
Abstract
To investigate the clinical significance of suppressor of cytokine signaling (SOCS)-2 and SOCS6 in human hepatocellular carcinoma (HCC). The expression levels of SOCS2 and SOCS6 mRNA and protein in tumor, para-tumor and normal liver tissues were detected in 106 HCC patients by real-time quantitative RT-PCR (qRT-PCR) and Western blot. According to qRT-PCR and western blot analyses, we first found that both the expression levels of SOCS2 and SOCS6 mRNA and protein in HCC were significantly lower than those in para-tumor (both P < 0.001) and normal liver tissues (both P < 0.001). Then, the correlation analysis showed that both SOCS2 and SOCS6 protein downregulation were significantly correlated with advanced TNM stage (both P < 0.001) and high serum AFP (P = 0.008 and 0.01, respectively). Especially, the reduced expression of SOCS2 more frequently occurred in HCC patients with vascular invasion (P = 0.03), and that of SOCS6 was also associated with tumor recurrence (P = 0.01). Moreover, HCC patients with low expression of SOCS2 and SOCS6 had significantly shorter overall (P = 0.008 and 0.01, respectively) and disease-free survival (both P = 0.01). Furthermore, multivariate analysis showed that both SOCS2 and SOCS6 downregulation were independent prognostic factors of overall (P = 0.01 and 0.03, respectively) and disease-free survival (P = 0.01 and 0.03, respectively) in HCC. Our data demonstrate for the first time that SOCS2 and SOCS6 expression were remarkably reduced in HCC and may be served as potential prognostic markers for patients with this deadly disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) ranks the fifth most prevalent malignant tumors and the third leading cause of cancer-related death in the world [1]. Especially in the Asian Pacific region, HCC is among the top three causes of cancer death because of the high prevalence of chronic hepatitis B or C viral infections. In recent years, the incidence of HCC in the United States and in Western Europe has been increasing [2]. Although many risk factors, such as hepatitis B or C viral infections, alcohol consumption and genetic predisposition, have been identified, the exact molecular mechanisms and pathogenic processes underlying hepatocarcinogenesis have not been fully elucidated. Despite the advancement of diagnostic and therapeutic technology in HCC, the mortality of this tumor is very high, because most patients are in advanced stage at the time of diagnosis and cannot be treated with radical hepatectomy [3]. Therefore, it is necessary to identify novel and effective molecular markers which could give some clues to understand the carcinogenic processes of HCC, and could enhance the diagnostic and prognostic levels to provide scientific guidance to clinical management.
The suppressor of cytokine signaling (SOCS) family of proteins, containing eight members, CIS and the SOCS1-7 proteins, are negative feedback regulators of several cytokine pathways, particularly the receptor-associated tyrosine kinase/signal transducer and activator of transcription (Jak/STAT) pathways of transcriptional activation [4]. These proteins have been classified according to their structural domains: a conserved C-terminus referred to as the SOCS box, a central SH2 (src homology-2) domain, and a unique N-terminal region of variable length [5]. The deregulation of SOCSs, correlated with transcriptional silencing, has been found to be associated with many diseases, such as cancers, autoimmune diseases and disorders in hematopoiesis [6]. Recent studies have demonstrated that two members of this family, SOCS1 and SOCS3, may be involved into the tumorigenesis and tumor progression of HCC. For example, Okochi et al. [7] identified SOCS1 as a tumor suppressor of HCC and indicated that the aberrant methylation of SOCS1 might be a key event for HCC transformation of cirrhotic nodules; Niwa et al. [8] demonstrated that methylation silencing of SOCS3 could promote cell growth and migration by enhancing Jak/STAT and FAK signalings in human HCC. However, the involvement of other SOCS members in HCC is still unclear.
SOCS2, similar with the other members of the SOCS family, can regulate the cytokine-dependent Jak/STAT signaling pathway in several systems in vitro [9]. SOCS1 and SOCS3 inhibit the Jak/STAT pathway by direct interaction with Jak proteins, whereas SOCS2 presumably binds to cytokine receptors. It is also able to regulate the GH, IGF-1, PRL, IL-2, IL-3, EPO, LIF, EGF, leptin and IFN-α-dependent signaling pathways, either positively or negatively [10]. Accumulating studies have reported that SOCS2 plays important roles in the central nervous system, the regulation of metabolism, the immune response, and the mammary gland development [11]. Consistent with the role of cytokines in human physiology, aberrant expression of SOCS2 may lead to a broad range of pathologies such as cardiovascular diseases, insulin resistance, cancer, and severe infections [12]. Especially in human malignancies, recent studies have demonstrated that SOCS2 imbalance may be associated with myeloid leukemia, pulmonary adenocarcinoma, ovarian cancer, breast cancer, and anal cancers [13–16]. However, its role in HCC has not been elucidated yet.
SOCS6, unlike other SOCS family members, has a unique addition of 300 amino acids to its N-terminal region and the role of this addition is still unclear [17]. Thus, its function might be expected to be different from the other SOCS members. It has been demonstrated that SOCS6 does not interact with Jak2 or inhibit signaling by interleukins, GH, leukemia inhibitory factor, or prolactin. SOCS6 protein localizes to the nucleus and directly regulates insulin receptor (IR) signaling by interacting with IRS-2, IRS-4 and the p85 subunit of phosphoinositide (PI) 3-kinase [18]. It also interacts with KIT to suppress stem cell factor (SCF)-induced cell proliferation. The SOCS6 transgenic mice had no significant defects in cytokine signaling and hematopoietic system but displayed significant improvement in glucose metabolism [19]. Regarding to the relationship to carcinogenesis, SOCS6 is able to reduce STAT3, a transcription factor important for cancer progression [20]. Loss of SOCS6 may correlate with colorectal cancer and gastric cancer [21, 22]. Yoon et al. [23] found that SOCS6 expression was downregulated in thyroid grand and liver cancer tissues. However, the roles of SOCS6 in HCC are still unclear.
To confirm the potential value of SOCS2 and SOCS6 in human HCC, we performed real-time quantitative RT-PCR (qRT-PCR) and Western blot to determine the expression of SOCS2 and SOCS6 in HCC samples, and evaluated their relationship to clinical features and prognosis of HCC patients.
Materials and methods
Patients and tissue samples
The study was approved by the Research Ethics Committee of Fourth Military Medical University & the 302nd Hospital of PLA, China. Informed consent was obtained from all of the patients. All specimens were handled and made anonymous according to the ethical and legal standards.
Fresh tissue samples of tumor, para-tumor (defined as ≤2.0 cm distance from tumor edge) and normal (defined as >2.0 cm distance from tumor edge) liver tissues were collected from 106 HCC patients who underwent curative hepatectomy between April 2001 and May 2009 at Xijing Hospital, the 302nd Hospital of PLA & Tangdu Hospital. The criteria for curative hepatectomy were defined as complete resection of the tumor without macroscopic evidence of residual tumor. All patients were confirmed by histological diagnosis. None of the patients received preoperative anticancer treatment. One hundred and six patients with HCC included 78 male and 28 female, with a median age of 52 years old (mean ± SD 52.1 ± 14.8, range 31–72). Preoperative liver function was evaluated by the Child–Pugh score system. Tumor stage was determined according to the tumor-node-metastasis (TNM) classification system of the International Union against Cancer (2002). Tumor differentiation was graded by the Edmondsonp–Steiner classification system. The clinicopathological features of the patients are summarized in Table 1. The fresh tissue samples were immediately immersed in RNAlater (Ambion, Inc., USA) after surgical resection, stored at 4 °C overnight to allow thorough penetration of the tissue and then frozen at −80 °C until use.
Follow-up usually included serum α-fetoprotein (AFP) level, abdominal ultrasonography, and chest radiography every 1–3 months after curative hepatectomy, and was completed in December 2012. The follow-up time for these patients ranged from 2 to 65 months with a median follow-up time of 26 months. When tumor recurrence was suspected, computed tomography scan or/and magnetic resonance imaging scan was performed to confirm the diagnosis. Overall survival was defined as the interval between the date of surgery and the date of death. Disease-free survival was defined as the interval between the date of surgery and the date when recurrence was diagnosed or to the date of the last follow up.
Real-time quantitative RT-PCR
Total RNA was extracted from frozen tissues using TRIzol reagent (Invitrogen, USA) according to the manufacturer’s instruction. The integrity of all tested total RNA samples was verified using a Bioanalyzer 2100 (Agilent Technologies). Reverse transcription (RT) was performed with 2 μg of total RNA. cDNA was synthesized from the RNA by M-MLV Reverse Transcriptase (Promega, USA) with random primers (Promega, USA) in a 20 μL volume. Real-time PCR amplifications were performed using ABI PRISM 7900HT instruments (Applied Biosystems) in a total volume of 10 μL with the following amplification steps: an initial denaturation step at 94 °C for 80 min, which was followed by 40 cycles of denaturation at 95 °C for 15 s and elongation at 60 °C for 1 min. Primers for SOCS2, SOCS6, and GAPDH were designed as follows: SOCS2, forward: CGA GCT CAG TCA AAC AGG TAG G, reverse: GCT TTC AGA TGT AGG GTG CTT CC; SOCS6, forward: AAG AAT TCA TCC CTT GGA TTA GGT AAC, reverse: CAG ACT GGA GGT CGT GGA A; GAPDH, forward: CTC CTC CTG TTC GAC AGT CAG C, reverse: CCC AAT ACG ACC AAA TCC GTT. The relative expression levels of the SOCS2 and SOCS6 in HCC were normalized against the endogenous GAPDH using the comparative threshold cycle (2−ΔΔCt) method.
Western blot analysis
The fresh tissues from HCC patients were homogenated in a RIPA lysis buffer and centrifuged at 20,000×g for 60 min at 4 °C to pellet any precipitate. The protein concentration of the lysate was determined by the BCA assay. For western blot analysis, 20 μg of the protein extracts were loaded onto 12 % SDS–PAGE and transferred to PVDF membranes (GE healthcare, USA). After being blocked with 5 % milk for 1 h at room temperature, the membranes were then incubated overnight at 4 °C with anti-SOCS2 (1:500) (Abcam, Cambridge, MA, USA), anti-SOCS6 (1:500) (Abcam, Cambridge, MA, USA) or anti-GAPDH (1:1,000) (Santa Cruz Biotechnology, USA) antibodies. After being washed three times, the protein bands were developed by ECL. To confirm equal loading, GAPDH antibody was served as a control.
Statistical analysis
SPSS13.0 software for Windows (SPSS Inc, USA) was used for statistical analysis. Continuous variables were expressed as \( \overline{X} \pm s \). Paired Student t test was used to compare the expression levels between tumor and para-tumor, tumor and normal liver tissues. Group comparisons of categorical variables were evaluated using the χ2 test. The Spearman rank correlation coefficient was also used to assess the significance of the correlation between mRNA and protein levels of SOCS2 or SOCS6 expression. Kaplan–Meier method was used for the question of survival. Cox proportional hazards regression model was performed for ordinal datum and the multivariate analysis, respectively. The P values of <0.05 were considered to be statistically significant.
Results
Reduced expression of SOCS2 and SOCS6 at mRNA and protein levels in HCC
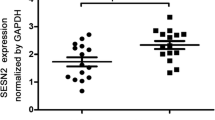
The expression of SOCS2 and SOCS6 at mRNA and protein levels were detected and analyzed in all fresh tissues from 106 HCC patients. The qRT-PCR results (Fig. 1a) showed that both the expression levels of SOCS2 mRNA and SOCS6 mRNA were significantly lower in tumor tissue than those in para-tumor tissue (for SOCS2: 0.8 ± 0.05 vs. 1.2 ± 0.1, P < 0.001; for SOCS6: 0.8 ± 0.08 vs. 1.1 ± 0.1, P < 0.001) and in normal liver tissue (for SOCS2: 0.8 ± 0.05 vs. 1.3 ± 0.1, P < 0.001; for SOCS6: 0.8 ± 0.08 vs. 1.2 ± 0.1, P < 0.001). The differences between para-tumor and normal liver tissues had no statistical significance. In addition, the Western blot analysis (Fig. 1b) of SOCS2 and SOCS6 proteins also showed that the expression of SOCS2 and SOCS6 proteins were significantly lower in tumor tissue than those in para-tumor tissue (for SOCS2: 0.7 ± 0.02 vs. 1.1 ± 0.08, P < 0.001; for SOCS6: 0.8 ± 0.03 vs. 1.2 ± 0.07, P < 0.001) and in normal liver tissue (for SOCS2: 0.7 ± 0.02 vs. 1.2 ± 0.08, P < 0.001; for SOCS6: 0.8 ± 0.03 vs. 1.3 ± 0.1, P < 0.001). Moreover, the Spearman rank correlation analysis showed that the expression level of SOCS2 mRNA was closely correlated with that of SOCS2 protein (Spearman’s r = 0.8; P < 0.001), as well as the correlation between SOCS6 mRNA expression and SOCS6 protein expression (Spearman’s r = 0.8; P < 0.001). Therefore, we chose the expression levels of SOCS2 and SOCS6 proteins to analyze their relationship with clinicopathological characteristics and prognosis in HCC patients.

Expression of SOCS2 and SOCS6 at mRNA (a) and protein (b) levels in tumor (HCC), para-tumor and normal liver tissues
Association of SOCS2 and SOCS6 expression with the clinicopathologic characteristics of HCC
In order to analyze the association of SOCS2 and SOCS6 expression with various clinicopathologic characteristics of HCC patients, we divided 106 HCC patients into four groups according to the expression levels of SOCS2 and SOCS6 proteins. HCC patients expressing SOCS2 protein at levels less than the median expression level (0.8) were assigned to the low SOCS2 expression group (mean expression value 0.6, n = 56), and those samples with expression equal or above the median value were assigned to the high SOCS2 expression group (mean expression value 1.0, n = 50). HCC patients expressing SOCS6 protein at levels less than the median expression level (0.8) were assigned to the low SOCS6 expression group (mean expression value 0.6, n = 58), and those samples with expression equal or above the median value were assigned to the high SOCS2 expression group (mean expression value 1.0, n = 48). As shown in Table 1, both SOCS2 and SOCS6 protein downregulation were significantly correlated with advanced TNM stage (both P < 0.001) and high serum AFP (P = 0.008 and 0.01, respectively). Especially, the reduced expression of SOCS2 more frequently occurred in HCC patients with vascular invasion (P = 0.03), and that of SOCS6 was also associated with tumor recurrence (P = 0.01). There was no significant difference in age, sex, etiology, background liver pathology, Child–Pugh, tumor size, tumor differentiation between the patients’ groups.
Association of SOCS2 and SOCS6 expression with prognosis in patients with HCC
The association of SOCS2 and SOCS6 expression in HCC with the survival of all 106 HCC patients was analyzed with Kaplan–Meier survival analysis. Patients with low expression of SOCS2 and SOCS6 were likely to be with significantly shorter overall survival (P = 0.008 and 0.01, respectively, Fig. 2a, b) and disease-free survival (both P = 0.01, Fig. 2c, d).

Kaplan–Meier survival curves for SOCS2 expression (a for overall survival, b for disease-free survival) and SOCS6 expression (c for overall survival, d for disease-free survival) in HCC tissues
Then, we evaluated the expression of SOCS2 and SOCS6, and other clinicopathologic characteristics on prognosis of HCC using univariate analyses. Results as shown in Table 2 indicated that the expression of SOCS2 (P = 0.008 and 0.01, respectively) and SOCS6 (P = 0.01 and 0.02, respectively), as well as TNM stage (both P = 0.001), serum AFP level (P = 0.01 and 0.02, respectively) and tumor recurrence (P = 0.02 and 0.04, respectively), were significantly associated with overall survival and disease-free survival of HCC patients. It was important to note that, in our series, the expression of SOCS2 predicted the overall and disease-free survival better than serum AFP and tumor recurrence, but poorer than TNM stage. Regarding to SOCS6, its prognostic efficiency was better than tumor recurrence, but poorer than TNM stage and serum AFP.
Furthermore, the expression of SOCS2 and SOCS6, and those clinicopathologic characteristics significant in univariate analysis (TNM stage, serum AFP level and tumor recurrence) were further evaluated in multivariate analysis. Results as shown in Table 3 suggested that the expression of SOCS2 (for overall survival: HR 10.6, 95 % CI 1.3–20.8, P = 0.01; for disease-free survival: HR 11.5, 95 % CI 1.6–21.2, P = 0.01) and SOCS6 (for overall survival: HR 8.5, 95 % CI 1.0–17.3, P = 0.03; for disease-free survival: HR 8.1, 95 % CI 1.3–17.0, P = 0.03) were also independent predictors for overall survival and disease-free survival of HCC patients.
Discussion
HCC is a lethal human malignancy in the worldwide especially in developing countries. The molecular mechanisms of the oncogenic signaling pathways which are involved in liver carcinogenesis play a crucial role in disease progression and persistence. In this study, to elucidate the clinical role of SOCS2 and SOCS6 in HCC, we applied qRT-PCR and Western blot to examine their expression in a cohort of Chinese patients. The significant declines of SOCS2 and SOCS6 expression levels were both observed in HCC tissues, compared with the para-tumor and normal liver tissues. To our knowledge, this is the first study to analyze SOCS2 and SOCS6 expression in HCC at both mRNA and protein levels.
SOCS are known as negative regulators of cytokine- and growth factor-induced signal transduction. Recently, they have emerged as multifunctional proteins with regulatory roles in inflammation, autoimmunity, and cancer. The previous studies have shown the involvement of SOCS1 and SOCS3 in HCC [7, 8]. Until now, research on the relationship between expression status of other SOCSs and the clinicopathological parameters in HCC has not been reported yet. At first, our results demonstrated that the expression of SOCS2 mRNA and protein in HCC tissues were both lower than that in para-tumor and normal liver tissues. Low SOCS2 expression was associated with aggressive clinicopathological characteristics including advanced TNM stage, high serum AFP and positive vascular invasion, and was predicted shorter overall and disease-free survival. After adjusting for TNM stage, serum AFP level, and tumor recurrence, low SOCS2 expression remained an independent predictor for poor prognosis. Similar to our observations, Farabegoli et al. [24] first demonstrated that high SOCS2 protein expression is associated with lower pathological grade and lower cell proliferation indices of breast cancer cells. Then, Haffner et al. [25] reported that high SOCS2 expression in breast cancer tissues was an independent predictor for good prognosis. Hendriksen et al. [26] found that low SOCS2 expression in prostate cancer was associated with an increased incidence of metastasis and SOCS2 mRNA levels decreased during prostate cancer progression. In pulmonary adenocarcinoma, SOCS2 expression was also found to be decreased [14]. Together with our findings of highly significant negative correlation between SOCS2 expression and TNM stage, serum AFP level, vascular invasion status and poor prognosis, these results indicate that SOCS2 may be a marker for various tumors. However, the findings of Raccurt et al. [27], who indicated that SOCS2 expression was higher in cancerous ducts and reactive stroma as compared to normal breast tissues by using in situ hybridization, were not in agreement with our findings. The reason for this difference may be the heterogenicity of different tumors. Regarding to SOCS6, our data showed its downregulation in HCC as compared with para-tumor and normal liver tissues. These results were consistent with previous study [23]. Besides the results mentioned above, the SOCS6 expression data obtained from Western blot analysis showed that low expression of SOCS6 protein in HCC was significantly associated with TNM stage, tumor recurrence and serum AFP. The similar result was observed in gastric cancer, indicating that SOCS6 may be involved in the tumorigenesis and associated with aggressive clinical stage. In the Kaplan–Meier survival analysis, patients with low SOCS6 protein expression had a significant poorer prognosis than patients with high SOCS6 protein expression. Furthermore, multivariate Cox regression analysis indicated that SOCS6 expression level was an independent factor of survival and may constitute a prognostic factor for HCC patients.
In conclusion, our data demonstrate for the first time that SOCS2 and SOCS6 expression were remarkably reduced in HCC and might be served as potential prognostic markers for patients with this deadly disease. However, we believe that the diagnostic and prognostic values of SOCS2 and SOCS6 should be validated by a larger number of cases before using them as markers in practice. Since the investigation into the critical roles of SOCS2 and SOCS6 in tumorigenesis and tumor progression may provide important insight into the malignant process and link deregulation of key signal pathways to HCC, as well as establish new targets for diagnostics of this malignancy, SOCS proteins merit further study with respect to the molecular pathogenesis and control of HCC.
References
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics. CA Cancer J Clin 55:74–108
Bruix J, Sherman M (2005) Management of hepatocellular carcinoma. Hepatology 42:1208–1236
El-Serag HB, Rudolph KL (2007) Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 132:2557–2576
Fujimoto M, Naka T (2003) Regulation of cytokine signaling by SOCS family molecules. Trends Immunol 24:659–666
Kile BT, Schulman BA, Alexander WS, Nicola NA, Martin HM, Hilton DJ (2002) The SOCS box: a tale of destruction and degradation. Trends Biochem Sci 27:235–241
Elliott J, Johnston JA (2004) SOCS: role in inflammation, allergy and homeostasis. Trends Immunol 25:434–440
Okochi O, Hibi K, Sakai M, Inoue S, Takeda S, Kaneko T, Nakao A (2003) Methylation-mediated silencing of SOCS-1 gene in hepatocellular carcinoma derived from cirrhosis. Clin Cancer Res 9:5295–5298
Niwa Y, Kanda H, Shikauchi Y, Saiura A, Matsubara K, Kitagawa T, Yamamoto J, Kubo T, Yoshikawa H (2005) Methylation silencing of SOCS-3 promotes cell growth and migration by enhancing JAK/STAT and FAK signalings in human hepatocellular carcinoma. Oncogene 24:6406–6417
Rico-Bautista E, Flores-Morales A, Fernández-Pérez L (2006) Suppressor of cytokine signaling (SOCS) 2, a protein with multiple functions. Cytokine Growth Factor Rev 17:431–439
Tannahill GM, Elliott J, Barry AC, Hibbert L, Cacalano NA, Johnston JA (2005) SOCS2 can enhance interleukin-2 (IL-2) and IL-3 signaling by accelerating SOCS3 degradation. Mol Cell Biol 25:9115–9126
Jegalian AG, Wu H (2002) Differential roles of SOCS family members in EpoR signal transduction. J Interferon Cytokine Res 22:853–860
Goldshmit Y, Walters CE, Scott HJ, Greenhalgh CJ, Turnley AM (2004) SOCS2 induces neurite outgrowth by regulation of epidermal growth factor receptor activation. J Biol Chem 279:16349–16355
Schultheis B, Carapeti-Marootian M, Hochhaus A, Weisser A, Goldman JM, Melo JV (2002) Overexpression of SOCS-2 in advanced stages of chronic myeloid leukemia: possible inadequacy of a negative feedback mechanism. Blood 99:1766–1775
Wikman H, Kettunen E, Seppanen JK, Karjalainen A, Hollmen J, Anttila S et al (2002) Identification of differentially expressed genes in pulmonary adenocarcinoma by using cDNA array. Oncogene 21:5804–5813
Sutherland KD, Lindeman GJ, Choong DY, Wittlin S, Brentzell L, Phillips W et al (2004) Differential hypermethylation of SOCS genes in ovarian and breast carcinomas. Oncogene 23:7726–7733
Arany I, Muldrow M, Tyring SK (2001) The endogenous interferon system in anal squamous epithelial lesions with different grades from HIV-positive individuals. Int J STD AIDS 12:229–233
Hwang MN, Min CH, Kim HS, Lee H, Yoon KA, Park SY, Lee ES, Yoon S (2007) The nuclear localization of SOCS6 requires the N-terminal region and negatively regulates Stat3 protein levels. Biochem Biophys Res Commun 360:333–338
Wang T, Gao Q, Nie P, Secombes CJ (2010) Identification of suppressor of cytokine signalling (SOCS) 6, 7, 9 and CISH in rainbow trout Oncorhynchus mykiss and analysis of their expression in relation to other known trout SOCS. Fish Shellfish Immunol 29:656–667
Lin HY, Lai RH, Lin ST, Lin RC, Wang MJ, Lin CC, Lee HC, Wang FF, Chen JY (2013) Suppressor of cytokine signaling 6 (SOCS6) promotes mitochondrial fission via regulating DRP1 translocation. Cell Death Differ 20:139–153
Sriram KB, Larsen JE, Savarimuthu Francis SM, Wright CM, Clarke BE, Duhig EE, Brown KM, Hayward NK, Yang IA, Bowman RV, Fong KM (2012) Array-comparative genomic hybridization reveals loss of SOCS6 is associated with poor prognosis in primary lung squamous cell carcinoma. PLoS ONE 7:e30398
Storojeva I, Boulay JL, Ballabeni P, Buess M, Terracciano L, Laffer U, Mild G, Herrmann R, Rochlitz C (2005) Prognostic and predictive relevance of DNAM-1, SOCS6 and CADH-7 genes on chromosome 18q in colorectal cancer. Oncology 68:246–255
Lai RH, Hsiao YW, Wang MJ, Lin HY, Wu CW, Chi CW, Li AF, Jou YS, Chen JY (2010) SOCS6, down-regulated in gastric cancer, inhibits cell proliferation and colony formation. Cancer Lett 288:75–85
Yoon S, Yi YS, Kim SS, Kim JH, Park WS, Nam SW (2012) SOCS5 and SOCS6 have similar expression patterns in normal and cancer tissues. Tumour Biol 33:215–221
Farabegoli F, Ceccarelli C, Santini D, Taffurelli M (2005) Suppressor of cytokine signalling 2 (SOCS-2) expression in breast carcinoma. J Clin Pathol 58:1046–1050
Haffner MC, Petridou B, Peyrat JP, Révillion F, Müller-Holzner E, Daxenbichler G, Marth C, Doppler W (2007) Favorable prognostic value of SOCS2 and IGF-I in breast cancer. BMC Cancer 7:136
Hendriksen PJ, Dits NF, Kokame K, Veldhoven A, van Weerden WM, Bangma CH, Trapman J, Jenster G (2006) Evolution of the androgen receptor pathway during progression of prostate cancer. Cancer Res 66:5012–5020
Raccurt M, Tam SP, Lau P, Mertani HC, Lambert A, Garcia-Caballero T, Li H, Brown RJ, McGuckin MA, Morel G, Waters MJ (2003) Suppressor of cytokine signalling gene expression is elevated in breast carcinoma. Br J Cancer 89:524–532
Author information
Authors and Affiliations
Corresponding authors
Additional information
Xinyu Qiu and Jianyong Zheng offer the equal contribution to this study.
Rights and permissions
About this article
Cite this article
Qiu, X., Zheng, J., Guo, X. et al. Reduced expression of SOCS2 and SOCS6 in hepatocellular carcinoma correlates with aggressive tumor progression and poor prognosis. Mol Cell Biochem 378, 99–106 (2013). https://doi.org/10.1007/s11010-013-1599-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-013-1599-5