. Encino, CA: Multivariate Software Inc.
Bhullar, N., Schutte, N. S., & Malouff, J. M. (2011). Writing about satisfaction processes increases well-being. Individual Differences Research, 9, 22–32.
Biesanz, J. C., Falk, C. F., & Savalei, V. (2010). Assessing mediational models: Testing and interval estimation for indirect effects. Multivariate Behavioral Research, 45, 661–701. doi:10.1080/00273171.2010.498292.
Bjornebekk, G. (2007). Motivation and distance to goal time: Their effect on cognitive and affective manifestations (unpublished doctoral dissertation). University of Norway, Oslo.
Bjornebekk, G. (2008). Positive affect and negative affect as modulators of cognition and motivation: The rediscovery of affect in achievement goal theory. Scandanavian Journal of Educational Research, 52, 153–170. doi:10.1080/00313830801915788.
Bjornebekk, G. (2009). Psychometric properties of the scores on the behavioral inhibition and activation scales in a sample of Norwegian children. Educational and Psychological Measurement, 69, 636–654.
Buchanan, K. E., & Bardi, A. (2010). Acts of kindness and acts of novelty affect life satisfaction. The Journal of Social Psychology, 150, 235–237. doi:10.1080/00224540903365554.
Cheong, J., MacKinnon, D. P., & Khoo, S. T. (2003). Investigation of mediational processes using parallel process latent growth curve modeling. Structural Equation Modeling, 10, 238–262. doi:10.1207/S15328007SEM1002_5.
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). New York, NY: Guilford Press.
Davila, J., & Beck, J. G. (2002). Is social anxiety associated with impairment in close relationships? A preliminary investigation. Behavior Therapy, 33, 427–446. doi:10.1016/S0005-7894(02)80037-5.
Eisen, A. R., Rapee, R. M., & Barlow, D. H. (1990). The effects of breathing rate and pCO2 levels on relaxation and anxiety in a non-clinical population. Journal of Anxiety Disorders, 4, 183–190. doi:10.1016/0887-6185(90)90010-7.
Elliot, A. J. (2006). The hierarchical model of approach-avoidance motivation. Motivation and Emotion, 30, 111–116. doi:10.1007/s11031-006-9028-7.
Elliot, A. J., Gable, S. L., & Mapes, R. R. (2006). Approach and avoidance motivation in the social domain. Personality and Social Psychology Bulletin, 32, 378–391. doi:10.1177/0146167205282153.
Feske, U., & Chambless, D. L. (1995). Cognitive behavioral versus exposure only treatment for social phobia: A meta-analysis. Behavior Therapy, 26, 695–720. doi:10.1016/S0005-7894(05)80040-1.
Fink, M., Akimova, E., Spindelegger, C., Hahn, A., Lanzenberger, R., & Kasper, S. (2009). Social anxiety disorder: Epidemiology, biology and treatment. Psychiatria Danubina, 21, 533–542.
Fredrickson, B. L. (1998). What good are positive emotions? Review of General Psychology, 2, 300–319. doi:10.1037/1089-2680.2.3.300.
Gable, S. L. (2006). Approach and avoidance social motives and goals. Journal of Personality, 74, 175–222. doi:10.1111/j.1467-6494.2005.00373.x.
Gable, S. L., & Gosnell, C. L. (2013). Approach and avoidance behavior in interpersonal relationships. Emotion Review, 5, 269–274. doi:10.1177/1754073913477513.
Gould, R. A., Buckminster, S., Pollack, M. H., Otto, M. W., & Yap, L. (1997). Cognitive-behavioral and pharmacological treatment for social phobia: A meta-analysis. Clinical Psychology: Science and Practice, 4, 291–306.
Hawthorne, G., & Elliott, P. (2005). Imputing cross-sectional missing data: Comparison of common techniques. Australian and New Zealand Journal of Psychiatry, 39, 583–590. doi:10.1111/j.1440-1614.2005.01630.x.
Heerey, E. A., & Kring, A. M. (2007). Interpersonal consequences of social anxiety. Journal of Abnormal Psychology, 116, 125–134. doi:10.1037/0021-843X.116.1.125.
Heimberg, R. G., Mueller, G. P., Holt, C. S., Hope, D. A., & Liebowitz, M. R. (1992). Assessment of anxiety in social interaction and being observed by others: The Social Interaction Anxiety Scale and the Social Phobia Scale. Behavior Therapy, 23, 53–73. doi:10.1016/S0005-7894(05)80308-9.
Helgeson, V. S., & Palladino, D. K. (2012). Agentic and communal traits and health: Adolescents with and without diabetes. Personality and Social Psychology Bulletin, 38, 415–428. doi:10.1177/0146167211427149.
Holtforth, M. G., Bents, H., Mauler, B., & Grawe, K. (2006). Interpersonal distress as a mediator between avoidance goals and goal satisfaction in psychotherapy inpatients. Clinical Psychology and Psychotherapy, 13, 172–182. doi:10.1002/cpp.486.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. doi:10.1080/10705519909540118.
Johnstone, K. A., & Page, A. C. (2004). Attention to phobic stimuli during exposure: The effect of distraction on anxiety reduction, self-efficacy and perceived control. Behaviour Research and Therapy, 42, 249–275. doi:10.1016/S0005-7967(03)00137-2.
Kashdan, T. B., & Steger, M. F. (2006). Expanding the topography of social anxiety: An experience-sampling assessment of positive emotions, positive events, and emotion suppression. Psychological Science, 17, 120–128. doi:10.1111/j.1467-9280.2006.01674.x.
Kurtz, J. L., & Lyubomirsky, S. (2008). Toward a durable happiness. In S. J. Lopez (Ed.), Positive psychology: Exploring the best in people (Vol. 4, pp. 21–36)., Pursuing human flourishing Westport, CT: Praeger Publishers/Greenwood Publishing Group.
Levinson, C. A., Rodebaugh, T. L., & Frye, T. (2011). An examination of the factor, convergent, and discriminant validity of the behavioral inhibition system and behavioral activation system scales. Journal of Psychopathology and Behavioral Assessment, 33, 87–100.
Lyubomirsky, S., & Della Porta, M. D. (2010). Boosting happiness, buttressing resilience: Results from cognitive and behavioral interventions. In J. W. Reich, A. J. Zautra, & J. S. Hall (Eds.), Handbook of adult resilience (pp. 450–464). New York, NY: Guilford Press.
Lyubomirsky, S., & Dickerhoof, R. (2010). A construal approach to increasing happiness. In J. E. Maddux & J. P. Tangney (Eds.), Social psychological foundations of clinical psychology (pp. 229–244). New York, NY: Guilford Press.
Lyubomirsky, S., Sheldon, K. M., & Schkade, D. (2005). Pursuing happiness: The architecture of sustainable change. Review of General Psychology, 9, 111–131. doi:10.1037/1089-2680.9.2.111.
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36, 455–470. doi:10.1016/S0005-7967(97)10031-6.
McNulty, J. K., & Fincham, F. D. (2012). Beyond positive psychology? Toward a contextual view of psychological processes and well-being. American Psychologist, 67, 101–110. doi:10.1037/a0024572.
Meleshko, K. G. A., & Alden, L. E. (1993). Anxiety and self-disclosure: Toward a motivational model. Journal of Personality and Social Psychology, 64, 1000–1009. doi:10.1037/0022-3514.64.6.1000.
Muthén, B. O., & Curran, P. J. (1997). General longitudinal modeling of individual differences in experimental designs: A latent variable framework for analysis and power estimation. Psychological Methods, 2, 371–402. doi:10.1037/1082-989X.2.4.371.
Nikitin, J., & Freund, A. M. (2010). When wanting and fearing go together: The effect of co-occurring social approach and avoidance motivation on behavior, affect, and cognition. European Journal of Social Psychology, 40, 783–804.
Otake, K., Shimai, S., Tanaka-Matsumi, J., Otsui, K., & Fredrickson, B. L. (2006). Happy people become happier through kindness: A counting kindnesses intervention. Journal of Happiness Studies, 7, 361–375. doi:10.1007/s10902-005-3650-z.
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy, 35, 741–756.
Rodebaugh, T. L. (2009). Social phobia and perceived friendship quality. Journal of Anxiety Disorders, 23, 872–878. doi:10.1016/j.janxdis.2009.05.001.
Rodebaugh, T. L., Woods, C. M., & Heimberg, R. G. (2007). The reverse of social anxiety is not always the opposite: The reverse-scored items of the social interaction anxiety scale do not belong. Behavior Therapy, 38, 192–206. doi:10.1016/j.beth.2006.08.001.
Rodebaugh, T. L., Woods, C. M., Heimberg, R. G., Liebowitz, M. R., & Schneier, F. R. (2006). The factor structure and screening utility of the Social Interaction Anxiety Scale. Psychological Assessment, 18, 231–237. doi:10.1037/1040-3590.18.2.231.
Ryan, A. M., & Shim, S. S. (2006). Social achievement goals: The nature and consequences of different orientations toward social competence. Personality and Social Psychology Bulletin, 32, 1246–1263. doi:10.1177/0146167206289345.
Ryan, A. M., & Shim, S. S. (2008). An exploration of young adolescents’ social achievement goals and social adjustment in middle school. Journal of Educational Psychology, 100, 672–687. doi:10.1037/0022-0663.100.3.672.
Seaman, M. A., Levin, J. R., & Serlin, R. C. (1991). New developments in pairwise multiple comparisons: Some powerful and practicable procedures. Psychological Bulletin, 110, 577–586. doi:10.1037/0033-2909.110.3.577.
Selig, J. P., & Preacher, K. J. (2009). Mediation models for longitudinal data in developmental research. Research in Human Development, 6, 144–164. doi:10.1080/15427600902911247.
Shrive, F. M., Stuart, H., Quan, H., & Ghali, W. A. (2006). Dealing with missing data in a multi-question depression scale: A comparison of imputation methods. BMC Medical Research Methodology, 6, 57–67. doi:10.1186/1471-2288-6-57.
Sin, N. L., & Lyubomirsky, S. (2009). Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. Journal of Clinical Psychology, 65, 467–487. doi:10.1002/jclp.20593.
Sparrevohn, R. M., & Rapee, R. M. (2009). Self-disclosure, emotional expression and intimacy within romantic relationships of people with social phobia. Behaviour Research and Therapy, 47, 1074–1078. doi:10.1016/j.brat.2009.07.016.
Taylor, C. T., & Alden, L. E. (2011). To see ourselves as others see us: An experimental integration of the intra and interpersonal consequences of self-protection in social anxiety disorder. Journal of Abnormal Psychology, 120, 129–141. doi:10.1037/a0022127.
Thompson, E. R. (2007). Development and validation of an internationally reliable short-form of the positive and negative affect schedule (PANAS). Journal of Cross-Cultural Psychology, 38, 227–242. doi:10.1177/0022022106297301.
Trew, J. L., & Alden, L. E. (2012). Positive affect predicts avoidance goals in social interaction anxiety: Testing a hierarchical model of social goals. Cognitive Behaviour Therapy, 41, 174–183. doi:10.1080/16506073.2012.663402.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070. doi:10.1037/0022-3514.54.6.1063.
West, S. G., Biesanz, J. C., & Kwok, O. M. (2004). Within-subject and longitudinal experiments: Design and analysis issues. In C. Sansone, C. C. Morf, & A. T. Panter (Eds.), The Sage handbook of methods in social psychology (pp. 287–312). Thousand Oaks, CA: Sage.
Yuan, K. H., & Bentler, P. M. (2000). Three likelihood-based methods for mean and covariance structure analysis with nonnormal missing data. Sociological Methodology, 30, 165–200. doi:10.1111/0081-1750.00078.
Acknowledgments
This manuscript includes data from the first author’s doctoral dissertation. This research was supported by IODE Canada, the Social Sciences and Humanities Research Council of Canada, and the University of British Columbia. The authors would like to thank Sara Yuen, Elisa Choi, Carmen Gee, Brett Sinclair, Rachelle Pullmer, Angela Cheung, Uyoyouoghene Eto, Donya Samadi, Janet Jung, Lucinda Xin, Ingrid Tsang, Anna Bourak, Dawn Lee, Dedy Wong, Annie Tang, and Jade McGregor for their assistance with data collection and preparation, Dr. Rebecca Cobb for her feedback on an earlier draft of this manuscript, and Morgan Donahue, Dorianna Dickson, and Roza Mohammadi for their assistance with data coding.
Conflict of interest
The authors have no potential conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Trew, J.L., Alden, L.E. Kindness reduces avoidance goals in socially anxious individuals. Motiv Emot 39, 892–907 (2015). https://doi.org/10.1007/s11031-015-9499-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11031-015-9499-5