
Abstract
Cesarean delivery on maternal request (CDMR), a primary cesarean without medical indication for a singleton, term pregnancy, has been identified by physicians as one factor in the increasing rate of cesarean delivery despite nationwide efforts to the contrary. The purpose of this project was to better understand women’s preferences and motivations for their desired mode of delivery. A 62-item survey was administered to pregnant women asking for their delivery preference, their reasons, sources of information, feelings about this pregnancy, and opinions about delivery options. Responses were analyzed for candidates for CDMR or for repeat cesarean section, separately; the standard error of measure is ±4% (95% CI). 396 patients returned surveys (response rate = 63.2%). CDMR was desired by 34/316 (11%) candidates; repeat cesarean was desired by 32/70 (46%) patients. Significant correlates of CDMR included choosing during the first trimester (22% vs. 8.2%; RR = 2.72; P = 0.015), smoking during pregnancy (19.7% vs. 7.6%; RR = 2.60; P = 0.036), and being worried about the delivery (P = 0.004). Desire for CDMR increased as worries increased from unworried (4.4%) to somewhat (11.8%) to very worried (27.6%). Primary reasons included existing medical complications and preventing birth injury. The majority of patients believed CDMR should be an “informed choice”; other opinions varied by delivery preference. The majority of women preferred vaginal deliveries suggesting little contribution of CDMR to the increasing cesarean rate. Contrary to physicians’ beliefs, the women’s primary objective was their infants’ health rather than their own well-being.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
An important goal of our national public health promotion and disease prevention program, Healthy People 2010 (HP 2010), is the well being of mothers, infants, and children. One objective calls for the reduction of cesarean births to low risk women, specifically those with a term, singleton, vertex presentation pregnancy [1]. This objective is consistent with the International Federation of Gynecology and Obstetrics (FIGO) 1999 conclusion that “At present, because hard evidence of net benefit does not exist, performing cesarean section for nonmedical reasons is ethically not justified” [2].
Targeted improvements from baseline rates, established in 1998, include a 16.7% reduction in primary cesareans from 18 to 15% and a 12.5% reduction in repeat cesareans from 72 to 63%, by 2010. The midcourse year review indicates no progress towards reduction; data from the National Vital Statistics System, the Center for Disease Control, and the National Center for Health Statistics indicates increases of 133 and 167%, respectively [1].
Explanation for the increases includes the perception that women themselves are responsible, in part, due to requesting elective cesareans for non-medical reasons, otherwise known as “cesarean delivery on maternal request” (CDMR). CDMR was defined by the 2006 NIH State-of-the-Science Conference on CDMR as a term, cesarean delivery for a singleton pregnancy, requested by the mother, in absence of any medical indication [3].
Rates of CDMR
National estimates for CDMR range widely as there is no appropriate ICD-9 code for the elective, primary cesarean [4]. Estimates from inpatient surveys in the early 2000s indicate an increasing trend peaking at 28.3% [5]. Estimates from hospital discharge data through the mid 2000s, indicate a declining rate reaching 1.34% of all primary cesareans [6]. In 2005, only 0.4% of women who delivered by cesarean reported initiating CDMR, and 0.8% reported their physicians initiated CDMR [7]. The American Congress of Obstetricians and Gynecologists (ACOG) estimates the rate to be 2.5% of all births in 2007 [8]. Thus, no consensus exists as to prevalence.
The CDMR Controversy
It is not only the estimated rates of prevalence that vary greatly; there is considerable controversy in modern obstetrics concerning CDMR. In early 2006, the NIH-State-of-the-Science Conference on CDMR concluded there is insufficient evidence regarding the benefits and risks of CDMR. Therefore, decisions about CDMR need to be individualized, consistent with ethical principles, not before 39 weeks’ gestation, and not motivated by a lack of pain management [3]. Subsequently, ACOG’s committee opinion in December 2007 approved CDMR with several caveats. CDMR should only be performed at greater than 39 weeks gestation unless fetal lung maturity is documented. Additionally, CDMR should not be performed for women who desired several children as multiple cesarean sections increase risks of placenta accreta and previa. And CDMR should not be motivated by the unavailability of effective pain management [8].
Despite this shift in acceptance for CDMR among scientists and ACOG, the Healthy People 2020 plan proposes to retain the objective to reduce cesareans among low risk women [9]. The controversy has continued with considerable debate focusing on the ethics of CDMR as well as the varying perspectives of both providers and patients. The ethical issues hotly debated include: patient versus provider autonomy; beneficence versus nonmaleficence; and justice (e.g., [10–13]). The focus on providers’ perspectives includes obstetricians’ preferences, their understanding of patients’ preferences, and their willingness to perform CDMR [14–29]. Attention to the patients’ perspectives focuses primarily on self-reported delivery preferences and rationales [27, 30–38].
Ethical Considerations Regarding CDMR
Ethical arguments can be made both for and against CDMR. While consideration of the ethical principles involved is very complex, it is as easy to justify an argument against CDMR citing physician autonomy and the right to refuse to perform a procedure deemed unnecessary, as an argument for CDMR citing patient autonomy and the right to make an informed decision about an elective surgical procedure.
It is difficult to generate sound evidence-based arguments regarding risks and benefits since conclusive evidence on CDMR is not available [3, 31]. There are no agreed upon definitions of the costs and benefits for use in comparative analyses and adverse outcomes can be relatively rare, attributable to other risk factors, or not manifested for years. Consideration of the equitable distribution of medical resources begs the question of financial responsibility for CDMR, another complex issue. A cesarean delivery with prolonged hospital stay and increased risk to the mother and infant is potentially more expensive than an uncomplicated spontaneous labor and vaginal delivery; however, a failed trial of labor resulting in an emergency cesarean section is most risky and most expensive [12, 13]. Thus, CDMR remains highly controversial.
Opinions About CDMR
The data regarding desire for CDMR stems primarily from surveys with obstetricians abroad and in the US, and from patient surveys conducted primarily abroad. Obstetricians reported retrospectively on their patients’ preferences and their own experiences or projectively on hypothetical desires for themselves or their partners. Patients reported both retrospectively in the postpartum period and prospectively during their pregnancy.
Physicians’ Preferences and Rationales
Obstetricians surveyed about their delivery preferences for themselves or their partners suggest a minority of physicians would choose CDMR. Internationally, about 8% of men and 11–31% of women would opt for CDMR [14–17]. In the US, about 16% overall would prefer CDMR, but this varied by sex and sub-specialty within obstetrics [18]. Female obstetricians reported 22% of their deliveries by cesarean were elective [19]. Only 9.5% of US maternal-fetal medicine specialists (MFMs) surveyed would want CDMR; however, 45.5% of US urogynecologists would [20].
When surveyed as to the reasons for this delivery preference of the obstetrician-gynecologists, the majority cited fears of incontinence, perineal damage and sexual dysfunction [14–20]. Thus desire to prevent complications potentially attributable to vaginal delivery underlay their preferences for themselves or their partners.
Physicians’ Reports about Requests and Responses
The motivation to prevent harm also appeared in physician’s reported understanding about their patients’ delivery preferences and their own responses to requests for CDMR, both favorable and unfavorable. This understanding and willingness to provide CDMR also varied considerably by sex and subspecialty training, as well as by country of practice, age and hypothetical case scenario [16, 18–28].
Physicians reported patients’ requests for CDMR are motivated primarily by desire to prevent incontinence, prolapse, perineal damage, sexual dysfunction, fetal injury, and labor complications [18–23]. Other important considerations include maternal fear of childbirth, history of adverse birth experience, maternal age, plans for more children, fetal size, and maternal anxiety [19, 23–26]. Few cited pain avoidance as a motivation for request [22].
In response to these reported requests, approximately two-thirds of all ACOG obstetricians surveyed in 2003 reported they would perform CDMR [27]. Among subspecialists surveyed, 55% of MFMs and 83.4% of urogynecologists would perform CDMR [20]. In actuality, 53% of ACOG Fellows surveyed reported performing CDMR, but only 10.2% did so regularly [19].
The opponents of CDMR were asked why they would not be willing to perform CDMR. Physicians cited risk of complications for future deliveries, doubt that cesarean delivery confers any protection from pelvic floor disorders and concern for patients’ limited knowledge of risks and benefits including the overestimation of the safety of cesareans [20, 25, 28].
Thus the desire to prevent harm from the sequelae of both vaginal and cesarean deliveries contributed to physicians’ reported responses to patients’ requests for CDMR although decision-making processes lead to opposite conclusions for different obstetricians. That the perception of risks and benefits of CDMR relative to vaginal delivery and willingness to perform CDMR would vary greatly between physicians who specialize in antepartum care for high risk pregnancies and those who specialize in treatment for incontinence and pelvic floor injury is not surprising. Nor is it surprising that perception of risks and benefits is greatly varied among all obstetricians given that evidence is inconclusive [3, 4, 29]. Consequently, the ability to ethically and responsibly conduct an informed consent process is highly complex and open to physicians’ influence on patients’ choice [4, 30]. Add in scheduling convenience, differences in assessment of medical need, and outside influences such as family, friends, media sources, etc., the true desire for CDMR among pregnant women and any associated impact on the increasing cesarean delivery rate is difficult to ascertain validly [4, 19, 25, 30].
Patients’ Preferences and Rationales
Surveys of patients themselves have sought to ascertain their true desire for CDMR and the rationales for this preference; estimates, however, ranged widely. And likewise with physicians, patients’ delivery preferences and reasons vary depending upon a number of factors including: country, age, personality characteristics, perceived safety of cesarean delivery, fears or anxiety, history of trauma during previous delivery, history of previous cesarean delivery, and timing of assessment [26, 31–38].
In Brazil, the overall cesarean delivery rate is 50–60% and as high as 90% among the well educated. Women cited fear of labor pain and fear of damage to perineal and/or perivulvar musculature as their primary motivations [31].
Conversely, in European countries and Australia, only a minority of women surveyed (1–11.5%) indicated a preference for CDMR [32, 34, 36]. And their reported reasons for this preference focused primarily (54%) on a substantial concern for their infants’ safety and well being [32, 34–36]. The vast majority of women believed a right to choose should not supersede health considerations [36].
Additional concerns women cited included: fear or anxiety of a traumatic delivery and potential incontinence (34%), pain (26%), loss of control (18%) and some concern for limited support during labor. Women reported these fears were driven primarily by friends’ and families’ stories of bad birth experiences or a belief that cesarean was the safest route of delivery for their babies [32, 34–36].
Women preferring CDMR tended to be older, planning smaller families, more likely to have undergone IVF, less healthy and had greater levels of “monotony avoidance” characterized by a high level of sensation-seeking, need for change or action, a susceptibility to boredom, and low endurance [32–34]. Women with a history of previous cesarean delivery and those with previous negative birth experiences also tended to report greater desire to have a cesarean delivery. It is important to note, however, that the majority of women who have had previous bad birthing experiences or a previous cesarean section still preferred a vaginal delivery [29, 31].
It is also important to note that preference for CDMR was not static, but rather, varied over repeated assessment during a pregnancy. Desire for CDMR among women in Liverpool varied from 3.3% at first prenatal visit to 1% at 20–24 weeks and then 1.9% at 32–36 weeks. With the exception of one woman with a chronic medical condition, all women changed their minds at least once over the three assessments. And in concert with the majority of surveyed women opting for CDMR, safety for their babies was the overriding concern [36].
While considerable effort has been made internationally to ascertain women’s opinions directly, we found only one recent publication of a survey conducted in the US that detailed opinions from pregnant women without a history of cesarean delivery, receiving prenatal care in New York City in 2007. The majority of these women (88%) were minorities including primarily black and Hispanic women. The vast majority (93%) desired a vaginal delivery, and very few (5%) supported the idea of CMDR [38].
Summary
Obstetricians reported patients were motivated for CDMR primarily by concerns for their own health and fear avoidance. Most patients reported their primary consideration was the health and well being of their infants followed by their concerns about a potentially traumatic (psychological or physical) delivery experience. Given this discrepancy and how little data exists from women in the US, we thought it important to provide more women with the opportunity to participate in this healthcare debate.
Objective
The purpose of this project was to better understand women’s preferences and motivations for their desired mode of delivery.
Materials and Methods
We provided an Institutional Review Board-approved survey to all pregnant women receiving prenatal care at a residency clinic serving 16 counties of western North Carolina. English or Spanish research packets were put in charts of consecutive patients between July 2009 and April 2010, and charts were tagged to preclude repeated administration. Nurses provided the packets containing an information sheet, the paper–pencil survey and a self-addressed envelope to voluntary participants in exam rooms. Patients completed the surveys, sealed the envelopes and returned them to nurses or the check-out staff.
We created the 62-item survey using published results as a guide for important variables regarding delivery preference, rationales, sources of medical information, socio-demographics, pregnancy and delivery history, and familiarity with pelvic organ prolapse and incontinence. We included questions focused on the current pregnancy including intention to be pregnant at this time, positive feelings about the pregnancy, worries about the impending delivery, and intended family size.
We asked patients, “If you had the possibility to choose, how would you like to give birth?” and asked them to pick between “vaginal delivery” or “cesarean delivery”. Patients then selected their reasons from a list of statements cited by others as potentially important to decision-making (e.g., “Vaginal delivery is safer for me” or “Cesareans are safe for women in developed countries”); we provided space to write in additional reasons. Lastly, we included nine attitude questions with a 5-point Likert-like scale of agreement (strongly disagree to strongly agree) such as, “As long as women understand the risks and benefits of delivery methods, they should have the option to choose between a vaginal and cesarean delivery”.
Respondents were categorized as either a candidate for CDMR or eligible for a repeat cesarean section to delineate preferences and rationales among women without versus with the confounding experience of a previous cesarean section that affects preferences [29, 31]. The standard error of measure is ±4% (95% CI). We compared the cohorts using Chi square, Mann–Whitney or t test analyses; we utilized binary logistic regression to identify significant correlates of preference for CDMR. Multivariate analysis of variance was used to examine differences in opinions. All analyses were conducted using SPSS 18.
Results
Of the 627 women offered participation, 396 returned surveys (response rate = 63.2%). Nine were excluded for incompleteness or postpartum administration. Three hundred thirty-two (86%) were seen by a resident or faculty physician and 54 (14%) by a certified nurse midwife. Thirty (8%) surveys were in Spanish, compared to 357 (92%) in English.
Most respondents were candidates for CDMR [317 (82%)]. They were younger and more likely to have had previous vaginal deliveries than women eligible for repeat cesarean delivery (RCD); otherwise the two groups were very similar (see Table 1).
The majority of all women preferred a vaginal delivery for this pregnancy; candidates for CDMR were significantly less likely to opt for a cesarean delivery than women eligible for a repeat cesarean delivery (see Fig. 1). Among candidates for CDMR, the majority of both primigravidas [112 (88.2%)] and multigravidas [171 (90%)] preferred vaginal delivery (P = 0.369). Significant correlates of CDMR among candidates included choosing during the first trimester (22% vs. 8.2%; RR = 2.72; P = 0.015), smoking during pregnancy (19.7% vs. 7.6%; RR = 2.60; P = 0.036), and being somewhat to very worried about the delivery (P = 0.004). Desire for CDMR increased as worries increased from unworried (4.4%) to somewhat (11.8%) to very worried (27.6%).

Delivery route preference
Among women eligible for repeat cesarean delivery, those with an exclusive cesarean delivery history were much more likely to opt for a cesarean delivery than women with a history of both cesarean and vaginal deliveries [28 (57.1%) vs. 4 (19%); P = 0.006]. Other correlates included smoking during pregnancy (66.7% vs. 33.3%; RR = 2; P = 0.036) and seeing a doctor rather than a CNM (45.7% vs. 100%; P = 0.002).
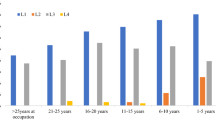
Women chose multiple statements they believed were important in the decision making about their delivery preference. The primary reasons for CDMR (see Fig. 2) included medical problems, possible need for cesarean, lack of confidence to deliver vaginally, desire for a bilateral tubal ligation (BTL), and preventing birth injury. The majority opting for RCD indicated a need for a repeat section; half indicated a desire for BTL. Primary reasons for choosing vaginal deliveries among candidates for CDMR (see Fig. 3) included thinking it is the natural method, being confident in their ability to deliver vaginally, desiring a faster recovery, being young and healthy, preventing surgery, and having a shorter hospital stay. Women eligible for RCD reported preferring the natural method and desiring to experience a natural birth or a vaginal birth after cesarean delivery (VBAC), preventing surgery and thus a faster recovery.

Reasons for CDMR or RCD

Reasons for vaginal delivery
Among candidates for CDMR who preferred a vaginal delivery, friends and family were the most frequent sources of information about their delivery choice (61 and 52%, respectively), with only 1 in 3 women citing their doctor as a source. Women preferring CDMR reported family, friends and doctors as important sources (41, 31 and 31%, respectively). Among women eligible for RCD, doctors were the primary source of information regardless of their preferred delivery option (vaginal delivery 56% and RCD 76%).
Mean opinion ratings did not vary significantly between candidates for CDMR versus RCD, nor was there an interaction of candidacy and delivery choice (P = 0.654 and P = 0.899, respectively). There were, however, significantly different opinions between women opting for cesarean versus vaginal delivery (P = 0.0001). The majority of patients believe that CDMR should be a matter of informed choice, but they also believe patients should follow their doctors’ advice regardless of personal preference. Women expressed attitudes consistent with their delivery preference (see Table 2).
Conclusions
The purpose of this paper was to include the self-reported attitudes and opinions of more American women in the health care debate on CDMR. Our data suggest that while the majority of women think CDMR should be an informed choice option, very few women prefer this option. The few candidates for CDMR preferring cesarean delivery worried about potential complications necessitating surgical delivery and ultimately, the safety of their babies. The majority of women, including those who might need a repeat cesarean delivery, desired a non-surgical, “natural,” vaginal delivery.
Our findings concur with reported desire among low income, minority New Yorkers as well as most European women [32–38]. Additionally, our findings seem consistent with the reported absence of scientific data evincing any substantial increase in the overall rate of cesarean delivery due to maternal request [4].
Our respondents’ focus on medical concerns and infant safety as the primary underlying rationales for delivery preference mirrored reasoning by many international women [19, 23–32, 35]. Thus, maternal request for cesarean delivery was a preemptive move to avoid uncertainty about the ultimate delivery route and the inherent risks to their babies. These findings contradict physicians’ perceptions that requests for CDMR were motivated primarily by women’s desires to protect their own health and well-being [18–20, 22, 23, 26].
The misperception of motivation for CDMR is particularly troublesome in light of our finding that women who chose cesarean delivery cited doctors more frequently as a source of information than women desiring vaginal deliveries and the previous findings that twice as many women undergoing CDMR reported it as their doctor’s choice rather than their own choice [7]. While possibly indicative of fetal and/or maternal conditions incompatible with vaginal birth, our findings could be the result of a less benign phenomenon: the insidious encroachment of business into medicine such that the provider prefers the convenience of a scheduled delivery. In this way, office schedules and other surgeries are not interrupted with the unpredictable timing of vaginal birth or vaginal birth gone awry requiring urgent cesarean. This is unlikely in our practice however, as we are a residency training program, and physician coverage is assigned in-house 24 h a day.
Another reason why doctors might recommend a particular delivery mode to patients may be a reflection of the provider’s personal preference for delivery. The influx of female providers in obstetrics may play a part here indeed. The majority of recent graduates of obstetrics and gynecology training programs surveyed reported they would be willing to perform CDMR for the indication of preventing pelvic floor disorders. However, they also indicated that they routinely recommend a trial of labor after cesarean delivery (TOLAC) over repeat cesarean (88%) [39].
The majority of specialists in Urogynecology and Maternal Fetal Medicine (the two specialties with the most expertise in the pelvic floor and obstetric outcomes, respectively) reported they would perform elective cesarean delivery [20]. While many obstetricians, and some Australian and Brazilian patients preferring CDMR shared these concerns regarding increased risks for pelvic organ prolapsed (POP) or incontinence, very few other samples of patients did [31, 35]. Most of our patients were not even familiar with these diagnoses, especially POP.
Our patients were more concerned about the potential benefit of a bilateral tubal ligation during cesarean delivery than preventing damage to the pelvic floor. Although immediate postpartum mini laparotomy or delayed postpartum laparoscopic surgical sterilization may not be as convenient as tubal ligation during cesarean delivery, the operative risks are substantially less than those of major abdominal surgery. It is difficult to hypothesize any circumstances that might justify desire for tubal ligation as a rational for CDMR.
It is also difficult to justify emotional distress, fear or excessive worry, as the superseding motivation for surgical delivery. Nevertheless, fears and worries for the safety of one’s baby coupled with a lack of confidence to deliver vaginally are substantial considerations shared internationally [19, 23–32, 35]. While the incidence of birth trauma is low, there is little clear cut evidence on risks and benefits of delivery type to assuage concerns for those who are very worried [4, 40]. Counseling and open access to supportive guidance during vaginal delivery (e.g., Doulas, midwifery care) may be better, albeit less convenient options than cesarean delivery.
Whatever the underlying rationale or motivation, the majority of women in this and other similar studies, both domestic and foreign, would choose a vaginal delivery if offered the option. Although the rate of cesarean is on the rise nationally (24% in 1994) and is even higher in some other countries, it seems that the majority of patients would not willingly choose this option even if they believe CDMR should be a matter of informed choice.
Further, a small majority of women who previously delivered via cesarean also desired a vaginal delivery, primarily to experience the “natural method” of birth. With the NIH’s new consensus statement reflected in ACOG’s new guidelines for a trial of labor after cesarean (TOLAC), more women may be able to fulfill these desires [41]. While our study sought to give a voice to women of western North Carolina in the national debate on CDMR, it may be that this particular “great debate” is largely an academic one.
It is important to note that our findings are limited to voluntary participants, primarily white and low income, seeking care in a resident clinic in the southern Appalachians. Our response rate of 63.2% and the 6.3-grade reading level of the survey excluded the opinions of some of our patients especially immigrant women who may be illiterate or speak other languages. Additionally, some women attend their prenatal care visits with small children or other family member and may have been unable to complete the survey as administered. Furthermore, we did not gather data on race, thus we were unable to ascertain the influence of race, ethnicity, or socio-economic status on delivery preference or opinions about CDMR.
Nevertheless, our findings suggest that physicians and other obstetrical care providers must be cognizant of their own biases as well as their patients’ understanding of the risks and benefits of delivery options, their desires for the delivery, and their underlying rationales. Furthermore, providers need to understand that the decision making factors are multifaceted, confounded with worries, influenced by friends and families, and driven primarily by a desire to prevent harm to their babies.
ACOG recognizes CDMR may be an individualized, informed choice option for some women [8]. In counseling patients, the main objective should always be informed consent. It may be helpful to start off the conversation about patients’ birth plans by asking them which delivery mode they would prefer. After carefully reviewing the medical history and risk factors, the provider could then engage the patient in a discussion about the ramifications of this choice. For example, in our particular population, knowing that fear is a factor for some who would choose cesarean, counseling could be directed at allaying fear and familiarizing the patient with the birth process and what to expect in labor. If conversely, cesarean is the indicated delivery route for a patient who would prefer a vaginal delivery, then reviewing the reason for that recommendation and educating the patient about cesarean birth may make her more comfortable with that option.
The optimal birth experience is defined differently for each patient and provider. An open and ongoing discussion about birth expectations and desired route of delivery is an important piece of optimizing birth. Ultimately, patients and providers share the same goal: healthy mothers with healthy babies.
References
US Department of Health and Human Services HP. (2010). Midcourse review. Available at http://www.healthypeople.gov/data/midcourse/default.htm. Accessed January 26, 2010.
International Federation of Gynecology and Obstetrics (FIGO). (1999). Ethical guidelines on human reproduction and women’s health. International Journal of Gynecology and Obstetrics, 64, 317–322.
NIH State-of-the Science Conference Statement on Cesarean Delivery on Maternal Request (2006). NIH Conses Sci Statements. March 27–29, 23, 1–29.
Coleman, V. H., Lawrence, H., & Schulkin, J. (2009). Rising cesarean delivery rates: The impact of cesarean delivery on maternal request. Obstetrical and Gynecological Survey, 64(2), 115–119.
Meikle, S. F., Steiner, C. A., Zhang, J., & Lawrence, W. L. (2005). A national estimate of the elective primary cesarean delivery rate. American Journal of Obstetrics and Gynecology, 105, 751–756.
Gossman, G. L., Joesch, J. M., & Tanfer, K. (2006). Trends in maternal request cesarean delivery from 1991 to 2004. Obstetrics and Gynecology, 108(6), 1506–1516.
Childbirth Connection. Mothers report cesarean views and experiences: New national Listening to Mothers survey results. Available at http://www.childbirthconnection.org/article.asp?ck=10372. Accessed December 29, 2009.
Cesarean Delivery on Maternal Request. (2007). ACOG Committee Opinion No. 394. American Congress of Obstetricians and Gynecologists. Obstetrics & Gynecology, 110, 1501–1504.
US Department of Health and Human Services. Healthy People 2020 Proposed Objectives. Available at http://www.healthypeople.gov/hp2020/Objectives/TopicAreas.aspx Accessed January 26, 2010.
Minkoff, H., Powderly, K. R., Chervenak, F., & McCullough, L. B. (2004). Ethical dimensions of elective primary cesarean delivery. Obstetrics and Gynecology, 103, 387–392.
Kalish, R. B., McCullough, L. B., & Chervenak, F. A. (2008). Patient choice cesarean delivery: Ethical issues. Current Opinion in Obstetrics and Gynecology, 20, 116–119.
Bost, B. W. (2003). Cesarean delivery on demand: What will it cost? American Journal of Obstetrics and Gynecology, 188, 1418–1423.
Grady, D. (2008). After Cesareans, Some See Higher Insurance Cost. New York Times, June 1, 2008. Available at http://www.nytimes.com. Accessed January 26, 2010.
Al-Mufti, R., McCarthy, A., & Fisk, N. M. (1997). Survey of obstetricians’ personal preference and discretionary practice. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 73, 1–4.
Land, R., Parry, A., Rane, A., & Wilson, D. (2001). Personal preference of obstetricians towards child birth. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 41, 249–252.
Gonen, R., Tamir, A., & Degani, S. (2002). Obstetricians’ opinions regarding patient choice in cesarean delivery. Obstetrics and Gynecology, 99, 577–580.
Berholt, T., Ostberg, B., Legarth, J., & Weber, T. (2004). Danish obstetricians’ personal preference and general attitude to elective cesarean section on maternal request: A nation-wide survey. Acta Obstetricia et Gynecologica Scandinavica, 83, 262–266.
American Congress of Obstetricians and Gynecologists. ACOG News Release: New ACOG opinion addresses elective cesarean controversy. October 31, 2003. Available at www.acog/org/from_home?publications/press_releases/nr10-31-03-1.cfm. Accessed January 26, 2010.
Bettes, B. A., Coleman, V. H., Zinberg, S., Spong, C. Y., Portnoy, B., DeVoto, E., et al. (2007). Cesarean delivery on maternal request: Obstetrician-gynecologists’ knowledge, perception, and practice patterns. Obstetrics and Gynecology, 109(1), 57–66.
Wu, J. M., Hundley, A. F., & Visco, A. G. (2005). Elective primary cesarean delivery: Attitudes of urogynecologists and maternal-fetal medicine specialists. American Journal of Obstetrics and Gynecology, 105(2), 301–306.
Cotzias, C. S., Paterson-Brown, S., & Fisk, N. M. (2001). Obstetricans say yes to maternal request for elective caesarean section: A survey of current opinion. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 97, 15–16.
Ghetti, C., Chan, B. K. S., & Guise, J. M. (2004). Physicians’ responses to patient-requested cesarean delivery. Birth, 31, 280–284.
Wax, J. R., CArtin, A., Pinette, M. G., & Blackstone, J. (2005). Patient choice cesarean-the Maine experience. Birth, 32(3), 203–206.
Liu, T. C., Lin, H. C., Chen, C. S., & Lee, H. C. (2008). Obstetrician gender and the likelihood of performing a maternal request for a cesarean delivery. European Journal of Obstetrics, Gynecology, 136, 46–52.
Karlstrom, A., Engstrom-Olofsson, R., Nystedt, A., Thomas, J., & Hildingsson, I. (2009). Swedish caregivers’ attitudes towards caesarean section on maternal request. Women and Birth, 22, 57–63.
Mancuso, A., DeVivo, A., Fanara, G., Albiero, A., Priolo, A. M., Giacobbe, A., et al. (2008). Cesarean section on request: Are there loc-regional factors influencing maternal choice? An Italian experience. Journal of Obstetrics and Gynaecology, 28(4), 382–385.
American Congress of Obstetricians and Gynecologists. ACOG News Release: Gallup survey reveals women ob-gyns benefit from “insider knowledge.” December 9, 2003. Available at www.acog/org/from_home?publications/press_releases/nr12-09-03-2.cfm. Accessed November 19, 2008.
Gamble, J., & Creedy, D. (2000). Women’s preference for a cesarean section: Incidence and associated factors. Birth, 28(2), 101–110.
Lavender, T., Hofmeyr, G. J., Neilson, J. P., Kingdon, C., Gyte, G. M. L. (2006). Caesarean section for non-medical reasons at term. Cochran Database of Systematic Reviews, 2006(3). Art No. CD004660. doi:10.1002/14651858.CD00460.pub2.
Gamble, J., Creedy, D. K., McCourt, C., Weaver, J., & Beake, S. (2007). A critique of the literature on women’s request for cesarean section. Birth, 34(4), 331–340.
Pinott, J. A., & Pinotti, M. (1994). The cesarean epidemic in South America. JSOGC, 6, 154–157.
Hildingsson, I., Radestad, I., Rubertsson, C., & Waldenstrom, U. (2002). Few women wish to be delivered by cesarean section. British Journal of Obstetrics and Gynaecology, 109, 618–623.
Wiklund, I., Edman, G., Larsson, C., & Andolf, E. (2006). Personalty and mode of delivery. Acta Obstetrics and Gynaecology, 85, 1225–1230.
Wiklund, I., Edman, G., & Andolf, E. (2007). Cesarean section on maternal request. Cesarean section on maternal request: Reasons for the request, self-estimated health, expectations, experience of birth and signs of depression among first-time mothers. Acta Obstetricia et Gynecologica Scandinavica, 86, 451–456.
Weaver, J. J., Statham, H., & Richards, M. (2007). Are there “unnecessary cesarean sections? Perceptions of women and obstetricians about cesarean sections for nonclinical indications. Birth, 34(1), 32–41.
Robson, S., Carey, A., Mishra, R., & Dear, K. (2008). Elective cesarean delivery at maternal request: A preliminary study of motivations influencing women’s decision-making. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 48, 415–420.
Kingdon, C., Neilson, J., Singleton, V., Gyte, G., Hart, A., Gabbay, M., et al. (2009). Choice and birth method: Mixed-method study of caesarean delivery for maternal request. BJOG, 116, 886–895.
Pevzner, L., Goffman, D., Comerford, M., & Dayal, A. K. (2008). Patients’ attitudes associated with cesarean delivery on maternal request in an urban population. American Journal of Obstetrics and Gynecology, 198(5), e35–e37.
Kenton, K., Brincat, C., Mutone, M., & Brubaker, L. (2005). Repeat cesarean section and primary elective cesarean section: Recently trained obstetrician-gynecologist practice patterns and opinions. American Journal of Obstetrics and Gynecology, 192, 1872–1876.
Russo, C. A., Andrews, R. M. Potentially avoidable injuries to mothers and newborns during childbirth, 2006. Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project Statistical Brief #74. May 2009. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb74.jsp Accessed November 15, 2010.
American College of Obstetricians and Gynecologists (ACOG). (2010). Vaginal birth after previous cesarean delivery. ACOG Practice Bulletin # 115. Obstetrics and Gynecology, 116(2), 450–463.
Acknowledgments
The authors would like to thank Dr. Robert Henderson for his contributions to the formulation of the research objective and the survey content.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Romero, S.T., Coulson, C.C. & Galvin, S.L. Cesarean Delivery on Maternal Request: A Western North Carolina Perspective. Matern Child Health J 16, 725–734 (2012). https://doi.org/10.1007/s10995-011-0769-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-011-0769-x