
Abstract
Imatinib, nilotinib, dasatinib, bosutinib, ponatinib, and asciminib are FDA-approved tyrosine kinase inhibitors (TKIs) for chronic myeloid leukemia (CML), each of which has a specific pharmacological profile. Asciminib has been recently (2021) approved for patients resistant to former TKIs, and because the binding site of this drug (the myristoyl pocket in the ABL1 kinase) is different from that of other TKIs (ATP-binding sites), it is, therefore, effective against T315I mutation of BCR-ABL oncoprotein. All TKIs have a different pharmacological profile due to different chemical structures. Imatinib is the only TKI whose absorption depends on both influx (OCT1 and OATP1A2) and efflux (ABCB1 and ABCG2) transporters, whereas the others rely only on efflux transporters. The efflux of dasatinib is also regulated by ABCC4 and ABCC6 transporters. Nilotinib and ponatinib are transported passively, as no role of transporters has been found in their case. A phenomenon common to all in the metabolic aspect is that the CYP3A4 isoform of CYP450 primarily metabolizes TKIs. Not only does CYP3A4, flavin-containing monooxygenase 3 (FMO3), and uridine 5'-diphospho-glucuronosyltransferase (UGT) also metabolize dasatinib, and similarly, by glucuronidation process, asciminib gets metabolized by UGT enzymes (UGT1A3, UGT1A4, UGT2B7, and UGT2B17). Additionally, the side effects of TKIs are categorized as hematological (thrombocytopenia, neutropenia, anemia, and cardiac dysfunction) and non-hematological (diarrhea, nausea, vomiting, pleural effusion, and skin rash). However, few toxicities are drug-specific, like degradation of biomolecules by ponatinib-glutathione (P-GSH) conjugates and clinical pancreatitis (dose-limited toxicity and manageable by dosage alterations) are related to ponatinib and asciminib, respectively. This review focuses on the pharmacokinetics of approved TKIs related to CML therapy to comprehend their specificity, tolerability, and off-target effects, which could help clinicians to make a patient-specific selection of CML drugs by considering concomitant diseases and risk factors to the patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic Myeloid Leukemia (CML) is a clonal, myeloproliferative disease that develops when the hemopoietic stem cell acquires the Philadelphia chromosome. This chromosome forms after the reciprocal translocation between chromosomes 9 and 22, i.e., t (9; 22). In this genetic translocation, the Abelson (Abl) gene on chromosome 9 gets translocated to the Breakpoint cluster region (Bcr) on chromosome 22, forming a fused oncogene (Bcr-Abl) on the truncated chromosome 22 (the Philadelphia Chromosome) [1]. This oncogene codes for BCR-ABL oncoprotein, which regulates several signaling pathways due to constitutively stimulation of ABL-related tyrosine kinase activity. Tyrosine kinases are mediators of various cell signaling pathways that cause physiological changes like cell proliferation, differentiation; and dysregulation in these tyrosine kinases results in cancer [2]. These kinases have an extracellular ligand-binding domain to which the corresponding ligand binds, which then induces dimerization and phosphorylation of the cytoplasmic domain of the kinase, and further regulation of several cytoplasmic signaling pathways occurs [3].
In the last decade, specific inhibitors against tyrosine kinases have been developed to control tumor progression, which proved quite effective with respect to other targeted therapies [3]. The TKIs are potentially competitive inhibitors for ATP-binding sites and inhibit the substrate-binding at the kinase domain, which prevents the phosphorylation of BCR-ABL oncoprotein [4]. Approximately 20 TKIs have been developed (Table 1), and only six of them (imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and asciminib) have been clinically approved in the case of CML [5]. Of all, imatinib was the effective drug, but because of T315I mutation and multidrug resistance (MDR), investigators began to explore new therapies, and in pursuit of that, other TKIs have been developed [6, 7]. Nevertheless, only ponatinib was found to be effective against the T315I mutation, but because of its more adverse effects on organs, it is of little use [7, 8].
In addition to these, a few more kinase inhibitors (radotinib, danusertib, and asciminib) got approval. Radotinib (IY5511HCl) is a structural analog of imatinib, primarily nilotinib, is gaining interest and is undergoing phase III studies to analyze their efficacy and safety in treating chronic phase CML patients [9, 10]. Danusertib (PHA-739358) is found to be a potent inhibitor of both Aurora kinase and BCR-ABL, and is in phase II clinical trials for the therapy of CML; and asciminib (ABL001) acts as a selective allosteric ABL1 inhibitor that recently received FDA approval [11, 12]. The search did not stop here, and yet, there is a clinical trial for a new novel inhibitor such as Bafetinib, Rebastinib, Tozasertib, Danusertib, HG-7–85-01, GNF-2, GNF-5, and 1,3,4-thiadiazole derivatives are ongoing [13,14,15,16,17]. It is anticipated that these novel inhibitory molecules may help to combat previously formed TKI resistance in leukemia.
Numerous studies reported alterations in the Bcr-Abl gene, mutations in BCR-ABL oncoprotein, and the manufacturing of novel TKIs, but there are little data on the comparative pharmacology of these TKIs. This review aims to elucidate the drug profiles of TKIs (imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and asciminib) related to CML, to understand their pharmacological differences that may be a reason for patient-wise selection of these TKIs.
Imatinib
Imatinib is a TKI approved in the United States after the failure of previously used treatments for CML patients with blast crisis, accelerated, or chronic phases [18]. In the late 1990s, biochemist Nicholas Linden developed imatinib at Novartis Pharmaceuticals, which then led to clinical trials of the drug. And after receiving approval from the US FDA in May 2001, the drug was used at the Dana-Farber Institute to treat CML [4]. Imatinib is a derivative of 2-phenyl amino pyrimidine that is specific only against certain tyrosine kinases. The structural analysis revealed that imatinib binds to BCR-ABL near the ATP-binding site leading to the conformational change at the ABL active site motif Asp-Phe-Gly (DFG), constraining BCR-ABL kinase activity, and finally reduces cell proliferation [19]. Imatinib is selective for the Bcr-Abl gene but is also effective against other tyrosine kinases such as cytokine receptor (c-kit), expressible in GIST; and platelet-derived growth factor (PDGF) receptor [20, 21]. It is not that imatinib only acts on cancer cells, while it also inhibits the Abl1 gene in the normal cells. But the normal cells continue proliferation due to additional tyrosine kinases. Since tumor cells are completely dependent on the Bcr-Abl kinase protein, cancers expressing the Bcr-Abl oncogene can be treated by imatinib [22]. Despite inhibition by imatinib, the BCR-ABL protein enters the nucleus but is unable to perform any of its regular roles, such as the anti-apoptotic function, and eventually causes tumor cell death [23].
Transport
After oral intake, imatinib gets quickly absorbed from the gut due to its rapid dissolution at acidic pH [24]. Two primary sites of imatinib absorption through the influx transporters are the enterocytes of the intestine and hepatocytes of the liver. These transporters regulate inflow through electrochemical gradients of transport substrates to ions across a membrane. In imatinib uptake, mainly the organic cation transporter 1 (OCT1 or the SLC22A1 gene product) and to a minor extent, organic anion transporting polypeptide 1A2 (OATP1A2, the SLCO1A2 gene product), situated at the apical membrane of enterocytes, play the lead role [25, 26]. Additionally, the solute carriers OATP1B3 (SLCO1B3 gene product) and OCTN2 (SLC22A5 gene product), expressed on the basolateral membrane of hepatocytes, promote hepatic drug absorption [25]. Another influx of imatinib is the transporter ABCC4, expressed on the basolateral membrane of hepatocytes and supports systemic imatinib uptake (flow of imatinib from the liver into the systemic circulation) [25].
If the drug has entered, it has to exit the cell also, and here comes the role of efflux transporters. The efflux transporters related to imatinib are the ATP-binding cassette (ABC) transporters such as the ABCB1 (formerly known as P-glycoprotein or MDR1) [27,28,29] and ABCG2 (formerly known as breast cancer resistance protein, BCRP) [29, 30]. These transporters cause drug excretion through ATP hydrolysis and subsequent phosphorylation of the transporters as energy sources, leading to active transport across multiple cell membranes [31]. Both ABCB1 and ABCG2 are found to be expressed in several tissues, including the liver (at the sinusoidal basolateral membrane, as well as the apical bile canalicular membrane of hepatocytes, intestine, placenta, kidney, and the blood–brain barrier [32,33,34,35]. Compared to influx transporters, these efflux transporters have been studied and examined more due to their role in MDR. Furthermore, the absolute availability of imatinib depends on the balance between influx and efflux transporters over the intestinal barrier, preferring the active drug uptake.
Metabolism
The recommended dose of imatinib is 400 mg/day in CML and GIST patients, and 600 mg/day in the accelerated phase or blast crisis of CML [36]. The dosage has to be taken once a day in combination with a meal and water. Differences between imatinib-related pharmacokinetics across individuals are due to interpatient variability in the expression of drug transporters [34].
Imatinib is an orally administered drug with a mean absolute systemic availability of 98% [37]. After 2–4 h of imatinib administration, it becomes available in plasma, where this drug is bound to plasma proteins, primarily albumin and α1-acid glycoproteins [24, 38]. This drug is actively cleared from the blood to the liver, the site of metabolism. Imatinib is metabolized through cytochrome P450 (CYP450) isoforms CYP3A4 and CYP3A5; and then after analyzing the metabolite patterns in plasma, urine, and feces, N-desmethyl imatinib (CGP74588) found to be the most active metabolite [39, 40]. CYP3A4 and CYP3A5 are responsible for most of the biotransformation of imatinib and, to a lesser extent, the CYP1A1/2, 1B1, 2C8/9, 2C19, and 2D6 enzymes as well [24, 41, 42]. In the plasma, apart from imatinib and CGP74588, few other metabolites whose structure could be partially determined by LC–MS. were also found, and those were categorized as N-oxide-, deaminated-, hydroxy-, and glucuroconjugate metabolites [43] (Fig. 1).

Imatinib metabolic pathway (https://www.pharmgkb.org/pathway/PA164713427)
Gschwind et al. studied the imatinib metabolism in detail and reported that metabolism occurs in two phases [40]. The phase I metabolic pathway includes the metabolites pyridine N-oxidation (CGP72383), benzylic hydroxylation (AFN911), N-demethylation (CGP7458, M20.0a, M25.6, M28.8, and APG049), piperazine-N-4 oxidation (CGP71422), and piperazine ring oxidation with lactam formation (APG049, APG050, M23.7, M25.6, M27.6, M28.8, and M29.6) (Fig. 2). In the phase II metabolism, the conjugation of imatinib and CGP74588 with glucuronic acids (M21.0 and M20.0a, respectively) occurs, and glucuronic acid gets oxidized to carboxylic acid (M42.2). It is estimated that an average of 75% of imatinib doses undergo biotransformation. Excretion occurs more either through bile (20% as parent compounds and 68% as metabolites) or renal excretion (5% of the parent compound and 13% of the metabolites) [36].

Imatinib, along with the different metabolites that formed after metabolism in humans. The main metabolite is CGP74588, which formed through the N-demethylation metabolic pathway [38]
Toxicity
Imatinib is usually well tolerated, with insignificant common side effects, such as nausea and vomiting, diarrhea, muscle cramps, fatigue, skin rash, and edema. In a study, the GIST and CML patients showed fewer side effects such as nausea, emesis, distressingly demonstrated fatigue, and minor hemorrhage [44]. This drug-induced subsequent hepatotoxicity in a female patient treated with CML-related therapies, i.e., hydroxyurea, INF-α, and imatinib, concurrently [45]. Following histological examination of this patient, some findings were found, such as fold necrosis of hepatocytes and slight infiltration of lymphocytes around the necrosis lesions and on the sinusoids of the liver, similar to acute viral hepatitis [45]. Apart from CML, acute liver failure was obtained in GIST related case study after ten weeks of imatinib treatment [46]. Liver biopsy confirmed hepatotoxicity by revealing sinusoidal congestion, inflammation, necrosis of hepatocytes, and hepatocytes drop-out around hepatic venules [46]. Besides this, imatinib is also associated with water retention and edema, and as a result, some high protein content in blood exhibits hepatotoxicity [47]. One study first time reported, three cases of splenic rupture as a side effect of imatinib treatment; two of these three were CML patients and one patient with myeloid metaplasia [48]. All the patients had been treated with a dose of 600 mg/day of imatinib with an average duration of more than one week. Computed tomography (CT) revealed that there was a solitary splenic rupture in the CML patients, whereas drug-induced thrombocytosis and splenic rupture were observed in myeloid metaplasia patients [48].
As previously mentioned, imatinib affects c-Kit and PDGFR tyrosine kinases. And both kinases play a major role in regulating testicular organogenesis, Leydig cell differentiation, and luteinizing hormone receptors, so it was tested whether this drug has any side effects on the male reproductive system [49,50,51]. Prasad et al. demonstrated that imatinib significantly affects testosterone and LDH levels, but the effect is reversible once the drug is withdrawn [51]. The c-kit tyrosine kinase is also located in melanocytes and plays a role in melanogenesis and pigmentation [52, 53]. So, it is believed that due to this kinase, imatinib also exhibited dermatological side effects by inducing hyperpigmentation after six months of therapy in one patient, which developed into a chloasma-like appearance after one year of therapy [54]. So far, several side effects were observed in patients, but imatinib-induced pneumonitis was unnoticed. One case study reported that a patient associated with a chronic myeloid neoplasm underwent one month of imatinib treatment, and after that, was diagnosed with shortness of breath and productive cough [55]. CT revealed bilateral pulmonary interstitial syndrome, which resolved after systemic corticosteroid therapy, but the same symptoms recurred upon resumption of imatinib therapy [55].
Nilotinib
Despite its high efficacy, in about 20% of patients, imatinib proved ineffective due to mutation, MDR, and side effects [56]. So, in the quest for better therapy, the second generation TKIs were developed, and in that row, nilotinib ranks first. Like imatinib, nilotinib is also an orally taken drug with 30-fold more potent and selective for BCR-ABL in comparison to imatinib [57]. Nilotinib is an analog of imatinib, a phenyl amino pyrimidine derivative in which the alignment of the amide is reversed, and the methylpiperazine is substituted with a trifluoromethyl and a methyl-imidazole, discovered by re-engineering imatinib, using medicinal chemistry and structural biology approaches to improve selectivity toward BCR-ABL finally efficacy [58]. FDA-approved this drug in 2007 for CML patients of chronic and accelerated phases and imatinib-resistant patients [59].
Preliminary studies proved good efficacy and tolerability of nilotinib when administered twice a day at a dose of 400 mg and having a half-life of 15–24 h in plasma [59]. Nilotinib is also influential in treating edema, which occurred due to inhibition of PDGFR in the case of imatinib therapy. The dose of nilotinib (400 mg twice daily) increases the bioavailability of this drug so that its accumulation cannot inhibit this receptor tyrosine kinase, and a rare occurrence of edema occurred [58].
Transport
Cellular transportation of nilotinib is different from imatinib [60]. As mentioned above, OCT1 is a transporter of the cationic drug imatinib due to the presence of the basic N-methylpiperazine group at physiological pH in this specific drug. Since this group is absent in nilotinib, OCT1 does not support this drug uptake. Therefore, the uptake of nilotinib is primarily passive, resulting in an advantage of nilotinib over imatinib in diseases caused by c-Kit and PDGFR [26]. In addition, nilotinib efficiency is less likely influenced through transporters due to its high hydrophobic nature than imatinib [61]. Furthermore, because nilotinib and imatinib have different transport pumps, this results in the stability of the drug intracellularly and proves beneficial in imatinib-resistant patients [62].
Like imatinib, the prime efflux transporters of nilotinib are ABCB1 and ABCG2. A study has shown that ABCB1 inhibits nilotinib-mediated kinase at high concentrations, but such a role is not played by ABCG2 [63]. This indicates that nilotinib is predominantly transported via ABCB1 and has no strong interaction with ABCG2. For the first time through TaqMan transporter array technology, Eddie et al. reported that increased concentration of nilotinib (up to 2 μM) in K562 cells leads to a 57-fold higher mRNA expression of ABCC6 than in control cells [64]. Nilotinib resistance in patients can be overcome by increasing the concentration of this drug or by using a pump inhibitor [61, 65].
Metabolism
Like imatinib, nilotinib is also an orally administered drug, but despite their structural similarity, the pharmacokinetics of both drugs is different. The bioavailability of nilotinib is only 30%, which increases to 50% after consumption with a meal containing fat due to the hydrophobic nature of this specific drug [19]. Nilotinib is tightly (~ 99%) bound to plasma proteins and transported to the liver, where CYP3A4 metabolizes it through oxidation and hydroxylation pathways to form nilotinib carboxylic acid and nilotinib N-oxide [66]. Nilotinib also regulates the hepatic enzymes (CYP3A4, CYP2C8, CYP2C9, CYP2D6, and UGT1A1) through a feedback mechanism (Fig. 3).

Nilotinib metabolic pathway (https://www.pharmgkb.org/pathway/PA166178331)
Toxicity
The in vivo and in vitro studies reported the significant toxicological effect of this drug on different organs such as the liver, bile duct, and gall bladder, while mild toxicity was observed in the spleen, heart, pancreas, and thyroid [67]. The most significant toxicity related to nilotinib is the inhibition of hERG (a gene that codes for a protein known as Kv11.1, the alpha subunit of a potassium ion channel) that regulates electric current across the heart [19]. Due to cardiac problems with nilotinib, several death events were reported, and these reports suggested that this may be due to ventricular re-polarization abnormalities. Furthermore, elevated hepatic enzymes were observed in ~ 10–15% of patients who rarely progressed to hepatitis [67].
Dasatinib
Dasatinib is an ATP-competitive TKI like imatinib and nilotinib, but it acts more potently than the two. Dasatinib received FDA approval in 2006 to treat chronic-accelerated- or myeloid or lymphoid blast phase of CML, and Ph+ ALL, which are resistant to previous treatments [68]. Like others, this drug is also given orally but is structurally different from imatinib, and as a result, dasatinib bounds to those BCR-ABL conformations to which imatinib does not bind [69, 70]. The recommended starting dose of dasatinib in chronic phase CML patients is 100 mg orally once daily, compared to 140 mg once daily in accelerated phase, myeloid blast phase, and lymphoid blast phase CML or Ph+ ALL [71, 72].
The main targets of dasatinib are BCR-ABL, Src, c-kit, ephrin receptors, and other tyrosine kinases [73]. Dasatinib binds strongly to the BCR-ABL kinase, which, despite a plasma life of 3–5 h, proved to be a more potent and longer effective drug than other previous CML treatments, such as imatinib and nilotinib [73, 74]. Furthermore, a BCR-ABL related in vitro study reported that dasatinib (IC50: 0.8 nmol/L) is»325-fold and»16-fold more potent than imatinib (IC50: 260 nmol/L) and nilotinib (IC50: 13 nmol/L), respectively [75]. One reason behind this high potency may be that unlike imatinib, which only binds to the inactive conformation of BCR-Abl, dasatinib is known to bind to both the active and inactive conformations of this kinase enzyme. So, it is believed that due to this difference, dasatinib is effective against imatinib-resistant BCR-ABL mutations (but not in the case of T315I mutation), which have disrupted the inactive conformation [69, 70, 76].
Transport
The absorption of dasatinib is mainly a passive process in contrast to the active transportation of imatinib. A study illustrated that the organic cation transporters (OCT1, OCT-2, and OCT-3) have no role in dasatinib cellular uptake, but this drug is a substrate of the efflux transporters (ABCB1 and ABCG2) in leukemic cells [77]. In addition to the above two transporters, dasatinib is also a substrate of the ABCC4 (MDR4) transporter located in the stomach and gastrointestinal tract, which facilitates gastric absorption of the respective drug [78]. Furthermore, the studies reported that the absorption of dasatinib is dependent on the acidic pH as its absorption ranges from 18.4 mg/mL at pH 2.6 to only 0.008 mg/mL at pH 6.0 [79]. Therefore, the stomach plays a vital role in the absorption of dasatinib due to its acidic pH, as the pH rises to 6 in the duodenum and then gradually to 7.4 in the terminal ileum; and as a consequence of this, the absorption mainly occurs in the upper segment of the intestinal tract [78, 80].
The first time the dasatinib resistance role of ABCC6 was evaluated by experimenting with the effect of ABCC6 inhibitors (pantoprazole, indomethacin, and probenecid) on the efficacy of dasatinib and imatinib [28]. The study demonstrated that the inhibitors reduce the IC50 of dasatinib but not of imatinib, representing that inhibition of ABCC6 enhanced the efficacy of dasatinib by reducing its efflux through ABCC6 and increasing intracellular drug concentration. So, dasatinib transport depends on the bioavailability of ABC transporters, regardless of OCTs' existence.
Metabolism
Dasatinib is rapidly absorbed orally, with peak plasma concentration (Cmax) within 0.5–3 h after administration [71]. Unlike nilotinib, dasatinib administration is not based on the type of food; this drug is highly plasma protein bound (96%) and widely distributed in the extravascular space [81].
In the liver, CYP3A4 enzymes primarily metabolize dasatinib with the help of Flavin-containing monooxygenase 3 (FMO3) and Uridine 5'-diphospho-glucuronosyltransferase (UGT), and 30% of the drug remains unchanged. The different metabolites formed after biotransformation of dasatinib have been identified through in vitro incubation of 14C. The metabolites are found to be developed through either primary metabolic pathway (M4, M5, M6, M9, M20, and M24) or multiple metabolic pathways (M3a/b, M7, M21, M23a/b, M28a/b, M29a/b/c, and M30) in the liver microsomes and hepatocytes [82]. Some metabolites (M3a/b, M23a/b, M28a/b, and M29a/b/c) are pairs of positional isomers that have not been sufficiently resolved from each other in chromatography. The M4, M5, and M6 metabolites are categorized as N-dealkylated Dasatinib (deshydroxyethyl), piperazine N-oxide, and carboxylic acid. Out of these three, M4 is equipotent to dasatinib, while the other two (M5 and M6) are tenfold less active. The metabolites M3a/b are found to be positional isomers of the 2-chloro-6-methylphenyl ring-hydroxylated derivatives of the N-oxide of dasatinib. M7 is the N-oxide of the carboxylic acid metabolite, and metabolite M9 is the metabolite formed with the initial metabolism of the 2-chloro-6-methyl carboxamide moiety, followed by the formation of a new 6-membered ring. In the same study, M20 was confirmed as the 4-hydroxy-2-chloro-6-methylphenyl metabolite of dasatinib, and M21 as the sulfate conjugate of M20. The metabolites M23a/b are identified as the positional isomer of the 2-chloro-6-methylphenyl ring-hydroxylated derivative of the carboxylic acid metabolite, and M28a/b as the positional isomer of the 2-chloro-6-methylphenyl ring-hydroxylated M4. The metabolites M24 and M30 were confirmed as benzyl alcohol derivatives of dasatinib and sulfate conjugates of 2-chloro-6-methylphenyl ring-hydroxylated M6, respectively. The oxidative metabolites M20 and M24 are abundant in liver microsome and hepatocyte incubations, and the plasma prominent metabolite M21 is also a major metabolite of the hepatocyte incubations [82]. The isomers of M29, i.e., M29a/b/c, were identified as the positional isomer of dehydroxylated dasatinib, both hydroxylations occurring on the 2-chloro-6-methylphenyl ring. The primary route of dasatinib clearance is oxidative biotransformation through which circulating metabolites are formed. These metabolites include products of hydroxylation, alcohol oxidation, N-oxidation, N-dealkylation, sulfate, and glucuronide conjugation, and secondary metabolites that are byproducts of primary metabolites (Fig. 4).

Dasatinib metabolic pathway (https://www.pharmgkb.org/pathway/PA166164906)
Dasatinib acts as both an inhibitor and inducer of CYP3A4 depending on its concentration; also, the metabolism of the respective drug is affected by concomitant drugs metabolized by CYP3A4. Following co-administration of dasatinib with inhibitors of CYP3A4 (e.g., erythromycin, clarithromycin, itraconazole, ketoconazole), the systemic exposure of this TKI increased by 4- to fivefold; and when the same drug was co-administered with CYP3A4 inducers (e.g., phenytoin, rifampicin, dexamethasone, carbamazepine, or phenobarbital), the systemic exposure of dasatinib reduced by ~ 80% [81, 82]. The elimination of this drug mainly occurs in the feces (85%) and is minor in urine (4%). The 19% of dosage of dasatinib was recovered as an unchanged form in feces and the remaining percentage as the different metabolites of dasatinib [83].
Toxicity
Despite its high potency, this drug showed adverse effects in a few patients. These effects may be of mild to moderate severity, usually non-hematological adverse events (incidence of 12–29%) being fluid retention events (including superficial edema or pleural effusion), adverse gastrointestinal events (including diarrhea and nausea), skin rash, hemorrhage, dyspnea, headache, musculoskeletal pain, pyrexia, and fatigue [71]. The severe hematological adverse event comprises thrombocytopenia, in which few patients suffer from CNS hemorrhage, and others from gastrointestinal hemorrhage [81].
The broad term fluid retention event leads to pulmonary hypertension (PH) and congestive heart failure/ cardiac dysfunction, which means this drug directly and specifically affects the pulmonary and blood vessels [83]. In addition, some patients suffer from hepatotoxicity due to the induction of oxidative stress. This was confirmed after a clinical trial of the drug in rat primary hepatocytes, where dasatinib increased the level of reactive oxygen species (ROS), reduced glutathione in the cell, reduced activity of superoxide dismutase (SOD), declined membrane potential of mitochondria, and eventually enhanced other events to promote oxidative stress [83].
Bosutinib
Bosutinib, a substituted 4-anilino-3- quinoline carbonitrile, is an orally available kinase inhibitor that acts against the Src and Abl kinases and explicitly inhibits the Bcr-Abl oncoprotein. Even at a low dose, bosutinib proved more effective than imatinib and overcame most imatinib-resistant BCR-ABL mutations (D276G, Y253F, and E255K; except T315I) [84]. This drug received its first approval in 2012 for CML therapy in combination with prior TKIs (imatinib, nilotinib, and dasatinib); and later approved as a first-line treatment for newly diagnosed chronic phase CML patients in the United States and the European Union in 2017 and 2018, respectively [37]. The clinically approved dosages of bosutinib are 400 mg once daily (QD) for newly diagnosed chronic phase Ph+ CML patients and 500 mg QD for chronic Phase, accelerated phase, or blast phase Ph+ CML patients resistant to prior therapies [85]. Due to its long half-life (average mean half-life varies from 32.4 to 41.2 h), the prescribed once daily regimen is sufficient for bosutinib [58].
Transport
It was previously thought that the transporters ABCB1 and ABCG2 did not exert a noticeable protective effect in bosutinib-associated cellular toxicity assays, which confirmed no role of these transporters in efflux and resistance to this drug. A study evaluated the similar phosphorylated Bcr-Abl pattern in bosutinib-treated K562, K562/ABCB1 (overexpressing ABCB1), and K562/ABCG2 (overexpressing ABCG2), which further verified that this TKI proved to be a potent anticancer drug by overcoming MDR caused by ABCB1 and ABCG2 transporters [86].
But later, another study noticed the vital role of ABCB1 as an efflux transporter for bosutinib and claimed that the data could help determine appropriate treatment options for bosutinib-resistant patients. In this in vitro and in vivo study, the interaction of bosutinib with three transporters (ABCB1, ABCG2, and SLC22A1) was analyzed; and subsequent drug and transporter interactions were assessed with transporter inhibitors (verapamil, ABCB1 inhibitor; fumitremorgin C, ABCG2 inhibitor; amantadine, SLC22A1 inhibitor) [87]. The results demonstrated an increased and decreased bosutinib concentration according to the low and high levels of ABCB1, but no such effect was obtained in the case of the remaining two transporters. And in line with this finding, the IC50 value of bosutinib increased in ABCB1-overexpressing cells which decreased after verapamil treatment only in ABCB1-overexpressing cells, not in the wild-type cells. The inhibitors of ABCG2 and SLC22A1 did not show any significant difference in the drug concentration, so it is clear that only ABCB1 is responsible for the bosutinib-related MDR [87].
Metabolism
Bosutinib is a highly permeable and less soluble drug, and because of this characteristic, it is prescribed to be taken with food as the tolerability and risk of bosutinib increases with combined intake. This TKI is widely distributed, proved because of highly binding to human plasma proteins in vitro (94%) and ex vivo in healthy subjects (96%); and bosutinib binding is independent of its concentration [88]. Like other TKIs, the metabolism of bosutinib is regulated by CYP3A4, and this was investigated through the use of an inhibitor (ketoconazole) and inducer (rifampin) of CYP3A4. The result demonstrated the same as the inducer reduced plasma concentration and increased drug clearance, and the inhibitor did the opposite [89]. Other reports also add to this investigation by demonstrating that bosutinib's co-administration with ketoconazole decreases the mean apparent clearance of this drug by ninefold and increases half-life from 46.2 to 69.0 h [58, 88].
After CYP3A4 activity, two primary bosutinib-related metabolites, i.e., oxidized bosutinib (M2) and N-desmethyl bosutinib (M5) were found to circulate, and both were considered to be fewer active metabolites as they contribute ≤ 5% to bosutinib activity [90, 91] (Fig. 5). One study reported a rapid and complete (94.6%) metabolism of bosutinib following a dose of 500 mg (a mixture of radiolabeled and unlabeled bosutinib) drug in six male patients and also confirmed that the majority of drug excreted through feces (91.3%) and minorly through urine [92]. Subsequently, it was also found that bosutinib and M5 are the major drug-related components in feces, while bosutinib and M2 are in the urine.

Bosutinib metabolic pathway (https://www.pharmgkb.org/pathway/PA166178011)
Toxicity
The adverse effects of bosutinib are manageable and categorized as hematological and non-hematological toxicities. The hematological toxicities include thrombocytopenia, neutropenia, and anemia, which all upsurges after prior first-, second-, and third-line bosutinib treatment of CML [93,94,95]. Neutropenia adversity was less in bosutinib treatment than in imatinib (11% vs. 24%, respectively), but thrombocytopenia and anemia frequencies were similar in both TKI treatments. Most persistent non-hematological toxicities related to bosutinib include diarrhea, nausea, vomiting, rashes, abdominal pain, pyrexia, headache, constipation, and cough. Of all these, diarrhea is the major toxicity due to its abundance in 84% of patients, which can be controlled through interruption or reduction of drug dosage [94, 96]. Arthralgia, myalgia, muscle cramps, bone pain, and peripheral or periorbital edema were observed less frequently in bosutinib-treated patients than in imatinib-treated patients [96].
Apart from these minor, non-hematological toxicities, other bosutinib-related adverse events are heart failure, hypertension, and pleural effusion. In an investigation, 0.8% of 248 patients taking bosutinib as first-line therapy and 4.4% of 570 patients taking bosutinib as second, third, or fourth-line therapy for CML or advanced stages of leukemia were found to be suffering from heart failure [93]. The same study evaluated that 7.8% of 818 patients who were receiving bosutinib treatment for CML or ALL developed hypertension-related adverse events; relatively, they had no record of any such disease in the past [93]. A report stated that 4% of 248 patients were diagnosed with pleural effusion after receiving first-line bosutinib therapy [97].
Ponatinib
Ponatinib is the orally available pan-BCR-ABL TKI developed by ARIAD Pharmaceuticals through a computational and structure-based approach [98]. It is the only FDA-approved TKI for T315I-positive Ph+ ALL and T315I-positive CML (at any stage); and also, for leukemic patients who have not taken any TKIs other than ponatinib [99, 100]. This TKI is effective against the T315I mutation due to the presence of a novel triple bond ethynyl linker in it, through which ponatinib overcomes the steric hindrance that arises after replacement of threonine with isoleucine on the 315 (T315I) position of mutant BCR-ABL oncoprotein [98]. This linker helps ponatinib to span the bulky isoleucine side chain present in the T315I mutant BCR-ABL protein, which the prior TKIs could not execute. A structure–activity-based study has shown that triple bonds give ten times higher potency than single or double bond systems, and the data from this study provide another reason for ponatinib to be the most efficient TKI [101].
Transport
The interaction of Ponatinib with drug transporters is poorly explored, and in that also there are little data on drug interactions with influx transporters compared with efflux transporters. The most studied efflux transporters in ponatinib are ABCB1, ABCC10, and ABCG2 transporter, which induce MDR by extruding anticancer compounds from the cell. Ponatinib was shown to be an inhibitor of ABCB1 and ABCG2, as it hinders the efflux of chemotherapeutic drugs by these transporters and, in addition, increases the intake of those drugs also [24]. Two surveys after analyzing IC50ponatinib (concentration of drug required to inhibit a biological process by half) in K562 cells and variants: ABCB1-overexpressing K562-DOX and ABCG2 overexpressing K562-ABCG2, revealed that, unlike imatinib, nilotinib and dasatinib, ponatinib is not exported via ABCB1 and ABCG2 [102, 103]. Besides efflux transporters, Lu et al. also scrutinized no role of OCT1, the import transporter, in the transport of ponatinib in target BCR-ABL positive leukemic cells [103]. Conversely, in regions where ABCB1 and ABCG2 are highly accumulated, this TKI becomes ineffective. This condition was observed in brain tumors, where ponatinib fails to enhance anticancer drug sensitivity due to its inability to cross the blood–brain barrier, a locus where efflux transporters (ABCB1 and ABCG2) accumulate in high proportions [104].
Although ABCC10 (also known as MRP7) has not been heavily investigated compared to ABCB1 and ABCG2, some in vitro and in vivo studies revealed its activity as the efflux transporter for anticancer drugs, e.g., taxanes [105, 106]. Some previous experiments proved that ponatinib alone or in combination with chemotherapeutic drugs might prove to be a potent reversal drug for MDR therapy. And in that aspect, one study reported for the first time that ponatinib induced intracellular accumulation of the chemotherapeutic drug [3H]-paclitaxel by inhibiting the MRP7 function and protein expression at a clinically achievable concentration, and thus attenuated the MRP7-mediated MDR [107]. Consequently, it became known through several studies that ponatinib can be passively transported into cells, and the likelihood of MDR due to major ATP efflux transporters (ABCB1 or ABCG2) in patients administered ponatinib is very low or negligible.
Metabolism
The prescribed dose of ponatinib is 45 mg daily, confirmed after phase 1 and phase 2 trials in CML and Ph+ ALL patients [108, 109]. Instead, the US FDA recommended a dosage of 30 mg in patients with hepatic impairment, whereas the dosage of ponatinib had to be given with caution in patients with impaired kidney function, and the use of ponatinib during pregnancy and lactation has been banned [108]. 92% of the dose was recovered after drug administration, with 86.6% being recovered in feces and 5.4% in urine. This drug is readily absorbed with a steady-state maximum plasma concentration (Cmax) of 145 nM at 4–8 h and a mean terminal elimination half-life (t1/2) ~ 22 h [109].
Ponatinib is metabolized primarily by CYP3A4 and to a lesser extent by CYP3A5, CYP2C8, and CYP2D6; to N-oxide and N-desmethyl metabolites (Fig. 6) [108, 110]. N-desmethyl metabolite is fourfold less potent than ponatinib [108]. The effect of CYP3A4 on the metabolism of ponatinib has been investigated following co-administration of ponatinib and ketoconazole (CYP3A4 inhibitor), in which it was confirmed that inhibition of CYP3A4 increases plasma concentration (Cmax) and area under the concentration–time curve (AUC) [111]. Along with CYP3A4, CYP1A1 also metabolizes ponatinib, and it biotransforms the parent drug into monohydroxylated, and di-hydroxylated products [108].
Yihua et al. studied detail about the metabolite profiling of radioactive [14C] ponatinib after administering a single dose of 45 mg in six male volunteers [112] (Fig. 6). In this study, through radio-chromatographic profiling and mass spectral analysis, ponatinib and its amide hydrolysis acid metabolite (M14) were two abundant metabolites of plasma. In addition to these two metabolites, some other ponatinib metabolites evaluated were M14 glucuronide (M15), despiperazinyl acid (M23), hydroxyponatinib glucuronide (M24), ponatinib glucuronide (M29), ponatinib N-oxide (M36), and N-desmethyl ponatinib (M42); and they all accounted for 3.4, 7.0, 2.1, 6.0, 0.5, and 0.5% of the plasma radioactivity, respectively. The same study reported the metabolite profile of urine and detected a trace level of ponatinib. The major metabolites of urine were M14 and M15, and these two, together with M16, accounted for 53.5% of the total urinary radioactivity. Within 35–41 min after dosing, a group of metabolites (M25, M29, M30, M31, M32, M33, M34, M35, M36, M38, M39, M41, and other co-eluting metabolites) is excreted in the urine, that wholly accounts for 14.0% of the urine radioactivity. During fecal metabolite profiling, 23.7% of radioactive ponatinib was quantified; and hydroxyponatinib (M31) and M42 were categorized as the main metabolites because of their 20.4 and 9.6% radioactivity, respectively. Metabolite peaks not well distinguished in chromatography formed one cluster, the M23 cluster, which contributed 17.2% of the fecal radioactivity. Further metabolites, M32, M33, M35, M36, M38, M39, and M41, were assessed in feces, which contributed 2.1% of the total fecal radioactivity [112]. In feces, no M14-derived metabolites were found. After a single oral dose, ponatinib gets eliminated through multiple pathways, i.e., hydroxylation (18%), N-demethylation (8.3%), methylation (8.4%), and amide bond hydrolysis (4.4%) (Fig. 7) [112, 113].

Ponatinib metabolic pathway (https://www.pharmgkb.org/pathway/PA166178200)
Toxicity
As mentioned above, CYP1A1 regulates ponatinib metabolism by forming mono- and di-hydroxylated ponatinib metabolites; and with the addition of glutathione (GSH), these hydroxylated metabolites get reduced into electrophilic intermediates, i.e., P-GSH conjugates/epoxides. These epoxides are reactive and contribute to adverse effects related to ponatinib by binding and mutating both protein and DNA. This was further confirmed by comparing the ponatinib metabolism in wild type and treated (treated with CYP1A1 inducers: 2,3,7,8-tetrachlorodibenzodioxin or 3-methylcholanthrene) mice, where the results reassured the role of CYP1A1 by showing the presence of P-GSH conjugates only in the feces of treated mice [108]. So, this ensured that despite the normal metabolism of ponatinib by CYP1A1, this enzyme also regulates the formation of electrophilic intermediates that may boost ponatinib toxicity.

Ponatinib and different metabolites (M) with their metabolite profile formed after biotransformation through multiple pathways. CYP3A4-regulated pathways are Hydroxylation and N-demethylation [112]
Previously ponatinib-related toxicities were manageable such as rash, dry skin, headache, abdominal pain, and constipation, which were found in approximately 40% of ponatinib-treated CML patients [109]. But after that, major adverse events had been reported during clinical trials, which occurred in two phases. In the phase I study, no thrombotic events were initially observed, whereas an 8% incidence of severe arterial thrombotic events was observed in the phase II trial [99, 108]. Subsequent additional follow-up of these drug trials uncovered a higher frequency of serious adverse vascular events (48% and 24% in phase I and II trials, respectively) [114]. This led the FDA and ARIAD Pharmaceuticals to withdraw ponatinib from the market in October 2013 rapidly. This withdrawal caused problems for patients who were responding exclusively to this drug alone. With those specific patients in mind, providers then launched single-patient investigational new drug (IND) applications; and between November 2013 and January 2014, more than 370 patients were administered with single-patient INDs [114]. Given this situation, the FDA again allowed ponatinib to be re-marketed in January 2014, but only to patients to whom no other TKI is prescribed. One way to avoid adverse events is to use low doses of ponatinib in combination with other therapeutic agents, resulting in reduced resistance in cells, leading to long-term effects [115].
Asciminib
The target site of the five previously discussed and accepted TKIs is the ATP-binding site of BCR-ABL, and mutations in that region result in clinical resistance against those drugs. Considering drug resistance and intolerable toxicities (vascular and pulmonary) of past TKIs, asciminib was studied continuously for the past five years and recently received FDA approval (29th October 2021) for the treatment of chronic phase Ph+ CML patients with the T315I mutation [116,117,118]. Asciminib, a first-in-class STAMP (Specifically Targeting the ABL Myristoyl Pocket) inhibitor, specifically and potently inhibits BCR-ABL1 by binding to a pocket different from the ATP-binding site of the kinase [119]. Several investigations are underway on asciminib to know its post-approval pharmacology.
Asciminib is an orally bioavailable potent and specific BCR-ABL inhibitor that differs from other TKIs in that it binds to the myristoyl pocket, and through this asciminib targets both native and mutated BCR-ABL1 oncoprotein even after T315I mutation. The myristoyl pocket is usually occupied by the myristoylated N-terminal of ABL1, which causes autoinhibition by locking the ABL1 kinase in the inactive state, but in CML after the formation of BCR–ABL oncoprotein, this motif is lost, and then ABL1 kinase always remains in the active state [117]. So, the allosteric binding of aciminib to the myristoyl site restores the inactive state of ABL1 and inhibits the kinase activity of the BCR-ABL oncoprotein (Fig. 8). Despite all conformations of the myristoyl pocket, this drug is specific only for the ABL1 kinase motif of this pocket, and asciminib has a low range of activity toward all clinically observed ATP mutants, including T315I [10, 120]. Since the myristoyl pocket is rarely available in other kinases, asciminib proved highly selective for BCR/ABL1 and clinically significant for CML patients in whom many of the approved TKIs had failed.

Mode of action of asciminib (A Autoinhibition of ABL1 kinase by binding of the myristoylated N-terminal; B Loss of myristoylated N-terminal due to formation of BCR-ABL oncoprotein; C Allosteric binding of asciminib at the myristoyl site restores autoinhibition) [117]
Transport
Several studies have revealed the role of ABC transporters (mainly drug efflux transporters ABCB1 and ABCG2) in TKI therapy, but there is still little study in the aspect of asciminib. During the evaluation of the association between asciminib resistance and the transporter (ABCB1 and ABCG2) in three cell types: K562-Dox (ABCB1-overexpressing via doxorubicin exposure), the naive BCR-ABL1+ cell line K562 (negligible ABCB1/ABCG2 expression), and K562-ABCG2 (ABCG2 overexpression via transduction), asciminib efflux by both the ABCB1 and ABCG2 transporters were demonstrated [121]. This is further confirmed as the same study showed increased Lethal Dose (LD50asciminib) in K562-Dox and K562-ABCG2 cells contrasted with K562 control cells; and again, sensitivity is wholly restored with cyclosporine and Ko143, the inhibitors of ABCB1 and ABCG2, respectively [122].
Metabolism
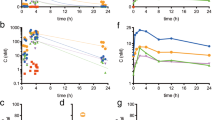
After the failure of previous ABL kinase inhibitors, one group conducted a phase I trial of aciminib (dose 10 mg- 200 mg) for 14 months in 150 CML patients (141 patients in chronic phase and 9 in accelerated phase) who had unacceptable side effects or were resistant from prior TKIs [117]. After 12 months of follow-up, the study found a major molecular response achieved in patients with resistance or toxicity to ponatinib and those with a T315I mutation. At various doses, 40 mg twice daily and 80 mg once improved preclinical 90% inhibitory concentration against phosphorylated signal transducer and activator of transcription 5 (pSTAT5); and a dose of 40 mg twice daily was found to be above the preclinical 90% inhibitory concentration for pSTAT5 inhibition in 100% of patients without a T315I mutation [117]. Similarly, another scientific group used aciminib first time for realistic clinical practice against CML patients after allowance by Novartis under a managed access program (MAP) to investigate the efficacy and safety of this drug [123]. The difference between the two studies is that patients in the current study did not receive any alternative TKI therapy, whereas patients in the former study (phase I trial) received asciminib after the failure of at least two TKIs, and the subsequent study found no dose discontinuation, but both studies revealed hematological or pancreatitis toxicities related to the drug.
The pharmacokinetic profile of aciminib (Table 2) showed a half-life between 0.5 and 4 h, and also that the absorption of the drug is completely dependent on its bioavailability [120]. After absorption asciminib is distributed in all tissues with little penetration into the reproductive system except the CNS. After administration, the drug remains in its primary form and is evacuated via biliary excretion, and the excreted half-life is reported to be 5 to 6 h [10]. Through various studies, it was determined that the metabolism of the respective drug varies in different model species, whereas, in humans, glucuronidation is the metabolic pathway that occurs by UGT1A3, UGT1A4, UGT2B7, and UGT2B17 [10, 119, 120]. Asciminib has a reversible inhibition effect on liver enzymes (CYP3A4/5, CYP2B6, CYP2C8, and CYP2C9), and this drug shows inhibition against the drug transporters (ABCB1, ABCG2, and OCT1) as well [10, 119, 120].
Toxicity
Although asciminib shows less toxicity than other drugs, some toxic effects include an asymptomatic increase in lipase and clinical pancreatitis; and other effects include nausea, headache, fatigue, joint pain, thrombocytopenia, and high blood pressure in both types of patients taking either a single or double daily dose of asciminib [117]. All in all, clinical pancreatitis is considered dose-limiting toxicity, as it occurs at doses greater than 40 mg twice daily, and is manageable following dosage modifications.
Conclusion
To date, six orally administered tyrosine kinase inhibitors (TKIs) have received approval (in the European Union and the United States) for CML therapy, and each has its efficacy and pharmacological profile. They all also differ based on chemical structure, but the presence of pyrimidine structure is common to all except bosutinib, which is quinazoline. In addition to the differences in structure and pharmacological effects, these TKIs also differ from each other in their association with CYP450 isoforms. Imatinib, nilotinib, dasatinib, and bosutinib are metabolized by CYP3A4, whereas ponatinib is metabolized primarily by CYP3A4/5 and minorities via CYP2C8 and CYP2D6. For asciminib, little information is there, but the inhibitory effect of this drug on several hepatic enzymes (CYP3A4/5, CYP2B6, CYP2C8, and CYP2C9) has been studied. Furthermore, all TKIs except bosutinib modulate CYP450 interactions with other compounds and thus alter the efficacy of this enzyme; consequently, bosutinib may be a better option for polymedicated patients.
Besides pharmacological profiles, these approved drugs also differ in their toxicity profiles. Nilotinib shows a lower level of fluid retention and possibly less hematological toxicity than other TKIs. At the same time, there is a higher incidence of headache, skin rash, pancreatitis, high blood glucose, hyperlipidemia, and cardiovascular toxicity in nilotinib-treated patients compared to imatinib. On the other hand, pleural effusion and gastrointestinal toxicity occurred more frequently in dasatinib patients. Comparing the effects of nilotinib, dasatinib, and imatinib, it has been verified that nilotinib- and dasatinib-treated patients have a higher risk of acute myocardial infarction as well as arterial and venous events. Adverse effects of ponatinib are headache, rash, abdominal pain, pancreatitis, and diarrhea; the prominent toxicities include cardiac toxicity (peripheral arterial occlusive disease, acute myocardial infarction, and arterial thrombosis) and cerebrovascular toxicity which limits its use despite having an effect against the simultaneous T315I mutation. In the case of asciminib-treated patients, low-grade toxicity (nausea, headache, fatigue, joint pain, thrombocytopenia, and high blood pressure) and clinical pancreatitis were found, but later it was found to be dose-dependent, and other than this, the myristoyl pocket mutation was found to be in only 5% of patients. The combination effect of asciminib with other TKIs generates a mechanism of action in which asciminib is effective against all catalytic site-associated mutations and another’s against myristoylic mutations, so the dual inhibition and synergistic effect results in a potent action in CML.
As is known so far, the treatment landscape of CML has changed radically after the introduction of multiple TKIs, which has enabled CML patients and clinicians to select the most appropriate drug by considering patients' concomitant medications, concomitant diseases, and risk factors. This review focuses on the absorption, metabolism, and toxicity of TKIs and provides a holistic view to the researchers and clinicians of TKIs on CML.
References
Frazer R, Irvine AE, McMullin MF (2007) Chronic myeloid leukaemia in the 21st century. Ulster Med J 76:8–17
Sattlermc M, Griffin JD (2003) Molecular mechanisms of transformation by the BCR-ABL oncogene. Semin Hematol 40:4–10. https://doi.org/10.1053/shem.2003.50034
Iqbal N, Iqbal N (2014) Imatinib: a breakthrough of targeted therapy in cancer. Chemother Res Pract. https://doi.org/10.1155/2014/357027
Sherbenou DW, Hantschel O, Kaupe I et al (2010) BCR-ABL SH3-SH2 domain mutations in chronic myeloid leukemia patients on imatinib. Blood 116(17):3278–3285. https://doi.org/10.1182/blood-2008-10-183665
Rosenzweig SA (2018) Acquired resistance to drugs targeting tyrosine kinases. Adv Cancer Res 138:71–98
Singh P, Gupta SK, Ali V, Verma M (2018) Downregulation of Bcr-Abl oncogene in chronic myeloid leukemia by micro RNAs. Asian Pac J Health Sci 5(4):65–84. https://doi.org/10.21276/apjhs.2018.5.4.12
Zabriskie MS, Vellore NA, Gantz KC et al (2015) Radotinib is an effective inhibitor of native and kinase domain-mutant BCR-ABL1. Leukemia 29(9):1939–1942. https://doi.org/10.1038/leu.2015.42
Gontarewicz A, Balabanov S, Keller G et al (2008) Simultaneous targeting of Aurora kinases and Bcr-Abl kinase by the small molecule inhibitor PHA-739358 is effective against imatinib-resistant BCR-ABL mutations including T315I. Blood 111(8):4355–4364. https://doi.org/10.1182/blood-2007-09-113175
https://clinicaltrials.gov/ct2/show/study/NCT03459534. Accessed 5 January 2022
Wylie AA, Schoepfer J, Jahnke W et al (2017) The allosteric inhibitor ABL001 enables dual targeting of BCR–ABL1. Nature 543(7647):733–737. https://doi.org/10.1038/nature21702
https://drugs.ncats.io/drug/M3X659D0FY. Accessed 5 January 2022
https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-asciminib-philadelphia-chromosome-positive-chronic-myeloid-leukemia. Accessed 5 January 2022
dos Santos SC, Mira NP, Moreira AS, Sá-Correia I (2012) Quantitative- and phospho-proteomic analysis of the yeast response to the tyrosine kinase inhibitor imatinib to pharmacoproteomics-guided drug line extension. OMICS 16(10):537–551. https://doi.org/10.1089/omi.2012.0012
Khateb M, Ruimi N, Khamisie H et al (2012) Overcoming Bcr-Abl T315I mutation by combination of GNF-2 and ATP competitors in an Abl-independent mechanism. BMC Cancer 12(1):1–10. https://doi.org/10.1186/1471-2407-12-563
Meirson T, Genna A, Lukic N et al (2018) Targeting invadopodia-mediated breast cancer metastasis by using ABL kinase inhibitors. Oncotarget 9(31):22158. https://doi.org/10.18632/oncotarget.25243
Salah E, Ugochukwu E, Barr AJ et al (2011) Crystal structures of ABL-related gene (ABL2) in complex with imatinib, tozasertib (VX-680), and a Type I inhibitor of the triazole carbothioamide class. J Med Chem 54(7):2359–2367. https://doi.org/10.1021/jm101506n
Lyseng-Williamson K, Jarvis B (2001) Imatinib Drugs 61(12):1765–1774. https://doi.org/10.2165/00003495-200161120-00007
Duckett DR, Cameron MD (2010) Metabolism considerations for kinase inhibitors in cancer treatment. Expert Opin Drug Metab Toxicol 6(10):1175–1193. https://doi.org/10.1517/17425255.2010.506873
Buchdunge E, Cioffi CL, Law N et al (2000) Abl Protein-Tyrosine Kinase Inhibitor STI571 Inhibits In Vitro Signal Transduction Mediated by c-Kit and Platelet-Derived Growth Factor Receptors. J Pharmacol Exp Ther 295:139–145
Blanke CD (2001) Evaluation of the safety and efficacy of an oral molecularly-targeted therapy, STI571, in patients with unresectable or metastatic gastrointestinal stromal tumors (GISTs) expressing c-kit (CD 117). Proc Am Soc Clin Oncol 20:1a
Deininger MWN, Druker BJ (2003) Specific targeted therapy of chronic myelogenous leukemia with imatinib. Pharmacol Rev 55(3):401–423. https://doi.org/10.1124/pr.55.3.4
Vigneri P, Wang JYJ (2001) Induction of apoptosis in chronic myelogenous leukemia cells through nuclear entrapment of BCR–ABL tyrosine kinase. Nat Med 7(2):228–234. https://doi.org/10.1038/84683
Peng B, Lloyd P, Schran H (2005) Clinical pharmacokinetics of imatinib. Clin Pharmacokinet 44(9):879–894. https://doi.org/10.2165/00003088-200544090-00001
White DL, Lu L, Clackson TP et al (2011) ATP dependent efflux transporters ABCB1 and ABCG2 are unlikely to impact the efficacy, or mediate resistance to the tyrosine kinase inhibitor, ponatinib. Blood 118:2745–2745. https://doi.org/10.1182/blood.V118.21.2745.2745
Hegedűs T, Őrfi L, Seprődi A et al (2002) Interaction of tyrosine kinase inhibitors with the human multidrug transporter proteins, MDR1 and MRP1. Biochim Biophys Acta Mol Basis Dis 1587(2–3):318–325. https://doi.org/10.1016/S0925-4439(02)00095-9
Hu S, Franke RM, Filipski KK et al (2008) Interaction of imatinib with human organic ion carriers. Clin Cancer Res 14(10):3141–3148. https://doi.org/10.1158/1078-0432.CCR-07-4913
Shukla S, Sauna ZE, Ambudkar S (2008) Evidence for the interaction of imatinib at the transport-substrate site(s) of the multidrug-resistance-linked ABC drug transporters ABCB1 (P-glycoprotein) and ABCG2. Leukemia 22(2):445–447. https://doi.org/10.1038/sj.leu.2404897
Dohse M, Scharenberg C, Shukla S et al (2010) Comparison of ATP-binding cassette transporter interactions with the tyrosine kinase inhibitors imatinib, nilotinib, and dasatinib. Drug Metab Dispos 38(8):1371–1380. https://doi.org/10.1124/dmd.109.031302
Burger H, van Tol H, Boersma AWM et al (2004) Imatinib mesylate (STI571) is a substrate for the breast cancer resistance protein (BCRP)/ABCG2 drug pump. Blood 104(9):2940–2942. https://doi.org/10.1182/blood-2004-04-1398
Giacomini KM (2005) Membrane transporters and drug response. Goodman & Gilman’s The Pharmacological Basis of Therapeutics 41–70
Maliepaard M, Scheffer GL, Faneyte IF et al (2001) Subcellular localization and distribution of the breast cancer resistance protein transporter in normal human tissues. Cancer Res 61(8):3458–3464
Nagashige M, Ushigome F, Koyabu N et al (2003) Basal membrane localization of MRP1 in human placental trophoblast. Placenta 24:951–958. https://doi.org/10.1016/S0143-4004(03)00170-X
Eechoute K, Sparreboom A, Burger H et al (2011) Drug transporters and imatinib treatment: implications for clinical practice. Clin Cancer Res 17(3):406–415. https://doi.org/10.1158/1078-0432.CCR-10-2250
Gupta SK, Singh P, Ali V, Verma M (2020) Role of membrane-embedded drug efflux ABC transporters in the cancer chemotherapy. Oncol Rev 14(2):448. https://doi.org/10.4081/oncol.2020.448
Hartmann J, Haap M, Kopp H-G, Lipp H-P (2009) Tyrosine kinase inhibitors – a review on pharmacology, metabolism and side effects. Curr Drug Metab 10(5):470–481. https://doi.org/10.2174/138920009788897975
Beumer JH, Natale JJ, Lagattuta TF et al (2006) Disposition of imatinib and its metabolite CGP74588 in a patient with chronic myelogenous leukemia and short-bowel syndrome. Pharmacotherapy 26(7):903–907. https://doi.org/10.1592/phco.26.7.903
Gambacorti-Passerini C, le Coutre P, Piazza R (2020) The role of bosutinib in the treatment of chronic myeloid leukemia. Future Oncol 16(02):4395–4408. https://doi.org/10.2217/fon-2019-0555
Dutreix C, Peng B, Mehring G et al (2004) Pharmacokinetic interaction between ketoconazole and imatinib mesylate (Glivec) in healthy subjects. Cancer Chemother Pharmacol 54(4):290–294. https://doi.org/10.1007/s00280-004-0832-z
Rochat B (2005) Role of cytochrome P450 activity in the fate of anticancer agents and in drug resistance. Clin Pharmacokinet 44(4):349–366. https://doi.org/10.2165/00003088-200544040-00002
Gschwind H-P, Pfaar U, Waldmeier F et al (2005) metabolism and disposition of imatinib mesylate in healthy volunteers. Drug Metab Dispos 33(10):1503–1512. https://doi.org/10.1124/dmd.105.004283
Nebot N, Crettol S, D’Esposito F et al (2010) Participation of CYP2C8 and CYP3A4 in the N-demethylation of imatinib in human hepatic microsomes. Br J Pharmacol 161(5):1059–1069. https://doi.org/10.1111/j.1476-5381.2010.00946.x
Marull M, Rochat B (2006) Fragmentation study of imatinib and characterization of new imatinib metabolites by liquid chromatography–triple-quadrupole and linear ion trap mass spectrometers. J Mass Spectrom 41(3):390–404. https://doi.org/10.1002/jms.1002
Wyman K, Atkins MB, Prieto V et al (2006) Multicenter Phase II trial of high-dose imatinib mesylate in metastatic melanoma. Cancer 106(9):2005–2011. https://doi.org/10.1002/cncr.21834
Ohyashiki K, Kuriyama Y, Nakajima A et al (2002) Imatinib mesylate-induced hepato-toxicity in chronic myeloid leukemia demonstrated focal necrosis resembling acute viral hepatitis. Leukemia 16(10):2160–2161. https://doi.org/10.1038/sj.leu.2402702
Tonyali O, Coskun U, Yildiz R et al (2010) Imatinib mesylate-induced acute liver failure in a patient with gastrointestinal stromal tumors. Med Oncol 27(3):768–773. https://doi.org/10.1007/s12032-009-9284-y
O’Brien SG, Meinhardt P, Bond E et al (2003) Effects of imatinib mesylate (STI571, Glivec) on the pharmacokinetics of simvastatin, a cytochrome P450 3A4 substrate, in patients with chronic myeloid leukaemia. Br J Cancer 89(10):1855–1859. https://doi.org/10.1038/sj.bjc.6601152
Elliott MA (2002) Imatinib mesylate. Reactions Weekly. https://doi.org/10.2165/00128415-200208920-00026
Brennan J (2003) Pdgfr-alpha mediates testis cord organization and fetal Leydig cell development in the XY gonad. Genes Dev 17(6):800–810. https://doi.org/10.1101/gad.1052503
Huang CTF, Weitsman SR, Dykes BN, Magoffin DA (2001) Stem cell factor and insulin-like growth factor-I stimulate luteinizing hormone-independent differentiation of rat ovarian theca cells. Biol Reprod 64(2):451–456. https://doi.org/10.1095/biolreprod64.2.451
Bairy K, Ramnarayan K, Prasad A, Nalini K (2011) Effect of imatinib on the biochemical parameters of the reproductive function in male Swiss albino mice. Indian J Pharmacol 43(4):389. https://doi.org/10.4103/0253-7613.83107
Arora B, Kumar L, Sharma A et al (2004) Pigmentary changes in chronic myeloid leukemia patients treated with imatinib mesylate. Ann Oncol 15(2):358–359. https://doi.org/10.1093/annonc/mdh068
Tsao AS, Kantarjian H, Cortes J et al (2003) Imatinib mesylate causes hypopigmentation in the skin. Cancer 98(11):2483–2487. https://doi.org/10.1002/cncr.11812
Valizadeh N (2011) Imatinib induced facial skin hyperpigmentation in a case of chronic myelogenous leukemia. Shiraz E Med J 12:162–164
Orasan O, Stefan A, Minciuna I et al (2020) Imatinib-induced interstitial pneumonitis – a literature review and case report. J Mind Med Sci 7(1):94–99. https://doi.org/10.22543/7674.71.P9499
Deininger M, O’Brien SG, Guilhot F et al (2009) International randomized study of interferon Vs STI571 (IRIS) 8-year follow up: sustained survival and low risk for progression or events in patients with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP) treated with imatinib. Blood 114(22):1126. https://doi.org/10.1182/blood.V114.22.1126.1126
Weisberg E, Manley PW, Cowan-Jacob SW et al (2007) Second generation inhibitors of BCR-ABL for the treatment of imatinib-resistant chronic myeloid leukaemia. Nat Rev Cancer 7:345–356. https://doi.org/10.1038/nrc2126
Saglio G, Kim D-W, Issaragrisil S et al (2010) Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med 362:2251–2259. https://doi.org/10.1056/NEJMoa0912614
Hegedűs C, Özvegy-Laczka C, Apáti Á et al (2009) Interaction of nilotinib, dasatinib and bosutinib with ABCB1 and ABCG2: implications for altered anti-cancer effects and pharmacological properties. Br J Pharmacol 158(4):1153–1164. https://doi.org/10.1111/j.1476-5381.2009.00383.x
Weisberg E, Manley PW, Cowan-Jacob SW et al (2007) Second generation inhibitors of BCR-ABL for the treatment of imatinib-resistant chronic myeloid leukaemia. Nat Rev Cancer 7(5):345–356. https://doi.org/10.1038/nrc2126
Thomas J, Wang L, Clark RE, Pirmohamed M (2004) Active transport of imatinib into and out of cells: implications for drug resistance. Blood 104(12):3739–3745. https://doi.org/10.1182/blood-2003-12-4276
Prenen H, Guetens G, de Boeck G et al (2006) Cellular uptake of the tyrosine kinase inhibitors imatinib and AMN107 in gastrointestinal stromal tumor cell lines. Pharmacology 77(1):11–16. https://doi.org/10.1159/000091943
Eadie LN, Saunders VA, Hughes TP, White DL (2013) Degree of kinase inhibition achieved in vitro by imatinib and nilotinib is decreased by high levels of ABCB1 but not ABCG2. Leuk Lymphoma 54(3):569–578. https://doi.org/10.3109/10428194.2012.715345
Eadie LN, Dang P, Goyne JM et al (2018) ABCC6 plays a significant role in the transport of nilotinib and dasatinib, and contributes to TKI resistance in vitro, in both cell lines and primary patient mononuclear cells. PLoS ONE 13(1):e0192180. https://doi.org/10.1371/journal.pone.0192180
Brendel C, Scharenberg C, Dohse M et al (2007) Imatinib mesylate and nilotinib (AMN107) exhibit high-affinity interaction with ABCG2 on primitive hematopoietic stem cells. Leukemia 21(6):1267–1275. https://doi.org/10.1038/sj.leu.2404638
Yin OQP, Gallagher N, Tanaka C et al (2009) Effects of hepatic impairment on the pharmacokinetics of nilotinib: an open-label, single-dose, parallel-group study. Clin Ther 31:2459–2469. https://doi.org/10.1016/j.clinthera.2009.11.015
Hazarika M, Jiang X, Liu Q et al (2008) Tasigna for chronic and accelerated phase philadelphia chromosome-positive chronic myelogenous leukemia resistant to or intolerant of imatinib. Clin Cancer Res 14(17):5325–5331. https://doi.org/10.1158/1078-0432.CCR-08-0308
Kantarjian H, Jabbour E, Grimley J, Kirkpatrick P (2006) Dasatinib. Nat Rev Drug Discov 5(9):717–719. https://doi.org/10.1038/nrd2135
Keam SJ (2008) Dasatinib BioDrugs 22(1):59–69. https://doi.org/10.2165/00063030-200822010-00007
McCormack PL, Keam SJ (2011) Dasatinib Drugs 71(13):1771–1795. https://doi.org/10.2165/11207580-000000000-00000
Condorelli F, Genazzani AA (2010) Dasatinib BioDrugs 24(3):157–163. https://doi.org/10.2165/11535870-000000000-00000
Talpaz M, Saglio G, Atallah E, Rousselot P (2018) Dasatinib dose management for the treatment of chronic myeloid leukemia. Cancer 124(8):1660–1672. https://doi.org/10.1002/cncr.31232
Piscitani L, Sirolli V, di Liberato L et al (2020) Nephrotoxicity associated with novel anticancer agents (Aflibercept, Dasatinib, Nivolumab): case series and nephrological considerations. Int J Mol Sci 21(14):4878. https://doi.org/10.3390/ijms21144878
Braun TP, Eide CA, Druker BJ (2020) Response and resistance to BCR-ABL1-targeted therapies. Cancer Cell 37(4):530–542. https://doi.org/10.1016/j.ccell.2020.03.006
O’Hare T, Walters DK, Stoffregen EP et al (2005) In vitro Activity of Bcr-Abl Inhibitors AMN107 and BMS-354825 against clinically relevant imatinib-resistant Abl kinase domain mutants. Cancer Res 65:4500–4505. https://doi.org/10.1158/0008-5472.CAN-05-0259
Hughes T, Saglio G, Branford S et al (2009) Impact of baseline BCR-ABL mutations on response to nilotinib in patients with chronic myeloid leukemia in chronic phase. J Clin Oncol 27(25):4204. https://doi.org/10.1200/JCO.2009.21.8230
Hiwase DK, Saunders V, Hewett D et al (2008) Dasatinib cellular uptake and efflux in chronic myeloid leukemia cells: therapeutic implications. Clin Cancer Res 14(12):3881–3888. https://doi.org/10.1158/1078-0432.CCR-07-5095
Furmanski BD, Hu S, Fujita K et al (2013) Contribution of Abcc4-mediated gastric transport to the absorption and efficacy of dasatinib. Clin Cancer Res 19:4359–4370. https://doi.org/10.1158/1078-0432.CCR-13-0980
Eley T, Luo FR, Agrawal S et al (2009) Phase I study of the effect of gastric acid pH modulators on the bioavailability of oral dasatinib in healthy subjects. J Clin Pharmacol 49(6):700–709. https://doi.org/10.1177/0091270009333854
Fallingborg J (1999) Intraluminal pH of the human gastrointestinal tract. Dan Med Bull 46(3):183–196
Lindauer M, Hochhaus A (2010) Dasatinib. In: Martens U. (eds) Small molecules in oncology. Recent results in cancer research vol 184 pp.83–102. Springer Berlin Heidelberg. https://doi.org/10.1007/978-3-642-01222-8_7
Christopher LJ, Cui D, Wu C et al (2008) Metabolism and disposition of dasatinib after oral administration to humans. Drug Metab Dispos 36(7):1357–1364. https://doi.org/10.1124/dmd.107.018267
McCafferty EH, Dhillon S, Deeks ED (2018) Dasatinib: a review in pediatric chronic myeloid leukemia. Paediatr Drugs 20(6):593–600. https://doi.org/10.1007/s40272-018-0319-8
Xue T, Luo P, Zhu H et al (2012) Oxidative stress is involved in Dasatinib-induced apoptosis in rat primary hepatocytes. Toxicol Appl Pharmacol 261(3):280–291. https://doi.org/10.1016/j.taap.2012.04.010
Cortes JE, Apperley JF, DeAngelo DJ et al (2018) Management of adverse events associated with bosutinib treatment of chronic-phase chronic myeloid leukemia: expert panel review. J Hematol Oncol 11(1):1–12. https://doi.org/10.1186/s13045-018-0685-2
Abbas R, Hug BA, Leister C et al (2011) Effect of ketoconazole on the pharmacokinetics of oral bosutinib in healthy subjects. J Clin Pharmacol 51(12):1721–1727. https://doi.org/10.1177/0091270010387427
Redaelli S, Perini P, Ceccon M et al (2015) In vitro and in vivo identification of ABCB1 as an efflux transporter of bosutinib. J Hematol Oncol 8(1):1–10. https://doi.org/10.1186/s13045-015-0179-4
Abbas R, Hsyu P-H (2016) Clinical pharmacokinetics and pharmacodynamics of bosutinib. Clin Pharmacokinet 55(10):1191–1204. https://doi.org/10.1007/s40262-016-0391-6
Hsyu P-H, Mould DR, Abbas R, Amantea M (2014) Population Pharmacokinetic and Pharmacodynamic Analysis of Bosutinib. Drug Metab Pharmacokinet DMPK. https://doi.org/10.2133/dmpk.DMPK-13-RG-126
Abbas R, Boni J, Sonnichsen D (2015) Effect of rifampin on the pharmacokinetics of bosutinib, a dual Src/Abl tyrosine kinase inhibitor, when administered concomitantly to healthy subjects. Drug Metab Pers Ther 30(1):57–63. https://doi.org/10.1515/dmdi-2014-0026
Perea J, Rada B, Gandía N (2018) Comparative pharmacology of tyrosine kinase inhibitors for the treatment of chronic myeloid leukemia. Int. J. Clin. Pharmacol. Pharmacother 3:134. https://doi.org/10.15344/2456-3501/2018/134
Abbas R, Leister C, Sonnichsen D (2013) A clinical study to examine the potential effect of lansoprazole on the pharmacokinetics of bosutinib when administered concomitantly to healthy subjects. Clin Drug Investig 33(8):589–595. https://doi.org/10.1007/s40261-013-0103-z
Cortes JE, Kantarjian HM, Brümmendorf TH et al (2011) Safety and efficacy of bosutinib (SKI-606) in chronic phase Philadelphia chromosome–positive chronic myeloid leukemia patients with resistance or intolerance to imatinib. Blood 118(17):4567–4576. https://doi.org/10.1182/blood-2011-05-355594
Gambacorti-Passerini C, Cortes JE, Lipton JH et al (2014) Safety of bosutinib versus imatinib in the phase 3 BELA trial in newly diagnosed chronic phase chronic myeloid leukemia. Am J Hematol 89(10):947–953. https://doi.org/10.1002/ajh.23788
Khoury HJ, Cortes JE, Kantarjian HM et al (2012) Bosutinib is active in chronic phase chronic myeloid leukemia after imatinib and dasatinib and/or nilotinib therapy failure. Blood 119(15):3403–3412. https://doi.org/10.1182/blood-2011-11-390120
Koschmieder S (2013) Profile of bosutinib and its clinical potential in the treatment of chronic myeloid leukemia. Onco Targets Ther 6:99–106. https://doi.org/10.2147/OTT.S19901
Cortes JE, Jean Khoury H, Kantarjian H et al (2016) Long-term evaluation of cardiac and vascular toxicity in patients with Philadelphia chromosome-positive leukemias treated with bosutinib. Am J Hematol 91(6):606–616. https://doi.org/10.1002/ajh.24360
Lim C, Miller GD, Bruno BJ (2014) Resistant mutations in CML and Ph+ALL – role of ponatinib. Biol Targets Ther 8:243. https://doi.org/10.2147/BTT.S50734
Cortes JE, Kantarjian H, Shah NP et al (2012) Ponatinib in refractory philadelphia chromosome-positive leukemias. N Engl J Med 367(22):2075–2088. https://doi.org/10.1056/NEJMOA1205127
O’Hare T, Shakespeare WC, Zhu X et al (2009) AP24534, a Pan-BCR-ABL inhibitor for chronic myeloid leukemia, potently inhibits the T315I mutant and overcomes mutation-based resistance. Cancer Cell 16(5):401–412. https://doi.org/10.1016/J.CCR.2009.09.028
Zhou T, Commodore L, Huang W-S et al (2011) Structural mechanism of the Pan-BCR-ABL inhibitor ponatinib (AP24534): lessons for overcoming kinase inhibitor resistance. Chem Biol Drug Des 77:1. https://doi.org/10.1111/j.1747-0285.2010.01054.x
Sen R, Natarajan K, Bhullar J et al (2012) The novel BCR-ABL and FLT3 inhibitor ponatinib is a potent inhibitor of the MDR-associated ATP-binding cassette transporter ABCG2. Mol Cancer Ther 11(9):2033–2044. https://doi.org/10.1158/1535-7163.MCT-12-0302
Lu L, Saunders VA, Leclercq TM et al (2015) Ponatinib is not transported by ABCB1, ABCG2 or OCT-1 in CML cells. Leukemia 29(8):1792–1794. https://doi.org/10.1038/leu.2015.35
Laramy JK, Kim M, Parrish KE et al (2018) Pharmacokinetic assessment of cooperative efflux of the multitargeted kinase inhibitor ponatinib across the blood-brain barrier. J Pharmacol Exp Ther 365(2):249–261. https://doi.org/10.1124/jpet.117.246116
Malofeeva E, v., Domanitskaya N, Gudima M, Hopper-Borge EA, (2012) Modulation of the ATPase and transport activities of broad-acting multidrug resistance factor ABCC10 (MRP7). Cancer Res 72(24):6457–6467. https://doi.org/10.1158/0008-5472.CAN-12-1340
Hopper-Borge EA, Churchill T, Paulose C et al (2011) Contribution of Abcc10 (Mrp7) to in vivo paclitaxel resistance as assessed in Abcc10 −/− Mice. Cancer Res 71(10):3649–3657. https://doi.org/10.1158/0008-5472.CAN-10-3623
Sun YL, Kumar P, Sodani K et al (2014) Ponatinib enhances anticancer drug sensitivity in MRP7-overexpressing cells. Oncol Rep 31(4):1605–1612. https://doi.org/10.3892/or.2014.3002
Cortes JE, Kim D-W, Pinilla-Ibarz J et al (2012) A pivotal phase 2 trial of ponatinib in patients with chronic myeloid leukemia (CML) and Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ALL) Resistant or Intolerant to Dasatinib or Nilotinib, or with the T315I BCR-ABL Mutation: 12-Month Follow-up of the PACE Trial. Blood 120(21):163. https://doi.org/10.1182/blood.V120.21.163.163
Narasimhan NI, Dorer DJ, Davis J et al (2014) Evaluation of pharmacokinetics and safety of ponatinib in subjects with chronic hepatic impairment and matched healthy subjects. Cancer Chemother Pharmacol 74(2):341–348. https://doi.org/10.1007/s00280-014-2511-z
Cortes JE, Kim D-W, Pinilla-Ibarz J et al (2013) A phase 2 Trial of ponatinib in philadelphia chromosome-positive leukemias. N Engl J Med 351(17):1721–1730. https://doi.org/10.1056/NEJMoa1306494
Lin D, Kostov R, Huang JT-J et al (2017) Novel pathways of ponatinib disposition catalyzed by CYP1A1 involving generation of potentially toxic metabolites. J Pharmacol Exp Ther 363:12–19. https://doi.org/10.1124/jpet.117.243246
Ye YE, Woodward CN, Narasimhan NI (2017) Absorption, metabolism, and excretion of [14C] ponatinib after a single oral dose in humans. Cancer Chemother Pharmacol 79(3):507–518. https://doi.org/10.1007/s00280-017-3240-x
Kadi AA, Darwish HW, Attwa MW, Amer SM (2016) Detection and characterization of ponatinib reactive metabolites by liquid chromatography tandem mass spectrometry and elucidation of bioactivation pathways. RSC Adv 6(76):72575–72585. https://doi.org/10.1039/C6RA09985H
Gainor JF, Chabner BA (2015) Ponatinib: accelerated disapproval. Oncologist 20(8):847. https://doi.org/10.1634/theoncologist.2015-0253
Sierra JR, Cepero V, Giordano S (2010) Molecular mechanisms of acquired resistance to tyrosine kinase targeted therapy. Mol Cancer 9(1):1–13. https://doi.org/10.1186/1476-4598-9-75
Gozgit JM, Squillace RM, Wongchenko MJ et al (2013) Combined targeting of FGFR2 and mTOR by ponatinib and ridaforolimus results in synergistic antitumor activity in FGFR2 mutant endometrial cancer models. Cancer Chemother Pharmacol 71(5):1315–2132. https://doi.org/10.1007/s00280-013-2131-z
Cortes JE, Saglio G, Kantarjian HM et al (2016) Final 5-year study results of dasision: the dasatinib versus imatinib study in treatment-naïve chronic myeloid leukemia patients trial. J Clin Oncol 34(12):1402. https://doi.org/10.1200/JCO.2015.64.8899
Hughes TP, Mauro MJ, Cortes JE et al (2019) Asciminib in chronic Myeloid leukemia after ABL kinase inhibitor failure. N Engl J Med 381(24):2315–2326. https://doi.org/10.1056/NEJMoa1902328
Réa D, Mauro MJ, Boquimpani C et al (2021) A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood 138(21):2031–2041. https://doi.org/10.1182/blood.2020009984
Manley PW, Barys L, Cowan-Jacob SW (2020) The specificity of asciminib, a potential treatment for chronic myeloid leukemia, as a myristate-pocket binding ABL inhibitor and analysis of its interactions with mutant forms of BCR-ABL1 kinase. Leuk Res 98:106458. https://doi.org/10.1016/j.leukres.2020.106458
Schoepfer J, Jahnke W, Berellini G et al (2018) Discovery of asciminib (ABL001), an allosteric inhibitor of the tyrosine kinase activity of BCR-ABL1. J Med Chem 61:8120–8135. https://doi.org/10.1021/acs.jmedchem.8b01040
Eadie LN, Saunders VA, Branford S et al (2018) The new allosteric inhibitor asciminib is susceptible to resistance mediated by ABCB1 and ABCG2 overexpression in vitro. Oncotarget 9(17):13423. https://doi.org/10.18632/oncotarget.24393
Breccia M, Colafigli G, Scalzulli E, Martelli M (2021) Asciminib: an investigational agent for the treatment of chronic myeloid leukemia. Expert Opin Investig Drugs. https://doi.org/10.1080/13543784.2021.1941863
Garcia-Gutiérrez V, Luna A, Alonso-Dominguez JM et al (2021) Safety and efficacy of asciminib treatment in chronic myeloid leukemia patients in real-life clinical practice. Blood Cancer J 11(2):1–4. https://doi.org/10.1038/s41408-021-00420-8
Acknowledgements
The authors acknowledge the support received from the Banaras Hindu University Varanasi, India in writing this manuscript. VK, PS, and VA are grateful to the CSIR, New Delhi, to award their fellowships.
Author information
Authors and Affiliations
Contributions
MV conceived and designed this review. VK collected the literature and made the first draft of the manuscript. MV, PS, SKG, and VA discussed and improved the study. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare there is no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, V., Singh, P., Gupta, S.K. et al. Transport and metabolism of tyrosine kinase inhibitors associated with chronic myeloid leukemia therapy: a review. Mol Cell Biochem 477, 1261–1279 (2022). https://doi.org/10.1007/s11010-022-04376-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-022-04376-6