
Abstract
This article focuses on the assessment of mechanistic relations with specific attention to medicine, where mechanistic models are widely employed. I first survey recent contributions in the philosophical literature on mechanistic causation, and then take issue with Federica Russo and Jon Williamson’s thesis that two types of evidence, probabilistic and mechanistic, are at stake in the health sciences. I argue instead that a distinction should be drawn between previously acquired knowledge of mechanisms and yet-to-be-discovered knowledge of mechanisms and that both probabilistic evidence and manipulation are essential with respect to newly discovered mechanisms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Mechanistic models are widely employed in the biomedical sciences. A browse through medical journals and textbooks shows how the notion of mechanism is extensively used to refer to mechanisms of diseases, for instance, the mechanisms of heart failure, cardiovascular diseases, migraine, obesity, complications of diabetes, and post-traumatic stress disorders. The notion is also invoked to refer to drugs and treatments, for instance, deep brain stimulation and percutaneous coronary intervention, and to indicate mechanisms by which socioeconomic status influences health. Mechanistic terms are even used to indicate pathologies that remain mysterious: ‘the mechanism of the disease’ is sometimes a label for a pathology that is largely unknown and that researchers are trying to discover. In many medical cases, the entity referred to as the mechanism is the final target of the research—something that is to be investigated further, such as the development of peripartum cardiomyopathy [1] or Paget’s disease [2] or the mechanisms linking infertility and congenital malformation [3]. At the same time, the mechanistic approach has increasingly been used as an account of causation in the contemporary philosophical debate, with a number of different mechanistic views being developed since the mid 1980s.Footnote 1
This article focuses on the assessment of mechanistic relations, with specific attention to medicine. The aim of the article is twofold. I will first survey recent contributions in the philosophical literature on mechanisms in so far as they are relevant to causal investigations in the health sciences. I will then take issue with a particular thesis put forward by Federica Russo and Jon Williamson, viz., that two different types of evidence are at stake in the health sciences, namely, probabilistic evidence and mechanistic evidence. Specifically, I will argue that with regard to the notion of mechanistic knowledge, a distinction should be drawn between previously acquired knowledge of mechanisms and yet-to-be-discovered knowledge of mechanisms and that both probabilistic evidence and manipulation are essential with respect to newly discovered mechanisms. Though crucial for the causation debate in general, the issue is tackled here with respect to medicine since the philosophy of medicine has recently witnessed a growing interest in mechanism.
Mechanisms and diseases
Philosophical views on mechanism have proliferated in the last few decades, with some recent theories—such as those of Machamer, Darden, and Craver—focusing specifically on biology and the neurosciences. The biomedical sciences commonly describe diseases in mechanistic terms derived from molecular medicine, and bedside medicine has been increasingly accompanied by laboratory-based investigations of biochemical events that lead to the pathology. The notion of mechanism is extensively employed to refer to complex multilevel systems, be they the workings of pathologies or of some therapeutic means. In a contribution specifically devoted to causation in medicine, ‘Interpreting Causality in the Health Sciences’ [6], Federica Russo and Jon Williamson argue that two kinds of evidence are at play in the health sciences, namely, probabilistic evidence and mechanistic evidence. While agreeing that these notions embody two crucial aspects of medical causation, I shall question whether such a distinction proves the fittest. I believe that to account for mechanistic causation—both within the health sciences and more generally—some clarification is in order and further distinctions should be drawn. I will start off with a preliminary outline of some of the main contemporary mechanistic views and their possible applications in medicine, and shall then address some specific issues concerning the identification of mechanisms.
The locus for any contemporary mechanistic account of causation is Wesley Salmon’s probabilistic theory, put forward in the 1980s as a process theory of causation, with genuine causal processes—as opposed to pseudo-processes—being identified by means of the principle of mark transmission. Salmon, in other words, proposed that a process is to be deemed causal if—were a mark, i.e., a modification of its structure, to be imposed on the process—it would be transmitted along the process from the point of interaction onwards without any additional intervention (see [7, 8]). In the early 1990s, this theory was criticised especially by Phil Dowe, whose main goal was to preserve Salmon’s objective and physical account of causation while getting rid of any use of counterfactuals. According to Dowe’s ‘conserved-quantity theory’, a causal process is the world lineFootnote 2 of an object exhibiting a conserved quantity, and a causal interaction is an intersection of processes in which a conserved quantity is exchanged [9].
In the last few years, various different notions of mechanism have been put forward that aim at being widely applied well beyond physics, the discipline to which Salmon’s and Dowe’s theories mainly refer. Among the definitions advanced, Machamer, Darden, and Craver define mechanisms as ‘entities and activities organised such that they are productive of regular changes from start-up to finish or termination conditions’ [10, p. 3]. Glennan states that ‘a mechanism for a behaviour is a complex system that produced that behaviour by the interaction of a number of parts, where the interactions between parts can be characterised by direct, invariant, change-relating generalizations’ [11, p. S344]. Bechtel and Abrahamsen maintain that ‘a mechanism is a structure performing a function in virtue of its component parts, component operations, and their organizations’ [12, p. 423].
Although more recent positions are gaining momentum, Salmon’s view has been deemed capable of capturing important general features of medical causation and its historical development. According to Paolo Vineis, Salmon’s idea of the propagation of a mark over time, to which the identification of genuinely causal processes is anchored, easily connects to the nineteenth century conception of the localisation of a disease, which holds that the cause is an alteration in the tissues and is characteristic of a given agent. The cause is construed by Vineis as a sort of ‘signature’ persisting over time, a broadly employed concept in the history of medicine that is now widespread due to the advances of molecular medicine. The concept is adopted within certain theories to account for, for instance, genetic alterations that leave a mark that is then transmitted. On a par with what has happened in the philosophical tradition—and often intersecting with it—medicine, throughout its history, has been using a number of different concepts of cause, and contemporary medicine still chooses to follow a number of lines of thought, often combining one with the other. Different perspectives can suit different medical fields, and molecular research ‘is the context in which the new causal pathways suggested by the intertwining between the probabilistic science of epidemiology and the idea of “marks propagating over time” of molecular biology can create and reinforce new causal hypotheses’ [13, p. 653]. Mechanist views, such as those of Machamer, Darden, and Craver, Bechtel and Abrahamsen, and Glennan, in turn can be held to provide an important perspective suiting the biomedical sciences, especially by virtue of their stress on the complexity and dynamism of mechanisms, which are internally structured and involve different levels of reality (e.g., molecules, genes, tissues, organs, etc.).Footnote 3 A multilevel notion of mechanism permits the representation of diseases as complex biopsychosocial phenomena resulting from the interaction of multiple factors, not only on the biochemical and genetic levels but also on the environmental, socioeconomic, and psychological levels.Footnote 4
Over and above differences between individual accounts, it can be claimed that a mechanism is usually construed as a system composed of entities that interact with each other. Entities must be localized and hierarchically organized within the system. It is not only their presence but also the organization of the entities and their activities that determine the ways in which they produce the phenomenon. Entities must be appropriately located along different levels and properly structured and oriented, and their activities and interactions must have a specific temporal order, rhythm, and duration. Built up with more or less basic ‘blocks’, mechanisms are understood as systems that can be decomposed according to structural or functional criteria, or both. Furthermore, continuity is usually required: entities and their activities must exhibit productive continuity, with each stage of the mechanism’s behaviour giving rise to the next. It is the ideas of productivity, continuity, and decomposability that also seem to be crucial in the medical uses of mechanistic terms. The link from remote causes to symptoms is conceived as a continuous chain of causal steps. And the possibility of thinking in terms of composable and decomposable systems allows us to single out a number of, so to speak, sub-nexuses, and hence, to deal with problems one at a time, thereby facilitating our understanding of the disease.
What is, therefore, the relevance of mechanistic causation for the health sciences? In general, mechanistic accounts are ontologically loaded: having mechanistic knowledge of a phenomenon is being able to say what really makes it work ‘out there’. It is on such grounds that mechanistic explanations are usually elaborated; mechanisms are largely—although, as will be shown, not only—sought in order to explain, to present the portion of the mechanistic network underlying the phenomenon at stake. Whereas the choice to select and highlight a particular portion of such a network can be affected by the context of enquiry, the mechanistic network itself is taken to be utterly objective and independent of any context.Footnote 5 A typical biomedical theory can be defined as a structure of overlapping inter-level causal models, which ‘usually constitute a series of idealized prototypical mechanisms.… Narrow classes of mechanisms, usually described in qualitative multilevel causal language,… constitute the vast majority of current biomedical explainers’ [17, pp. 2, 4].Footnote 6 In general, medical explanations require the specification of complex mechanisms that clarify the actions and effects of pathogenetic factors and describe the details of the processes these factors give rise to. Although complete and detailed mechanistic knowledge is rarely achieved, mechanisms are sought for explanatory purposes; medical researchers do not rest content with an understanding of what the causal factors are, but aim to know how one gets from the causes to the effect, i.e., what goes on between the causes and the effect. For instance, empirical evidence from observational epidemiology led to the conviction that tobacco causes lung cancer long before such a correlation was explained. Only relatively recently was a mechanism sketched: ‘in bronchial epithelial tissues, certain compounds of tobacco smoke, benzo[a]pyrenes, form DNA adducts at mutational hot-spots of the p53 oncogene. At last, we had an explanation!’ [19, p. 2004] As already pointed out by Salmon, to explain in mechanistic terms is to open nature’s black box. Moreover, mechanistic explanations often provide the framework for generalizing the results of a given research beyond the confines of the specific cases that have been tested and of the study particulars. The tracing of a mechanism usually also reduces the range of plausible explanations; alternatives are ruled out because any explanation will have to account not only for the association between the causal factors and the outcome but also for the explanatory power of the mechanism that has been identified.
In the context of the health sciences, the identification of the component parts and their mutual organization and interactions is crucial not only for a thorough understanding of the disease but also sometimes for its very characterization and classification. Whereas infectious diseases (e.g., tuberculosis) are classified on the basis of their etiological factor (e.g., Mycobacterium tuberculosis), the classification of cancer and other chronic diseases is much more complex. As far as morphology is concerned, ‘neoplasia’ and ‘anaplasia’ as attributes of cancer are hard to define in a straightforward way, and pathological tissue are difficult to differentiate from normal tissue in some cancers but obvious in others. From an etiological point of view, it is often hard to disentangle the role of single agents from multiple and/or mixed exposures. From the point of view of manifestations the situation does not look much better; for instance, ‘lung cancers due to asbestos seem to be identical to those due to smoking, and chronic myeloid leukemia due to benzene is identical to that caused by ionizing radiation. An alternative … might be a mechanistic classification. For example, cancers could be classified according to the presence of point mutations, chromosome rearrangement, or an “epigenetic” event’. A thorough investigation of pathogenetic mechanisms, including ‘specific mechanistic steps in carcinogenesis’, is needed to ‘adopt an unequivocal definition of cancer’ [20, pp. 951–952]. Often characterizations of diseases in molecular terms have allowed a new taxonomy for diseases, moving away from a phenotypic disease definition to one based on causative events and pathways. Such mechanistic definitions of diseases broke down ‘the disease heterogeneity that the phenotypic definitions had masked.… Little could be established with certainty about disease pathogenesis from measurements of physiological parameters, or even ordinary histopathology—these approaches could describe an abnormality, but could shed no conclusive light on disease causation or process’ [21, p. 477].
Mechanisms play some, more restricted, role with respect to diagnosis too. Also thanks to technological progress and increasing availability of achieved knowledge, it is no longer possible to work at the patient’s bedside without being aware of what is regarded as the mechanism of the pathology, i.e., its standard behaviour. At the same time, it is very rare to have patients who present all the alleged ‘typical’ symptoms of a given disease, and cases may occur in which clinicians do not know how to relate some signs to the mechanism believed to underlie the disease. While the availability of general models means that diseases are diagnosed by placing the patient’s situation in a larger framework of consolidated knowledge, each individual presents variations that distance him or her from what is taken to be the usual disease mechanism. Facing diseases in patients, clinicians see single occurrences as instantiations of a more general mechanism, albeit instantiations that often exhibit a number of peculiarities.
Finally, mechanisms can play a role with regard to the design and adoption of therapies as well as to the promotion of prevention strategies; the greater the mechanistic knowledge available, the more effective therapies and public health campaigns are likely to be. However, mechanisms are not essential in this respect. Mechanistic knowledge can provide the premises for the elaboration of the therapy, but in many cases the therapy itself can precede the discovery of mechanistic details. As pointed out by Vineis and Ghisleni [22], the history of medicine is full of examples in which the preventive measure was actually discovered much earlier (by a few to many decades) than the causal agent and the actual mechanism of action of the disease (see Table 1). Often the presence of a mechanism is hypothesized, but waiting for mechanistic knowledge would mean a serious delay in the implementation of those therapies and preventive strategies capable of reducing the incidence of the pathology.
Probabilistic evidence, mechanistic evidence, and the assessment of mechanistic relations
In this next section, I consider the relation between probabilistic evidence and mechanistic evidence and the role of manipulation in the assessment of mechanistic relations. In their 2007 paper, Russo and Williamson state that ‘two different types of evidence are at stake when deciding whether or not to accept a causal claim’, that is, ‘mechanistic and probabilistic evidence’ [6, pp. 163–164]. How is mechanistic evidence to be understood? What does it amount to exactly, and can it be conceived of on its own, separate from probabilistic evidence? I believe that some clarification and further distinctions are needed to have a better grasp of the assessment and roles of mechanistic relations.
To start with, it does not seem possible to think of mechanisms separately from probabilistic evidence. The assessment that a mechanistic production system is in place cannot but start from some probabilistic relations; the hypothesis that a mechanism is in place rests, first of all, on detected correlations. According to Russo and Williamson, ‘monistic accounts attempt to analyse causality solely in terms of one type of evidence, e.g., solely in terms of mechanisms or solely in terms of probabilistic relations’ [6, p. 158]. But it is hard to see how probabilistic relations can be neglected in the construction of mechanistic knowledge. Probabilistic evidence is required to substantiate mechanistic claims. In the contemporary philosophical debate on causality, ever since Salmon’s theory of causation was put forward in the 1980s, probability and mechanisms have been dealt with together, as closely linked and necessary to elucidate causation. Although the way in which probability and mechanisms are combined in Salmon’s view has been deemed entirely satisfactory, he has put forward an extended theory in which statistical relations and aleatory causality, defined in terms of processes, are both crucial to account for mechanistic causation.Footnote 7 Furthermore, neo-mechanist accounts also admit that mechanisms are largely of a probabilistic sort.
To further clarify what can be meant by ‘mechanistic evidence’, I believe a distinction should be drawn between evidence on mechanisms that have already been disclosed and evidence for mechanisms that are currently unknown and yet to be discovered. With respect to unknown mechanisms, the literature highlights how previously acquired mechanistic knowledge can play an important role in causal inference and in the elaboration of explanatory accounts. According to Paul Thagard, for instance, ‘knowledge of mechanisms is itself knowledge of causally related events which must have somehow been previously acquired’, and ‘for there to be a known mechanism by which c produces e, c must be a component or occurrence in a system of parts that is known to interact to produce e’ [27, pp. 68–69; italics added]. As highlighted by Thagard [28], being aware of an already established mechanism connecting events of type c to events of type e can facilitate the inference that c 1 causes e 1, enhance explanatory coherence, and deepen theories. In a recent paper on the role of mechanisms in causal understanding—and misunderstanding—in the health sciences, Leen de Vreese also argues for the confirmative power of mechanisms: as ‘inner causal indicators’, they are held to be an important tool which ‘can confirm the existence of possible causal relations assumed to be present on the basis of an outer indicator’ [29, p. 19]. This clearly works only in cases in which the mechanisms at stake are already known. Previously acquired mechanistic knowledge can play a confirmatory role as well as help in hypothesizing that some mechanistic relations hold in the investigation of still poorly understood phenomena. Causal hypotheses are not elaborated in a vacuum, and established mechanistic knowledge can provide useful support (for instance, insofar as analogies with the phenomenon under enquiry can be drawn).
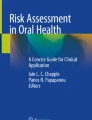
Yet what about the assessment of newly discovered mechanistic relations? How can it be established for the first time that a mechanism is in place? Obviously, in such cases, one cannot refer to mechanistic evidence as simply standing for evidence of something that is mechanistically connected. To get from correlations to mechanistic claims one usually needs to perform some interventions.Footnote 8 It is by testing hypothesized mechanisms that mechanistic relations are assessed. According to Thagard [27, 35], for instance, Barry Marshall and Robin Warren’s bacterial theory of ulcers, developed in 1983, illustrates how a causal relation is established. What was baptized ‘Helicobacter pylori’ bacterium had been observed in biopsies by both Warren and Marshall—starting with endoscopic examinations in 100 patients—and, later, by a number of other researchers. To answer the key question of whether bacteria cause ulcers, it was first necessary to show that Helicobacter pylori had the power to increase the occurrence of ulcers. Initial evidence showed that people with the bacteria more frequently had ulcers than those without. This did not suffice. In order to get from correlations to knowledge of mechanisms, studies regarding ‘antibiotics’ impact were performed which showed that the frequency of ulcers dropped substantially in patients whose bacteria had been eliminated’ [27, p. 66]. Warren and Marshall even performed some experiments on themselves to this end, ingesting bacteria and causing ulcers in themselves. Figure 1 illustrates how different sources of evidence, including evidence from manipulations (‘eradicating bacteria cures ulcers’), had to come together for the causal hypothesis—that Helicobacter pylori causes ulcers—to be accepted by the medical community. Mechanistic evidence as evidence for newly discovered mechanisms hence had to come from probabilistic relations, previous knowledge, and interventions.

‘Coherence relations in assessing the acceptability in 1995 of the hypothesis that bacteria cause ulcers. Thin lines indicate positive constraints based on hypotheses explaining evidence, and thick lines indicate negative constraints based on contradiction or competition’ (figure and description from Thagard [35, p. 132], Reprinted with permission from Elsevier)
Most disease mechanisms are extremely complex and intricate, and it takes many years of coordinated efforts by a large number of researchers to get from the detection of a strong correlation (or, rather, a number of correlations) to mechanistic claims. Another example can be provided by recent investigations on the relation between aflatoxins and liver cancer, which in the last couple of decades has been an extensive focus in the medical literature.Footnote 9 Aflatoxins were first isolated in the 1960s; the International Agency for Research on Cancer (IARC) first recognized aflatoxins as a carcinogenic in 1976, and subsequently reaffirmed naturally occurring mixtures of aflatoxins and AFB1 as Group I carcinogens (carcinogenic to humans). The first studies revealing an association between dietary exposure to AFB1 and an increased incidence of hepatocellular carcinoma (HCC) date back to the late 1970s. It was first observed that areas with the highest presumed aflatoxin intake (e.g., areas in Mozambique, South Africa, and Swaziland) also had the highest liver cancer rates. Areas with the largest exposure to aflatoxins also happened to be areas with the largest incidence of the hepatitis B virus (HBV), another risk factor involved in the aetiology of HCC.Footnote 10 Epidemiological studies have shown ‘that the two factors can act synergistically to increase the risk of HCC, but the underlying cellular and molecular mechanisms of interactions are as yet undefined’ [43, p. S441].
In the last decade or so, a number of studies have focused on the p53 tumour suppressor gene (TP53), the most common mutated gene detected in human cancers. Specific p53 damage—a mutation affecting the third nucleotide of codon 249 in the p53 gene (249ser p53 mutation)—is currently regarded as the starting point for the construction of mechanistic knowledge on aflatoxin-associated hepatocarcinogenesis: ‘a correlation at the individual level between aflatoxin exposure and the presence of the 249ser p53 mutation in hepatocellular carcinoma would … provide more direct evidence of a causal association’ [41, p. 1844]. A large amount of data has been collected on the occurrence of p53 mutations in hepatocellular carcinomas in many regions of the world with high exposure to aflatoxins, and a high frequency (more than 50%) of GC to TA transversions occurring at the third nucleotide of codon 249 has been detected in those regions as well. What is taken as the crucial point is that the same mutation is detected in HCC cases and in cases of high exposure to aflatoxins. Numerous investigations are being conducted to determine the frequency of TP53 mutations in populations with various levels of aflatoxin exposure. Research has been proceeding by observing that the frequency of the mutation at codon 249 parallels the level of AFB1 exposure, and investigators have taken this hint as far as to claim that ‘the most common mutations of p53 in HCC are the G to T transversions in codon 249 caused by aflatoxin exposure’ [44, p. 130; italics added]. These studies aim to provide hints regarding mechanistic activity. That HCC can be aflatoxin-dependent was acknowledged some time ago. What is still missing is an understanding of what happens between exposure to aflatoxins and onset of the tumour. Since specific genetic changes thought to be associated with aflatoxins have been observed, sophisticated experimental research, such as in vitro studies on DNA lesions formed by the toxins, are being carried out to shed light on the mechanism leading from the exposure to tumours. Mechanistic hypotheses first elaborated on the basis of probabilistic evidence and previously acquired mechanistic knowledge are thus being tested in order to get from correlations to the assessment of genuinely productive links. Newly assessed mechanistic knowledge, once established, is, in turn, likely to pave the way for further mechanistic enquiries on tumours and carcinogenicity.
Some final remarks: Looking for guidelines?
Causation in medicine can be seen as multifaceted: ‘a review of the various approaches to causation that have been taken by philosophers over the past two millennia suggests that the concept of causation may not be unitary.… Several of these diverse approaches need to be drawn on and intertwined to constitute an adequately robust analysis of causation in biology and medicine’ [45, p. 298]. Among the notions of causation, those that appear to emerge most clearly in biomedical examples are no doubt probabilistic causation (e.g., carcinogenetic factors increasing the frequency of occurrence of certain effects) and mechanistic causation (e.g., mechanisms of cancer induction). Generally speaking, mechanisms are first just sketchily hypothesized and then detailed as research develops. The search for causal mechanisms offers an understanding of how the pathology develops, which, most of the time, already fits and is supported by established knowledge. Yet an understanding of how one is to learn about mechanisms cannot be confined to analogies with already acquired mechanistic knowledge. Manipulative causation also plays a role that must not be neglected or underestimated.
No agreement has been reached on the proper and precise methodology for isolating mechanistic relations in medicine. The search for them, though, is undoubtedly assiduously pursued, and it is done with rough guidelines for organizing prima facie evidence for the existence of mechanisms. An example is provided by Vineis and Porta, who maintain that ‘a complete understanding of the cancer process in humans is expected to arise from a combination of “conventional” epidemiologic investigations, aimed at the investigation of risk factors, and of biomarker-based studies, aimed at the elucidation of intermediate steps’ [20, p. 954]. They argue that in order to evaluate whether a certain mechanism is active in cancer induction, something analogous to Austin Hill’s guidelines (see [46])—which, though far from being unproblematic and uncontroversial, are still very popularFootnote 11—could work; for example,
(1) Is the method used to investigate the mechanistic role of an end point reliable and reproducible? (2) Have the agent and the end point been studied in different species and/or different test systems? (3) Are there potential alternatives to a cause-effect interpretation of the findings (including bias, confounding, or chance)? (4) Is the design of the study that disclosed the association appropriate and meaningful? (5) Is the association between the agent, the measured end point, and cancer compatible with background knowledge on the carcinogenic process? [20, p. 955]
These questions are taken to be helpful in establishing whether a certain mechanism is functioning. If one takes a look at scientific works, it emerges that considerations even closer to some of Hill’s guidelines are expressed in order to assess whether something constitutes a mechanism. Going back to the case of aflatoxins, Montesano et al. [41, p. 1848] maintain that the strong association between aflatoxin exposure and the occurrence of the 249ser p53 mutation in hepatocellular carcinoma is (also) supported by the sound evidence that in regions of high exposure to aflatoxins, the 249ser p53 mutation is an early event. They argue that it is also supported in the perinatal period and then continues for the entire lifespan of the individual, thus recalling Hill’s second criterion regarding the temporal relation between hypothesized cause and effect. Sylla et al., in turn, highlight the biological plausibility of exposure-risk associations [42, p. 188] established thanks to the availability of biomarkers of exposure, while Suriawinata reports that ‘a dose-dependent relationship between p53 mutation load of 249ser mutant cells and the intake of AFB1 in non-tumorous liver tissue has been observed’ [50, p. 80; italics added]. Thus, they recall, respectively, Hill’s criterion of plausibility and criterion regarding the dose–response relation.
At the moment it is highly unlikely that a consensus will be reached on shared and uncontroversial criterions, but guidelines like those presented undoubtedly help to clarify what mechanistic evidence can count for. In this respect, among Hill’s guidelines—and in any attempt to revise and improve them—experimental evidence must be acknowledged as crucial in the assessment of mechanistic nexuses.
Notes
A world line is, in turn, defined as ‘the collection of points on a spacetime diagram that represents the history of an object. This means that processes are represented by elongated regions, or “worms” in spacetime’ [9, p. 90].
Machamer, Darden, Craver, and Glennan have been labeled as ‘neo-mechanists’; see Faucher [14].
See Campaner [15].
A different view is supported by Daniel Sirtes [16], who has been developing a ‘pragmatic-ontic account of mechanistic explanation’.
While criticizing the most recent revival of the mechanistic approach, and especially Machamer, Darden, and Craver’s notion of ‘activity’ as ‘far too opaque’, Schaffner admits that he has ‘frequently utilised references to “mechanisms” as another way to describe the “models” that are so widely found in biology, and which function broadly as surrogates for theories in the biomedical sciences’ [18, p. 398].
The role of interventions in the assessment of mechanistic relations has been discussed by Machamer, Darden, and Craver in various contributions; see, for instance, Darden and Craver [30], Machamer [31], Craver [32]. These scholars conceive of interventions mainly in a counterfactual sense. On this, see Campaner [33] and Campaner and Galavotti [34].
I thank Prof. Vineis for drawing my attention to this example. Mycotoxins are a broad class of toxic fungal metabolites estimated to contaminate up to 25% of the world’s food supplies. One potent group of mycotoxins are the aflatoxins, which are secondary metabolites of Aspergillus flavus (aflatoxins B1 and B2) and Aspergillus parasiticus (aflatoxins B1, B2, G1, and G2), aflatoxin B1 (AFB1) being the most common. They are present as mixtures in food (cereals, figs, oilseeds, nuts, tobacco, etc.), which work as substrates that allow for the growth and production of aflatoxin by aflatoxigenic moulds and are especially frequent in developing countries.
See, for instance, Strosnider et al. [35]; Williams et al. [36]; Wang and Tang [37]; Bennett and Klich [38]. Investigating the role that aflatoxins can play in the pathogenesis of hepatocellular carcinoma presents a number of difficulties. It is complicated to differentiate the influence of aflatoxins from that of HBV, to understand how representative the sampling of dietary components is at the population level, to estimate precisely human exposure, and, more generally, to collect data in the most affected countries (the poorest in the world). The use of animal models in studying aflatoxin carcinogenicity is controversial; see, for instance, Cardwell and Henry [39]; Montesano et al. [40]; Sylla et al. [41]; Turner et al. [42].
References
Sliwa, K., J. Fett, and U. Elkayan. 2006. Peripartum cardiomyopathy. Lancet 368: 687–693.
Whyte, M.P. 2006. Paget’s disease of bone. New England Journal of Medicine 355: 593–600.
Zhu, J.L., O. Basso, C. Obel, C. Bille, and J. Olsen. 2006. Infertility, infertility treatment, and congenital malformation: Danish national birth cohort. British Medical Journal 333: 679.
Stathis, P. 2002. Causation and mechanism. In Causation and explanation, 107–133. Durham, UK: Acumen Publishing Ltd.
Glennan, S. 2009. Mechanisms. In The oxford handbook of causation, ed. H. Beebee, C. Hitchcock, and P. Menzies, 315–325. Oxford: Oxford University Press.
Russo, F., and J. Williamson. 2007. Interpreting causality in the health sciences. International Studies in the Philosophy of Science 21: 157–170.
Salmon, W. 1984. Scientific explanation and the causal structure of the world. Princeton: Princeton University Press.
Salmon, W. 1998. Causality and explanation. Oxford: Oxford University Press.
Dowe, P. 2000. Physical causation. Cambridge: Cambridge University Press.
Machamer, P., L. Darden, and C. Craver. 2000. Thinking about mechanisms. Philosophy of Science 67: 1–25.
Glennan, S. 2002. Rethinking mechanistic explanation. Philosophy of Science 69: S342–S353.
Bechtel, W., and A. Abrahamsen. 2005. Explanation: A mechanist alternative. Studies in the History and Philosophy of the Biological and Biomedical Sciences 36: 421–441.
Vineis, P. 2000. Exposure, mutations and the history of causality. Journal of Epidemiology and Community Health 54: 652–653.
Faucher, L. 2006. What’s behind a smile? The return of mechanism: Reply to Schaffner. Synthese 151: 403–409.
Campaner, R. Forthcoming. Causality and explanation: Issues from epidemiology. In Explanation, prediction, and confirmation: New trends and old ones reconsidered, ed. S. Hartmann, M. Weber, W. J. Gonzalez, D. Dieks and T. Uebel. Dordrecht: Springer.
Sirtes, D. Working paper. A pragmatic-ontic account of mechanistic explanation. Phil-Sci Archive. http://philsci-archive.pitt.edu/5181/. Accessed Nov. 3, 2010.
Schaffner, K. Forthcoming. Theories, models, and equations in biology: The heuristic search for emergent simplifications in neurobiology. Phil-Sci Archive. http://philsci-archive.pitt.edu/3289/. Accessed Nov. 3, 2010.
Schaffner, K. 2006. Reduction: The Cheshire cat problem and a return to roots. Synthese 151: 377–402.
Vandenbroucke, J. 1998. Medical journals and the shaping of medical knowledge. Lancet 352: 2001–2006.
Vineis, P., and M. Porta. 1996. Causal thinking, biomarkers, and mechanisms of carcinogenesis. Journal of Clinical Epidemiology 49: 951–956.
Bell, J.I. 1999. Clinical research is dead; long live clinical research. Nature Medicine 5: 477–478.
Vineis, P., and M. Ghisleni. 2004. Risks, causality and the precautionary principle. Topoi 23: 203–210.
Wynder, E.L. 1994. Studies in mechanism and prevention: Striking a proper balance. American Journal of Epidemiology 139: 547–549.
Galavotti, M.C. 2008. Causal pluralism and context. In Reasoning, Rationality and Probability, ed. M.C. Galavotti, R. Scazzieri, and P. Suppes, 233–252. Stanford: CSLI.
Hitchcock, C. 1995. Discussion: Salmon on explanatory relevance. Philosophy of Science 62: 304–320.
Hitchcock, C. 1996. The mechanist and the snail. Philosophical Studies 84: 91–105.
Thagard, P. 1998. Explaining disease: Causes, correlations, and mechanisms. Minds and Machines 8: 61–78.
Thagard, P. 2007. Coherence, truth, and the development of scientific knowledge. Philosophy of Science 74: 28–47.
De Vreese, L. 2008. Causal (mis)understanding and the search for scientific explanations: A case study from the history of medicine. Studies in the History and Philosophy of the Biological and Biomedical Sciences 39: 14–24.
Darden, L., and C. Craver. 2002. Strategies in the interfield discovery of the mechanism of protein synthesis. Studies in the History and Philosophy of Biology and Biomedical Sciences 22: 1–28.
Machamer, P. 2004. Counterfactuals and causal explanation. International Studies in the Philosophy of Science 18: 41–72.
Craver, C. 2007. Explaining the brain. Oxford: Oxford University Press.
Campaner, R. 2006. Mechanisms and counterfactual: A different glimpse of the (secret?) connexion. Philosophica 77: 15–44.
Campaner, R., and M.C. Galavotti. 2010. Evidence and the assessment of causal relations in the health sciences. Paper presented at the Progress in Medicine Conference, University of Bristol, Bristol, U.K., April 13-15.
Thagard, P. 1998. Ulcers and bacteria I: Discovery and acceptance. Studies in History and Philosophy of Biological and Biomedical Sciences 29: 107–136.
Strosnider, A., E. Azziz-Baumgartner, M. Banziger, et al. 2006. Workgroup report: Public health strategies for reducing aflatoxin exposure in developing countries. Environmental Health Perspectives 114: 1898–1903.
Williams, J.H., T.D. Phillips, P.E. Jolly, J.K. Stiles, C.M. Jolly, and D. Aggarwal. 2004. Human aflatoxicosis in developing countries: A review of toxicology, exposure, potential health consequences and interventions. American Journal of Clinical Nutrition 80: 1106–1122.
Wang, J., and L. Tang. 2005. Epidemiology of aflatoxin exposure and human liver cancer. In Aflatoxin and food safety, ed. H.K. Abbas, 195–211. Boca Raton, FL: CRC Press.
Bennett, W., and M. Klich. 2003. Mycotoxins. Clinical Microbiology Reviews 16: 497–516.
Cardwell, K.F., and S.H. Henry. 2005. Risk of exposure to and mitigation of effects of aflatoxin on human health: A West African example. In Aflatoxin and food safety, ed. H.K. Abbas, 213–235. Boca Raton, FL: CRC Press.
Montesano, R., P. Hainaut, and C.P. Wild. 1997. Hepatocellular carcinoma: From gene to public health. Journal of the National Cancer Institute 89: 1844–1851.
Sylla, A., M.S. Diallo, J. Castegnaro, and C.P. Wild. 1999. Interactions between hepatitis B virus infection and exposure to aflatoxins in the development of hepatocellular carcinoma: A molecular epidemiological approach. Mutation Research 428: 187–196.
Turner, P.C., A. Sylla, M.S. Diallo, J.J. Castegnaro, A.J. Hall, and C.P. Wild. 2002. The role of aflatoxins and hepatitis viruses in the etiopathogenesis of hepatocellular carcinoma: A basis for primary prevention in Guinea-Conarky, West Africa. Journal of Gastroenterology and Hepatology 17: S441–S448.
McKillop, I.H., D.M. Moran, X. Jin, and L.G. Koniaris. 2006. Molecular pathogenesis of hepatocellular carcinoma. Journal of Surgical Research 136: 125–135.
Schaffner, K. 1993. Discovery and explanation in biology and medicine. Chicago: University of Chicago Press.
Hill, B. 1965. The environment of disease: Association or causation? Proceedings of the Royal Society of Medicine 58: 295–300.
Charlton, B.G. 1996. Attribution of causation in epidemiology: Chain or mosaic? Journal of Clinical Epidemiology 49: 105–107.
Weed, D. 1997. On the use of causal criteria. International Journal of Epidemiology 26: 1137–1141.
Wynder, E.L. 1996. Invited commentary: Response to Science article, ‘Epidemiology faces its limits’. American Journal of Epidemiology 143: 747–749.
Suriawinata, A., and X. Ruliang. 2004. An update on the molecular genetics of hepatocellular carcinoma. Seminars in Liver Disease 24: 77–88.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Campaner, R. Understanding mechanisms in the health sciences. Theor Med Bioeth 32, 5–17 (2011). https://doi.org/10.1007/s11017-010-9166-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11017-010-9166-5