
Abstract
Insulin resistance has been shown to be the major contributing factor to the metabolic syndrome, which comprises a cluster of risk factors for metabolic aberrations such as obesity, dyslipidemia, hypertension, and hyperglycemia. Additionally, insulin resistance has been associated with the occurrence of cardiovascular disease and type 2 diabetes. Epidemiological studies indicate that obesity and diabetes have become alarmingly prevalent in recent years. Substantial evidence suggests that dietary interventions and regular exercise greatly improve body mass index and lipid profile as well as alleviate insulin resistance. Therefore, dietary supplements such as insulin-sensitizing agents may be beneficial in the prevention and treatment of obesity and type 2 diabetes. Numerous in vitro and in vivo studies suggest that chromium supplements, particularly niacin-bound chromium or chromium-nicotinate, may be effective in attenuating insulin resistance and lowering plasma cholesterol levels. Utilizing the powerful technology of nutrigenomics to identify the genes regulated by chromium supplementation may shed some light on the underlying mechanisms of chromium-gene interactions, and thus provide strategies to mitigate and prevent insulin-resistance-related disorders.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
It is estimated that in developed countries up to 35% of the population have one or more attributes of insulin resistance, the major contributing factor of metabolic syndrome (MS) [1]. Insulin-resistance-related disorders such as type 2 diabetes mellitus (T2D) and obesity have reached epidemic proportions in the recent years [2]. These emerging epidemics are exacerbated by the expansion of the aged population because aging facilitates aberrant insulin regulations [3, 4]. It is predicted that the aged population will increase to 32% (currently at 18%) by the year 2050 [5]. To alleviate the socioeconomic burden inflicted by insulin-resistance-related disorders as well as increase the health-related quality of life among the ever-growing aging population, it is of great importance to explore means to forestall or prevent these diseases.
Studies have shown that suboptimal intake of chromium(III) is a major contributing factor for chronic diseases such as T2D and cardiovascular diseases (CVD) [6]. Chromium deficiency resulting from suboptimal diet has been shown to augment the MS-associated risk factors such as elevated levels of blood glucose, circulating insulin, cholesterol and triglycerides, and decreased lean body mass [7]. However, these conditions are readily correctable by chromium supplementation [6, 8]. Indeed, chromium was first identified five decades ago as an essential trace element required to maintain normal glucose tolerance and thus termed “glucose tolerance factor” (GTF) based on its biological function [9, 10]. Therefore, chromium supplementation may present a key factor for the intervention of MS-related diseases.
Chromium valence states and biological activity
Chromium is a transition metal with valence states ranging from −2 to +6 [11]. The biological activity of chromium is conferred by its valence state. The common stable valence forms include the inert metallic chromium Cr(0), trivalent chromium Cr(III), and hexavalent chromium Cr(VI) [12, 13]. Cr(VI) is commonly found in industrial chemicals used in stainless steel manufacture, metal finishing and chrome plating, welding, pigment production, leather tanning, wood preservatives, and as corrosion inhibitors [12, 14]. Studies have shown that Cr(VI) is a potent carcinogen and a respiratory irritant which causes lipid peroxidation, DNA damage, cell death [7, 14]. Cr(III), on the other hand, is an essential micronutrient that is required for normal carbohydrate, protein, and lipid metabolism, and enhanced glucose-insulin sensitivity [6]. Although the underlying mechanism by which Cr(III) exerts its beneficial effects remain unclear, numerous in vitro and in vivo studies have indicated that Cr(III) plays an important role in the maintenance of normal blood glucose level, the reduction of plasma cholesterol and triglycerides, and the inhibition of oxidative stress and inflammatory cytokine secretion [15].
Dietary sources and daily intake
Dietary sources of Cr(III) include seafood, oysters, meat, liver, cheese, whole grains, fruits, green beans, spinach, and broccoli. Brewer’s yeast, identified as a source of GTF, is particularly enriched in organic Cr(III) ligand complexes [10]. It has been used in numerous studies to isolate and characterize the organic ligand component(s) of GTF [16]. Subsequently, it has been proposed that the naturally occurring GTF is a complex of Cr(III), nicotinate, and glutathione based on its similar biological activity to GTF found in Brewer’s yeast and its ability to bind tightly to insulin [17]. Therefore, Cr(III) nicotinate (NBC) and other Cr(III) complexes have been synthesized and widely used as dietary supplements [18].
The Estimated Safe and Adequate Daily Dietary Intake (ESADDI) for Cr(III) established by the National Research Council (NRC) is 50–200 μg/day which corresponds to 0.71–2.9 μg/kg/day for a 70 kg adult [19, 20]. A comparable Reference Daily Intake (RDI) for Cr was set at 120 μg/day by the Food and Drug Administration (FDA) [21].
Bioavailability, deficiency, and diseases
Chromium bioavailability is highly dependent on the nature of the Cr(III) ligand complexes ingested or formed in vivo [22–24]. For instance, the inorganic form of Cr(III) chloride (CrCl3) complex has been shown to be excreted more quickly than its organic counterparts such as niacin-bound Cr(III) (NBC) and Cr(III) picolinate (CrPic) [23, 25]. Indeed, an in vivo study comparing the absorption and retention of CrCl3, CrPic, and NBC has revealed that there were significant differences in the bioavailability of these three Cr complexes [25]. This study measured the absorption and retention of radiolabeled 51Cr over a period of 12 h post-ingestion. The average percent 51Cr retained in the majority of the fluids and tissues over the 12-h time course was significantly higher in rats gavaged with NBC than those with CrCl3 and CrPic [25].
The mode of Cr(III) absorption and transport has recently been reported [26]. It has been shown that Cr(III) is absorbed by the gastrointestinal tract, bound by transferrin in the bloodstream, and then transferred to various tissues in the transferring-bound state. The major Cr(III) target tissues have been identified as liver and kidneys [27]. Cr(III) is released and processed intracellularly after transport to tissues by transferrin. A portion of the transferred Cr(III) is bound to low-molecular weight chromium-binding substances (LMWCr) or chromodulins [28, 29]. LMWCr is a mammalian oligopeptide of approximately 1.5 kDa that binds four chromic ions [30–32]. The LMWCr-bound chromium is expelled from cells into the bloodstream and then excreted in the urine [26, 27]. Insulin has been shown to stimulate intracellular processing of Cr(III), thus confirming the connection between chromium and insulin signaling [33–35].
The average dietary Cr(III) intake for adults is generally lower than the minimum suggested daily Cr(III) intake of 50 μg [36, 37]. In fact, up to 90% of the US population failed to meet the minimum ESADDI [32]. This problem is exacerbated by the fact that Cr(III) is poorly absorbed. While other essential trace metals such as copper, iron, and zinc are absorbed on the order of 10–40%, Cr(III) is absorbed 0.5–2% depending on dietary intake [36]. Even a well-balanced meal formulated by nutritionists does not provide the minimum suggested daily Cr(III) intake [6]. Chromium deficiency is particularly prevalent in certain demographics such as athletes, pregnant women, and the elderly [38]. This is due to enhanced chromium loss resulting from strenuous exercise, long periods of stress during pregnancy, and age-related inability to efficiently absorb or convert inorganic chromium into the active form [39, 40]. Further chromium losses are attributed to consuming refined foods, especially those enriched in simple sugars, because these foods are not only low in chromium but they also facilitate chromium loss through urine excretion [33, 41].
The common indications of chromium deficiency in humans include insulin resistance, hyperglycemia, and lipid abnormalities [24, 42, 43]. Severe chromium deficiency arose in patients receiving total parenteral nutrition (TPN) without chromium supplementation [44]. These patients developed diabetic-like symptoms such as glucose intolerance, weight loss, and neuropathy. However, these symptoms were reversed by chromium supplementation [45, 46]. Therefore, chromium is now included in TPN solutions [47].
Animal studies have shown that rats on a chromium deficient diet developed aortic plaques and elevated blood cholesterol. These abnormalities were abolished upon chromium supplementation [48]. The beneficial effects of supplemental chromium have also been reported in other animals such as mice, monkeys, pigs, cattle, and horses [42, 49].
Supplementation, safety, and efficacy
Cr(III) dietary supplements exist mainly in the form of CrCl3, CrPic, and the oxygen-coordinated niacin-bound chromium or NBC [13, 48]. A substantial number of studies have devoted to evaluating the safety and efficacy of these Cr(III) supplements.
There has been in vitro evidence demonstrating that CrPic was genotoxic and caused mutation at the hypoxanthine (guanine) phosphoribosyltransferase locus of the Chinese hamster ovary (CHO) cells [50, 51]. CrPic has also been shown to induce clastogenesis or chromosomal damage in CHO cells whereas at the same physiologic dose neither CrCl3 nor NBC incurred any clastogenic effect [52]. Since the clastogenic effect only occurred in CrPic and picolinic acid but not in CrCl3, NBC, or nicotinic acid, it was concluded that the observed clastogenicity was induced by picolinic acid and not by chromium per se [53]. In fact, several clinical cases have linked CrPic to nephrotoxicity resulting in renal failure [54, 55].
On the other hand, numerous studies on the safety of NBC have generally shown that there is no toxic effect associated with NBC [56, 57]. A comprehensive pharmacotoxicology rodent study has been conducted to evaluate the safety of NBC [56]. Acute oral and dermal toxicity as well as primary dermal and eye irritation studies have not produced any signs of toxicity or irritation induced by NBC. Ames bacterial reverse mutation and mouse lymphoma mutagenicity assays have shown that NBC was non-mutagenic. A 90-day subchronic toxicity study has not shown any toxicological effects of NBC [56]. A recent long-term safety study has revealed that rats orally administered with a human equivalent dose of 1,000 μg/day elemental Cr(III) in the form of NBC for a duration of 52 weeks showed no signs of NBC-induced toxicological effects [57]. Specifically, the results from this study have indicated that there were no significant changes in hepatic lipid peroxidation and DNA fragmentation, hematology and clinical chemistry, and histopathological parameters examined [57].
Clinical records have revealed no evidence of toxicity in patients receiving Cr(III)-supplemented TPN for more than 20 years [24]. Human clinical studies have generally demonstrated evidence of efficacy for Cr(III) supplementation in improving insulin sensitivity and/or blood lipid profiles [58].
Chromium interventions in metabolic syndrome, obesity, and diabetes
Metabolic syndrome, also known as the “insulin resistance syndrome” or “syndrome X,” is associated with cellular deregulation of insulin action [59, 60]. Insulin resistance occurs when the ability of insulin to stimulate glucose metabolism is disrupted resulting in high levels of glucose and insulin in the blood. Insulin signaling transduction pathways in adipose and muscle cells are intricate processes involving binding of insulin to its receptor, activation of kinases, and caveolin-mediated translocation of glucose transporter 4 (GLUT4) leading to the uptake of glucose [61–63]. A major characteristic of insulin resistance is the reduction in the insulin-regulated, GLUT4-mediated glucose uptake in adipocytes and muscle cell [64]. A recent study showed that NBC supplementation increased the phosphorylation of AMP-activated protein kinase (AMPK) and endothelial nitric oxide synthase (eNOS) as well as facilitated the translocation of GLUT4 to the cell membrane through regulation of caveolins in streptozotocin-induced diabetic rats [65]. This study presented for the first time a novel mechanism by which NBC mediates glucose uptake, hence further supported the beneficial effects of NBC as observed in numerous animal and human studies.
It is estimated that MS-associated factors are present in 25–35% of the population in Western countries [1]. MS is characterized by increased plasma triglyceride level accompanied by a reduced high-density lipoprotein (HDL) leading to perturbed insulin signal transduction [66]. Impairment in insulin signaling increases cardiovascular risk factors and contributes to diseases such as atherosclerosis and type 2 diabetes (T2D) [4, 67]. It has been shown that obesity correlates positively with the prevalence of MS [68]. While MS was present in 4.6% of normal weight and 22.4% of overweight men, it was present in an astounding 59.6% of obese men [68].
Obesity is a multifactoral chronic condition that is characterized by an excess of body adiposity resulting from tipping the balance between caloric intake and energy expenditure in favor of the former [69, 70]. Clinically obesity is defined as a body mass index (BMI) greater than 30 kg/m2, whereas overweight is defined as a BMI greater than 25 kg/m2 [71]. According to these definitions, the number of overweight or obese adult Americans has recently surpassed the number of normal weight adult Americans for the first time in history [72, 73]. Obesity is also a major risk factor for T2D [74, 75]. Diabetes is the most prevalent endocrine disorder affecting more than 170 million people globally, and this number is expected to double in the year of 2030 [63]. T2D is the most common form of diabetes accounting for more than 90% of the diabetic patients [63]. It is not surprising, then, to find that the prevalence of obesity paralleled that of T2D in recent years to reach epidemic proportions [2]. This alarming phenomenon imposes a tremendous burden on the health care resources. Unless preventive measures are taken to forestall this global epidemic, it will get worse in the years to come. The current strategies used to treat obesity and T2D include pharmacotherapy, dietary interventions, and lifestyle modifications [76, 77].
Since its identification as the central component of the GTF 50 years ago, trivalent chromium has been widely used in dietary interventions to improve insulin sensitivity and to curb weight gains [8]. Numerous studies have provided evidence of efficacy that Cr(III) supplementation is beneficial in maintaining healthy carbohydrate and lipid metabolism, regulating appetite and reducing sugar cravings, and reducing fat mass and increasing lean body mass [48].
To evaluate the effect of Cr(III) supplementation combined with exercise on weight management, Grant et al. conducted a clinical study involving 43 young, healthy sedentary, obese women for a period of 9 weeks [78]. The subjects were divided into four groups: CrPic supplemented without exercise (CP), exercise training with CrPic-supplemented (E/CP), exercise training with placebo (E/P), and exercise training with NBC-supplemented (E/CN) [78]. Chromium supplements were taken orally twice a day as 200 μg tablets for a total of 400 μg/day for those receiving chromium supplements. The placebo tablets contained inert ingredients. The results revealed that not only was CrPic ineffective in reducing weight, it actually increased the body weight in the CP group [78]. No significant changes in body weight were observed in the E/P or E/CP groups. On the contrary, E/CN group showed a significant weight loss and a significant lowered insulin response to an oral glucose load indicating for the first time that combining with exercise, NBC was effective in promoting weight loss and reducing certain CVD and T2D risk factors [78].
A subsequent clinical study has shown that oral intake of 600 μg/day NBC over a two-month period by African-American women who were undergoing a modest dietary and exercise regimen resulted in a significant fat loss without affecting muscle mass [79]. Blood chemistry analysis indicated no perturbations or adverse effects from daily intake of 600 μg of NBC for 2 months [79].
A growing body of evidence has demonstrated that chromium may play an important role in preventing atherosclerosis and CVD by reducing plaque buildup in the arteries, lowering total cholesterol (TC), low-density lipoprotein (LDL), and triglyceride levels [80–84]. Furthermore, a number of human studies have provided evidence to suggest that chromium supplementation may be beneficial for patients with T2D and gestational diabetes [85–88].
Numerous studies have reported efficacy of NBC supplementation on glucose and insulin regulation [8, 48]. A randomized, double-blind, placebo-controlled study has been carried out to investigate the effect of NBC supplementation on insulin sensitivity [89]. Twenty-six subclinical chromium deficient, otherwise healthy young adults were randomly assigned to the placebo group (n = 11) or the Cr-supplemented group (n = 15) receiving 220 μg/day elemental Cr(III) in the form of NBC. Although there was no significant difference in the percent change of fasting immunoreactive insulin (IRI) level between the placebo group and the Cr-supplemented group at the conclusion of the trial, the subjects within the Cr-supplemented group (n = 6) with high initial fasting IRI levels (56 pmol/l) exhibited a statistically significant decrease in IRI level (38 pmol/l) after 90 days of supplementation. The results suggested that NBC supplementation may benefit these subjects by improving insulin sensitivity over time [89].
Another double-blind clinical trial has been carried out to evaluate the efficacy of NBC on blood glucose and triglyceride parameters [90]. Twenty volunteers received either a daily dose of 300 μg elemental Cr(III) in the form of NBC or a placebo for 3 months. The mean fasting glucose levels in the NBC-supplemented group were lowered significantly, while glucose levels remained unchanged in the placebo group. NBC supplementation also attenuated the mean blood triglycerides and glycosylated hemoglobin (Hb1Ac), a biomarker for long-term glucose control [90].
Although evidence supports the use of Cr(III) especially in the form of NBC in promoting insulin sensitivity, healthy blood glucose, and weight loss, there exists controversy as to which form of Cr(III) is beneficial. In a 6-month randomized, double-blind, placebo-controlled clinical trial, Cr(III) in the form of CrPic was given to overweight patients with T2D who received more than 50 units of insulin daily and was found to be ineffective in improving lipid profile, BMI, blood pressure, and insulin requirements [91]. Subsequently, the same research group conducted a similar study using Cr(III) in the form of chromium yeast showed no evidence that treatment with chromium yeast was effective in improving glycemic control in T2D patients [92]. The effect of high dose CrPic supplementation on middle-aged healthy subjects of normal body weight and BMI with T2D was evaluated and the results showed improved glucose and insulin metabolism [86]. The result of this study may have been confounded by the fact that the subjects were taking various medications including sulfonylurea drugs, phenformin, and insulin. Several patients were taking more than one medication [86]. Even though no significant toxic effects have been observed in the inorganic CrCl3, it is poorly absorbed by the body and may not be an efficacious Cr(III) dietary supplement [15, 93]. However, available evidence suggests that supplemental Cr(III) in the form of NBC is more bioavailable, efficacious, and safe. Therefore, the chromium controversy seems to have arisen from the dispute of which form of chromium is more effective [76].
Chromium(III) and gene regulation: nutrigenomics approach
The underlying mechanism for the observed beneficial effects of chromium remains to be elucidated. With the completion of the Human Genome Project, a new wave of powerful multidisciplinary technologies has emerged for the study of diet-gene interactions in the field of nutraceutical research [72, 94]. Nutrigenomics is a genome-wide high-throughput screening (HTS) technology applied to investigate how diets affect gene expression patterns (transcriptome) [95, 96].
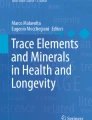
A recent study has utilized the nutrigenomics approach to investigate the effect of oral niacin-bound chromium (NBC) supplementation on the transcriptome of subcutaneous adipose tissues from obese mice homozygous for type 2 diabetes spontaneous mutation (Lepr db) [97]. Male Lepr db mice were randomly divided into the NBC-supplemented (n = 7, NBC) or placebo (n = 7, PBO) group. Supplementation regimen began when the mice were 10 week of age and lasted for a period of 10 weeks. Lipid profiles were analyzed at week 6 post-supplementation and the results were compared to baseline data collected at week 0 presupplementation. Parameters assessed included blood glucose level, TC, HDL cholesterol (HDLC), triglycerides, LDL, and the TC-to-HDLC ratio. Oral glucose tolerance test (OGTT) was carried out at week 8 post-supplementation. Mice were euthanized at week 10 post-supplementation. Subcutaneous fat was extracted from the mice for isolation of total RNA, which was used for the high-density comprehensive mouse genome (45,101 probe sets) expression microarrays [97]. Blood lipid profile indicated that NBC supplementation significantly lowered TC, TC-to-HDLC ratio, LDL cholesterol, and triglyceride levels while increased HDLC in the plasma of these obese diabetic mice (Fig. 1). OGTT demonstrated a significant improvement on the clearance of blood glucose between one- and two-hour of glucose challenge in the NBC group as compared to that in the PBO group. These findings are consistent with the beneficial effects of NBC on glucose and lipid metabolism observed previously in other human and animal studies [97].

Improvement of plasma lipid profiles by NBC supplementation in type 2 diabetic rats. Lipid profiles in placebo-fed and NBC-fed type 2 diabetic rats were analyzed at week 6 post-supplementation and results were expressed in percentage of placebo [97]. Data indicate mean ± SD with n = 7 per group. *P < 0.005, indicates statistical significance as compared to the placebo group
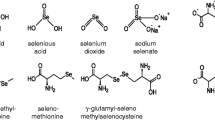
To delineate the underlying physiological benefits of NBC in the current study, the effect of NBC supplementation on the transcriptome of subcutaneous fat of these obese diabetic mice was screened by high-throughput whole mouse genome expression microarrays. Unbiased genome-wide interrogation of the transcriptome revealed, for the first time, that NBC supplementation consistently altered the expression of a small subset (approximately 0.61%) of the 41,101 probe sets in the adipose tissues of the obese diabetic rats. NBC supplementation exerted a positive effect on the transcriptome of fat tissues with more up-regulated genes. Specifically, while there were 161 genes up-regulated, only 91 genes were suppressed by NBC supplementation. The results indicated a specific effect of chromium-gene regulation rather than a random, genome-wide perturbation caused by the supplement [97]. Selected candidate genes with a significant fold change ≥1.2 from microarray screening (Fig. 2) were further verified by real-time RT-PCR analysis. The genes that were up-regulated in the fat tissue by NBC supplementation were mostly the muscle-specific genes such as those involved in glycolysis, muscle contraction, muscle metabolism, and muscle development (Table 1). These findings are of great importance because studies have shown that adipocytes and skeletal myoblasts are derived from a common mesodermal stem cell lineage and that preadipocytes may differentiate into myogenic lineage [98, 99]. Adipose tissue contains pluripotent cells; in addition, mesenchymal cells isolated from adipose tissue can differentiate along other cell lineages including osteogenic, chondrogenic, and myogenic lineages [100]. Therefore, adipose tissues are capable of differentiating into myocytes if they are instructed to do so by myogenic signals.

Selected candidate genes from microarray analysis. Differential gene expression in the adipose tissue of placebo- or NBC-treated obese diabetic mice was analyzed with Affymatrix mouse genome microarray (430 v2.0). Selected candidate genes with a fold change ≥1.2 were chosen for further verification by real-time RT-PCR analysis. The expression of genes depicted in the graph exhibited a significant change induced by NBC supplementation when compared to that by placebo supplementation as confirmed by real-time RT-PCR (P ≤ 0.05). Data represent average fold change ± SD (n = 4) of genes which were up-regulated (■) or down-regulated (□) by NBC-supplementation. Refer to Table 1 for abbreviation of genes [97]
Enolase 3 (ENO3) was the most NBC-sensitive gene up-regulated in the fat tissues of the obese diabetic mice. Enolase is a dimeric glycolytic enzyme that catalyzed the interconversion of 2-phosphoglycerate and phosphoenolpyruvate. ENO3 encodes for the β-enolase subunit which accounts for more than 90% of the enolase activity in adult human muscle [101]. A clinical study has indicated that a patient with mutation in the ENO3 gene, which resulted in reduced level of β-enolase enzyme in the muscle, exhibited exercise intolerance and myalgia. Ultrastructural analysis has revealed focal sarcoplasmic accumulation of glycogen beta particles in the patient that may lead to metabolic myopathy caused by defects in distal glycolysis [101]. The glucose phosphate isomerase 1 (GPI1) gene, which is also involved in glycolysis, was found to be up-regulated in the adipose tissue of the NBC-supplemented obese diabetic mice. GPI1 gene product is a multifunctional protein also known as autocrine motility factor (AMF), neuroleukin, and differentiation and maturation mediator [102, 103]. GPI1 protein catalyzes the interconversion of glucose-6-phosphate to fructose-6-phosphate. It is involved in both glycolysis and glucogenesis [104]. Glycolytic genes such as ENO3 and GPI have been found to be down-regulated in the visceral adipose tissues of morbidly obese individuals [105]. Thus, the current study suggests that NBC supplementation facilitates the homeostasis of glycolysis through up-regulation of ENO3 and GPI1 in the obese diabetic mice.
It has been shown that glucose transport and metabolism to glucose-6-phosphate are essential for insulin regulation of calcium homeostasis in vascular smooth-muscle cells (VSMC) through a glucose-6-phosphate-dependent carbohydrate-responsive element in the calcium-ATPase gene [106]. Bioactive Cr(III) has been linked to the enhancement of VSMC calcium transport by stimulating plasmalemmal calcium-ATPase mRNA and protein expression [107]. The current study showed that calsequestrin expression was induced by NBC supplement. Since calsequestrin is the most abundant calcium-binding protein responsible for calcium storage in the sarcoplasmic reticulum and that elevated intracellular free calcium level has been observed in adipocytes, it is plausible to speculate that NBC supplementation decreases the free intracellular calcium level by increasing the levels of calsequestrins [108]. The expression of tropomyosin-1 (TPM1) was up-regulated by NBC supplementation. TPM1 encodes for the α-subunit of the tropomyosin family of proteins. Calcium influx from sarcoplasmic reticulum facilitates tropomyosin-coordinated muscle contraction [109–111]. It has been demonstrated that differentiation of preadipocytes into adipocytes is accompanied by a gradual decrease in the expression of extracellular matrix and cytoskeletal proteins such as fibronectin and tropomyosin [112]. Expression of these up-regulated NBC-specific myogenic genes in adipocytes over time has been shown to diminish the fat content of these fat cells [113].
The NBC-suppressed genes included cell-death-induced DNA fragmentation factor (CIDEA), thermogenic uncoupled protein 1 (UCP1), and tocopherol transfer protein (TTP) (Table 1). It has been revealed that CIDEA is expressed at high levels in brown adipose tissue (BAT), which is the major site of adaptive thermogenesis [114]. Mice deficient in CIDEA are lean and resistant to diet-induced obesity and diabetes [115]. These CIDEA-knockout mice exhibit higher metabolic rate and lipolysis in BAT suggesting a functional role for CIDEA in modulating energy balance and adiposity [115]. UPC1 is another NBC-suppressed gene that is otherwise highly expressed in BAT [116]. Indeed, ultrastructural analysis indicates that brown adipocytes contain numerous large mitochondria packed with UCP1 [116]. UPC1 has been found to mediate the thermogenic activity of BAT and impaired BAT activity has been proposed to play an important role in the development of obesity [114]. TTP is involved in the transport of α-tocopherol (vitamin E) from hepatocytes to peripheral tissues including adipose tissues which serve as the major α-tocopherol storage [117]. Vitamin E readily interconverts and equilibrates between lipoproteins and TTP is likely to be responsible for the incorporation of α-tocopherol into LDLs such that TTP facilitates the preferential enrichment of LDL with α-tocopherol [118, 119]. Down-regulation of TTP by NBC supplementation is expected to reduce the level of LDL in the adipose tissues. Interestingly, the lipid profile analysis revealed that LDL levels in the plasma of NBC-treated obese diabetic mice were significantly reduced (Fig. 1). Since α-tocopherol severs as potent antioxidant, down-regulation of TTP may decrease the lipid-phase antioxidant defense in the adipose tissue thereby facilitating adipose tissue breakdown [97]. Taken together, the nutrigenomics data suggest that NBC exerts its beneficial effects through regulation of specific genes in the fat cells of obese diabetic mice. Thus the current study paved the way for future nutrigenomic investigations of the possible molecular basis of chromium-gene interactions.
Conclusion
Accumulating evidence over the past five decades has established that chromium supplementation is beneficial in lowering blood pressure and plasma cholesterols, enhancing insulin sensitivity, facilitating weight loss, increasing lean body mass, and reducing MS-related risk factors. Even though unequivocal research results indicate an important role of chromium in the intervention of CVD and T2D as well as other MS-related conditions, it is only until recently that the molecular mechanism behind the beneficial effects of chromium has begun to come to light [120]. Using the powerful tool of nutrigenomics, it is possible to identify candidate genes that are regulated by chromium supplementation. The physiologic nutrigenomic study by Rink et al. clearly offers a working basis for the elucidation of chromium-gene regulation in mammalian biological systems and provides strategies to identify novel targets for weight intervention by Cr(III) supplementation [97].
References
Grimm JJ (1999) Interaction of physical activity and diet: implications for insulin-glucose dynamics. Public Health Nutr 2:363–368
Banegas JR, Lopez-Garcia E, Graciani A, Guallar-Castillon P, Gutierrez-Fisac JL, Alonso J, Rodriguez-Artalejo F (2007) Relationship between obesity, hypertension and diabetes, and health-related quality of life among the elderly. Eur J Cardiovasc Prev Rehabil 14:456–462
Preuss HG (1997) Effects of glucose/insulin perturbations on aging and chronic disorders of aging: the evidence. J Am Coll Nutr 16:397–403
Day C (2007) Metabolic syndrome, or what you will: definitions and epidemiology. Diab Vasc Dis Res 4:32–38
United Nations (2005): World population prospects: the 2004 Review. Department of Economic and Social Affairs, Population Division. United Nations, New York
Preuss HG, Anderson RA (1998) Chromium update: examining recent literature 1997–1998. Curr Opin Clin Nutr Metab Care 1:509–512
Zafra-Stone S, Yasmin T, Bagchi M, Chatterjee A, Vinson JA, Bagchi D (2007) Berry anthocyanins as novel antioxidants in human health and disease prevention. Mol Nutr Food Res 51:675–683
Bagchi M, Preuss HG, Zafra-Stone S, Bagchi D (2007) Chromium (III) in promoting weight loss and lean body mass. In: Bagchi D, Preuss HG (eds) Obesity: epidemiology, pathophysiology, and prevention. CRC Press, Boca Raton, pp 339–347
Schwarz K, Mertz W (1957) A glucose tolerance factor and its differentiation from factor 3. Arch Biochem Biophys 72:515–518
Schwarz K, Mertz W (1959) Chromium(III) and the glucose tolerance factor. Arch Biochem Biophys 85:292–295
Sawyer HJ (1994) Chromium and its compounds. In: Zenz C, Dickerson OB, Horvath EP (eds) Occupational medicine. Mosby-Year Book Inc., St Louis, pp 487–495
Stohs SJ, Bagchi D (1995) Oxidative mechanisms in the toxicity of metal ions. Free Radic Biol Med 18:321–336
Porter DJ, Raymond LW, Anastasio GD (1999) Chromium: friend or foe? Arch Fam Med 8:386–390
Costa M (1997) Toxicity and carcinogenicity of Cr(VI) in animal models and humans. Crit Rev Toxicol 27:431–442
Jain SK, Rains JL, Croad JL (2007) High glucose and ketosis (acetoacetate) increases, and chromium niacinate decreases, IL-6, IL-8, and MCP-1 secretion and oxidative stress in U937 monocytes. Antioxid Redox Signal 9:1581–1590
Evans GW, Roginski EE, Mertz W (1973) Interaction of the glucose tolerance factor (GTF) with insulin. Biochem Biophys Res Commun 50:718–722
Toepfer EW, Mertz W, Polansky MM, Roginski EE, Wolf WR (1976) Preparation of chromium-containing material of glucose tolerance factor activity from brewer’s yeast extracts and by synthesis. J Agric Food Chem 25:162–166
Vincent JB, Stallings D (2007) Introduction: a history of chromium studies (1955–1995). In: Vincent JB (ed) The nutritional biochemistry of chromium(III). Elsevier, Amsterdam, pp 1–40
NRC (1989) Recommended dietary allowance. National Academy Press, Washington D.C., pp 241–243
EPA (1998) Toxicological review of trivalent chromium. U.S. Environmental Protection Agency, Washington D.C., pp 7–8
FDA (1995) Food labeling: reference daily intakes, final rule. The Food and Drug Administration, pp 67164–67175
Mertz W (1975) Effects and metabolism of glucose tolerance factor. Nutr Rev 33:129–135
Kerger BD, Paustenbach DJ, Corbett GE, Finley BL (1996) Absorption and elimination of trivalent and hexavalent chromium in humans following ingestion of a bolus dose in drinking water. Toxicol Appl Pharmacol 141:145–158
Jeejeebhoy KN (1999) The role of chromium in nutrition and therapeutics and as a potential toxin. Nutr Rev 57:329–335
Olin KL, Stearns DM, Armstrong WH, Keen CL (1994) Comparative retention/absorption of 51chromium (51Cr) from 51Cr chloride, 51Cr nicotinate and 51Cr picolinate in a rat model. Trace Elem Electrolytes 11:182–186
Clodfelder BJ, Vincent JB (2005) The time-dependent transport of chromium in adult rats from the bloodstream to the urine. J Biol Inorg Chem 10:383–393
Clodfelder BJ, Emamaullee J, Hepburn DD, Chakov NE, Nettles HS, Vincent JB (2001) The trail of chromium(III) in vivo from the blood to the urine: the roles of transferrin and chromodulin. J Biol Inorg Chem 6:608–617
Yamamoto A, Wada O, Ono T (1987) Isolation of a biologically active low-molecular-mass chromium compound from rabbit liver. Eur J Biochem 165:627–631
Davis CM, Vincent JB (1997) Isolation and characterization of a biologically active chromium oligopeptide from bovine liver. Arch Biochem Biophys 339:335–343
Yamamoto A, Wada O, Ono T (1981) A low-molecular-weight, chromium-binding substance in mammals. Toxicol Appl Pharmacol 59:515–523
Davis CM, Vincent JB (1997) Chromium oligopeptide activates insulin receptor tyrosine kinase activity. Biochemistry 36:4382–4385
Davis CM, Vincent JB (1997) Chromium in carbohydrate and lipid metabolism. J Biol Inorg Chem 2:675–679
Mertz W (1969) Chromium occurrence and function in biological systems. Physiol Rev 49:163–239
Morris BW, Blumsohn A, Mac Neil S, Gray TA (1992) The trace element chromium – a role in glucose homeostasis. Am J Clin Nutr 55:989–991
Vincent JB (1994) Relationship between glucose tolerance factor and low-molecular-weight chromium-binding substance. J Nutr 124:117–119
Anderson RA, Kozlovsky AS (1985) Chromium intake, absorption and excretion of subjects consuming self-selected diets. Am J Clin Nutr 41:1177–1183
Anderson RA (1997) Chromium as an essential nutrient for humans. Regul Toxicol Pharmacol 26:S35–S41
Offenbacher EG, Pi-Sunyer FX (1980) Beneficial effect of chromium-rich yeast on glucose tolerance and blood lipids in elderly subjects. Diabetes 29:919–925
Shapcott D, Hubert J (1979) Chromium in nutrition and metabolism. In: Proceedings of the symposium on chromium in nutrition and metabolism, held in Sherbrooke, Canada on July 13–15, 1979. Elsevier/North-Holland Biomedical Press, Amsterdam
Lefavi RG, Anderson RA, Keith RE, Wilson GD, McMillan JL, Stone MH (1992) Efficacy of chromium supplementation in athletes: emphasis on anabolism. Int J Sport Nutr 2:111–122
Schroeder HA (1971) Losses of vitamins and trace minerals resulting from processing and preservation of foods. Am J Clin Nutr 24:562–573
Offenbacher EG, Pi-Sunyer FX (1988) Chromium in human nutrition. Annu Rev Nutr 8:543–563
Striffler JS, Law JS, Polansky MM, Bhathena SJ, Anderson RA (1995) Chromium improves insulin response to glucose in rats. Metabolism 44:1314–1320
Jeejeebhoy KN, Chu RC, Marliss EB, Greenberg GR, Bruce-Robertson A (1977) Chromium deficiency, glucose intolerance, and neuropathy reversed by chromium supplementation, in a patient receiving long-term total parenteral nutrition. Am J Clin Nutr 30:531–538
Freund H, Atamian S, Fischer JE (1979) Chromium deficiency during total parenteral nutrition. JAMA 241:496–498
Brown RO, Forloines-Lynn S, Cross RE, Heizer WD (1986) Chromium deficiency after long-term total parenteral nutrition. Dig Dis Sci 31:661–664
Anderson RA (1995) Chromium and parenteral nutrition. Nutrition 11:83–86
Zafra-Stone S, Bagchi M, Preuss HG, Bagchi D (2007) Benefits of chromium(III) complexes in animal and human health. In: Vincent JB (ed) The nutritional biochemistry of chromium(III). Elsevier, Amsterdam, pp 183–206
Anderson RA (1998) Chromium, glucose intolerance and diabetes. J Am Coll Nutr 17:548–555
Coryell VH, Stearns DM (2006) Molecular analysis of hprt mutations induced by chromium picolinate in CHO AA8 cells. Mutat Res 610:114–123
Stearns DM, Silveira SM, Wolf KK, Luke AM (2002) Chromium(III) tris(picolinate) is mutagenic at the hypoxanthine (guanine) phosphoribosyltransferase locus in Chinese hamster ovary cells. Mutat Res 513:135–142
Hathcock JN (1997) Vitamins and minerals: efficacy and safety. Am J Clin Nutr 66:427–437
Stearns DM, Wise JP Sr, Patierno SR, Wetterhahn KE (1995) Chromium(III) picolinate produces chromosome damage in Chinese hamster ovary cells. FASEB J 9:1643–1648
Wasser WG, Feldman NS, D’Agati VD (1997) Chronic renal failure after ingestion of over-the-counter chromium picolinate. Ann Intern Med 126:410
Cerulli J, Grabe DW, Gauthier I, Malone M, McGoldrick MD (1998) Chromium picolinate toxicity. Ann Pharmacother 32:428–431
Shara M, Yasmin T, Kincaid AE, Limpach AL, Bartz J, Brenneman KA, Chatterjee A, Bagchi M, Stohs SJ, Bagchi D (2005) Safety and toxicological evaluation of a novel niacin-bound chromium (III) complex. J Inorg Biochem 99:2161–2183
Shara M, Kincaid AE, Limpach AL, Sandstrom R, Barrett L, Norton N, Bramble JD, Yasmin T, Tran J, Chatterjee A, Bagchi M, Bagchi D (2007) Long-term safety evaluation of a novel oxygen-coordinated niacin-bound chromium (III) complex. J Inorg Biochem 101:1059–1069
Mertz W (1993) Chromium in human nutrition: a review. J Nutr 123:626–633
Kashyap SR, Defronzo RA (2007) The insulin resistance syndrome: physiological considerations. Diab Vasc Dis Res 4:13–19
Bailey CJ (2007) Treating insulin resistance: future prospects. Diab Vasc Dis Res 4:20–31
Saad MJ (1994) Molecular mechanisms of insulin resistance. Braz J Med Biol Res 27:941–957
Roth RA, Liu F, Chin JE (1994) Biochemical mechanisms of insulin resistance. Horm Res 41(Suppl 2):51–55
Schinner S, Scherbaum WA, Bornstein SR, Barthel A (2005) Molecular mechanisms of insulin resistance. Diabet Med 22:674–682
Dugani CB, Klip A (2005) Glucose transporter 4: cycling, compartments and controversies. EMBO Rep 6:1137–1142
Penumathsa SV, Thirunavukkarasu M, Samuel M, Zhan L, Maulik G, Bagchi M, Bagchi D, Maulik N (2007) Role of niacin-bound chromium (NBC) in ameliorating the symptoms of metabolic syndrome. J Am Coll Nutr 25:483
Dandona P, Aljada A, Chaudhuri A, Mohanty P, Garg R (2005) Metabolic syndrome: a comprehensive perspective based on interactions between obesity, diabetes, and inflammation. Circulation 111:1448–1454
Petersen JL, McGuire DK (2005) Impaired glucose tolerance and impaired fasting glucose–a review of diagnosis, clinical implications and management. Diab Vasc Dis Res 2:9–15
Park YW, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield SB (2003) The metabolic syndrome: prevalence and associated risk factor findings in the US population from the Third National Health and Nutrition Examination Survey, 1988–1994. Arch Intern Med 163:427–436
Haffner S, Taegtmeyer H (2003) Epidemic obesity and the metabolic syndrome. Circulation 108:1541–1545
Caballero B (2007) The global epidemic of obesity: an overview. Epidemiol Rev 29:1–5
Wang Y, Beydoun MA (2007) The obesity epidemic in the United States – gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev 29:6–28
Ordovas JM (2004) The quest for cardiovascular health in the genomic era: nutrigenetics and plasma lipoproteins. Proc Nutr Soc 63:145–152
Gibbs WW (2005) Obesity: an overblown epidemic? Sci Am 292:70–77
Joyal SV (2004) A perspective on the current strategies for the treatment of obesity. Curr Drug Targets CNS Neurol Disord 3:341–356
Walker CG, Zariwala MG, Holness MJ, Sugden MC (2007) Diet, obesity and diabetes: a current update. Clin Sci (Lond) 112:93–111
Kelly GS (2000) Insulin resistance: lifestyle and nutritional interventions. Altern Med Rev 5:109–132
Bianchi C, Penno G, Romero F, Del Prato S, Miccoli R (2007) Treating the metabolic syndrome. Expert Rev Cardiovasc Ther 5:491–506
Grant KE, Chandler RM, Castle AL, Ivy JL (1997) Chromium and exercise training: effect on obese women. Med Sci Sports Exerc 29:992–998
Crawford V, Scheckenbach R, Preuss HG (1999) Effects of niacin-bound chromium supplementation on body composition in overweight African-American women. Diabetes Obes Metab 1:331–337
Abraham AS, Brooks BA, Eylath U (1991) Chromium and cholesterol-induced atherosclerosis in rabbits. Ann Nutr Metab 35:203–207
Preuss HG, Wallerstedt D, Talpur N, Tutuncuoglu SO, Echard B, Myers A, Bui M, Bagchi D (2000) Effects of niacin-bound chromium and grape seed proanthocyanidin extract on the lipid profile of hypercholesterolemic subjects: a pilot study. J Med 31:227–246
Vinson JA, Mandarano MA, Shuta DL, Bagchi M, Bagchi D (2002) Beneficial effects of a novel IH636 grape seed proanthocyanidin extract and a niacin-bound chromium in a hamster atherosclerosis model. Mol Cell Biochem 240:99–103
Thirunavukkarasu M, Penumathsa S, Juhasz B, Zhan L, Bagchi M, Yasmin T, Shara MA, Thatte HS, Bagchi D, Maulik N (2006) Enhanced cardiovascular function and energy level by a novel chromium (III)-supplement. Biofactors 27:53–67
Thirunavukkarasu M, Penumathsa SV, Juhasz B, Zhan L, Cordis G, Altaf E, Bagchi M, Bagchi D, Maulik N (2006) Niacin-bound chromium enhances myocardial protection from ischemia-reperfusion injury. Am J Physiol Heart Circ Physiol 291:H820–H826
Abraham AS, Brooks BA, Eylath U (1992) The effects of chromium supplementation on serum glucose and lipids in patients with and without non-insulin-dependent diabetes. Metabolism 41:768–771
Anderson RA, Cheng N, Bryden NA, Polansky MM, Cheng N, Chi J, Feng J (1997) Elevated intakes of supplemental chromium improve glucose and insulin variables in individuals with type 2 diabetes. Diabetes 46:1786–1791
Jovanovic-Peterson L, Gutierrez M, Peterson CM (1999) Chromium supplementation for women with gestational diabetes mellitus. J Trace Elem Exp Med 12:91–97
Ravina A, Slezak L, Mirsky N, Bryden NA, Anderson RA (1999) Reversal of corticosteroid-induced diabetes mellitus with supplemental chromium. Diabet Med 16:164–167
Wilson BE, Gondy A (1995) Effects of chromium supplementation on fasting insulin levels and lipid parameters in healthy, non-obese young subjects. Diabetes Res Clin Pract 28:179–184
Bagchi M, Jensen N, Preuss HG, Bagchi D (2004) Efficacy and toxicological assessment of a novel, niacin-bound chromium in ameliorating metabolic disorders. In: 10th international congress of toxicology, Finland, p 354
Kleefstra N, Houweling ST, Jansman FG, Groenier KH, Gans RO, Meyboom-de Jong B, Bakker SJ, Bilo HJ (2006) Chromium treatment has no effect in patients with poorly controlled, insulin-treated type 2 diabetes in an obese Western population: a randomized, double-blind, placebo-controlled trial. Diabetes Care 29:521–525
Kleefstra N, Houweling ST, Bakker SJ, Verhoeven S, Gans RO, Meyboom-de Jong B, Bilo HJ (2007) Chromium treatment has no effect in patients with type 2 diabetes in a Western population: a randomized, double-blind, placebo-controlled trial. Diabetes Care 30:1092–1096
Stearns DM, Belbruno JJ, Wetterhahn KE (1995) A prediction of chromium(III) accumulation in humans from chromium dietary supplements. FASEB J 9:1650–1657
Kaput J, Noble J, Hatipoglu B, Kohrs K, Dawson K, Bartholomew A (2007) Application of nutrigenomic concepts to type 2 diabetes mellitus. Nutr Metab Cardiovasc Dis 17:89–103
Afman L, Muller M (2006) Nutrigenomics: from molecular nutrition to prevention of disease. J Am Diet Assoc 106:569–576
Ferguson LR (2006) Nutrigenomics: integrating genomic approaches into nutrition research. Mol Diagn Ther 10:101–108
Rink C, Roy S, Khanna S, Rink T, Bagchi D, Sen CK (2006) Transcriptome of the subcutaneous adipose tissue in response to oral supplementation of type 2 Leprdb obese diabetic mice with niacin-bound chromium. Physiol Genomics 27:370–379
Lee JH, Kemp DM (2006) Human adipose-derived stem cells display myogenic potential and perturbed function in hypoxic conditions. Biochem Biophys Res Commun 341:882–888
Sasao N, Hirayama E, Kim J (2003) Characterization of heterokaryons between skeletal myoblasts and preadipocytes: myogenic potential of 3T3-L1 preadipocytes. Eur J Cell Biol 82:97–103
Xu Y, Malladi P, Wagner DR, Longaker MT (2005) Adipose-derived mesenchymal cells as a potential cell source for skeletal regeneration. Curr Opin Mol Ther 7:300–305
Comi GP, Fortunato F, Lucchiari S, Bordoni A, Prelle A, Jann S, Keller A, Ciscato P, Galbiati S, Chiveri L, Torrente Y, Scarlato G, Bresolin N (2001) Beta-enolase deficiency, a new metabolic myopathy of distal glycolysis. Ann Neurol 50:202–207
Jeffery CJ, Bahnson BJ, Chien W, Ringe D, Petsko GA (2000) Crystal structure of rabbit phosphoglucose isomerase, a glycolytic enzyme that moonlights as neuroleukin, autocrine motility factor, and differentiation mediator. Biochemistry 39:955–964
Yanagawa T, Funasaka T, Tsutsumi S, Watanabe H, Raz A (2004) Novel roles of the autocrine motility factor/phosphoglucose isomerase in tumor malignancy. Endocr Relat Cancer 11:749–759
Kanno H, Fujii H, Hirono A, Ishida Y, Ohga S, Fukumoto Y, Matsuzawa K, Ogawa S, Miwa S (1996) Molecular analysis of glucose phosphate isomerase deficiency associated with hereditary hemolytic anemia. Blood 88:2321–2325
Baranova A, Collantes R, Gowder SJ, Elariny H, Schlauch K, Younoszai A, King S, Randhawa M, Pusulury S, Alsheddi T, Ong JP, Martin LM, Chandhoke V, Younossi ZM (2005) Obesity-related differential gene expression in the visceral adipose tissue. Obes Surg 15:758–765
Kim YC, Zemel MB (1995) Insulin stimulation of intracellular free Ca2+ recovery and Ca(2+)-ATPase gene expression in cultured vascular smooth-muscle cells: role of glucose 6-phosphate. Biochem J 311(Pt 2):555–559
Moore JW, Maher MA, Banz WJ, Zemel MB (1998) Chromium picolinate modulates rat vascular smooth muscle cell intracellular calcium metabolism. J Nutr 128:180–184
McCarty MF (2006) PKC-mediated modulation of L-type calcium channels may contribute to fat-induced insulin resistance. Med Hypotheses 66:824–831
Eyre H, Akkari PA, Wilton SD, Callen DC, Baker E, Laing NG (1995) Assignment of the human skeletal muscle alpha-tropomyosin gene (TPM1) to band 15q22 by fluorescence in situ hybridization. Cytogenet Cell Genet 69:15–17
Ruiz-Opazo N, Weinberger J, Nadal-Ginard B (1985) Comparison of alpha-tropomyosin sequences from smooth and striated muscle. Nature 315:67–70
Gordon AM, Homsher E, Regnier M (2000) Regulation of contraction in striated muscle. Physiol Rev 80:853–924
Rodriguez Fernandez JL, Ben-Ze’ev A (1989) Regulation of fibronectin, integrin and cytoskeleton expression in differentiating adipocytes: inhibition by extracellular matrix and polylysine. Differentiation 42:65–74
Kocaefe YC, Israeli D, Ozguc M, Danos O, Garcia L (2005) Myogenic program induction in mature fat tissue (with MyoD expression). Exp Cell Res 308:300–308
Lin SC, Li P (2004) CIDE-A, a novel link between brown adipose tissue and obesity. Trends Mol Med 10:434–439
Zhou Z, Yon Toh S, Chen Z, Guo K, Ng CP, Ponniah S, Lin SC, Hong W, Li P (2003) CIDEA-deficient mice have lean phenotype and are resistant to obesity. Nat Genet 35:49–56
Cinti S (2002) Adipocyte differentiation and transdifferentiation: plasticity of the adipose organ. J Endocrinol Invest 25:823–835
Stocker A (2004) Molecular mechanisms of vitamin E transport. Ann N Y Acad Sci 1031:44–59
Bjornson LK, Gniewkowski C, Kayden HJ (1975) Comparison of exchange of alpha-tocopherol and free cholesterol between rat plasma lipoproteins and erythrocytes. J Lipid Res 16:39–53
Traber MG, Burton GW, Hamilton RL (2004) Vitamin E trafficking. Ann N Y Acad Sci 1031:1–12
Vincent JB (1999) Mechanisms of chromium action: low-molecular-weight chromium-binding substance. J Am Coll Nutr 18:6–12
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lau, F.C., Bagchi, M., Sen, C.K. et al. Nutrigenomic basis of beneficial effects of chromium(III) on obesity and diabetes. Mol Cell Biochem 317, 1–10 (2008). https://doi.org/10.1007/s11010-008-9744-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-008-9744-2