
Abstract
School success predicts many pathways for health and well-being across the life span. Factors promoting or potentially impeding school success are critical to understand for all children and for children with special health care needs (CSHCN), whose life course trajectories are already impacted by their chronic health problems. The 2007 National Survey of Children’s Health was used (1) to estimate national and state prevalence and within and across states disparities in factors promoting school success (engagement, participation, safety) or potentially impeding success (missing school, grade repetition, school identified problems) for all children and CSHCN and (2) to evaluate associations with CSHCN service need complexity and presence of emotional, behavioral or developmental problems (EBD) as well as with school case management policies in states. Among school age children, 60 % experienced all three factors promoting school success (49.3–73.8 % across states), dropping to 51.3 % for CSHCN (39.4–64.7 % across states) and to 36.2 % for the 40 % of all CSHCN who have both more complex service needs and EBD. CSHCN were more likely to experience factors potentially impeding school success. After accounting for child factors, CSHCN living in states requiring case management in schools for children with disabilities were less likely to experience grade repetition (OR 0.65). Within-state disparities between non-CSHCN and CSHCN varied across states. Threats to school success for US children are pervasive and are especially pronounced for CSHCN with more complex needs and EBD. Findings support broad, non-condition specific efforts to promote school success for CSHCN and consideration of state school policies, such as case management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
School and its ancillary network of peer relationships, interactions with teachers and staff, and social activities, occupy a large portion of children’s lives. Within this social environment, education inculcates knowledge and intellectual skills, while molding attitudes and behaviors that influence health. The assessment of school success commonly focuses on the lagging indicators of attendance, grades, and standardized achievement test scores. However, school success also involves development of children’s sense of competence and social belongingness which, when achieved, facilitate school engagement and the motivation to learn, which are leading indicators of academic performance [1].
Engaged and motivated students exhibit more achievement-oriented behaviors (e.g., effort and participation) and are less likely to behave in ways that undermine their school success (i.e., inattentive or aggressive behavior) [2, 3]. In addition, school attendance and participation in the school social environment and extracurricular activities are both essential and predictive of enhanced peer relationships and overall school success [4, 5]. If needs for participation are unmet, children may feel socially isolated from peers and the school community [1]. Over time, these conditions may operate in combination with the many other challenges associated with development and having a chronic disorder, thereby increasing risk for skills deficits, student disengagement, and ultimately school failure for the increasing proportion of children with such problems [6].
Chronic health conditions for which children require special health care services in childhood present challenges to school success by directly affecting a child’s potential learning capabilities, their engagement in the learning process, and their desire to learn [7]. Given that school success predicts so many future pathways for health and well-being across the life course [8], it is essential to identify and evaluate factors that promote or potentially impede its attainment for all children and children with special health care needs (CSHCN). School and healthcare professionals agree that health and education are dynamically intertwined for children [9–11]. However, the empirical evidence supporting a relationship between chronic conditions, special health care needs and factors promoting or impeding positive school outcomes is mixed. Asthma [12–15] and obesity [16, 17] do not appear to be associated with academic performance, whereas children with attention deficit hyperactivity disorder (ADHD) do more poorly on standardized testing and receive lower grades than those without ADHD [18, 19]. Children with emotional and behavioral issues are often most likely to have challenges succeeding in school [20].
CSHCN vary widely in the burden and complexity of their health care needs [21]. Complexity of need influences the amount and type of health care and educational support service requirements, which affects school experience and success in different ways. For example, those whose conditions are managed primarily with prescription medication differ from children whose conditions additionally require above routine use of other types of health and educational services, or who have more serious functional impairments [22]. CSHCN status and complexity of needs are likely to impact school success for children with chronic conditions, though there are few data describing these challenges in the population.
Case management for children with chronic conditions in the school setting has been shown to be effective in improving the quality of life for children with disabilities by increasing their readiness to learn, their classroom participation and their grades [23, 24]. Many states require case management for children with chronic conditions or disabilities in the educational setting. The specific requirements for state mandated case management for students with disabilities varies across states and by individual school districts but is generally expected to include elements to ensure that school health officials, parents, and primary care physicians are part of a team which prepares students to be ready to learn and achieve in the school setting [23, 25]. The impact of state policies to require case management on population-based prevalence of school success factors such as having to repeat a grade has not been evaluated.
The purpose of this manuscript is to present nationally representative statistics on factors promoting or potentially impeding school success and to examine the impact of a child’s special health care needs on these outcomes. First, we estimate the prevalence of school success factors nationally and across states for all children and CSHCN. Second, we examine at the individual child level whether CSHCN differ substantially from non-CSHCN on leading and lagging school success factors after adjustment for other factors and whether further variation is observed according to the presence of one or more emotional, behavioral or developmental problems and/or the complexity of service needs among CSHCN. Third, as a beginning for evaluating whether state school health-related policies are independently associated with a child’s probability of experiencing school success factors, we test the hypotheses that the probability of repeating a grade in school (1) varies across states after accounting for differences across states in children’s CSHCN and socioeconomic status and (2) is positively impacted if a state has a policy to provide school-based case management services for children with disabilities.
Methods
Data Source and Study Sample
The data used for this study were from the 2007 National Survey of Children’s Health (NSCH) [26, 27], which is described elsewhere in this special issue of the journal [28]. Analyses were restricted to children age 6–17 years old currently enrolled in school (home, public or private). Child level variables included: age (6–10, 11–14 and 15–17; categorized to align with grade level), gender, race/ethnicity (White–non-Hispanic, Hispanic with English primary household language, Hispanic with non-English primary household language, African American–non-Hispanic and multi/other race-non-Hispanic); household income based on federal poverty level (FPL) status (0–99 % FPL, 100–199 % FPL, 200–399 % FPL and 400 % or greater FPL); and the insurance type (public or private sector) and adequacy of child’s current insurance (insurance meets child’s needs, has reasonable out of pocket expenses, and allows child to see needed providers).
Children with Special Health Care Needs
Children with special health care needs were identified using the standardized CSHCN Screener [29]. Two measures of complexity were developed: (1) whether CSHCN whose service needs go beyond the need or use of prescription medication management and also involve above routine and/or specialized services [22] and (2) whether children currently experience one of seven emotional, behavioral or developmental (EBD) problems or conditions assessed in the NSCH (ADHD/ADD, depression, anxiety, conduct or behavioral problems, autism spectrum disorder, developmental delay, Tourette syndrome) [26, 27].
School Success Factors
Three dichotomous outcome variables assessed factors promoting school success: whether the child/youth is usually or always engaged in school behaviorally (does all required homework) and cognitively (cares about doing well in school); participates in sport, volunteer or other activities outside of school; and, usually or always feels safe at school. A summary measure of promoting factors was calculated (engaged, participates and feels safe).
Three factors that may potentially impede school success were evaluated as dichotomous outcome variables: missed more than 2 weeks (11 or more days) of school in the past year; has repeated any grade since beginning kindergarten; and has school problems which resulted in 3 or more school calls home due to problems in school in the past year. Cut-points for missing school (11+ days) and calls home (3+) represent 2–3 times the average number for all children and were selected to differentiate among CSHCN analytic subgroups and reflect research on the impact on test scores, grade repetition and other school outcomes [5, 30].
State-Level Variables
A state-level school-based case management policy variable was constructed from the 2006 School Health Policy and Program Study survey, respondents to which were state education agency personnel in all 50 states plus the District of Columbia [31]. The survey item used was: “Has your state adopted a policy stating that districts or schools will provide case management for students with disabilities when needed?” This survey item asked only about a state requirement for provision of case management services, but did not include state-level details of services required. Twenty-six states indicated the presence of such a policy in their state (DC, HI, ID, IL, IN, KY, MD, ME, MI, MN, MO, MS, NJ, NM, NV, NY, OH, OR, SD,TN, UT, VA, VT, WA, WV, WY). Two other state-level variables were constructed: (1) proportion of CSHCN in a state who have more (versus less) complex service needs (60.8 % all CSHCN; ranges from 52.1 to 76.6 % of CSHCN across states) and (2) proportion of CSHCN in a state who have more complex service needs and also have one or more emotional, behavioral or developmental problems (39.3 % all CSHCN; ranges from 28.8 to 48.6 % of CSHCN across states).
Analytic Methods
National and state-level prevalence rates for each promoting or potentially impeding factor were calculated for all children and sub-groups of children. Variations between non-CSHCN and CSHCN and subgroups across states were represented by calculating a disparity index constructed by dividing prevalence rates to obtain a rate ratio of less than or greater than 1 [32]. Logistic regression analysis was employed to assess associations between school success factors and the presence, complexity and type of special health care need a child has, using non-CSHCN without EBD as the reference category and controlling for child’s age, sex, race/ethnicity, household income, insurance type and insurance adequacy.
Two multi-level logistic regression models (MLM) were fit to evaluate the chances of grade repetition among CSHCN. MLM analyses were restricted to the grade repetition outcome variable due to limitations in both space and availability of valid and standardized state level policy variables for other outcomes. The two MLM models conducted assessed associations between repeating a grade in school and individual child and family characteristics (level 1), noted by the Adjusted Odds Ratio [AOR], estimated variations across states in these associations (level 1), noted by the Median Odds Ratio [MOR] statistic and evaluated whether states have a school policy requiring case management for children with disabilities, noted by state-level odds ratio [OR] (level 2). The first MLM additionally included as a level 2 variable the proportion of CSHCN with more complex needs and the second model included the proportion of CSHCN with more complex needs and EBD problems. Multilevel analyses used MLwiN version 2.22 [33–35]. All other analyses used SPSS’s Complex Sample Module V 18.0. All statistical analyses included an adjustment to standard errors to account for weighting, clustering, stratification, and increased variability that result from the NSCH’s complex sampling design.
Results
Characteristics of the Study Population
The demographic characteristics of the population (n = 63,843; weighted estimate 49.08 million) are given in Table 1. The age distribution of the 22.9 % of all school-age children with special health care needs does not differ substantially from non-CSHCN. However, CSHCN are significantly more likely to be male and publicly insured. Compared to all children, the 13.5 % of school age children with emotional, behavioral or developmental problems (EBD) are more likely to be older (15–17 years), male, publicly insured, and living below the federal poverty level. All CSHCN and especially CSHCN who also experience EBD are less likely to have adequate health insurance (Table 1).
Prevalence, State Variations and CSHCN Disparities in School Success Factors
Promoting Factors: Engagement, Participation, Feels Safe at School
Approximately 60 % of all school age children and half of all CSHCN (51.3 %) experienced all three factors promoting school success. For all children, prevalence of school engagement, participation in activities and feeling safe at school ranged from 49.3 to 73.8 % across states (including District of Columbia). Prevalence of CSHCN experiencing all of the promoting factors ranged from 39.4 to 64.7 % across states (Table 2). Children with EBD were less likely to experience all of the promoting factors (engaged, participates, feels safe), regardless of their CSHCN status (Table 3). The 40 % of CSHCN with more complex needs and EBD were least likely to do so (36.2 %; AOR 0.35). Compared to non-CSHCN without EBD and after adjustment for child characteristics, the lower prevalence of promoting factors remained statistically significant for all CSHCN subgroups, except for CSHCN with less complex needs and no EBD.
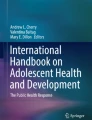
As shown in Table 2, a 1.22 fold difference between non-CSHCN and CSHCN was observed nationally in the prevalence experiencing all three promoting factors (62.8 vs. 51.3). Across states, this CSHCN status disparity ratio varied from a low of 0.98 (no difference) to a 1.67 fold difference. Within state differences between non-CSHCN and CSHCN were statistically significant for 38 states. Differentials in disparities across states were most pronounced when comparing the 74.2 % of all school age children who were non-CSHCN with no EBD to the 9.0 % of all school age children who are CSHCN with both more complex service needs and EBD. Figure 1 illustrates the variation across states in within-state disparities between these two groups (1.22–2.94 range in rate ratios). For all but three states, within state differences were statistically significant (p < 0.05). See the technical appendix for state by state prevalence, disparity ratios and results of statistical tests comparing the significance of differences between groups for each state.

Prevalence ratio between non-CSHCN without EBD and CSHCN with EBD/more complex service needs meeting all three promoting school success factor measures
Potentially Impeding Factors: Missed School, Grade Repetition, School Calls Due to Problems
As expected, CSHCN were more likely than non-CSHCN to miss more than 11 days of school (13.6 vs. 3.5 %), repeat a grade in school (18.3 vs. 8.2 %) and to have had repeated school calls home due to problems (27.1 vs. 7.7 %) (Table 2). More revealing are findings that CSHCN with more complex service needs were similarly likely to miss 2 or more weeks of school regardless of their EBD status and non-CSHCN with EBD problems were equally likely to miss school as CSHCN with EBD problems and less complex service needs (9.1 % each) (Table 3).
Regardless of their CSHCN status, children with EBD problems were more likely to have repeated a grade(s) and have three or more calls home due to school identified problems. However, CSHCN with EBD and more complex service needs were still much more likely to have repeated calls home due to problems (50 %). As shown in Table 3, comparisons between non-CSHCN without EBD problems and CSHCN subgroups remained statistically significant after adjustment for family and child characteristics for all but CSHCN with less complex needs and no EBD for the “calls home” and “grade repetition” measures.
Substantial variations across states were observed in the prevalence of factors potentially impeding school success for both CSHCN and non-CSHCN. These were greatest for grade repetition, where a 15.9-fold difference across states was observed for CSHCN and 12.7 fold difference for non-CSHCN (measured as the ratio between the highest and lowest prevalence). When comparing CSHCN to non-CSHCN, nationally, a 2.23 fold difference in prevalence was observed. Across states, the CSHCN versus non-CSHCN prevalence ratio varied from a 1.33-fold to a 3.91-fold difference for grade repetition and between group differences in prevalence were statistically significant for 37 states. The technical appendix includes state by state prevalence rates for CSHCN and non-CSHCN, disparity ratios and results of statistical tests comparing the significance of differences for each state.
CSHCN and State Policy Associations with Grade Repetition
Across state variation in the prevalence of CSHCN who experienced grade repetition (2.5–39.7 %) was statistically significant (p < 0.001; ICC = 0.070; MOR = 1.61). Variance was reduced by 38.9 % when child-level characteristics (age, sex, race/ethnicity, household income, EBD & CSHCN service need complexity and insurance type and adequacy) were accounted for. As presented in Fig. 2, CSHCN with more complex service needs and EBD problems had nearly 5 times greater adjusted odds (AOR: 4.96) of repeating a grade compared to CSHCN with less complex needs and no EBD. This effect also varied significantly across states (MOR: 1.30). CSHCN who lived in states with a school policy requiring case management for students with disabilities had significantly lower odds of repeating a grade (OR = 0.65; p = 0.001) compared to CSHCN who did not, even after controlling for child-level characteristics and either (a) the proportion of CSHCN in the state or (b) the proportion of CSHCN in the state with more complex needs and EBD problems. The ORs were the same for both sets of controls. Variance was reduced by 61 % when both child variables and the state-level policy variable were accounted for. See the technical appendix for results of multilevel regression analyses.

CSHCN grade repetition: associations across CSHCN subgroups and effect of state school policy requiring case management for children with disabilities
Discussion
With 40 % of all children and half of CSHCN failing to experience the low threshold measure of factors promoting school success (engaged, participates, feels safe), we conclude that threats to school success for US children, and especially CSHCN, are pervasive. Particularly at risk are the 9 % of all children who are CSHCN with both more complex service needs and EBD. We find that CSHCN and EBD are inextricably intertwined with respect to factors promoting or potentially impeding school success. Some children with EBD problems are expected to not qualify as having a special health care need, for reasons of the nature, frequency, severity or persistence of symptoms that may fall below a diagnostic or indicated treatment threshold. Nonetheless, non-CSHCN with EBD are a critical, albeit small (2.9 %) group of children requiring early identification and inclusion in efforts to facilitate promoting factors and attenuate impeding factors to school success.
In addition to EBD problems, variations in school success factors are likely to exist for other specific health condition(s) children have. Yet, it is critical to note that few CSHCN have only one type of health condition (e.g. 83.1 % of CSHCN with EBD have other conditions assessed in the NSCH) and there is substantial variation in need and functioning even among children with similar condition profiles. Also, while varying in intensity and manifestation, the nature of many of the underlying risks to school success CSHCN face are likely to be common. These observations support broad-based, non-condition specific efforts by states.
Findings suggest a protective effect of state-level school policies requiring case management for children with disabilities and support enhanced collaboration between healthcare and education in promoting school success among CSHCN. While it was beyond the scope of this study to evaluate the effect of state policies on each school success factor, findings from grade repetition analyses as well as those demonstrating across state variations in within-state disparities between CSHCN and non-CSHCN encourage further research to do so.
School success factor variables available in the NSCH are indicative of school success protective and risk factors. However, they do not directly measure test scores or longer-term school outcomes. In addition, some are more crude than ideal. For instance, the longer-term impact of grade repetition likely varies by a child’s grade in school. Yet, such information was not available for inclusion in analyses.
Findings suggest numerous hypotheses for future research and confirm the value of the NSCH as a critical data source for understanding the interrelated effects of children’s health and school success and priorities for state policy and programs.
Abbreviations
- NSCH:
-
National Survey of Children’s Health
- CSHCN:
-
Children with special health care needs
- EBD:
-
Emotional, behavioral or developmental problem
- AOR:
-
Adjusted odds ratio
References
National Research Council, Institute of Medicine (2004). Engaging schools: Fostering High School students’ motivation to learn. Committee on increasing high school students’ engagement and motivation to learn. Board on children, youth, and families, division of behavioral and social sciences and education. Washington, DC: The National Academies Press.
Connell, J. P., Wellborn, J. G., Gunnar, M. R., Sroufe, A. (1991). Competence, autonomy, and relatedness: A motivational analysis of self-system processes. In M. R. Gunnar & A. Sroufe (Eds.), Self-processes and development: Minnesota symposium on child psychology (pp. 43–77). Hillsdale, NJ: Erlbaum.
Finn, J. D. (1989). Withdrawing from school. Review of Educational Research, 59, 117–142.
Howie, L. D., Lukacs, S. L., Pastor, P. N., Reuben, C. A., & Mendola, P. (2010). Participation in activities outside of school hours in relation to problem behavior and social skills in middle childhood. The Journal of School Health, 80(3), 119–125.
Schatz, J. (2004). Academic attainment in children with sickle cell disease. Journal of Pediatric Psychology, 29(8), 627–633.
Power, T. J., & Phelps, L. (2006). Collaborative practices for managing children’s chronic health needs. Chronic health-related disorders in children: Collaborative medical and psychoeducational interventions (pp. 7–26). Washington, DC: American Psychological Association.
Currie, J., & Madrian, B. (1999). Health, health insurance and the labor market. In O. Ashenfelter & D. Card (Eds.), Handbook of labor economics (Vol. 3, pp. 3309–3407). Amsterdam: North Holland.
Fiscella, K., & Kitzman, H. (2009). Disparities in academic achievement and health: The intersection of child education and health policy. Pediatrics, 123(3), 1073–1080.
Dunkle, M., & Nash, M. A. (1991). Beyond the health room. Washington, DC: Council of Chief State School Officers, Resource Center on Educational Equity.
Novello, A. C., Degraw, C., & Kleinman, D. V. (1992). Healthy children ready to learn: An essential collaboration between health and education. Public Health Report, 107(1), 3–15.
Berkeley, CA: U. C. Berkeley College of Natural Resources. http://cwh.berkeley.edu/sites/greeneventsguide.org.cwh/files/primary_pdfs/CewaerPaper_Research.pdf.
Forrest, C. B., Starfield, B., Riley, A. W., & Kang, M. (1997). The impact of asthma on the health status of adolescents. Pediatrics, 99(2), E1.
Moonie, S., Sterling, D. A., Figgs, L. W., & Castro, M. (2008). The relationship between school absence, academic performance, and asthma status. The Journal of School Health, 78(3), 140–148.
Silverstein, M. D., Mair, J. E., Katusic, S. K., Wollan, P. C., O’Connell, E. J., & Yunginger, J. W. (2001). School attendance and school performance: A population-based study of children with asthma. Journal of Pediatrics, 139(2), 278–283.
Taras, H., & Potts-Datema, W. (2005). Childhood asthma and student performance at school. The Journal of School Health, 75(8), 296–312.
Cottrell, L. A., Northrup, K., & Wittberg, R. (2007). The extended relationship between child cardiovascular risks and academic performance measures. Obesity, 15(12), 3170–3177.
Huang, T. T.-K., Goran, M. I., & Spruijt-Metz, D. (2006). Associations of adiposity with measured and self-reported academic performance in early adolescence. Obesity (Silver Spring), 14(10), 1839–1845.
Loe, I. M., & Feldman, H. M. (2007). Academic and educational outcomes of children with ADHD. Journal of Pediatric Psychology, 32(6), 643–654.
Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Weaver, A. L., & Jacobsen, S. J. (2007). Long-term school outcomes for children with attention-deficit/hyperactivity disorder: A population-based perspective. Journal of Developmental and Behavioral Pediatrics, 28(4), 265–273.
Reid, R., Gonzalez, J. E., Trout, A., & Epstein, M. H. (2004). A meta-analysis of the academic status of students with emotional/behavioral disturbance. The Journal of Special Education, 38, 130–143.
McPherson, M., Arango, P., Fox, H., et al. (1998). A new definition of children with special health care needs. Pediatrics, 102(1 Pt 1), 137–140.
Bramlett, M. D., Read, D., Bethell, C., & Blumberg, S. J. (2009). Differentiating subgroups of children with special health care needs by health status and complexity of health care needs. Maternal and Child Health Journal, 13(2), 151–163.
Engelke, M. K., Guttu, M., Warren, M. B., & Swanson, M. (2008). School nurse case management for children with chronic illness: Health, academic and quality of life outcomes. Journal of School Nursing, 24(4), 205–214.
Erickson, C. D., Splett, P. L., Mullett, S. S., & Heiman, M. B. (2006). The health learner model for student chronic condition management–Part 1. Journal of School Nursing, 22(6), 310–318.
Asthma and Allergy Foundation of America. (2011). Annual report of state asthma and allergy policies for schools: 2010 update to the state honor roll (Washington state example). http://www.aafa.org/display.cfm?id=5&sub=105&cont=649. Accessed April 10, 2011.
Blumberg, S., Foster, E., Frasier, A., et al. (2009). Design and operation of the National Survey of Children’s Health, 2007. Washington, DC: National Center for Health Statistics.
National Survey of Children’s Health. (2007). Maternal and Child Health Bureau in collaboration with the National Center for Health Statistics. 2007 NSCH Indicator SPSS Data Set prepared by the Data Resource Center for Child and Adolescent Health, Child and Adolescent Health Measurement Initiative. http://www.childhealthdata.org.
Kogan, M. D., Ghandour, R. M., Schempf, A. H. (2012). Introduction to the Special Issue of Articles from the 2007 National Survey of Children’s Health. Maternal and Child Health Journal Supplement. doi:10.1007/s10995-012-1007-x.
Bethell, C. D., Read, D., Stein, R. E., Blumberg, S. J., Wells, N., & Newacheck, P. W. (2002). Identifying children with special health care needs: Development and evaluation of a short screening instrument. Ambulatory Pediatrics, 2(1), 38–48.
Center for Policy Studies, Education Research, and Community Development (CPSER). (2011). Research brief: Criteria for grade to grade promotion and/or retention. Obtained at: http://icee.isu.edu/Publications-All/PS&ERPublications/Gradetogradepromandreten.pdf. Accessed June 26, 2011.
Brener, N. D., Wheeler, L., Wolfe, L. C., Vernon-Smiley, M., & Caldart-Olson, L. (2007). Health services: Results from the School Health Policies and Programs Study 2006. The Journal of School Health, 77(8), 464–485.
Pearcy, J., & Keppel, K. (2002). A summary measure of health disparity. Public Health Reports, 117, 273–280.
Carle, A. C. (2009). Fitting multilevel models in complex survey data with design weights: Recommendations. BMC Medical Research Methodology, 9, 49.
Centre for Multilevel Modeling. (2009). A user’s guide to MLwiN version 2.10. Bristol: University of Bristol.
Merlo, J., Chaix, B., Ohlsson, H., et al. (2006). A brief conceptual tutorial of multilevel analysis in social epidemiology: Using measures of clustering in multilevel logistic regression to investigate contextual phenomena. Journal of Epidemiology Community Health, 60(4), 290–297.
Acknowledgments
This study was partly supported by the federal Maternal and Child Health Bureau under Cooperative Agreement 1-US9-MC06980-01.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bethell, C., Forrest, C.B., Stumbo, S. et al. Factors Promoting or Potentially Impeding School Success: Disparities and State Variations for Children with Special Health Care Needs. Matern Child Health J 16 (Suppl 1), 35–43 (2012). https://doi.org/10.1007/s10995-012-0993-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-012-0993-z