
Abstract
Objective
To assess the risk for neurodevelopmental delays for children of mothers who were obese (≥200 pounds) prior to pregnancy, and to characterize delays associated with maternal obesity among children referred to and found eligible to receive Early Intervention Program services.
Methods
We conducted a retrospective cohort study (N = 541,816) using a population-based New York City data warehouse with linked birth and Early Intervention data. Risks for children suspected of a delay and ‘significantly delayed’, with two moderate or one severe delay, were calculated. Among the group of children eligible by delay for Early Intervention, analyses assessed risk for being identified with a moderate-to-severe delay across each of five functional domains as well as risks for multiple delays.
Results
Children of mothers who were obese were more likely to be suspected of a delay (adjusted RR 1.19 [CI 1.15–1.22]) and borderline association for ‘significantly delayed’ (adjusted RR 1.01 [CI 1.00–1.02). Among children eligible by delay, children of mothers who were obese evidenced an increased risk for moderate-to-severe cognitive (adjusted RR 1.04 [CI 1.02–1.07]) and physical (adjusted RR 1.04 [CI 1.01–1.08]) delays and for global developmental delay (adjusted RR 1.05 [CI 1.01–1.08]).
Conclusion
Maternal obesity is associated with increased risk of developmental delay in offspring. Among children with moderate or severe delays, maternal obesity is associated with increased risk of cognitive and physical delays as well as with increased risk for global developmental delay. While causation remains uncertain, this adds to the growing body of research reporting an association between maternal obesity and neurodevelopmental delays in offspring.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
What is already known on this subject?
Obesity of the mother during pregnancy impacts physical and mental health of her offspring.
What this study adds?
Obesity of the mother during pregnancy appears to be linked to substantial, severe and specific developmental delays in early childhood. Children of mothers who were obese during pregnancy had significantly higher risks of cognitive, physical, and global developmental delays, even after controlling for important maternal and infant risk factors.
Introduction
Obesity during pregnancy contributes to increased risks for maternal health issues, as well as adverse pregnancy outcomes and increased health risks for the offspring [1–5]. Recent studies focusing on longer-term risks for offspring of pre-pregnancy obesity in the mother suggest an association with neurodevelopmental delays in early childhood. While some prior studies found no association with maternal obesity and offspring’s motor development [6, 7], attention, non-verbal [8] or verbal skills [6], recent studies have reported an association with cognitive delays or impairment [7, 9, 10] and developmental delays [11] in early childhood, as well as behavior problems [12] and autism [11]. A burgeoning field of study, the risks for neurodevelopmental delays and severity of delays associated with maternal obesity is not well characterized. With the high prevalence of obesity affecting over 30 % of US women of child-bearing age [13], identifying the associated risks is of public health importance. Additionally, as developmental delays are noted to be amenable to change, negative long-term effects could be mitigated by early detection and intervention [14].
Using a large and diverse urban cohort, this study aims to contribute to the growing body of research by assessing risk for delays across a range of five functional domains used to identify developmental delays in early childhood: communication, cognitive, physical, social–emotional, and adaptive, among a high-risk cohort of children referred and found eligible for Early Intervention services. Additionally, we consider the complexity of delays for children of mothers who were obese prior to pregnancy, assessing risk for multiple delays, simultaneously.
Methods
Population
This study comprised a birth cohort of children born in New York City (NYC) of resident mothers from 1994 to 2001 (N = 541,816) with the study focusing on those receiving a referral to the NYC Early Intervention Program through 2004 (N = 59,589) and a subset of those referred and found eligible by delay for Early Intervention services (N = 45,709). Data were obtained from the Longitudinal Study of Early Development data warehouse, a compilation of linked de-identified data from birth and death certificates and Early Intervention Program records from the NYC Department of Health and Mental Hygiene.
The cohort of children referred to Early Intervention was limited to those who had been born in NYC and who had been referred to Early Intervention in NYC. Therefore, it did not include those who moved into NYC, or those who moved out of NYC prior to being referred for early intervention services. Inclusion criteria identified children of mothers 18–45 years at delivery, singleton pregnancies, and children born at 32 weeks or more gestational age. Children of mothers with sexually-transmitted diseases and rubella, as well as children with congenital anomalies at birth, were excluded. If, after exclusions, children of the same mother remained in the cohort, one child was randomly selected and the other(s) excluded. List-wise deletion was employed for missing data.
Measures
Since maternal height data were unavailable, maternal body mass index (BMI) could not be calculated. Using weight data, obesity was categorized as pre-pregnancy weight of 200 pounds or more. The 200 pound cut-point has been used in prior studies to categorize maternal obesity when height data were not available [15–17]. Based on the US standard for obesity (BMI ≥ 30 kg/m2) [18], approximately 0–5 % of women would not be obese at 200 pounds (NYC DOHMH 2014) [19].
We controlled for socio-demographic variables, including maternal and infant characteristics obtained from birth certificate records. Self-reported maternal variables were coded as noted in Table 1: maternal race/ethnicity (Non-Hispanic black, Non-Hispanic white, Hispanic, Asian, Other), age (18 < 20, 20 < 35, 35+ years), education level (<high school education yes/no), nativity (foreign born yes/no), marital status (married yes/no), insurance payer (Medicaid yes/no), parity (nulliparous yes/no), and drug use during pregnancy (smoking, drinking, drugs yes/no). Maternal weight gain was considered excessive if women <200 pounds gained >40 pounds or if women 200 pounds or more gained >25 pounds. A variable indicating maternal diabetes included women with either chronic or gestational diabetes. Infant characteristics included infant year of birth, birth weight (<1500, 1500–2499, 2500–3999, 4000–6000), and preterm birth (32–36 weeks/>36 weeks). Since specific delays are more prevalent at different developmental stages, we also adjusted for the influence of the child’s age at referral on their risk for delays. The age at first referral, obtained from Early Intervention records, was categorized into five age-spans: 0–11, 12–17, 18–23, 24–29, and 30+ months.
Referred to Early Intervention Children referred to the NYC Early Intervention program at any time from birth to 3 years of age were categorized as ‘suspected of having a developmental delay’. Early Intervention is a government program established by the Education of the Handicapped Act Amendments of 1986 (renamed in 1990, the Individuals with Disabilities Education Act), enacted to ensure infants and toddlers with developmental delays receive services (PL 99-457) [20, 21]. Children suspected of having a developmental delay can be referred to Early Intervention by parents directly, or by medical or social service professionals with parental permission [22].
Eligible by Delay for Early Intervention Services Each child referred to Early Intervention is expected to be assessed for delays across five functional domains: communication, cognitive, physical (fine/gross motor, hearing, vision), social–emotional, and adaptive (life skills) [20, 23, 24]. In line with the NYC Early Intervention definition, a ‘significant delay’ was defined as having at least a 12-month or 33 % delay in any one domain, or a 25 % delay in each of two domains, or performing at least 2.0 standard deviations (SD) below the mean on assessments in one domain or 1.5 SD below the mean on assessments in each of two domains [22]. Children identified with a ‘significant delay’ are eligible by delay for Early Intervention in NYC. While most children eligible for Early Intervention are found eligible by delay, children can also be eligible for Early Intervention if they are identified with a condition that is known to result in developmental delays (e.g., infantile cerebral palsy) [25].
Characterizing Risk in Functional Domains Among children fully evaluated and found eligible by delay for Early Intervention, we characterized risks for specific delays across the five functional domains for children of mothers who were obese prior to pregnancy. A delay was defined by 1.5 SD or more below the mean on assessments in a specific domain or exhibiting at least a 25 % chronological age delay in a specific domain. Accordingly, this category comprised children evaluated and identified with a moderate or severe delay in the noted domain. Based on the data available from Early Intervention records, children with a mild delay (1.0 SD to less than 1.5 SD below the mean) were included in the ‘no delay/mild delay’ reference group.
Children were considered to have a global developmental delay if they have a severe delay (at least 2.0 SD below the mean on assessments) in two or more domains [26, 27].
This study was approved by the Department of Health and Mental Hygiene Institutional Review Board.
Statistical Analysis
Chi-square statistics were computed to compare groups in relation to maternal and perinatal data. Bivariate and multiple regression analyses were conducted to evaluate the associations between maternal obesity and children being referred to Early Intervention at any time and eligible by delay for Early Intervention. Among those found eligible by delay, analyses were also conducted to assess the risk for a delay in each of the five domains, a global developmental delay, and a delay in all five domains simultaneously. All associations were assessed with significance set at p < .05. Covariates were identified a priori based on prior research; as such, models were not corrected for multiple comparisons.
All analyses were conducted using SAS 9.3 (SAS Institute Inc., Cary, NC). We used the log-binomial genmod procedure to obtain relative risks. Log-binomial models that did not converge were assessed using Poisson regression with robust error variance and an unstructured correlation matrix for obtaining relative risks [28, 29]. Multiple models for each outcome variable were assessed: the main effect models, models controlling for all maternal and infant covariates, and, when assessing risk for delays, full models also adjusted for age at first referral.
Additional analyses were conducted to confirm and elucidate results. As a sensitivity analysis, to assess attenuation of risk related to women who were obese but weighed less than 200 pounds and to ensure that risks related to severe obesity were not exaggerating the risks for children of mothers who were obese, we assessed relative risks differentiating maternal weight by five weight categories (<100, 100–149 [reference], 150–199, 200–299, ≥300). An additional sensitivity analysis was conducted to assess any change in the risk for children of women who were obese when controlling for neighborhood poverty level. Poverty levels were categorized as in Vital Statistics records to report the percent of families living in poverty in the neighborhood (0–4, 5–9, 10–19, 20–29 and ≥30 %). Furthermore, to benchmark the risks found in this high-risk population of those evaluated for Early Intervention, relative risks for children of mothers who had less than a high school education were assessed to serve as a comparison to understand magnitude of risks found for maternal obesity. In all analyses, final full models were not reduced, but rather included all conditions and covariates. Proportional change in variance for the full models assessing risk for each developmental delay was assessed using McFadden’s pseudo-R2.
Results
Maternal and perinatal characteristics for children referred, fully evaluated, and found eligible by delay for Early Intervention are presented in Table 1.
Suspected of Delay, Fully Evaluated, and Eligible by Delay
From the 1994–2001 birth cohort (N = 541,816), 11 % were suspected of a delay and referred to Early Intervention. Compared to children of mothers who weighed less than 200 pounds, children of mothers who were obese prior to pregnancy were 19 % more likely to be suspected of having a developmental delay and referred to Early Intervention (ARR 1.19 [CI 1.15–1.22]).
Of those referred (n = 59,589), 10.4 % did not receive further services, 3.3 % were found eligible for Early Intervention prior to an Early Intervention evaluation, and the remaining 86.3 % were evaluated by Early Intervention (Fig. 1). Of those evaluated, 98.6 % (n = 50,735) received a full evaluation of all five functional domains. Among the 50,735 children referred to Early Intervention and fully evaluated for delays, 90.1 % (45,709) were reported to have at least one severe delay or two or more moderate delays across the five domains (i.e., ‘significantly delayed’), and were thus ‘eligible by delay’ to receive Early Intervention services. Among this NYC birth cohort, children found eligible by delay represent 91.3 % of all children found eligible for Early Intervention services.

Early Intervention Referral, Evaluation, and Delays in 1994–2001 Birth Cohort
Among children suspected of a delay and referred to Early Intervention, maternal obesity was not associated with being fully evaluated, but, among those evaluated, was borderline significant for being ‘eligible by delay’ for Early Intervention services (ARR 1.01 [CI 1.00–1.02]).
Risk for Delays in Functional Domains Among Children Eligible by Delay
Moderate to Severe Delays by Functional Domain
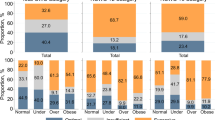
Among children eligible by delay for Early Intervention, being a child of a mother who was obese prior to pregnancy was associated with higher prevalence of a moderate-to-severe cognitive (64.6 vs. 59.9 % [p < .0001]), physical (54.1 vs. 50.5 % [p < .0001]), or social–emotional (46.8 vs. 43.5 % [p = .0002]) delay, as compared to children of mothers weighing less than 200 pounds (Table 2). In fully adjusted models, children of mothers who were obese evidenced an increased risk for a moderate-to-severe cognitive (ARR 1.04 [CI 1.02–1.07]) or physical (ARR 1.04 [CI 1.01–1.08]) delay (Table 3). McFadden’s pseudo-R2 for each model for each domain, which provides an approximate variance in the outcome accounted for by the variables in the model, ranged from 0.03 to 0.25 [adaptive (0.03); cognitive and emotional (0.05); physical (0.13); communication (0.25)].
Severity of Diagnosis
Among children who were eligible by delay for Early Intervention, children of mothers who were obese during pregnancy, compared to children of mothers who weighed <200 pounds, had a higher prevalence of a global developmental delay (52.1 vs. 49.0 %, respectively [p = .0005]), and a moderate-to-severe delay in all five domains (20.4 vs. 17.8 %, respectively [p = .0002]). Increased risk for a global developmental delay remained significant in adjusted risk models (ARR 1.05 [CI 1.01–1.08]). McFadden’s pseudo-R2 was 0.03 for both global developmental delay and the model assessing all five delays simultaneously.
Sensitivity Analyses
Risk for Delays by Refined Maternal Weight Categories and Risk for Delays Controlling for Neighborhood Poverty
Table 4 provides relative risks for delays by five maternal weight categories, among children found eligible by delay. When compared to the reference group of children of mothers weighing 100–149 pounds, children of mothers who weighed 200–299 pounds evidenced increased risk for a moderate-to-severe cognitive (ARR 1.07 [CI 1.04–1.10]) and physical (ARR 1.05 [CI 1.02–1.09]) delay, and a global developmental delay (ARR 1.07 [CI 1.03–1.10]) with slightly increased but similar results to the bivariate analysis which included women weighing 150–199 pounds in the non-obese category. Additionally, compared to the reference group, children of mothers who weighed 200–299 pounds evidenced an increased risk for a moderate-to-severe delay in all five domains (ARR 1.10 [CI 1.02–1.19]).
These results were similar when collapsing the 200–299 pounds obese and 300 pounds-or-more morbidly obese categories. Due to the small number of mothers who were morbidly obese in this cohort (N = 114), we were underpowered to separately report results for this group.
Additionally, sensitivity analyses indicated that relative risks for children of mothers who were obese were similar with or without controlling for neighborhood poverty level (See footnote Table 3).
Benchmarking Risk
Risk for Delays Related to Maternal Education
Magnitude of risks for delays associated with children of mothers with less than a high school education in this high risk group of children found eligible by delay for Early Intervention include a non-significant risk for a moderate-to-severe physical delay (ARR 1.02 [CI .99–1.04]), a 1 % increased risk for a moderate-to-severe communications delay (ARR 1.01 [CI 1.01–1.02]), a 5 % increased risk for a moderate-to-severe cognitive (ARR 1.05 [CI 1.04–1.07]) social–emotional (adjusted RR 1.05 [CI 1.03–1.07]), and global developmental delay (ARR 1.05 [CI 1.02–1.07]), a 6 % increased risk for a moderate-to-severe adaptive delay (ARR 1.06 [CI 1.03–1.09]), and a 9 % increased risk for a moderate-to-severe delay in all five domains (ARR 1.09 [CI 1.04–1.14]).
Discussion
Children of mothers who were obese prior to pregnancy evidenced an increased risk for being suspected of a developmental delay and referred to Early Intervention and for having a ‘significant delay’ and found eligible by delay for Early Intervention. Additionally, in adjusted models, among children who were identified as having a ‘significant delay’ and, thus, found eligible by delay for Early Intervention services, children of mothers who were obese evidenced an increased risk for a moderate-to-severe cognitive and physical delay and an increased risk for global developmental delay. In the sensitivity analysis, compared to a reference group of children whose mothers weighed 100–149 pounds, we also found significant increased risks for children of mothers who were obese to have a delay in all five domains.
Two recent studies support our findings of children of mothers who were obese being at increased risk for a delay in general. A recent study analyzing data from two control groups from a prior medical study, Craig et al. assessed associations between obesity in mothers and three domains in offspring: cognitive, language, and motor, in 101 two-year-old children. A significant association was found for children of mothers who were obese and a composite variable representing the risk for a delay in at least one area [30]. Yet, the authors note that the study may not have been large enough to detect differences in specific domains. Another study using a composite delay variable reported higher odds of having any developmental delay for children of mothers who were obese, but did not report associations between obesity and specific domains assessed [11]. Casas et al. also found an association with cognitive scores but mixed results for psycho-motor scores among 11–22 month old children in two cohorts in Europe [31]. While prior research also suggests an increased risk for attention and behavioral issues including those related to externalizing behavior at 2 years old [12], inattention as reported by teachers [32], and attention deficit hyperactivity disorder (ADHD) [33], further research is needed in each of the functional domains to confirm risks.
The present study extends the current research by characterizing risks across each of five functional domains. Beyond individual delays, we also were able to report on severe delays in two or more domains, which is understood to be a more profound condition than one specific delay, with notable long-term consequences [34]. Children with delays in multiple domains have demonstrated an increased risk for negative long-term school outcomes, such as grade retention or need for special assistance services, and need for special education [35]. Furthermore, children with early global developmental delay are likely to be diagnosed with a lasting impairment [36] and poor performance in all functional domains into the elementary school years [37].
An additional strength of our study includes adjustment for multiple maternal and infant characteristics obtained from official documents. Further, unlike many other studies in this area, we were able to control for the effect of diabetes on risk [38]. In a study on fetal anomalies in obese women, Biggio et al. reported that diabetes was associated with an increased risk for anomalies whereas BMI was not, suggesting that maternal weight ‘may be a surrogate’ for diabetes [16]. In controlling for diabetes, we were able to address this concern in relation to risk for delays in the current study.
A limitation of our study includes potential selection bias. Although Early Intervention is available to all children ages 0–3 years, some children may not have had contact with an adult aware of the system, the referral process, or the child’s need. While this is a limitation of using Early Intervention data to represent all children with moderate-to-severe delays, Early Intervention reportedly captures, not all, but the majority of children with delays in NYC with similar coverage expected before 2004. We conducted sensitivity analyses to explore bias in relation to referral and loss to follow-up and found none.
Analysis for our study was limited by data available in vital statistics records. In the absence of height data we were not able to calculate mothers’ body mass index and had to rely on weight as a measure of obesity as used in previous studies [15–17]. Based on NYC data from the 2002 Community Health Survey and the 2004 Health and Nutrition Examination Survey, our sensitivity analysis comparing the women in the 200–299 pound category with the reference group of women weighing 100–149 pounds would provide 99 % sensitivity and specificity for evaluating obese versus non-obese women (NYC DOHMH 2014). This analysis revealed a slightly higher risk for children of obese mothers weighing 200–299 pounds compared to a reference group of children of mothers weighing 100–149 pounds; an analysis that effectively excluded women who were obese and weighing 150–199 pounds, confirming that our bivariate cut-point provides conservative results. Additionally, our sensitivity analysis addressed the potential concern of exaggerated risk contributed by children of mothers who were severely obese [7]; risks for children of mothers who were obese were found to be similar in analyses with and without those weighing 300 pounds or more. Future cohort studies may assess risks for these various developmental delays across the range of maternal body mass index and ascertain a potential threshold for risk.
While relative risks were not large, results may be noteworthy due to the consistency in findings, the severity of delays reported, and their potential long-term impact. With higher obesity rates in the current generation of women of childbearing age [13], it should be of particular concern that obesity in pregnancy confers a higher risk for severe outcomes in important functional domains, including a global developmental delay. Although risks may seem low, these were risks among a defined high-risk group of children and the magnitude of the risks found for children of mothers that were obese were similar to the magnitude of risk found for other known maternal risk factors; in this study, risks for delays for children of mothers who were obese were not dissimilar to risks reported for children of mothers who did not finish high school.
The American College of Obstetricians and Gynecologists recommend that obese women lose weight before pregnancy. In light of these findings, these recommendations may have implications for child development in addition to the known implications for improved pregnancy outcomes [39]. However, it is important to note that our study does not confirm causality. While our study reports an increased risk for children of obese mothers, it remains unclear if the risk is related to pre-natal or post-natal factors. Studies are needed to better understand effects of obesity on the developing fetus; research suggests mechanisms such as inflammation and leptin levels in mothers who are obese during pregnancy may effect fetal brain structure or function, with the hippocampus, a region central to memory and spatial relations, of particular interest, making our findings related to cognitive and physical delays particularly compelling [40, 41]. Additional factors we were unable to assess may confound this relationship including maternal depression [42], maternal cognitive ability [9], maternal exercise, and breastfeeding [43, 44]. Future studies should examine these covariates.
Nonetheless, the mounting evidence suggests that secondary prevention efforts could be advisable. While causality may be a requisite for touting primary prevention efforts, the consistent associations found with maternal obesity and offspring’s risk for delays may be sufficient to encourage secondary intervention efforts [38]. Early intervention has been reported to be beneficial for both the child and the family and to diminish risks for long-term consequences, such as school retention and delinquency [14, 45]. If pediatricians and other health care providers are made aware of the potential increased risk for developmental delays for children of mothers who were obese during pregnancy, children in need may receive more timely screening and intervention services.
References
Cnattingius, S., Bergstrom, R., Lipworth, L., & Kramer, M. S. (1998). Prepregnancy weight and the risk of adverse pregnancy outcomes. New England Journal of Medicine, 338, 147–152.
Rosenberg, T. J., Garbers, S., Lipkind, H., & Chiasson, M. A. (2005). Maternal Obesity and diabetes as risk factors for adverse pregnancy outcomes: Differences among 4 racial/ethnic groups. American Journal of Public Health, 95(9), 1545–1551.
Brockelsby, J., & Dresner, M. (2006). Obesity and pregnancy. Current Anaesthesia and Critical Care., 17, 125–129.
Davies, G. A. L., Maxwell, C., & McLeod, L. (2010). Obesity in pregnancy. International Journal of Gynecology and Obstetrics., 110, 167–173.
Sebire, N. J., Jolly, M., Harris, J. P., Wadsworth, J., et al. (2005). Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. International Journal of Obesity, 25, 1175–1182.
Neggers, Y. H., Goldenber, R. L., Ramey, S. L., & Cliver, S. P. (2003). Maternal prepregnancy body mass index and psychomotor development in children. Acta Obstetricia et Gynecologica Scandinavica, 82, 235–240.
Hinkle, S. N., Schieve, L. A., Stein, A. D., Swan, D. W., Ramakrishnan, U., & Sharma, A. J. (2012). Associations between maternal prepregnancy body mass index and child neurodevelopment at 2 years of age. International Journal of Obesity., 36, 1312–1319.
Brion, M. J., Zeegers, M., Jaddoe, V., Verhulst, F., et al. (2011). Intrauterine effects of maternal prepregnancy overweight on child cognitive and behavior in 2 cohorts. Pediatrics, 127, e202–e211.
Tanda, R., Salsberry, P. J., Reagan, P. B., & Fang, M. Z. (2013). the impact of prepregnancy obesity on children’s cognitive test scores. Maternal Child Health Journal, 17, 222–229.
Helderman, J. B., OShea, T. M., Kuban, K. C. K., et al. (2012). Antenatal antecedents of cognitive impairment at 24 months in extremely low gestational age newborns. Pediatrics, 129(3), 494–502. doi:10.1542/peds.2011-1796.
Krakowiak, P., Walker, C. K., Bremer, A. A., et al. (2012). Maternal metabolic conditions and risk for autism and other neurodevelopmental disorders. Pediatrics, 129(5), e1121–e11128. doi:10.1542/peds.2011-2583.
VanLieshout, R. J., Schmidt, L. A., Robinson, M., Niccols, A., & Boyle, M. A. (2013). Maternal pre-pregnancy body mass index and offspring temperament and behavior at 1 and 2 years of age. Child Psychiatry and Human Development, 44, 382–390.
Flegal, K. M., Carroll, M. D., Kit, B. K., & Ogden, C. L. (2012). Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA, 307(5), 491–497. doi:10.1001/jama.2012.39.
Majnemer, A. (1998). Benefits of early intervention for children with developmental disabilities. Seminars in Pediatric Neurology, 5, 62–69.
Dodds, L., Fell, D. B., Shea, S., Armson, B. A., Allen, A. C., & Bryson, S. (2011). The role of prenatal, obstetric, and neonatal factors in the development of autism. Journal of Autism and Developmental Disorders, 41(7), 891–902. doi:10.1007/s10803-010-1114-8.
Biggio, J. R., Chapman, V., Neely, C., Cliver, S. P., & Rouse, D. J. (2010). Fetal anomalies in obese women: The contribution of diabetes. Obstetrics and Gynecology, 115(2), 290–296. doi:10.1097/AOG.0b013e3181c9b8c3.
Lu, G. C., Rouse, D. J., DuBard, M., Cliver, S., Kimberlin, D., & Hauth, J. C. (2001). The effect of the increasing prevalence of maternal obesity on perinatal morbidity. American Journal of Obstetrics and Gynecology, 185(4), 845–849. doi:10.1067/mob.2001.117351.
Centers for Disease Control and Prevention. (2012). Overweight and obesity: Adult overweight and obesity. http://www.cdc.gov/obesity/adult/defining.html. Accessed 15 Feb 2013.
McDowell, M. A., Fryar, C. D., Ogden, C. L., & Flegal, K. M. (2008). Anthropometric reference data for children and adults: Unites States, 2003–2006. National Health Statistics Reports, 10,1–45. http://www.cdc.gov/nchs/data/nhsr/nhsr010.pdf. Accessed 27 Feb 2013.
Education of the Handicapped Act Amendments of 1986, Pub. L. No. 99-457, 100 Stat. 1145–1146 (1986).
National Assessment of IDEA Overview (NCEE 2011-4026). Washington, DC: National Center for Education Evaluation and Regional Assistance, Institute of Education Sciences, U.S. Department of Education.
Early Intervention Program Memorandum 2005-02: Standards and Procedures for Evaluations, Evaluation Reimbursement, and Eligibility Requirements and Determination Under the Early Intervention Program. (2005). New York State Department of Health, Early Intervention. (p. 34). Downloaded 11/10/2013 from http://www.health.ny.gov/community/infants_children/early_intervention/memoranda/2005-02/eligibility_criteria.htm#state
Individuals with Disabilities Education Act Amendments of 1991, Pub. L. No. 102-119, 105 Stat. 597.
NICHCY Disability Fact Sheet #9. National Dissemination Center for Children with Disabilities. March 2012. Downloaded 11/10/13 from http://nichcy.org/disability/specific/dd#eval
Early Intervention Memorandum 2005-02: Appendix B -Personnel Qualified to Diagnose EIP Eligible Conditions. New York State Department of Health. Downloaded 11/15/2013 from:http://www.health.ny.gov/community/infants_children/early_intervention/memoranda/2005-02/appendix_b.htm
Riou, E. M., Ghosh, S., Francoeur, E., & Shevell, M. I. (2009). Global developmental delay and its relationship to cognitive skills. Developmental Medicine and Child Neurology, 51(8), 600–606.
Shevell, M. (2013). Personal communication 11/23/2013.
Spiegelman, D., & Hertmark, E. (2005). Easy SAS calculations for risk or prevalence ratios and differences. American Journal of Epidemiology, 162, 199e200. Downloaded 11/3/12 from http://aje.oxfordjournals.org/content/162/3/199.full
Zou, G. (2004). A modified Poisson regression approach to prospective studies with binary data. American Journal of Epidemiology, 159, 702–706.
Craig, W. Y., Palomaki, G. E., Neveux, L. M., & Haddow, J. E. (2013). Maternal body mass index during pregnancy and offspring neurocognitive development. Obstetric Medicine: The Medicine of Pregnancy, 6(20), 20–25.
Casas, M., Chatzi, L., Carsin, A. E., Amiano, P., Guxens, M., Kogevinas, M., et al. (2013). Maternal prepregnancy overweight and obesity, and child neuropsychological development: Two Southern European birth cohort studies. International Journal of Epidemiology, 42(2), 506–517.
Rodriguez, A. (2010). Maternal pre-pregnancy obesity and risk for inattention and negative emotionality in children. Journal of Child Psychology and Psychiatry, 51(2), 134–143.
Rodriguez, A., Miettunen, J., Henriksen, T. B., Olsen, J., Obel, C., Taanila, A., et al. (2008). Maternal adiposity prior to pregnancy is associated with ADHD symptoms in offspring: Evidence from three prospective pregnancy cohorts. International Journal of Obesity, 32, 550–557.
Shevell, M. (2008). Global developmental delay and mental retardation or intellectual disability: Conceptualization, evaluation, and etiology. Pediatric Clinics of North America, 55, 1071–1084.
Van Baar, A. L., van Wassenaer, A. G., Dekker, F. W., & Kok, J. H. (2005). Vey preterm birth is associated with disabilities in multiple developmental domains. Journal of Pediatrics Psychology., 30(3), 247–255.
Levy, Y., Ornoy, A., & Nevo, Y. (2011). Special issue on developmental delay. Developmental Disabilities: Research Reviews, 17, 57–58.
Shevell, M., & Webster, R. (2005). Developmental and functional outcomes at school age of preschool children with global developmental delay. Journal of Child Neurology, 20(8), 648–654.
Van Lieshout, R. J. (2013). Role of maternal adiposity prior to and during pregnancy in cognitive and psychiatric problems in offspring. Nutrition Reviews, 71(Suppl. 1), S95–S101.
American College of Obstetricians and Gynecologists. (2013). Obesity in pregnancy: Committee opinion No. 549. Obstetrics and Gynecology, 121, 213–217.
Boska, P. (2010). Effects of prenatal infection on brain development and behavior: A review of findings from animal models. Brain, Behavior, and Immunity, 24, 881–897.
Bilbo, S. D., & Tsang, V. (2010). Enduring consequences of maternal obesity for brain inflammation and behavior of offspring. FASEB Journal, 24(6), 2104–2115.
Deave, T., Heron, J., Evans, J., & Emond, A. (2008). The impact of maternal depression in pregnancy on early child development. BJOG, 115(8), 1043–1051.
Thorsdottir, I., Gunnarsdottir, I., Kvaran, M. A., & Gretarsson, S. J. (2005). Maternal body mass index, duration of exclusive breastfeeding and children’s developmental status at age of 6 years. European Journal of Clinical Nutrition, 59, 426–431.
Jacobson, S. W., & Jacobson, J. L. (2006). Breastfeeding and intelligence in children. BMJ, 333(7575), 929–930.
Gomby, D. S., Larner, M. B., Stevenson, C. S., Lewit, E. M., & Behrman, R. E. (1995). Long-term outcomes of early childhood programs: Analysis and recommendations. The Future of Children, 5(3), 6–24. Accessible from http://www.jstor.org/stable/1602365. Downloaded 23 Nov 2013.
Acknowledgments
The LSED data warehouse was made possible through the collaboration of the New York City Department of Health and Mental Hygiene and the New York City Department of Education. The authors would like to thank Melissa Pfeiffer and Meredith Slopen for their roles in constructing the data warehouse and preparing the analytic data file used in these analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Duffany, K.O., McVeigh, K.H., Kershaw, T.S. et al. Maternal Obesity: Risks for Developmental Delays in Early Childhood. Matern Child Health J 20, 219–230 (2016). https://doi.org/10.1007/s10995-015-1821-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-015-1821-z