
Abstract
Objective Growing evidence suggests that maternal socioeconomic mobility (SM) is associated with pregnancy outcomes. Our study investigated the association between maternal SM from childhood to adulthood and the risk of preterm delivery (PTD), and examined heterogeneity of associations by race/ethnicity. Methods In this study, 3019 pregnant women enrolled from 5 Michigan communities at 16–27 weeks’ gestation (1998–2004) provided their parents’ socioeconomic position (SEP) indicators (education, occupation, receipt of public assistance) and their own and child’s father’s SEP indicators (education, occupation, Medicaid status, and household income) at the time of enrollment. Latent class analysis was used to identify latent classes of childhood SEP indicators, adulthood SEP indicators, and SM from childhood to adulthood, respectively. A model-based approach to latent class analysis with distal outcome assessed relations between latent class and PTD, overall and within race/ethnicity groups. Results Three latent classes (low, middle, high) were identified for childhood SEP indicators and adulthood SEP indicators, respectively; while four latent classes (static low, upward, downward, and static high) best described SM. Women with upward SM had decreased odds of PTD (Odds ratio = 0.60, 95% confidence interval: 0.42, 0.87), compared to those with static low SEP. This SM advantage was true for all women and most pronounced in white/others women. Conclusions Maternal experiences of upward SM may be important considerations when assessing PTD risk. Our results support the argument that policies and programs aimed at improving women’s SEP could lower PTD rates.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Significance
Previous studies on socioeconomic mobility (SM) and pregnancy outcomes used predominately ecological measures of SM. Our study found that maternal upward SM was associated with decreased risk of preterm delivery (PTD), and is novel in several ways: (1) it includes in-depth, individual-level and ecological data to measure SM and a latent class analysis with distal outcome PTD; (2) the sample is large for this type of in-depth data and is racially and socioeconomically diverse; and (3) our community-based cohort was sampled from 52 prenatal care clinics, thereby avoiding biases seen in samples from select inner-city clinics and academic/teaching hospitals.
Introduction
Preterm delivery (PTD, delivery less than 37 completed weeks of gestation) is a leading cause of perinatal mortality and morbidity (Blencowe et al. 2013). The disparities in PTD rates between population subgroups defined by race/ethnicity and socioeconomic status are striking (Blumenshine et al. 2010). Previous studies have shown that maternal disadvantaged socioeconomic position (SEP) in adulthood is associated with higher PTD risk (Blumenshine et al. 2010; Morgen et al. 2008; Auger et al. 2009; Blumenshine et al. 2011; Hvas Mortensen et al. 2011; Matijasevich et al. 2010; Whitehead 2012; Joseph et al. 2014; Shankardass et al. 2014). Measures of SEP have included occupation, education and household income, and the relationship with PTD often varied by race/ethnicity (Blumenshine et al. 2010). Few studies have examined mother’s childhood SEP and pregnancy outcomes, though there is evidence that SEP in childhood has a significant effect on adult health (Cohen et al. 2010). A Brazilian intergenerational study observed that maternal childhood poverty, measured by family income, was strongly associated with shorter gestation (Gigante et al. 2015).
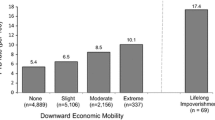
Socioeconomic mobility (SM) has been studied in relation to low birthweight (Basso et al. 1997; Spencer 2004; Colen et al. 2006; Astone et al. 2007; Love et al. 2010; Osypuk et al. 2016), small for gestational age (Love et al. 2010; Osypuk et al. 2016; Slaughter-Acey et al. 2016), and newborn body composition (Sletner et al. 2014). In our review of the literature, however, we found fewer studies examining SM and PTD (Love et al. 2010; Collins et al. 2006, 2011, 2015; Kramer et al. 2013). Collins et al. (2011) found that upward SM from an impoverished childhood was related to a decreased risk of PTD among African Americans. Women who experienced low, modest, or high upward SM had lower PTD rates of 16.0, 15.2, and 12.4%, respectively, than those with lifelong lower class status; rate ratio (RR) and 95% confidence interval (CI) = 0.9 (0.8, 0.9), 0.8 (0.7, 0.9), 0.7 (0.6, 0.8), respectively. In contrast, downward SM was linked to an elevated risk of PTD among white urban women (Collins et al. 2015). Those who experienced slight, moderate, or extreme downward SM had a higher risk of PTD rates than women with lifelong upper class status, with RR and 95% CI of 1.2 (1.0, 4.0), 1.6 (1.3, 1.9), and 1.9 (1.3, 2.6), respectively. However, these studies measured SM based on neighborhood census tract median family income rather than individual or household data.
Three conceptual models have been proposed to explain how disadvantaged life course SEP affects health later in life and they may not be mutually exclusive (Kendzor et al. 2012). One model focuses on critical developmental periods (e.g. childhood) when SEP may exert its strongest effect on later health. Another model views “accumulation” of socioeconomic disadvantage (intensity and duration) as posing the greatest health risk. A third model considers SEP trajectories, i.e. SM; it hypothesizes that upward SM remediates the negative effects of earlier socioeconomic disadvantage, while downward SM may result in poorer adult health despite relative socioeconomic advantages at earlier stages (Cohen et al. 2010; Kendzor et al. 2012). In all these models, determining the temporal order of SEP and health can be challenging.
The main objective of this study is to investigate associations between maternal SM from childhood to adulthood and risk of PTD in a Michigan, community-based cohort study that is racially and socioeconomically diverse. The availability of in-depth, individual-level data provides a unique opportunity to study SM. Based on the model of SEP trajectories, we hypothesize that: (1) women with low childhood SEP and low adulthood SEP will be at greatest risk of PTD; and (2) upward SM from childhood to adulthood will lower women’s risk of PTD. Because other studies reported that the relation of SEP (or SM) with PTD risk varied by maternal race/ethnicity (Blumenshine et al. 2010; Collins et al. 2011, 2015), we also examine evidence for this effect modification.
Methods
Study Population
This study included 3019 pregnant women enrolled at 16–27 weeks’ gestation in the prospective pregnancy outcomes and community health (POUCH) study (1998–2004) from five Michigan communities. Eligibility criteria included: English-speaking, age > 14 years, singleton pregnancy with no known congenital anomalies, no pre-existing diabetes, and prenatal maternal serum alpha-fetoprotein screening at 16–22 weeks’ gestation. The detailed study protocol can be found elsewhere (Holzman et al. 2001). The POUCH study received institutional review board approval from Michigan State University and all nine participating delivery hospitals.
At enrollment women provided informed written consent. Each woman met with a study nurse for a structured in-person interview and completed a self-administered questionnaire which collected information regarding demographics, lifestyle, psychosocial factors, medical history and health status. Pregnancy outcome data were abstracted from medical records. Self-reported maternal race/ethnicity was dichotomized as white/others or black. The numbers of “others” race/ethnicity were small and their PTD rates were similar to that of whites, therefore these groups were combined.
Measures
Childhood SEP and Adulthood SEP
Childhood SEP measures included a woman’s self-report of her parents’ socioeconomic indicators during her childhood, i.e. maternal mother’s and father’s highest level of education, maternal mother’s and father’s usual occupation, and receipt of public assistance by the family. Adulthood SEP measures included maternal socioeconomic indicators at enrollment, i.e. maternal and child’s father’s highest level of education, maternal and child’s father’s usual occupation, Medicaid Insurance status, and maternal annual household income. In separate models, a maternal neighborhood deprivation index (NDI) also was included in adulthood SEP. The NDI was calculated using information from the 1986 Census and followed a previously validated approach (Messer et al. 2006). NDI was dichotomized at the medium of the study population.
Maternal SM
SM was measured by using mother’s childhood and adulthood SEP indicators modeled as binary variables, i.e. education (≤ high school, > high school); usual occupation status based on US Census Bureau’s 1990 Occupational Classification System (“low” = service/blue collar, unemployed, and unknown; “high” = professional, manager, technical, clerical/sales, homemaker, military, retired, and student); public assistance (yes/no); Medicaid Insurance (yes/no); maternal household income (< $50,000 and ≥ $50,000). “Unknown” paternal occupation was assigned as “low” occupation status because it correlated with other low SEP indicators (Slaughter-Acey et al. 2016).
Preterm Delivery
Gestational age at delivery was estimated using date of last menstrual period unless this estimate disagreed with early ultrasound (< 25 weeks’ gestation) dating by two or more weeks, in which case ultrasound dating was given preference. PTD was defined as deliveries less than 37 completed weeks’ gestation.
Statistical Analysis
Initially we assessed maternal characteristics and SEP indicators overall and stratified by delivery timing (term/preterm), and tested for differences in proportions using Chi square tests. We used latent class analysis (LCA) to identify and describe distinct classes of childhood SEP indicators and adulthood SEP indicators and SM from childhood to adulthood. LCA classifies individuals with similar SEP characteristics into groups based on conditional probabilities (Collins and Lanza 2010). SM was defined by LCA according to a multidimensional set of SEP indicators from childhood to adulthood. We determined the optimal number of LCA classes by: (1) visualizing the plot of log-likelihoods of specified models across numbers of classes and eliminating models where the log-likelihoods no longer showed a substantial improvement in model fit (Nylund et al. 2007); (2) using the Bayesian Information Criterion (BIC), with a smaller BIC value indicating a better-fitted model (Schwarz 1978); (3) evaluating the entropy, an indicator for class separation and precision, that measures how well an individual fits into a specific class with values closer to 1 representing better fit (Ramaswamy et al. 1993); and (4) considering the size of the latent classes, uniqueness of classes, and meaningful interpretation of the pattern of response probabilities for each class. As a next step, we used the model-based approach to LCA with distal outcome to assess relations between exposure variables (i.e. childhood SEP, adulthood SEP, SM) and PTD (Lanza et al. 2013). Once the optimal number of classes was determined, LCA with distal outcomes was applied to allow the latent class membership to predict the risk of PTD.
Race/ethnicity was included as a grouping variable in LCA models to investigate associations among SEP, SM and risk of PTD within race/ethnic groups (white/others, black). Because SEP indicators may have different ranges and occur in different contexts across race/ethnic groups, we computed group-specific LCA following the same methodology described above. In a latter set of models we added NDI to adulthood SEP to examine its contribution to identifying SEP associations with PTD risk.
All statistical analyses were conducted using PROC LCA and its corresponding distal outcome macro in SAS 9.4 (Statistical Analysis Software, Cary, NC) (Lanza et al. 2015; Dziak et al. 2016). Proc LCA program uses full information maximum likelihood estimation to deal with missing data in the SEP indicators.
Results
Sample Characteristics
In the total sample of 3019 women, 11.1% of pregnancies ended in PTD and about one-fourth of women were black (Table 1). For the childhood SEP indictors, about 60% of grandmothers and 55% of grandfathers did not graduate from high school. Approximately 32% of grandmothers and 71% of grandfathers had a low-level occupation. About one-third of families received public assistance during the mother’s childhood period. For adulthood SEP indicators, 47% of mothers and 55% of fathers did not graduate from high school; 39% of mothers and 65% of fathers had a low-level occupation; 48% of pregnant women were insured by Medicaid; and 66% of families had an annual income of <$50,000. In bivariate analyses, increased risk of PTD was associated with two childhood SEP indicators, i.e., grandmother’s low-level occupation and family history of public assistance; and with all adulthood indicators of lower SEP, except NDI.
Latent Class Profile
In the LCA of childhood SEP, a three-class solution was considered optimal according to criteria described in our statistical Methods section (Table 2). The subgroups characterized by particular SEP indicators were interpreted and labelled according to the parameter estimates. Table 3 shows the latent class prevalence and item-response probability. Latent class prevalence is the proportion of individuals who have a similar SEP or SM pattern. Item-response probability indicates the probability of having the particular SEP indicator given the latent class membership. For childhood SEP Class 1, “low group”, (38% of women) grandmothers and grandfathers were less likely to graduate from high school (17 and 11%, respectively), to have a high-level occupation (23 and 11%, respectively), or to avoid public assistance during the mother’s childhood (43%) (Table 3). The probabilities of positive childhood SEP indicators improved in childhood SEP Class 2, “middle group”, (38% of women) with the exception of grandfathers’ education (11%) and occupation (17%). Childhood SEP Class 3, “high group”, (24% of women) showed high probabilities of all positive SEP indicators.
For adulthood SEP, a four-class model had the lowest BIC, however there was minimal improvement when moving from a three-class to four-class model, compared to the substantial log-likelihoods difference from a two-class to a three-class model. In addition, the entropy for the four-class model was smaller than that for the three-class model, indicating poor latent class separation for the four-class model (Ramaswamy et al. 1993). Based on additional considerations of class prevalence and interpretability we chose the three-class model for adulthood SEP (Table 2). Adulthood SEP Class 1, “low group”, (51% of women) mothers and fathers were less likely to graduate from high school (22 and 15%, respectively), to have a high-level occupation (40 and 16%, respectively), to have medical insurance other than Medicaid (15%), or to a family income ≥ $50,000 (4%) (Table 3). The probabilities of SEP indicators in adulthood SEP Class 2, “middle group”, (18% of women) varied; for example, fathers in this group had low probabilities of having a high-level education (19%) and occupation (23%) but women were more likely to have high-level occupations (73%) and medical insurance other than Medicaid (94%). About half of the families had an annual household income exceeding $50,000 (54%). In adulthood SEP Class 3, “high group”, (31% of women), all probabilities of positive SEP indicators were increased; about 64% of these families had annual household incomes exceeding $50,000.
We used both childhood and adulthood SEP indicators for the SM LCA. The BIC values decreased with increasing number of classes. After reviewing the plot of log-likelihoods of similarly specified models with different classes, improvements in model fit, size of the classes, and interpretability we chose the four-class solution for modeling SM from childhood to adulthood (Table 2). In SM from childhood to adulthood, Class 1, “static low group”, (45% women) women had low-level childhood SEP and low-level adulthood SEP indicators (Table 3). SM Class 2, “upwardly mobile group”, (24% of women) showed some improvement in two childhood indicators, i.e. probabilities of grandmother with high-level occupation (75%) and avoiding public assistance (81%), and higher probabilities in all positive adulthood SEP indicators. SM Class 3, “downwardly mobile group”, (16% of women) tended to have high-level childhood SEP and moderate to low-level adulthood SEP. In this group the fathers’ education and occupation were unlikely to be high-level (39 and 27%, respectively) and the probability of household income > $50,000 was low (15%). SM Class 4, “static high group”, (15% of women) had high-level SEP indicators throughout childhood and adulthood.
Latent class models also were examined for white/others women and black women separately using the methodology described above. For each race/ethnic group, based on fit indices and interpretability, we chose a three-class model for childhood SEP and adulthood SEP indicators and a four-class model for SM. The race/ethnicity-specific item-response probabilities for each indicator conditional on latent class membership are presented in Table 3. For the childhood SEP, the class percentages for white/others and black women, respectively, were: low group 24, 78%; middle group 46, 13%; and high group 30, 9%. For the adulthood SEP, the class percentages for white/others and black women, respectively, were: low group 44, 48%; middle group 19, 31%; and high group 37, 21%. For SM, the class percentages for white/others and black women, respectively, were: static low 38% (n = 855), 57% (n = 424); upwardly mobile 28% (n = 639), 15% (n = 114); downwardly mobile; 16% (n = 365), 21% (n = 152); and static high 18% (n = 418), 7% (n = 54).
LCA with Distal Outcome: PTD
Overall, the frequency of PTD in the low, middle, and high childhood SEP groups was 13.24, 9.57, 10.07%, respectively. The frequency of PTD in the low, middle, and high adulthood SEP groups was 12.91, 10.34, and 8.51%, respectively. In comparisons with their respective high SEP groups, women in the low SEP groups were more likely to deliver preterm: low childhood SEP group PTD odds ratio (OR) 1.36, (95% CI 0.98, 1.90); and low adulthood PTD OR 1.59, (95% CI 1.18, 2.15) (Table 4). PTD occurred in 8.34% of women who had upward SM and 11.62% of women who had downward SM. Women in the upward SM group had a decreased odds of PTD (OR 0.60, 95% CI 0.42, 0.87) compared to women in the static low SM group. The odds of PTD among women with downward SM was higher (OR 1.36, 95% CI 0.80, 2.30) than that of women with static high SM, however, the association was not statistically significant.
In a separate set of analyses we used race/ethnic-specific LCA models. Among the white/others women, low childhood SEP and low adulthood SEP were associated with increased odds of PTD in comparisons with their respective high SEP groups, PTD ORs 1.21, (95% CI 0.98, 1.90) and 1.44 (95% CI 1.02, 2.04). Women who experienced upward SM had a lower odds of PTD, OR 0.66, (95% CI 0.43, 1.00) when compared to those in the static low SM group. Among black women, PTD odds were greater in the low childhood SEP and low adulthood SEP groups compared to their respective high SEP groups, however, the small samples sizes for each SEP class resulted in more limited statistical power and no statistically significant associations.
We incorporated NDI in the adulthood SEP to examine its added effect on SEP associations with PTD. Table 5 in Appendix 1 summaries the LCA model fit statistics. In consideration of a combination of fit statistics and interpretability, we selected a three-class model for adulthood SEP with NDI and a four-class model for SM that included childhood SEP and adulthood SEP with NDI. The item-response probabilities for each SEP indicator conditional on latent class membership of adulthood SEP with NDI and SM are shown in Table 6 in Appendix 2. The latent class profiles were similar to those in adulthood SEP without NDI. When we assessed the associations between latent class membership and PTD (Table 7 in Appendix 3), NDI did not substantially change our original findings.
Discussion
Using a latent class approach with relevant indicators, we identified constructs of pregnant women’s childhood SEP, adulthood SEP, and SM from childhood to adulthood in association with risk of PTD. We found that women with low childhood SEP and low adulthood SEP were at greatest risk of PTD; and pregnant women who experienced upward SM had a lower likelihood of delivering preterm than those who had static low SEP. This SM advantage was true for all women and most pronounced in white/others women.
Our findings are consistent with Slaughter-Acey et al.’s analysis of POUCH Study data showing decreased risk of delivering a small-for-gestational-age infant among pregnant women with upward SM (Slaughter-Acey et al. 2016). In another study of African-American pregnant women, Collins et al. reported that upward SM was related to a decreased risk of PTD (Collins et al. 2011). The previous studies have typically measured SEP at a single time point, and used a single indicator, e.g. education, occupation or family income (Auger et al. 2009; Blumenshine et al. 2011; Joseph et al. 2014; Gigante et al. 2015). However, the multidimensional nature of SEP and the complexity of SEP transition from one time point to another suggest that SEP and SM cannot be measured completely with one indicator. In pregnancy outcomes studies, methods for combining multiple SEP indicators and for measuring SM from childhood to adulthood vary (Gigante et al. 2015; Slaughter-Acey et al. 2016). A novel contribution of our study is that we used a LCA approach for measuring SM in a dataset with individual-level data of maternal childhood and adulthood SEP indicators.
We also observed that disadvantaged SEP at adulthood was associated with a greater likelihood of PTD, a finding that is echoed across many previous studies (Morgen et al. 2008; Blumenshine et al. 2011; Matijasevich et al. 2010; Whitehead 2012; Joseph et al. 2014). In a systematic review of 106 studies from 1999 to 2007, Blumenshine et al. (2010) suggested that disadvantaged SEP was consistently linked to greater risk of adverse birth outcomes and observed racial/ethnic heterogeneity in the effect of SEP measures (Blumenshine et al. 2010). The inverse associations between maternal education and adverse birth outcomes were significant among non-Hispanic white pregnant women. Shankardass et al. (2014) found that the risk of spontaneous PTD was elevated across all the indicators of lower SEP, and women living in neighborhoods with higher NDI had greater risks of medically indicated and spontaneous PTD (Shankardass et al. 2014). In our study, the addition of NDI to the model did not substantively change the adulthood SEP relation to PTD risk.
Our findings support the hypothesis that improving women’s SEP from childhood to adulthood may improve pregnancy outcomes. According to the cumulative pathway life-course model, upward SM might decrease the accumulation of adverse exposures that create “wear and tear” to the body (allostatic load) (McEwen 1998), and thereby create a more optimal in-utero environment for the growing fetus (Slaughter-Acey et al. 2016). Pregnant women who experience upward SM may have: (1) greater access to high-quality food, reliable housing, a safe living environment, and high-quality health care; (2) more support for healthy lifestyle choices (diet, physical activity, no smoking, no alcohol use, etc.); and (3) greater opportunity for psychological health (less stress, more social integration, etc.). The benefit of SM also implies that the childhood environment (SEP) is not deterministic for women’s future risk of PTD. In our data, the adulthood SEP had the strongest association with PTD risk.
Some studies of SEP and pregnancy outcomes use logistic regression models with multiple SEP measures, often hoping to identify the most salient indicators. However, SEP indicators are highly correlated and SEP can be thought of as a latent construct. By using LCA, a more comprehensive strategy, we can better capture the latent constructs of SEP and SM. To our knowledge, this study is the first to use the model-based approach to LCA with distal outcome to elucidate complex relationships between SM and the risk of PTD among pregnant women in the United States. Typically, traditional classify-analyze strategies have been used to predict a distal outcome from latent class membership. In the first classification step, individuals were assigned to latent classes based on probabilities. In a second analysis step, the latent class membership was treated as observed and used to predict the distal outcome. From these strategies the results are biased to the extent that there is classification error. However, this model-based approach models measurement error and produces less biased estimates for the probability of PTD conditional on latent class membership (Collins and Lanza 2010). Moreover, use of the full-information expectation–maximization algorithm in LCA may include all participants who responded to at least one indicator of SEP (Collins and Lanza 2010). Most previous studies examining the impact of SM on pregnancy outcomes used a single SEP indicator to measure SM (Love et al. 2010; Collins et al. 2006, 2011, 2015; Kramer et al. 2013). Our study used multiple SEP indicators for childhood SEP and adulthood SEP measures, which may minimize misclassification bias. In addition, this study enrolled pregnant women with diverse SEP, which allowed us to observe a wider range of SM.
An important limitation in most SM research pertains to the inferences. When we study individuals we don’t randomly assign SM, therefore it is difficult to disentangle the extrinsic benefits of an improved socioeconomic environment from the unique attributes of individuals who are able to climb the SEP ladder (self-selection). In addition, our study had other limitations that should be noted. All SEP indicators were self-reported and recall bias cannot be ruled out, but the recall bias should apply equally to those with and without PTD because reporting occurred mid-pregnancy, well before delivery. Few black women experienced SM in this study, making it difficult to calculate accurate race/ethnicity-specific estimates of the SM-PTD association in this group. Our software and modeling strategy, i.e. model-based approach to LCA with distal outcome, could not accommodate adjustment for other covariates (potential confounders); this leaves open the possibility of unmeasured confounding. While we stratified on race/ethnicity, we considered maternal age, parity, and pre-pregnancy body mass index as important covariates. In sensitivity analyses we also looked to see whether our results would vary by these covariates. The analyses results suggested that our findings were robust even after the stratification. We cannot be sure if the relationships between SEP, SM and PTD observed in this study would apply to women in other countries, or cohorts embedded in different historical periods.
In summary, our study suggests that policies or programs to reduce socioeconomic inequalities may play an important role in decreasing adverse pregnancy outcomes such as PTD. Upward SM among pregnant women was associated with decreased risk of PTD. This relationship was most evident among white/others women in our study. Further research is needed to understand the specific elements accompanying SM that are protective for PTD and the best strategies for increasing SM among all race/ethnic groups.
References
Astone, N., Misra, D., & Lynch, C. (2007). The effect of maternal socio-economic status throughout the lifespan on infant birthweight. Paediatric and Perinatal Epidemiology, 21(4), 310–318.
Auger, N., Giraud, J., & Daniel, M. (2009). The joint influence of area income, income inequality, and immigrant density on adverse birth outcomes: a population-based study. BMC Public Health, 9(1), 237
Basso, O., Olsen, J., Johansen, A., & Christensen, K. (1997). Change in social status and risk of low birth weight in Denmark: Population based cohort study. BMJ, 315(7121), 1498–1502.
Blencowe, H., Cousens, S., Chou, D., Oestergaard, M., Say, L., Moller, A., Kinney, M., & Lawn, J. (2013). Born too soon: The global epidemiology of 15 million preterm births. Reproductive Health, 10(Suppl 1), S2.
Blumenshine, P., Egerter, S., Barclay, C., Cubbin, C., & Braveman, P. (2010). Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine, 39(3), 263–272.
Blumenshine, P., Egerter, S., Libet, M., & Braveman, P. (2011). Father’s education: An independent marker of risk for preterm birth. Maternal and Child Health Journal, 15(1), 60–67.
Cohen, S., Janicki-Deverts, D., Chen, E., & Matthews, K. (2010). Childhood socioeconomic status and adult health. Annals of the New York Academy of Sciences, 1186(1), 37–55.
Colen, C., Geronimus, A., Bound, J., & James, S. (2006). Maternal upward socioeconomic mobility and black–white disparities in infant birthweight. American Journal of Public Health, 96(11), 2032–2039.
Collins, J., Rankin, K., & David, R. (2015). Downward economic mobility and preterm birth: an exploratory study of Chicago-born upper class white mothers. Maternal and Child Health Journal, 19(7), 1601–1607.
Collins, J. W., Jr, D. R. J., Simon, D. M., & Prachand, N. G. (2006). Preterm birth among African American and white women with a lifelong residence in high-income Chicago neighborhoods: An exploratory study. Ethnicity and Disease, 17(1), 113–117.
Collins, J. W. Jr., Rankin, K. M., & David, R. (2011). African American womenʼs lifetime upward economic mobility and preterm birth: The effect of fetal programming. Obstetrical and Gynecological Survey, 66(6), 329–330.
Collins, L., & Lanza, S. (2010). Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences. United States: Wiley.
Dziak, J. J., Yang, J., Tan, X., Bray, B. C., Wagner, A. T., & Lanza, S. T. (2016). LCA distal SAS macro users’ guide (Version 3.0.2). University Park: The Methodology Center, Penn State. http://methodology.psu.edu. Accessed 7 March 7 2016.
Gigante, D., Horta, B., Matijasevich, A., Loret de Mola, C., Barros, A., & Santos, I., et al. (2015). Gestational age and newborn size according to parental social mobility: An intergenerational cohort study. Journal of Epidemiology and Community Health, 69(10), 944–949.
Holzman, C., Bullen, B., Fisher, R., Paneth, N., & Reuss, L. (2001). Pregnancy outcomes and community health: The POUCH study of preterm birth. Paediatric and Perinatal Epidemiology, 15(s2), 136–158.
Hvas Mortensen, L., Helweg-Larsen, K., & Nybo Andersen, A. (2011). Socioeconomic differences in perinatal health and disease. Scandinavian Journal of Public Health, 39(7 Suppl), 110–114.
Joseph, K., Fahey, J., Shankardass, K., Allen, V., O’Campo, P., & Dodds, L., et al. (2014). Effects of socioeconomic position and clinical risk factors on spontaneous and iatrogenic preterm birth. BMC Pregnancy and Childbirth, 14(1), 117.
Kendzor, D., Caughy, M., & Owen, M. (2012). Family income trajectory during childhood is associated with adiposity in adolescence: A latent class growth analysis. BMC Public Health, 12(1), 611.
Kramer, M., Dunlop, A., & Hogue, C. (2013). Measuring women’s cumulative neighborhood deprivation exposure using longitudinally linked vital records: A method for life course MCH research. Maternal and Child Health Journal, 18(2), 478–487.
Lanza, S., Tan, X., & Bray, B. (2013). Latent class analysis with distal outcomes: A flexible model-based approach. Structural Equation Modeling: A Multidisciplinary Journal, 20(1), 1–26.
Lanza, S. T., Dziak, J. J., Huang, L., Wagner, A., & Collins, L. M. (2015). PROC LCA and PROC LTA users’ guide (Version 1.3.2). University Park: The Methodology Center, Penn State. http://methodology.psu.edu. Accessed 7 March 2016.
Love, C., David, R., Rankin, K., & Collins, J. (2010). Exploring weathering: effects of lifelong economic environment and maternal age on low birth weight, small for gestational age, and preterm birth in African-American and white women. American Journal of Epidemiology, 172(2), 127–134.
Matijasevich, A., Victora, C., Lawlor, D., Golding, J., Menezes, A., & Araújo, C., et al. (2010). Association of socioeconomic position with maternal pregnancy and infant health outcomes in birth cohort studies from Brazil and the UK. Journal of Epidemiology and Community Health, 66(2), 127–135.
McEwen, B. (1998). Stress, adaptation, and disease: Allostasis and Allostatic load. Annals of the New York Academy of Sciences, 840(1), 33–44.
Messer, L., Laraia, B., Kaufman, J., Eyster, J., Holzman, C., & Culhane, J., et al. (2006). The development of a standardized neighborhood deprivation index. Journal of Urban Health, 83(6), 1041–1062.
Morgen, C. S., Bjork, C., Andersen, P. K., Mortensen, L. H., & Andersen, N., A (2008). Socioeconomic position and the risk of preterm birth: A study within the Danish national birth cohort. International Journal of Epidemiology, 37(5), 1109–1120.
Nylund, K., Asparouhov, T., & Muthén, B. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569.
Osypuk, T., Slaughter-Acey, J., Kehm, R., & Misra, D. (2016). Life-course social mobility and reduced risk of adverse birth outcomes. American Journal of Preventive Medicine, 51(6), 975–982.
Ramaswamy, V., Desarbo, W., Reibstein, D., & Robinson, W. (1993). An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Marketing Science, 12(1), 103–124.
Schwarz, G. (1978). Estimating the dimension of a model. The Annals of Statistics, 6(2), 461–464.
Shankardass, K., O’Campo, P., Dodds, L., Fahey, J., Joseph, K., Morinis, J., & Allen, V. (2014). Magnitude of income-related disparities in adverse perinatal outcomes. BMC Pregnancy and Childbirth, 14(1), 96.
Slaughter-Acey, J., Holzman, C., Calloway, D., & Tian, Y. (2016). Movin’ on up: Socioeconomic mobility and the risk of delivering a small-for-gestational age infant. Maternal and Child Health Journal, 20(3), 613–622.
Sletner, L., Jenum, A., Mørkrid, K., Vangen, S., Holme, I., Birkeland, K., & Nakstad, B. (2014). Maternal life course socio-economic position and offspring body composition at birth in a multi-ethnic population. Paediatric and Perinatal Epidemiology, 28(5), 445–454.
Spencer, N. (2004). Accounting for the social disparity in birth weight: results from an intergenerational cohort. Journal of Epidemiology & Community Health, 58(5), 418–419.
Whitehead, N. (2012). The relationship of socioeconomic status to preterm contractions and preterm delivery. Maternal and Child Health Journal, 16(8), 1645–1656.
Acknowledgements
Special thanks to members of the POUCH Study Team for their feedback and critique of this manuscript as it was being developed. The POUCH Study was supported by a Perinatal Epidemiologic Research Initiative Program Grant from the March of Dimes Foundation (Grants 20FY01-38 and 20-FY04-37) the National Institute of Child Health and Human Development and the National Institute of Nursing Research (Grant R01 HD34543), the Thrasher Research Foundation (Grant 02816-7) and the Centers for Disease Control and Prevention (Grant U01 DP000143-01).
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
See Table 5.
Appendix 2
See Table 6.
Appendix 3
See Table 7.
Rights and permissions
About this article

Cite this article
Tian, Y., Holzman, C., Slaughter-Acey, J. et al. Maternal Socioeconomic Mobility and Preterm Delivery: A Latent Class Analysis. Matern Child Health J 22, 1647–1658 (2018). https://doi.org/10.1007/s10995-018-2562-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-018-2562-6