
Abstract
Objectives The goals of interconception care are to optimize women’s health and encourage adequate spacing between pregnancies. Our study calculated trends in interpregnancy interval (IPI) patterns and measured the association of differing intervals with birth outcomes in California. Methods Women with “non-first birth” deliveries in California hospitals from 2007 to 2009 were identified in a linked birth certificate and patient discharge dataset and divided into three IPI birth categories: <6, 6–17, and 18–50 months. Trends over the study period were tested using the Cochran-Armitage two-sided linear trend test. Chi square tests were used to test the association between IPI and patient characteristics and selected singleton adverse birth outcomes. Results Of 645,529 deliveries identified as non-first births, 5.6 % had an IPI <6 months, 33.1 % had an IPI of 6–17 months, and 61.3 % had an IPI of 18–50 months. The prevalence of IPI <6 months declined over the 3-year period (5.8 % in 2007 to 5.3 % in 2009, trend p value <0.0001).Women with an IPI <6 months had a significantly higher prevalence of early preterm birth (<34 weeks), low birthweight (<2500 g), neonatal complications, neonatal death and severe maternal complications than women with a 6–17 month or 18–50 month IPI (p < 0.005). Comparing those with a 6–17 month vs 18–50 month IPI, there were increased early preterm births and decreased maternal complications, complicated delivery, and stillbirth/intrauterine fetal deaths among those with a shorter IPI. Conclusions for Practice In California, women with an IPI <6 months were at increased risk for several birth outcomes, including composite morbidity measures.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
Interpregnancy intervals (IPI) <18 months have been associated with poor birth outcomes. Our study of California data demonstrates that the highest risk for poor birth outcomes is observed for women experiencing <6 months IPI; excluding early preterm birth, increased risk was not observed for the 6–17 months IPI when compared to the oft-recommended 18–50 months IPI. If the observed pattern holds, increasing the IPI beyond 6 months would reduce the risk of preterm birth by 47 %, low birthweight by 38 %, neonatal death by 29 %, neonatal complications and stillbirth by 26 %, severe maternal complications by 20 %, and complicated delivery by 6 %.
Introduction
Public health efforts have focused on the “interconception” period between pregnancies as a prevention opportunity for women’s future health (Johnson et al. 2006; Moore 2008). Since many women may become pregnant again, one of the key components of interconception care has been to encourage adequate spacing between pregnancies. Short birth spacing has been shown to be an independent risk factor for adverse maternal and infant outcomes, regardless of a woman’s previous history, emphasizing the importance of pregnancy timing even among healthy women (Conde-Agudelo et al. 2006).
The birth interval and interpregnancy interval (IPI) are two ways to measure birth spacing with administrative data that only include historical live births. Birth interval is the time period between two live births, whereas IPI is the time period between conception and a previous live birth (World Health Organization 2006). Compared to IPI, birth interval measurement has an inherent bias because it includes but does not account for differences in the gestational length of the second pregnancy.
The risk of low birth weight, preterm birth and growth restriction, congenital anomalies, and stillbirths is elevated for women with short birth spacing (Conde-Agudelo et al. 2006; Salihu et al. 2011). For this reason, clinical recommendations for birth spacing have focused on establishing the minimum length to lessen the risk of adverse outcomes. As an example, the American College of Obstetricians & Gynecologists (ACOG) and the World Health Organization (WHO) make minimum spacing recommendations of at least 18 and 24 months after a live birth, respectively; no upper limit is suggested (Shachar 2012; World Health Organization 2006; American Congress of Obstetricians and Gynecoloists 2012). Although the risk of some birth outcomes decreases as the interval lengthens, there is also evidence that the risk increases with very long intervals (Salihu et al. 2011). Historically, the lowest risk IPI for perinatal outcomes has been between 18 and <51 months. Compared to the 18–50 month risk interval, IPIs of 6 months or less are associated with the highest risk of adverse perinatal outcomes. Slightly lower but still elevated risks can be found for women with IPIs of 6–17 months or ≥51 months. For maternal outcomes, IPIs greater than 59 months are associated with an increased risk of preeclampsia, and emerging evidence shows a risk of labor dystocia (Conde-Agudelo et al. 2007). There is preliminary evidence that short intervals are also associated with maternal mortality, anemia, placental abruption, placenta previa, and uterine rupture among women attempting vaginal delivery after previous cesarean (Conde-Agudelo et al. 2006, 2007; Bujold and Gauthier 2010; Getahun et al. 2010; Rutstein 2005; Stamilio et al. 2007). Folate depletion, incomplete healing of the uterine scar from previous cesarean delivery, vertical transmission of infections, and cervical insufficiency have been proposed as explanations for the association of IPI and birth outcomes, but there is only preliminary evidence to support these hypothesized mechanisms (Salihu et al. 2011; Conde-Agudelo et al. 2012). Birth spacing remains an independent risk factor, but in the absence of an established causal mechanism, it may be that birth spacing is a proxy for unmeasured biological constructs that vary with time.
Despite having experienced precipitous declines in the preterm birth, infant mortality and teen birth rates in recent years (California Department of Public Health 2014a; March of Dimes Prematurity Campaign 2013; California Department of Public Health 2014b), maternal and infant morbidity is increasing in California (Korst et al. 2014; Fridman et al. 2014, 2015). To guide the public health response, our study uses administrative data to: (1) determine birth spacing patterns in the diverse birthing population in California; (2) examine demographic trends in birth spacing; and, (3) explore associations of birth spacing with birth outcomes.
Methods
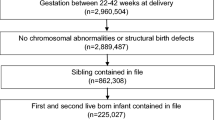
Linked birth cohort and patient discharge data were obtained from the California Office of Statewide Health Planning and Development (OSHPD) for delivering women and their infants born in California hospitals in 2007–2009. This dataset contains 98 % of births in the state and combines information from maternal antepartum hospitalizations 1 year prior to birth, the birth certificate, maternal and infant discharge records for the childbirth hospitalization, and postpartum maternal and infant hospital admissions or death records for the postnatal year. All linked records of live or stillborn deliveries to California resident women from 2007 to 2009 were included in the analyses. The study population of non-first births was comprised of multiparous women with a childbirth delivery during the 3-year study period (index birth) and a previous live birth less than 60 months prior to the index birth. Women with birth intervals of less than 5 months were considered erroneous and excluded from analysis. Index pregnancies delivered before 24 weeks gestation were also excluded because of an inconsistent ability to identify these pregnancies given the data source, i.e., hospital discharge data. Specifically, women with pregnancies ending before 24 weeks are often managed as outpatients or if admitted, discharge codes could reflect miscarriage—hence leading to under-reporting.
The interpregnancy interval (IPI) was obtained from the birth certificate by calculating the interval between the ‘Date of Last Live Birth’ variable and the date the index pregnancy began. Index conception date was calculated using the obstetric estimate from the birth certificate; the estimated conception date was obtained by subtracting this obstetric estimate from the birth date (of the last live birth). Using this calculation, there are three categories of IPIs: women who became pregnant less than 6 months after their previous birth (rapid repeat births), women who became pregnant 6–17 completed months after their previous birth (intermediate), and women who became pregnant 18–50 completed months after their previous birth (recommended). Women with previous live births resulting from pregnancies started more than 50 complete months before the index birth were censored because longer intervals tend to have missing previous live birth data.
We compared IPI categories by maternal age (in years), race/ethnicity, education, insurance status, risk level, and route of delivery to examine important maternal demographic differences in IPI. Maternal age was calculated using the interval from the woman’s date of birth to the start date of the index pregnancy; probable ages 12–54 years were included. Maternal race/ethnicity and highest level of education were obtained by self-report from the birth certificate. Insurance status was obtained by childbirth delivery payer source and stratified into a dichotomous variable for Medicaid vs other payers. The presence of pregnancy complications was used to categorize patients into high-risk and low-risk strata. Route of delivery, including presence of labor, were identified with International Classification of Diseases-version 9-Clinical Modification (ICD-9-CM) diagnostic codes using previously validated algorithms (Korst et al. 2014).
The outcome measures examined were early preterm delivery (prior to 34 completed weeks), low birth weight (less than 2500 g), stillbirth/intrauterine fetal death (IUFD), neonatal death, and composite indicators, which included neonatal complications (e.g., birth trauma, respiratory problems, sepsis), maternal complications (e.g., birth trauma, postpartum hemorrhage, venous thromboembolism, renal failure), severe maternal complications (maternal complications with critical presentation), and delivery complications, a composite measure of complications for the mother/infant dyad. Preterm delivery was calculated using the obstetric estimate from the birth certificate. The composite indicators were employed to capture the wide range of potential morbidity (including rare events), and to focus attention not on a single condition, but on the opportunity to recognize and explore multiple causes of birth outcomes within the maternal-fetal dyad (Korst et al. 2014). Birthweight was also obtained from the birth certificate, stillbirth/IUFD from the maternal discharge records’ ICD-9-CM diagnosis codes and neonatal death was obtained from the newborns’ discharge disposition. Maternal and neonatal conditions used in composite measures were assessed by examining ICD-9-CM diagnosis and procedure codes for the presence of any codes related to the condition of interest. The focus of the composite indicators is morbidity associated with childbirth among singleton term live born infants; therefore multiple gestation, preterm, and stillbirth/IUFD deliveries were excluded from analysis of all composite indicators.
Trends over the 2007–2009 birth cohorts were summarized and the percentage change between 2007 and 2009 was reported. Trends were tested using the Cochran-Armitage two-sided linear trend test. After combining the 3 years of data, χ2 tests were used to test the categorical association between the IPI and: (1) demographic variables and (2) birth outcomes (singleton index deliveries only). P values <0.05 were regarded as statistically significant. Odds ratios (OR) were calculated for the association between birth spacing intervals (recommended IPI as the referent category) and demographic and outcome variables; these are expressed with Wald 95 % confidence intervals (CI). ORs were also calculated for the association between birth spacing intervals and selected birth outcomes stratified by race/ethnicity. Data analyses were completed using SAS, version 9.3 (Cary, NC). This research was conducted in accordance with ethical principles for the protection of human subjects and was approved by the California Committee for the Protection of Human Subjects and by the Cedars-Sinai Medical Center Institutional Review Board.
Results
The OSHPD dataset included 1,586,987 deliveries that occurred between 2007 and 2009 that were linked to the birth certificate. Of these, 938,708 were identified as “non-first births,” and of these, 286,688 were excluded because they had an IPI ≥51 months and 6491 were excluded because of an IPI <5 months. The remaining 645,529 deliveries (638,239 singleton deliveries) remained in the final study population. Out of those, 36,143 (5.6 %) deliveries were among women with an IPI less than 6 months (rapid repeat births), 213,557 (33.1 %) were among women with an IPI of 6–17 months (intermediate) and 395,829 (61.3 %) were among women with an IPI of 18–50 months (recommended). Table 1 presents the IPI data for 2007–2009. The rate of rapid repeat birth decreased from 5.8 % in 2007 to 5.3 % in 2009, representing an 8.6 % decrease (p < 0.0001). During the same 3-year period, there were non-significant fluctuations in the percentage of women delivering during the intermediate interval, resulting in no net change. The percentage of women delivering in the recommended interval (18 to <51 months) increased slightly during the 3-year period from 61.3 to 61.8 %, a 0.8 % increase.
There were distinctive demographic patterns in age, race/ethnicity, maternal education, and insurance type associated with birth spacing. Women aged 24 and younger were most likely to experience rapid repeat birth and least likely to have a recommended IPI. Teenagers (age 19 and younger) had the highest rate of rapid repeat birth (16.7 %, Table 2), a rate more than three times as high as any age group over 25. Teenagers were also the most likely to have an intermediate IPI and thereby also least likely to have the recommended IPI.
Pacific Islander women had the highest prevalence of rapid repeat birth (12.6 %) followed by American Indian women (10.3 %), whereas White and Asian women had the lowest (3.8 and 4.0 %, respectively). Compared to White women (OR [95 %CI] relative to recommended IPI), Pacific Islander women were more likely to experience rapid repeat birth (4.22 [3.79–4.70]), followed by American Indian women (3.14 [2.74–3.59]) and Black women (2.42 [2.31–2.54]). College-educated women had the lowest rates of rapid repeat birth (3.6 %); women who completed high school or less than high school were twice as likely to experience rapid repeat birth (2.11 [2.05, 2.17] and 2.09 [2.04, 2.15], respectively). Women with Medicaid (Medi-Cal) insurance were twice as likely to experience rapid repeat birth as women with other insurance payers (2.16 [2.11–2.21]). Minor differences in IPIs were observed when comparing high-risk and low-risk multiparous women; high-risk women were more likely to have short IPIs and less likely to have intermediate IPIs (1.34 [1.31–1.38] and 0.98 [0.96–0.99]). Multiparous women without a prior cesarean were slightly more likely to have shorter IPIs (1.17 [1.14, 1.20]) than women with a prior cesarean.
Birth Outcomes
Statistically significant differences were observed for each of the maternal and neonatal outcomes (Table 3). However, when comparing the rapid repeat birth and the intermediate IPI to the recommended IPI, different patterns emerged.
Women with a rapid repeat birth were more likely to have the following conditions compared to women with the recommended IPI: early preterm birth (2.02 [1.89–2.17]), low birthweight (1.72 [1.64–1.80]), neonatal complications (1.36 [1.27–1.46]), neonatal death (1.52 [1.13–1.95]), and severe maternal complications (1.17 [1.07–1.29]).
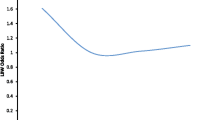
The clearest pattern was observed for the association between IPI and early preterm birth. Women with rapid repeat births were more likely to experience early preterm birth and there appeared to be an inverse relationship with IPI whereby the prevalence of early preterm birth decreased as the IPI increased. Women with intermediate IPI were also slightly more likely to experience early preterm birth than women with the recommended IPI (1.07 [1.03–1.12]). Apart from early preterm birth, there was not a clear pattern in the likelihood of these conditions when comparing women with an intermediate IPI to those with the recommended IPI.
A parabolic pattern was observed for stillbirth/IUFD and the composite measure of complicated delivery. Women with rapid repeat births had the highest prevalence of each condition (0.34 and 9.8 %, respectively); however, there was not a significant difference in prevalence when comparing rapid repeat birth and the recommended IPI. Women with an intermediate IPI had a lower odds of stillbirth/IUFD (0.87 [0.79–0.97]) and complicated delivery (0.94 [0.92–0.96]).
Contrary to expectation, women with the recommended IPI had significantly more maternal complications (7.7 %) than women with rapid repeat birth and intermediate IPI; the percentage of women experiencing maternal complications did not differ between the rapid repeat birth and intermediate IPI groups (7.1 % each). However, women with rapid repeat IPI had higher odds of severe maternal complications (1.17 [1.07, 1.29]).
Birth Outcomes by Race/Ethnicity
Stratification was performed for each of the birth outcomes by race/ethnicity. The clearest pattern was observed for early preterm birth. Table 4 shows the odds ratios for early preterm birth, comparing rapid repeat birth and intermediate IPI to the recommended interval. With the exception of Pacific Islander and American Indian women, the women with rapid repeat birth in each race/ethnic group were more likely to experience early preterm birth. The odds ratios were highest for multi-race women (3.42 [2.19–5.36]) and lowest for black women (1.40 [1.13–1.73]). Apart from Hispanic women (1.10 [1.03–1.17]), the odds of early preterm birth were not significantly different when comparing women with an intermediate interval to those with the recommended IPI.
Discussion
Our study describes birth spacing patterns and their association with birth outcomes among California women, and provides clear evidence of the need to strengthen postpartum and interconception health within key populations. Overall, we noted a significant decline in rapid repeat births, a stable birthrate for the intermediate IPI, and a slight increase in births in the recommended IPI. Differences in birth spacing however were starkest for younger women; teenage women were most likely to experience rapid repeat birth and least likely to have an index birth in the recommended IPI. This pattern occurred within the context of a 6.3 % decline in the overall California birthrate and an 11.7 % drop in the teen birthrate (ages 15–19) between 2007 and 2009. The repeat teen birth rate, however, decreased by just 2.2 %, indicating less progress in preventing repeat births than in the overall prevention of teen births (California Department of Public Health 2014b). While only 18 % of births to teens are repeat births, these data suggest that teens are more likely to have a short intervening period. While older age is associated with biological risks, younger age has social risks; in demographic analyses, younger women were least likely to have completed high school or college and were twice as likely as college-educated women to have had rapid repeat births (data not shown). Such findings underscore the value of programs such as the Adolescent Family Life Program and California Home Visiting Program dedicated to preventing repeat teen births and supporting high school completion.
Part of the study period corresponds to a national economic downturn which may have had a stronger impact on birth spacing among older women as compared to teens. Macro-level economic shifts may have direct impact on families; nationwide, 14 % of women aged 18–34 years and 8 % of women age 35–44 years reported that they postponed having a child because of the recession (Wang et al. 2009). For those women who already had children in California, this may have resulted in a shift from a shorter IPI to a longer one.
Pacific Islander and American Indian women were most likely to experience rapid repeat birth, least likely to give birth in the recommended interval, and their likelihood of rapid repeat birth was three to four times higher than White and Asian women. The factors underlying this finding are unclear, but the trend mirrors low rates of self-reported mistimed or unwanted pregnancies among White and Asian women responding to the California Maternal and Infant Health Assessment (MIHA), a population-based survey of postpartum California women (California Department of Public Health 2011).
Women insured by Medicaid were twice as likely as women insured by other payers to have rapid repeat births and women with unknown or missing insurance status were three times as likely as women with other payers to have short IPIs. Since the study period is prior to the implementation of the Patient Protection and Affordable Care Act (ACA) many women were only eligible for insurance during pregnancy and early postpartum (Lee and McConville 2011). Women with incomes up to 200 % of the Federal Poverty Level are likely to have been eligible for free or sliding scale family planning services through Title X and Family Planning, Access, Care and Treatment Program (Family PACT) programs prior to the implementation of ACA (California Department of Health Care Services 2015); however, women above that financial threshold may not have been able to access contraception through their insurance plan (U.S. Department of Health Care Services 2011). The highest likelihood of rapid repeat birth among women with missing/unknown insurance status may reflect an inability to access existing emergency coverage provisions during pregnancy and may reflect a population with higher social risk factors. Importantly, implementation of preventive services through ACA, the promotion and insurance coverage of long acting reversible contraceptives (LARC), and new data regarding LARC’s safety and efficacy when initiated in the immediate postpartum period could significantly decrease the rate of rapid repeat births in teenagers and women with Medicaid insurance (Rodriguez et al. 2014).
Studies of women with IPIs <18 months have shown an association with adverse maternal and neonatal birth outcomes and our results confirm this association (Conde-Agudelo et al. 2006, 2012; Salihu et al. 2011) with the following caveats: (1) the shortest birth intervals demonstrated a consistently increased risk for most of the birth outcomes, but unlike previous studies, the increased risk was demonstrated almost exclusively for the rapid repeat births (IPI <6 months). This pattern was also observed when stratifying the association of IPI and early preterm birth by race/ethnicity. The notable exceptions were American Indian and Pacific Islander women, both of which had small samples. (2) For the majority of the birth outcomes, the intermediate interval did not appear to put women at higher risk. For early preterm birth, the effect associated with intermediate interval only differed significantly from the recommended interval among Hispanic women. This finding is consistent with the only other similar study previously performed in California; that study included Mexican-origin and non-Hispanic White women and found that IPIs <18 months and >59 months were associated with increased preterm birth risk (Fuentes-Afflick and Hessol 2000). Collectively, these findings suggest that future studies on birth spacing will need to take into consideration race/ethnicity, the outcome of index pregnancy (e.g., gestational age, live birth), and the outcome of subsequent pregnancy as the risks may vary for each of these covariates.
Our data suggest that the highest risk for poor birth outcomes in California is observed for women experiencing rapid repeat birth. Therefore, minor shifts in the length of the IPI from rapid repeat birth to the intermediate interval may have appreciable impact on the risk for poor birth outcomes in California (Rodriguez et al. 2015). If we assume that the higher risk for poor outcomes among women with rapid repeat birth is due to the IPI, we can apply the outcome rates for other IPI categories to the rapid repeat births to determine how much they would change if the IPI were longer. Using this methodology, increasing the IPI beyond 6 months for rapid repeat index deliveries would reduce the risk (for these deliveries) of preterm birth by 47 %, low birthweight by 38 %, neonatal death by 29 %, neonatal complications and stillbirth by 26 %, severe maternal complications by 20 %, and complicated delivery by 6 %. Estimates of the societal costs of preterm birth above and beyond what would have been expended for infants born at term are $51,600 per infant of which $33,200 are medical costs and $3800 are maternal delivery costs, and the remainder are early intervention, lost productivity, and special education costs (Institute of Medicine et al. 2007). If we apply these estimates to preterm birth and are able to shift the rapid repeat index deliveries to the intermediate interval, the estimated savings would be $25.4 million dollars in societal costs of which $16.4 million would be direct health care costs.
The primary limitations of our study are the potential for interval misclassification and exclusion of possibly eligible prior or index deliveries due to unobserved information. The dataset does not include prior stillbirths, intrauterine fetal demise or pregnancies with gestational length less than 24 weeks, resulting in some women having a shorter non-pregnant interval than reported. We were also unable to account for deliveries not reporting to OSHPD (e.g., military hospitals, home deliveries, and inter-state migration). Deliveries with an IPI longer than 50 months were excluded from analysis as they comprise a different risk group and are prone to misclassification due to the difficulty in accounting for and verifying long IPI gaps. We expect that the potential birth spacing misclassification associated with our approach resulted in conservative estimates of short birth spacing patterns and their impact, thus increasing confidence in the results. In addition, we did not adjust by age or risk group because in our conceptual model age is a moderator and risk group is an intermediary; this may have contributed to the reported higher rate of maternal complications in the recommended IPI group, which was also the oldest. Again, we believe this approach results in conservative estimates of effect.
The timing of future pregnancies is influenced by many sociodemographic and economic factors such as age, sibling age interval, economic factors, and childcare access (Bryant et al. 2012) or, as is the case for almost one-third of live births in California, may be caused by unintended pregnancy (California Department of Public Health 2011). While public health has limited control over the social factors driving the timing of intentional pregnancies, reducing unintended pregnancies is within the purview of intervention, and additional research is needed to determine the influence of unintended pregnancy on rapid repeat birth. In published studies, an estimated 17–22 % of women resumed sexual intercourse by 4 weeks postpartum (Barrett et al. 2000; Faisal-Cury et al. 2015) which is commonly before the postpartum visit. Furthermore, data suggest that only 39 % of postpartum women discussed birth spacing with their provider (California Department of Public Health 2010). To address these factors, California Medicaid has adopted a policy to facilitate immediate postpartum LARC placement. Outreach programs are attempting to increase the attendance at postpartum visits by scheduling them earlier and promoting the visit during prenatal care. The Interconception Care Project of California guidelines standardize the content of the postpartum visit and emphasize universally addressing contraception and birth spacing (Preconception Health Council of California 2012).
While the risk of short non-pregnant intervals between pregnancies is repeatedly observed, alternative cut points may be relevant for different populations and clinical conditions. For example, short IPI’s (<6 months) may be appropriate after first trimester miscarriages (El Behery et al. 2013; Bigelow and Bryant 2015). Future research should establish a mechanism to explain adverse outcomes related to birth spacing, which may allow the tailoring of birth spacing to individual risk profiles. Meanwhile, existing insurance and public health programs that provide contraception and promote education about birth spacing can significantly impact the rate of short IPI, shifting repeat pregnancies into lower risk time periods with the potential for significant reduction in morbidity and healthcare costs.
References
American Congress of Obstetricians and Gynecoloists. (2012). The importance of contraceptive care to women’s medical care. ACOG Professional Letter. Retrieved Mar 2, 2016 from https://www.acog.org/~/media/Departments/Government%20Relations%20and%20Outreach/201202ImpOfContraception.pdf.
Barrett, G., Pendry, E., Peacock, J., et al. (2000). Women’s sexual health after childbirth. BJOG: An International Journal of Obstetrics and Gynaecology, 107(2), 186–195.
Bigelow, C. A., & Bryant, B. A. (2015). Short interpregnancy intervals: An evidence-based guide for clinicians. Obstetrics and Gynecology Survey, 70(7), 458–464. doi:10.1097/OGX.0000000000000195.
Bryant, A., Fernandez-Lamothe, A., & Kuppermann, M. (2012). Attitudes toward birth spacing among low-income, postpartum women: A qualitative analysis. Maternal and Child Health Journal, 16(7), 1440–1446. doi:10.1007/s10995-011-0911-9.
Bujold, E., & Gauthier, R. J. (2010). Risk of uterine rupture associated with an interdelivery interval between 18 and 24 months. Obstetrics and Gynecology, 115(5), 1003–1006. doi:10.1097/AOG.0b013e3181d992fb.
California Department of Health Care Services. (2011). Family PACT client eligibility/enrollment. California Department of Health Care Services, Sacramento, CA. Retrieved Sep 3, 2015 from http://www.familypact.org/Providers/client-eligibility-enrollment.
California Department of Public Health. (2010). Maternal Infant Health Assessment (MIHA) Snapshot, California. Sacramento, CA.
California Department of Public Health. (2011). Maternal Infant Health Assessment (MIHA) Snapshot, California. Sacramento, CA.
California Department of Public Health. (2014a). California’s Infant Mortality Rate Continues to Decline, But Disparities Persist. Sacramento, CA. Retrieved Sep 3, 2015 from https://www.cdph.ca.gov/Pages/NR14-006.aspx.
California Department of Public Health. (2014b). California Teen Births 2000–2012. Sacramento, CA. Retrieved Sep 3, 2015 from https://www.cdph.ca.gov/programs/mcah/Documents/MO-MCAH-2012TBR-DataSlides.pdf.
Conde-Agudelo, A., Rosas-Bermudez, A., & Kafury-Goeta, A. C. (2006). Birth spacing and risk of adverse perinatal outcomes: A meta-analysis. JAMA, 295(15), 1809–1823. doi:10.1001/jama.295.15.1809.
Conde-Agudelo, A., Rosas-Bermudez, A., & Kafury-Goeta, A. C. (2007). Effects of birth spacing on maternal health: A systematic review. American Journal of Obstetrics and Gynecology, 196(4), 297–308. doi:10.1016/j.ajog.2006.05.055.
Conde-Agudelo, A., Rosas-Bermudez, A., Castano, F., et al. (2012). Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Studies in Family Planning, 43(2), 93–114.
El Behery, M. M. S. S., Seksaka, M. A., & Ibrahim, Z. M. (2013). Reproductive performance in the next pregnancy for nulliparous women with history of first trimester spontaneous abortion. Archives of Gynecology and Obstetrics, 288(4), 939–944. doi:10.1007/s00404-013-2809-9.
Faisal-Cury, A., Menezes, P. R., Quayle, J., et al. (2015). The relationship between mode of delivery and sexual health outcomes after childbirth. The Journal of Sexual Medicine, 12(5), 1212–1220. doi:10.1111/jsm.12883.
Fridman, M., Korst, L. M., Chow, J., et al. (2014) Trends in maternal morbidity before and during pregnancy in California. American Journal of Public Health, 104(Suppl 1), S49–57. doi:10.2105/AJPH.2013.301583.
Fridman, M., El Haj Ibrahim, S., Griffin, F., et al. (2015). Trends in maternal morbidity, California 2007 to 2009: Report of Statewide and County levels of preexisting maternal health conditions, pregnancy complications, severe maternal and neonatal complications. California Department of Public Health, Center for Family Health, Maternal, Child and Adolescent Health Division, Sacramento, CA. Retrieved Sep 3, 2015 from https://www.cdph.ca.gov/programs/mcah/Documents/MCAH_Morbidity%20Trends%20Report__12Jan2016.pdf.
Fuentes-Afflick, E., & Hessol, N. A. (2000). Interpregnancy interval and the risk of premature infants. Obstetrics and Gynecology, 95(3), 383–390.
Getahun, D., Strickland, D., Ananth, C. V., et al. (2010). Recurrence of preterm premature rupture of membranes in relation to interval between pregnancies. American Journal of Obstetrics and Gynecology, 570(6), e1–e6. doi:10.1016/j.ajog.2009.12.010.
Institute of Medicine Preterm Birth. (2007). Causes, consequences, and prevention. Behrman, R. E., Butler, A. S. (Eds.), Washington, DC: National Academies Press (US).
Johnson, K., Posner, S. F., Biermann, J., et al. (2006) Recommendations to improve preconception health and health care–United States. A report of the CDC/ATSDR preconception care work group and the select panel on preconception care. MMWR. Recommendations and reports: Morbidity and mortality weekly report. Centers for Disease Control and Prevention. 55(RR-6), 1–23.
Korst, L. M., Fridman, M., Lu, M. C., et al. (2014). Monitoring childbirth morbidity using hospital discharge data: Further development and application of a composite measure. American Journal of Obstetrics and Gynecology, 211(3), 268.e1–268.e16. doi:10.1016/j.ajog.2014.03.011.
Lee, H., & McConville, S. (2011). Expanding Medi-cal: Profiles of potential new users. San Francisco, CA: Public Policy Institute of California 2011. Retreived Sep 3, 2015 from http://www.ppic.org/content/pubs/report/R_811HLR.pdf.
March of Dimes Prematurity Campaign. (2013). Progress Report. White Plains, NY. March 14, 2014, #37-2695-14. Retreived Sep 3, 2015 from http://www.marchofdimes.org/materials/prematurity-campaign-progress-report-2013.pdf.
Moore, L. E. (2008). Recurrent risk of adverse pregnancy outcome. Obstetrics and Gynecology Clinics of North America, 35(3), 459–471, ix. doi:10.1016/j.ogc.2008.04.003.
Preconception Health Council of California. (2012). Interconception Care Project of California Guidelines. Retreived Feb 18, 2016 from http://www.everywomancalifornia.org/content_display.cfm?contentID=359&categoriesID=120&CFID=9842306&CFTOKEN=e693932abb1b95e6-46EE283A-9986-420E-2A0DF1EE8B960EBE.
Rutstein, S. O. (2005) Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: Evidence from the demographic and health surveys. International Journal of Gynecology and Obstetrics, 89(Suppl 1), S7–24. doi:10.1016/j.ijgo.2004.11.012.
Rodriguez, M. I., Evans, M., & Espey, E. (2014). Advocating for immediate postpartum LARC: Increasing access, improving outcomes, and decreasing cost. Contraception, 90(5), 468–471. doi:10.1016/j.contraception.2014.07.001.
Rodriguez, M. I., Chang, R., & Thiel de Bocanegra, H. (2015). The impact of postpartum contraception on reducing preterm birth: Findings from California. American Journal of Obstetrics and Gynecology. doi:10.1016/j.ajog.2015.07.033.
Salihu, H. M., August, E. M., Mbah, A. K., et al. (2011). The impact of birth spacing on subsequent feto-infant outcomes among community enrollees of a federal Healthy Start project. Journal of Community Health, 37(1), 137–142. doi:10.1007/s10900-011-9427-x.
Shachar, B. Z. L. D. (2012). Interpregnancy interval and obstetrical complications. Obsterics and Gynecology Survey, 67(9), 584–596. doi:10.1097/OGX.0b013e31826b2c3e.
Stamilio, D. M., DeFranco, E., Pare, E., et al. (2007). Short interpregnancy interval: Risk of uterine rupture and complications of vaginal birth after cesarean delivery. Obstetrics and Gynecology, 110(5), 1075–1082. doi:10.1097/01.AOG.0000286759.49895.46.
U.S. Department of Health Care Services. (2011). Women’s Preventive Services Guidelines Affordable Care Act Expands Prevention Coverage for Women’s Health and Well-Being. Health Services Resources and Services Administration. Rockville, MD. Retreived Sep 3, 2015 from http://www.hrsa.gov/womensguidelines/.
Wang, W., & Morin, R. (2009). Recession brings many young adults back to the nest: Home for the Holidays…and every other day. Washington, D.C. Pew Research Center.
World Health Organization. (2006). Report of a WHO Technical Consultation on Birth Spacing, 13–15 June 2005. Geneva, Switzerland. Retreived Sep 3, 2015 from http://www.who.int/maternal_child_adolescent/documents/birth_spacing.pdf.
Acknowledgments
Financial support for this work was provided by federal Title V MCH block grant funding through the California Department of Public Health (CDPH), Maternal, Child and Adolescent Health (MCAH) Division under State of California Agreement Number 15-10008. We acknowledge the contributions of Samia El Haj Ibrahim (Cedars Sinai Medical Center, Department Obstetrics and Gynecology) for her assistance with manuscript drafts and Naomi H. Greene for her review of the manuscript. We also thank Marina Chabot and Dan (Susan) Sun of CDPH, MCAH for their critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declared no conflict of interest.
Rights and permissions
About this article

Cite this article
Cofer, F.G., Fridman, M., Lawton, E. et al. Interpregnancy Interval and Childbirth Outcomes in California, 2007–2009. Matern Child Health J 20 (Suppl 1), 43–51 (2016). https://doi.org/10.1007/s10995-016-2180-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-016-2180-0