
Abstract
Silicosis is one of the prolonged and irreversible occupational diseases. Crystalline silica dust, which has been linked with silicosis, occurs in different industrial areas such as constructions, ceramic, quarry, and pottery. There are significant numbers of newly diagnosed cases every year in Turkey. Patients with silicosis suffer from inflammatory respiratory disorders and silicosis-related complications such as rheumatoid arthritis, systemic sclerosis, and vasculitis. Oxysterols are defined as 27-carbon intermediates or end products of cholesterol. They are also implicated in the etiology of disease states such as atherosclerosis, neurodegenerative, and inflammatory diseases. The aim of the study is to evaluate cholesterol oxidation products in the patients with silicosis and determination of sphingosine-1-phosphate (S1P) levels which is a sphingolipid metabolite. In addition to these parameters, it is aimed to determine the possible lipid peroxidation by different parameters. For this purpose, blood samples and urine were collected from 47 patients and 30 healthy individual with their consents. In order to evaluate oxysterols, 7-ketocholesterol and cholestan 3β,5α,6β-triol levels were measured by LC–MS/MS method. The measured levels of 7-KC were 0.101 ± 0.005 µmol/l in patient and 0.050 ± 0.003 µmol/l in control plasma samples. Triol levels were measured as 0.038 ± 0.005 µmol/l in patient group and 0.033 ± 0.004 µmol/l in control group (p < 0.001). In addition, lipid peroxidation products were measured by human-8-isoprostane, human-4-hydroxynonenal (4-HNE), and human malondialdehyde (MDA) ELISA kits. The measured levels of HNE in the patient and control groups were 735.14 ± 288.80 pg/ml and 595.72 ± 108.62 pg/ml in plasma and 606.02 + 118.23 pg/ml and 531.84 + 107.18 pg/ml in urine, respectively (p < 0.05). F2-iP results of patients and controls were 450.0 + 101.40 pg/dl and 386.9 + 112.7 pg/ml for urine and 432.7 ± 188,8 pg/dl and 321.9 ± 69.4 pg/dl for plasma, respectively (p < 0.05). MDA levels of plasma were measured as 44.1 ± 14.6 nmol/ml in the patient and 31.9 ± 10.5 nmol/ml in the control (p < 0.05). Levels of MDA for urine samples were 30.15 + 5.06 nmol/ml and 25.15 + 6.07 nmol/ml in patients and controls, respectively (p < 0.05). S1P levels were decreased in patients compared to control group (49.05 ± 10.87 and 67.57 ± 16.25, p < 0.001). The results not only indicate a correlation between cholesterol oxidation, lipid peroxidation, and silicosis, but also provide better understanding of the role of the lipids in the mechanism of this inflammatory disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Silicosis is defined as the formation of small, typically round nodules in the lungs of persons exposed to crystalline silica dust. It is a progressive, fatal, irreversible, and untreatable fibrotic lung disease that is seen in individuals who are exposed to silica due to their occupation [1, 2]. The severity of the disease is related with the type of material inhaled and the intensity and duration of the exposure [3]. Occupational exposure to silica dust is an important health problem especially in developing countries [4,5,6]. There is a significant number of newly diagnosed silicosis cases every year in Turkey.
Patients with silicosis suffer from inflammatory respiratory disorders and silicosis-related complications such as rheumatoid arthritis, systemic sclerosis, and vasculitis [7, 8]. Oxidative stress has also been suggested to play a role in the pathophysiology of silicosis [9, 10] and silica radicals reportedly induce lipid peroxidation and DNA damage [11]. Therefore, researchers have explored the use of inflammatory and oxidative parameters as potential biomarkers of the disease and some studies have produced promising results [12]. However, studies focusing on the final products of lipid peroxidation such as malondialdehyde (MDA) and 4-hydroxynonenal (HNE) (collectively called reactive aldehydes), markers of in vivo oxidative stress (such as F2-isoprostane), and biologically active lipids including oxysterols and sphingosine-1-phosphate are few. Considering the biological properties and functions of oxysterols and S1P, it is apparent that further studies focused on these lipids, and lipid peroxidation products are necessary to understand whether these parameters are associated with silicosis pathophysiology.
Oxysterols are defined as 27-carbon intermediates or end products of cholesterol [13]. They are implicated in the development of neurodegenerative and inflammatory diseases and atherosclerosis [14]. Oxysterols such as 7-ketocholesterol (7-KC) and cholestane-3β,5α,6β-triol (C-triol) are recognized as non-enzymatically produced oxysterols and have pro-inflammatory properties; possibly making them ideal candidates for the assessment of oxidative stress and inflammatory activation [15, 16]. Sphingosine-1-phosphate (S1P), a sphingolipid metabolite, is a bioactive lipid which has been demonstrated to be central to various cellular and extracellular processes with its signaling properties. S1P is crucial for many physiological mechanisms including apoptosis, autophagy, angiogenesis, growth, inflammation, and cell migration [17].
Constant inflammatory activation in the lungs is a crucial pathophysiological process in silicosis progression, and oxidative stress plays a vital role in this activation [18]. Considering that lipids are susceptible to oxidation, and lipid peroxidation products are potential biomarkers for oxidative stress in vivo [16], we hypothesized that non-enzymatically produced oxysterols, S1P, and lipid peroxidation markers may be associated with silicosis development and progression. Therefore, in this study, our aim was to determine the levels of 7-KC, C-triol, S1P, and lipid peroxidation markers in patients with silicosis, and to evaluate whether they were associated with disease development and severity.
Materials and method
Subjects and biological samples
This study was approved by the Clinical Research Ethical Committee of Hacettepe University (Date and Number: 8/11/2016, GO 16/697-18).
The study group comprised 47 males with silicosis and 30 male controls. All patients were working in the ceramic industry, while those included in the control group were selected from male clerical workers who were comparable with the patient group in terms of age, smoking status, medications, and nutritional habits. A detailed questionnaire was prepared for all the participants. All samples (5 ml of urine, 5 ml of blood) from the patients and controls were obtained at Ankara Occupational and Environmental Diseases Hospital. Blood was collected in heparinized vacutainer tubes and urine samples (mid-stream) were kept in sterile containers. Plasma samples were obtained by centrifugation (10 min at 3000 rpm). All samples were aliquoted into Eppendorf tubes and were stored at − 80 °C until analyses were performed. The levels of triglycerides, cholesterol, high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL) of the study group were measured via auto-analyzers in the routine clinical chemistry laboratory.
The lung functions of the study group were evaluated via spirometry. The forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and FEV1/FVC ratio (as percentage) of all individuals were measured and recorded. A percentage lower than 75% for FEV1/FVC indicates airway obstruction and this value was used to determine the severity of airway obstruction. The International Labor Organization (ILO) International Classification of Radiographs of Pneumoconioses Guideline was used to categorize patients into 3 groups (categories 1, 2, and 3) according to radiography findings.
MDA, HNE, and F2-isoprostane analysis
MDA, HNE, and F2-isoprostane (F2-iP) were measured in the plasma and urine samples of all participants with commercial ELISA kits, which were obtained from Hangzhou Eastbiopharm Co., Ltd. (Hangzhou, China). For spectrophotometric measurement, a SpectraMax M2 device (Molecular Devices, Sunnyvale, CA, USA) was used and SoftMax Pro Software (Molecular Devices, Sunnyvale, CA, USA) was used for quantification of results.
Oxysterol analysis by LC–MS/MS
Oxysterol analysis was performed in 50 µl plasma samples by LC–MS/MS (Shimadzu Scientific Instruments, 8040) based on the method reported by Jiang et al. [19], which utilizes N,N-dimethylglycine ester derivatization for the quantification of free and unesterified oxysterol species. Internal standards were 3β,5α,6β-trihydroxycholestane D7 (Toronto) and 3β-hydroxy-5-cholestene-7-one D7 (Avanti). Standard calibration was done through eight-point calibration between 3.12 and 400 ng/ml. Two plasma quality control samples were prepared by spiking known amounts of 7-KC and C-triol standards to yield an endogenous level of 40/40 and 150/150 ng/ml, respectively. The liquid chromatography step was performed with a Symmetry C18 column (100 mm × 2.1 mm, 5 µm) (Thermo Fisher Scientific). The mobile phase consisted of a linear gradient of water and acetonitrile (1 mM ammonium formate at pH 3). Mass spectrometry analysis was performed in the positive ionization mode using electrospray ionization (ESI).
Sphingosine-1-phosphate analysis by LC–MS/MS
S1P analysis was performed by LC–MS/MS with a modified version of the method reported by Zhang et al. [20] with an Agilent 6420 triple quadrupole mass spectrometer. Plasma samples from patients and controls (50 µl) were mixed with 20 µl of 1000 ng/ml erythrosphingosine-d7 internal standard (Avanti, USA). After the addition of 500 µl’s of methanol, the tubes were vortexed (1 min) and centrifuged (3000 g, 10 min), and 400 µl of supernatant was taken for LC–MS/MS analysis (LC–MS/MS, Agilent 1260 Infinity UPLC). Chromatography was performed with an Agilent 1260 Infinity UPLC System equipped with refrigerated autosampler. A reverse-phase C18 type column set to 30 °C was used for separation (5 µm particle size, 4.6 × 50 mm). A binary solvent pump was used for mobile phase elution (A: Water with %0.01 formic acid and 10 mM ammonium acetate; B: Methanol with 0.01% formic acid). Elution conditions according to time were as follows: 0–0.5 min: 60% B, 0.5–1.1 min: increase B from 60 to 90%, 1.1–2.9 min: 90% B, 2.9–4 min: decrease B from 90 to 60%, and 4–8 min: 60% B. Total run time was 8 min with a flow rate of 0.4 ml/min. Agilent 6420 triple quadrupole mass spectrometer was set at multiple reaction monitoring (MRM) mode. Ion pairs were 380.2/264.3 (FV = 90, Collision energy = 12 eV) for S1P, and 309.1/164.8 (FV = 60, CE = 20 eV) for erythrosphingosine-d7. The ESI voltage was 5 kV, curtain gas flow was 40 lt/min, and source temperature was 500 °C.
Statistical analysis
Statistical analyses were performed using the SPSS version 20 software (IBM, Armonk, NY) and continuous variables were summarized by mean ± standard deviation. Initial comparisons of laboratory parameters between the two groups were performed using either the t-test for independent samples or the Mann–Whitney U test, depending on normality of distribution. Similarly, Spearman and Pearson’s correlation coefficients were used to evaluate associations between two continuous variables, depending on distribution. A p value lower or equal to 0.05 was accepted to show statistical significance.
Results
General characteristics and radiologic examination of the study population
A total of 47 (61%) patients with silicosis and 30 (39%) healthy controls were included in the study. All individuals were male. The mean age of the patient group was 41.8 ± 7.6 years, while mean age was 43.6 ± 9.6 years in the control group. Groups were similar in regard to age (p = 0.504). The percentage of individuals who smoked was 78.7% in the patients group and 43.3% in the control group. 85.1% of the patients had been working in the ceramic industry for more than 10 years. According to radiography findings, 43 of the patients were classified as category 1 and the other 4 patients were classified as category 2 and 3 according to ILO classification.
The FEV1/FVC percentages were calculated as 82.26 ± 6.5 and 84.27 ± 6.9 in controls and patients, respectively. There was no statistically significant difference between the groups. Additionally, 10.6% of patients with silicosis were found to have FEV1/FVC values lower than 75%.
Lipid profile in the patient and control groups
Plasma levels of triglycerides, cholesterol, HDL, and LDL were similar in both groups. The comparison of these values in regard to groups are depicted in Fig. 1.

Lipid profile in silicosis and control groups. HDL high-density lipoprotein, LDL low-density lipoprotein
Oxysterols, lipid peroxidation parameters, and S1P levels
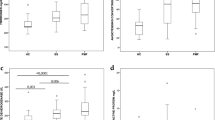
Plasma 7-KC and C-triol levels were significantly higher in patients with silicosis compared to controls (p < 0.001). The results are summarized in Fig. 2a, b.

Plasma 7-KC (a) and C-Triol (b) levels in silicosis and control groups, p < 0.001
The levels of F2-isoprostane, which is formed by non-enzymatic direct oxidation of arachidonic acid on the cell surface by oxygen radicals, were measured in the urine and plasma samples of all participants. Both the urine and plasma F2-isoprostane levels of patients were significantly higher than that of the controls (Fig. 3, p < 0.05).

Plasma and urine F2-isoprostane levels in patients with silicosis and controls, p < 0.05
MDA levels, one of the most important and frequently evaluated parameters of oxidative stress-induced lipid peroxidation, were also measured in study groups. The results showed that the urine and plasma MDA levels were statistically higher in the patient group compared to the control group (Fig. 4, p < 0.05).

Plasma and urine MDA levels in silicosis and control groups, p < 0.05
4-HNE levels in the patient group were significantly higher than the levels measured in controls (urine and plasma) (p < 0.05). The results are shown in Fig. 5.

Plasma and urine 4-HNE levels in patients with silicosis and controls, p < 0.05
Mean plasma S1P levels were significantly lower in patients (49.05 ± 10.87 ng/ml) compared to controls (49.05 ± 10.87 ng/ml) (p < 0.001).
The levels of all parameters and group comparisons are shown in Table 1.
Correlations between silicosis status, oxysterol levels (7-KC and C-triol), plasma and urinary levels of 4-HNE, MDA, and F2-iP were examined. The results of the correlation analysis are shown in Table 2.
A positive, high, and significant correlation was observed between silicosis state and 7-KC level (r = 0.984, p < 0.01). Similarly, there was a positive and significant relationship between C-triol and both 7-KC and silicosis. According to other laboratory parameters, positive correlations were observed between silicosis status and urine 4-HNE (r = 0.301, p < 0.01), plasma 4-HNE (r = 0.284, p < 0.05), urine MDA (r = 0.417, p < 0.01), plasma MDA (r = 0.289, p < 0.01), Urine F2-iP (r = 0.281, p < 0.05), and plasma F2-iP (r = 0.363, p < 0.01).
The relationships between laboratory parameters within the patients and controls control groups were also evaluated. The summary of significant correlations is given in Table 3. Negative correlations were observed between C-Triol and S1P in the control group (r = -0.380, p < 0.05), whereas there was a positive and significant relationship between C-Triol and urine MDA in the patient group (r = 0.339, p < 0.05). Similarly, negative correlations were determined between 7-KC and plasma MDA (r = − 0.313, p < 0.05); and between urine HNE and urine F2-iP in the patient group (r = − 0.323, p < 0.05).
Positive and significant correlations were found between the scores on the plasma HNE and plasma MDA (r = 0.886, p < 0.001), on the plasma HNE and plasma F2-iP (r = 0.830, p < 0.001), and on the plasma MDA and plasma F2-iP (r = 0.813, p < 0.001).
After determining that the plasma levels of MDA, HNE, and F2-iP showed high correlations in the patient group, and seeing that there were no significant relationships in the control group, we performed linear regression to evaluate these relationships in the patient group. The coefficient of determination obtained from the linear regression of these relationships also showed very strong results (R2 = 0.689, R2 = 0.785, R2 = 0.661). This result can be interpreted as a 1 ml increase in one of the plasma levels leading to a significant increase in the other plasma level.
Discussion
The results of our study clearly show that, compared to controls, patients with silicosis suffer from increased cholesterol oxidation and lipid peroxidation. In addition, we found that the plasma levels of lipid peroxidation products (MDA, 4-HNE, F2-iP) were highly correlated in patients, while this relationship was absent in controls. According to our results, there was no correlation between laboratory and spirometry tests results. These data can be found because of our limited case numbers.
Especially in developing countries, occupational exposure to silica is alarmingly common. Workers in many different sectors such as construction, ceramics, sand blasting, rock drilling, cutting, chipping or polishing, brick or tile cutting, concrete drilling, grinding, tunneling, demolition, mining, and also foundry workers are at risk for silicosis development [4, 21, 22]. Public attention was drawn to silicosis at the beginning of the twenty-first century due to the media attention surrounding the development of silicosis in thousands of individuals who worked in denim production with old sand-blasting machines [6, 23]. Since then, many other industries have been found to be associated with occupational silicosis, such as teflon cookware and electrical cable manufacturing [21]. Today, it is evident that any individual chronically exposed to crystalline silica is at risk for the development of various pulmonary diseases, including cancer and silicosis [24, 25]. Silica inhalation has also been associated with increased ROS formation, which increases lipid peroxidation and can cause damage to cells, tissues, and DNA [2, 16].
The cell membrane is a primary target for oxidative damage as one of its major functions is to protect the intracellular area from outside affects. The main component of the cell membrane is a double layer of lipids including phospholipids and cholesterol. 25 to 40% of the total lipid content of plasma membranes is cholesterol [26, 27]. Cholesterol modulates protein function in membranes and regulates the biophysical properties of lipid bilayers and many biological processes [26, 28].
This is the first study which demonstrated that lipid metabolism is affected and oxidative lipid damage is triggered in silicosis. Therefore, cholesterol oxidation can also be used as an important marker in this exposure group, and pathological changes in lipids may be effective in the disease progression. Chronic inflammation, oxidative stress, and cell death are suspected to play a role in the pathogenesis of many diseases. Several studies have suggested a link between cholesterol metabolism, especially the conversion of cholesterol to oxysterols, and inflammatory diseases [29]. The main mechanism of action for silicosis also could be related to inflammation formation. It could be also interesting to research other oxysterols and mechanisms with a large population. There is no currently available efficient treatments for most of the inflammatory diseases including silicosis. Therefore, a better knowledge of the biological activities of the different oxysterols is of interest, and constitutes an important step toward identification of pharmacological targets for the development of new therapeutic strategies.
Lipid peroxidation
In the current study, we found that the lipid profile of patients with silicosis was similar compare to controls. Furthermore, the levels of lipid peroxidation products were significantly increased in the serum and urine of patients with silicosis compared to controls. This finding is similar to prior studies in the literature which have consistently reported increased blood levels of MDA [30], 4-HNE [31, 32], and isoprostanes (including F2-iP) [33, 34] in silicosis and other diseases causing lung fibrosis. Malondialdehyde has been studied since the 1970s as a marker of lipid peroxidation, and has been shown to be associated with the severity of various diseases, especially those that cause chronic inflammatory activity [35, 36]. In a recent study by Nardi and colleagues, the plasma MDA levels of patients with silicosis and individuals occupationally exposed to crystalline silica were found to be higher than controls without exposure. The authors concluded that this may suggest MDA to be an early indicator of silica toxicity. Furthermore, the vitamin C levels of silicosis patients were significantly lower compared to controls, while those exposed to silica without silicosis diagnosis also had lower levels but statistical significance was not observed, indicating that the oxidant/antioxidant balance may not be excessively altered among individuals which have not progressed to silicosis (meaning their antioxidant defense may yet be capable of reducing the oxidative insult produced by silica exposure) [12]. The silicotic patients in our study had significantly increased levels of MDA compared to controls in both urine and plasma samples. Several other studies have similar results [37, 38], including a study from Turkey by Anlar et al. which reports increased MDA and lower levels of endogenous antioxidants such as catalase and superoxide dismutase in patients with silicosis [39].
4-Hydroxynonenal, another of the reactive aldehydes, received interest as a measure of lipid peroxidation after its discovery in 1991 [40], particularly due to its formation of protein adducts and the role of these adducts in various diseases characterized with increased oxidative stress, including cancer, neurodegenerative diseases, and conditions causing chronic inflammation [41, 42]. Isoprostanes are prostaglandin isomers that produced from polyunsaturated fatty acids by a free radical-catalyzed mechanism. F2-iP is one of the main classes of isoprostanes and the levels in blood or urine are widely regarded as the reference marker for the assessment of oxidative stress [43, 44]. To our knowledge, there are only a few studies which have evaluated 4-HNE and isoprostane levels in silicosis or other fibrotic lung diseases [32, 45]. In 2011, Pelclova et al. quantified the levels of 8-isoprostane, 4-HNE, and MDA in the breath condensate, plasma, and urine of 37 patients with silicosis and 29 controls. They showed that silicosis patients had significantly higher levels of 4-HNE and MDA in urine and plasma samples, respectively; while 8-isoprostane levels were only found to be increased in the breath condensate of patients with silicosis. They also evaluated whether systemic diseases such as ischemic heart disease, hypertension, and diabetes were effective on the levels of lipid peroxidation parameters, and found that 8-isoprostane and 4-HNE levels were not affected by the presence of systemic conditions and were a direct result of lung damage [32]. However, by doing so, they also included patients with diabetes and hypertension in their control group, which would have increased the levels of lipid peroxidation parameters in this group; thereby affecting statistical comparisons. In the current study, compared to healthy controls with similar characteristics, the levels of MDA, 4-HNE, and F2-iP were found to be significantly increased in both the plasma and urine samples of silicotic patients.
Oxysterols
Oxysterols are the 27-carbon oxidation products of cholesterol. They can be easily transported out of the cells with the addition of oxygen to the steroid ring or aliphatic side chain, which changes the hydrophobic/hydrophilic nature of the molecule [46, 47]. Oxysterol derivatives produced by autoxidation have been associated with many pathological conditions, and are suggested to be relatively accurate indicators of in vivo oxidation [29, 48]. Normally, oxysterols are found in mammalian tissues at very low concentrations; however, their levels are significantly altered in various pathological conditions including inflammatory diseases, atherosclerosis, neurological diseases, and cancer [8, 29, 49, 50].
Some oxysterols have important biological activities such as induction of cell death, and pro-oxidative and pro-inflammatory activities, and they can therefore contribute to the initiation and development of important diseases [51]. Moreover, there is an argument that oxysterols have a role in the initiation of the inflammatory process in chronic diseases [52]. There are also currently numerous experimental data supporting the notion that several oxysterols contribute to age-related diseases and are involved in aging process. Therefore, a better knowledge of the biological activities of oxysterols should permit to improve the understanding of aging process, and of the physiopathology of several age-related diseases [29].
Oxysterols may play role as immunosuppressors by affecting the production of cytotoxic lymphocytes and natural killer (NK) cells, which can inhibit the de novo biosynthesis of sterols. Cholesterol is required molecule for the proliferation and cytotoxicity of lymphocytes. Certain inflammatory functions of macrophages and lymphocytes are affected by oxysterols as the generation of ROS and the activity of interleukin (IL) 1. It is also shown in different cell lines that 7KC induced both expression and synthesis of key chemokines for monocytes/macrophages, particularly monocyte chemoattractant protein-1 (MCP-1) [51].
The current study aimed to evaluate oxysterol levels, which are formed by auto-oxidation of cholesterol in silicosis patients, determining S1P levels as a sphingolipid metabolite, and to determine the possible lipid peroxidation as well as the related parameters by different parameters.
In our study, it was found that 7-KC is positively and highly correlated with silicosis status. 7KC is a potent inducer of inflammation, and therefore it could also contribute in the inflammation observed in silicosis. Furthermore, our measured values are comparable with the literature which shows the specificity of our methods [51, 53]. These results generally show a relationship between increased urine and plasma levels, which suggests that it plays a potential role for silicosis disease. High and significant correlations between the plasma levels of MDA, 4-HNE, and F2-iP levels were observed in the patient group. Although there are studies evaluating oxidative stress and ROS formation in silicosis, to our knowledge, this is the first study to evaluate cholesterol oxidation and its association with lipid peroxidation in silicosis.
Hinamoto et al. evaluated the correlations between the plasma and urinary levels and the clinicopathological parameters in patients with renal disorders [52]. In their study, no significant relationship was found between plasma and urine levels, but plasma levels were found to be positively correlated with each other. They determined that urine levels were positively correlated with each other and the presence of mesangial hyper-cellularity [52]. These findings are quite consistent with our results.
Conclusion and recommendations
In order to determine cholesterol oxidation, levels of 7-KC and triol have been measured with elevated levels of silicosis and it has been predicted that they may be biomarkers in the disease. Therefore, it is thought that cholesterol oxidation in this patient group may also play a role in the pathogenesis of the disease. Findings have shown that lipid peroxidation is induced in these patients. Our results suggest that cholesterol oxidation can be used as an important marker in this group of exposures, and in silicosis lipid metabolism is affected and oxidative lipid damage is triggered. There are several important considerations regarding the physiological/pathophysiological functions and activities of the different oxysterols. It is therefore important to determine their biological activities and identify their signaling pathways, when they are used either in isolation or as mixtures. Therefore, it is concluded that it is meaningful to perform large-scale lipidomic studies by increasing the number of patients in the future. In addition, information was collected from the Department of Chest Diseases and Tuberculosis of the Ankara Kecioren Occupational and Environmental Diseases Hospital, Ankara, where samples were collected, indicating that new cases were lighter prognosis than previous applications, but structural changes due to oxidative damage were also determined at these stages of the disease. Due to oxidative lipid damage in patients, it can be suggested that antioxidant supplementation and attention to feeding of these patients are also important. Regular usage of antioxidant supplements can reduce free radical reactions and oxidative lipid damage, thus delaying the development of lung fibrosis.
References
Prasad B, Pandey J (2016) Serum copper and zinc level as biomarker for dust exposed lung diseases among coal miners. J Biodiv Environ Sci 8:65–74
Pandey JK, Agarwal D (2012) Biomarkers: a potential prognostic tool for silicosis. Indian J Occup environmental Med 16:101
Karkhanis VS, Joshi J (2012) Combined pulmonary fibrosis and emphysema in a tyre industry worker. Lung India 29:273
Akgun M, Araz O, Akkurt I, Eroglu A, Alper F, Saglam L, Mirici A, Gorguner M, Nemery B (2008) An epidemic of silicosis among former denim sandblasters. Eur Respir J 32:1295–1303
Anlar HG, Bacanli M, İritaş S, Bal C, Kurt T, Tutkun E, Hinc Yilmaz O, Basaran N (2017) Effects of occupational silica exposure on oxidative stress and immune system parameters in ceramic workers in Turkey. J Toxicol Environ Health Part A 80:688–696
Akgün M, Ergan B (2018) Silicosis in Turkey: is it an endless nightmare or is there still hope? Turkish Thorac J 19:89
Archontogeorgis K, Steiropoulos P, Tzouvelekis A, Nena E, Bouros D (2012) Lung cancer and interstitial lung diseases: a systematic review. Pulm Med. https://doi.org/10.1155/2012/315918
Sabuncuoğlu S, Öztaş Y (2014) Oxysterols and their metabolic roles beyond cholesterol: a reappraisal. Acta Med 45:75–79
Bargagli E, Olivieri C, Bennett D, Prasse A, Muller-Quernheim J, Rottoli P (2009) Oxidative stress in the pathogenesis of diffuse lung diseases: a review. Respir Med 103:1245–1256
Vallyathan V, Leonard S, Kuppusamy P, Pack D, Chzhan M, Sanders SP, Zweir JL (1997) Oxidative stress in silicosis: evidence for the enhanced clearance of free radicals from whole lungs. Mol Cell Biochem 168:125–132
Shi X, Mao Y, Daniel LN, Saffiotti U, Dalal NS, Vallyathan V (1994) Silica radical-induced DNA damage and lipid peroxidation. Environ Health Perspect 102(10):149–154. https://doi.org/10.1289/ehp.94102s10149
Nardi J, Nascimento S, Goethel G, Gauer B, Sauer E, Fao N, Cestonaro L, Peruzzi C, Souza J, Garcia SC (2018) Inflammatory and oxidative stress parameters as potential early biomarkers for silicosis. Clin Chim Acta 484:305–313. https://doi.org/10.1016/j.cca.2018.05.045
Luu W, Sharpe LJ, Capell-Hattam I, Gelissen IC, Brown AJ (2016) Oxysterols: old tale, new twists. Annu Rev Pharmacol Toxicol 56:447–467
Lütjohann D, Lizard G, Iuliano L (2017) Oxysterols: players in different metabolic leagues. J Steroid Biochem Mol Biol. https://doi.org/10.1016/j.jsbmb.2017.03.011
Iuliano L (2011) Pathways of cholesterol oxidation via non-enzymatic mechanisms. Chem Phys Lipid 164:457–468
Niki E (2008) Lipid peroxidation products as oxidative stress biomarkers. BioFactors 34:171–180
Maceyka M, Harikumar KB, Milstien S, Spiegel S (2012) Sphingosine-1-phosphate signaling and its role in disease. Trends Cell Biol 22:50–60. https://doi.org/10.1016/j.tcb.2011.09.003
Rimal B, Greenberg AK, Rom WN (2005) Basic pathogenetic mechanisms in silicosis: current understanding. Curr Opin Pulm Med 11:169–173
Jiang X, Sidhu R, Porter FD, Yanjanin NM, Speak AO, te Vruchte DT, Platt FM, Fujiwara H, Scherrer DE, Zhang J (2011) A sensitive and specific LC-MS/MS method for rapid diagnosis of Niemann-Pick C1 disease from human plasma. J Lipid Res 52:1435–1445
Zhang Y, Berka V, Song A, Sun K, Wang W, Zhang W, Ning C, Li C, Zhang Q, Bogdanov M, Alexander DC, Milburn MV, Ahmed MH, Lin H, Idowu M, Zhang J, Kato GJ, Abdulmalik OY, Zhang W, Dowhan W, Kellems RE, Zhang P, Jin J, Safo M, Tsai AL, Juneja HS, Xia Y (2014) Elevated sphingosine-1-phosphate promotes sickling and sickle cell disease progression. J Clin Invest 124:2750–2761. https://doi.org/10.1172/JCI74604
Sari G, Simsek C, Gebesoglu B, Gulgosteren S, Uzmezoglu B and Celik D (2017) Accelerated silicosis in teflon-coated pan manufacturing: case report. C59. SILICOSIS, American Thoracic Society, pp. A5963–A5963
Köksal N, Kahraman H (2011) Acute silicosis in teflon-coated pan manufacturing due to metal sandblasting. Int J Occup Environ Health 17:210–213
Thomas CR, Kelley TR (2010) A brief review of silicosis in the United States. Environ Health Insights 4:EHI-S4628
Peluso ME, Munnia A, Giese RW, Chellini E, Ceppi M, Capacci F (2015) Oxidatively damaged DNA in the nasal epithelium of workers occupationally exposed to silica dust in Tuscany region, Italy. Mutagenesis 30:519–525
Wang Y, Yang G, Zhu Z, Liang D, Niu P, Gao A, Chen L, Tian L (2015) Effect of bone morphogenic protein-7 on the expression of epithelial–mesenchymal transition markers in silicosis model. Exp Mol Pathol 98:393–402
Ikonen E (2008) Cellular cholesterol trafficking and compartmentalization. Nat Rev Mol Cell Biol 9:125–138. https://doi.org/10.1038/nrm2336
Berkowitz ML (2009) Detailed molecular dynamics simulations of model biological membranes containing cholesterol. Biochim Biophys Acta (BBA) 1788:86–96
Kulig W, Cwiklik L, Jurkiewicz P, Rog T, Vattulainen I (2016) Cholesterol oxidation products and their biological importance. Chem Phys Lipid 199:144–160. https://doi.org/10.1016/j.chemphyslip.2016.03.001
Zarrouk A, Vejux A, Mackrill J, O’Callaghan Y, Hammami M, O’Brien N, Lizard G (2014) Involvement of oxysterols in age-related diseases and ageing processes. Ageing Res Rev 18:148–162
Cojocaru M, Niculescu T (1997) Study of plasma lipid peroxides in silicosis. Jugoslovenska Medicinska Biohemija-Yugoslav Med Biochem 16:25–27
Syslova K, Kacer P, Kuzma M, Najmanova V, Fenclova Z, Vlckova S, Lebedova J, Pelclova D (2009) Rapid and easy method for monitoring oxidative stress markers in body fluids of patients with asbestos or silica-induced lung diseases. J Chromatogr B 877:2477–2486. https://doi.org/10.1016/j.jchromb.2009.06.008
Pelclova D, Fenclova Z, Syslova K, Vlckova S, Lebedova J, Pecha O, Belacek J, Navratil T, Kuzma M, Kacer P (2011) Oxidative stress markers in exhaled breath condensate in lung fibroses are not significantly affected by systemic diseases. Ind Health 49:746–754
Arezzini B, Vecchio D, Signorini C, Stringa B, Gardi C (2018) F2-isoprostanes can mediate bleomycin-induced lung fibrosis. Free Radic Biol Med 115:1–9. https://doi.org/10.1016/j.freeradbiomed.2017.11.007
Montuschi P, Ciabattoni G, Paredi P, Pantelidis P, du Bois RM, Kharitonov SA, Barnes PJ (1998) 8-Isoprostane as a biomarker of oxidative stress in interstitial lung diseases. Am J Respir Crit Care Med 158:1524–1527. https://doi.org/10.1164/ajrccm.158.5.9803102
Muus P, Bonta IL, den Oudsten SA (1979) Plasma levels of malondialdehyde, a product of cyclo-oxygenase-dependent and independent lipid peroxidation in rheumatoid arthritis: a correlation with disease activity. Prostaglandins Med 2:63–65
Bragt PC, Schenkelaars EP, Bonta IL (1979) Dissociation between prostaglandin and malondialdehyde formation in exudate and increased levels of malondialdehyde in plasma and liver during granulomatous inflammation in the rat. Prostaglandins Med 2:51–61
Zhang H, Yin G, Jiang H, Zhang C (2013) High-dose N-acetylcysteine decreases silica-induced lung fibrosis in the rat. J Int Med Res 41:1179–1186. https://doi.org/10.1177/0300060513488503
Azari M, Ramazani B, Ali Mosavian M, Movahadi M, Salehpour S (2011) Serum malondialdehyde and urinary neopterin levels in glass sandblasters exposed to crystalline silica aerosols. Int J Occup Hyg 3(1):29–32
Anlar HG, Bacanli M, Iritas S, Bal C, Kurt T, Tutkun E, Hinc Yilmaz O, Basaran N (2017) Effects of occupational silica exposure on oxidative stress and immune system parameters in ceramic workers in Turkey. J Toxicol Environ Health A 80:688–696. https://doi.org/10.1080/15287394.2017.1286923
Esterbauer H, Schaur RJ, Zollner H (1991) Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med 11:81–128
Barrera G, Pizzimenti S, Ciamporcero ES, Daga M, Ullio C, Arcaro A, Cetrangolo GP, Ferretti C, Dianzani C, Lepore A, Gentile F (2015) Role of 4-hydroxynonenal-protein adducts in human diseases. Antioxid Redox Signal 22:1681–1702. https://doi.org/10.1089/ars.2014.6166
Barrera G, Pizzimenti S, Daga M, Dianzani C, Arcaro A, Cetrangolo GP, Giordano G, Cucci MA, Graf M, Gentile F (2018) Lipid Peroxidation-derived aldehydes, 4-hydroxynonenal and malondialdehyde in aging-related disorders. Antioxidants (Basel). https://doi.org/10.3390/antiox7080102
Nikolaidis MG, Kyparos A, Vrabas IS (2011) F2-isoprostane formation, measurement and interpretation: the role of exercise. Prog Lipid Res 50:89–103
Czerska M, Zielinski M and Gromadzinska J (2015) Isoprostanes: a novel major group of oxidative stress markers Biochim Biophys Acta, 1851(4), 433–445.
Pelclova D, Fenclova Z, Kacer P, Navratil T, Kuzma M, Lebedova JK, Klusackova P (2007) 8-isoprostane and leukotrienes in exhaled breath condensate in Czech subjects with silicosis. Ind Health 45:766–774
Björkhem I, Diczfalusy U, Lütjohann D (1999) Removal of cholesterol from extrahepatic sources by oxidative mechanisms. Curr Opin Lipidol 10:161–165
Leonarduzzi G, Sottero B, Poli G (2002) Oxidized products of cholesterol: dietary and metabolic origin, and proatherosclerotic effects. J Nutr Biochem 13:700–710
van Reyk DM, Brown AJ, Hult'en LM, Dean RT, Jessup W (2006) Oxysterols in biological systems: sources, metabolism and pathophysiological relevance. Redox Rep 11:255–262. https://doi.org/10.1179/135100006X155003
Jusakul A, Yongvanit P, Loilome W, Namwat N, Kuver R (2011) Mechanisms of oxysterol-induced carcinogenesis. Lipids Health Dis. https://doi.org/10.1186/1476-511x-10-44
Poli G, Biasi F, Leonarduzzi G (2013) Oxysterols in the pathogenesis of major chronic diseases. Redox Biol 1:125–130
Vejux A, Lizard G (2009) Cytotoxic effects of oxysterols associated with human diseases: Induction of cell death (apoptosis and/or oncosis), oxidative and inflammatory activities, and phospholipidosis. Mol Aspects Med 30:153–170
Hinamoto N, Maeshima Y, Saito D, Yamasaki H, Tanabe K, Nasu T, Watatani H, Ujike H, Kinomura M, Sugiyama H (2014) Urinary and plasma levels of vasohibin-1 can predict renal functional deterioration in patients with renal disorders. PLoS ONE 9:e96932
Nury T, Zarrouk A, Ragot K, Debbabi M, Riedinger J-M, Vejux A, Aubourg P, Lizard G (2017) 7-Ketocholesterol is increased in the plasma of X-ALD patients and induces peroxisomal modifications in microglial cells: Potential roles of 7-ketocholesterol in the pathophysiology of X-ALD. J Steroid Biochem Mol Biol 169:123–136
Acknowledgements
The authors are thankful to all study participants. The authors would like to acknowledge all colleagues who assisted with this study. This study was supported by Hacettepe University Coordination Unit for Scientific Research Projects (GO 16/697-18).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Aksu, N., Samadi, A., Yalçınkaya, A. et al. Evaluation of oxysterol levels of patients with silicosis by LC–MS/MS method. Mol Cell Biochem 467, 117–125 (2020). https://doi.org/10.1007/s11010-020-03706-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-020-03706-w