
Abstract
The purpose of this study is to explore state-level fetal death rates and <24 h infant mortality rates for deliveries less than 500 g in order to estimate outcomes classification differences at the edge of viability. We selected singleton deliveries to US resident mothers born <500 g and >20 weeks gestation from the NCHS live birth-infant death and fetal death files for 1999–2002 (n = 37,813). Infant deaths within 24 h of birth were selected to estimate odds of classification as a fetal death versus a live birth/infant death by state. Logistic regression was used to derive odds of classification as a fetal death and to adjust for maternal characteristics, calculating unadjusted and adjusted odds ratios. We identified 37,813 outcomes from 48 states reporting in this birthweight category. Unadjusted odds of classification of outcomes as a fetal death versus a live birth/death within 24 h by state ranged from OR = 0.38 (95% CI = 0.24–0.59) to OR = 2.93 (95% CI = 2.26–3.78); adjusted for maternal age and race, the range narrowed slightly to a OR = 0.31 (95% CI = 0.20–0.48) to aOR = 2.54 (95% CI = 1.96–3.30). Six states were more likely to classify outcomes as a live birth/infant death, while 14 states were more likely to classify as a fetal death, when compared to a large reference state. The remaining states did not differ significantly in their outcomes. The fraction of outcomes classified as fetal deaths varied by state during the years studied. This study suggests fetal death and early infant death outcomes reported for babies less than 500 g reflect differential classification thus influencing the validity of these vital statistics data at the state level. Further studies are needed to explore the factors that influence these differences.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The perinatal mortality rate is a key indicator of the health of a community and the quality of the health care system. Declining infant mortality rates observed in the US during the past four decades reflect improvement in birth weight-specific mortality and have been attributed to improvement in perinatal health care practices, [1], yet inequities by race/ethnicity remain [2]. The United States infant mortality rate ranks poorly in comparison to those of other industrialized countries [3]. Consistently higher rates of infant mortality in the US have been attributed to the higher prevalence of maternal health risks, as well as inequities in access to health care [3, 4]. The state variation in infant mortality rates remains largely unexplained. [5].
Fetal deaths in the US account for nearly half of all deaths occurring from the 20th week of pregnancy through the end of the first year of life [6–8]. Although the US fetal mortality rate has also declined in recent years, improvements lag those observed for infant deaths. Since 1985, the US fetal mortality rate has declined 18%, from 7.8 per 1,000 live births plus fetal deaths to 6.4 in 2002 [9] compared with a 34% decline from 1985 to 2002 for infant deaths [10]. Improvement in overall fetal mortality has resulted primarily from declining late fetal mortality rates (fetal deaths 28 weeks gestation or greater); early fetal mortality rates (fetal deaths <28 weeks gestation) have not changed [11].
Evidence from prior investigations suggests that the classification of fetal death versus infant death for extremely low birth weight deliveries in both the US and Canada has changed over recent years [12–14]. These studies suggest the number of live births of very short gestations has increased due to shifts in the classification of a fetal death versus an infant death, and that this phenomenon may explain at least in part the recent lack of improvement in birth weight-specific mortality rates at the lowest birth weights.
The purpose of this study was to explore state-level variations in the classification of perinatal death by studying fetal and infant mortality rates for deliveries less than 500 g. Our goal was to provide evidence to support the hypothesis that differential classification of live birth or fetal death occurs at the state level and is reflected in the fetal and infant mortality rates for this birthweight group.
Methods
We used the National Center for Health Statistics (NCHS) live birth-infant death cohort and fetal death files from 1999 to 2002. We selected for singleton fetal deaths and live births (hereinafter referred to as deliveries) to US resident mothers, as multiple births present a unique set of issues related to birth weight and gestational age. We also selected for deliveries less than 500 g and >=20 weeks gestation for the 48 states (including the District of Columbia) that report this classification of fetal deaths (n = 37,813). This birth weight and gestational age range enabled us to examine those live births, infant deaths, and fetal deaths that occurred at the limits of viability. Three states (New Mexico, South Dakota and Tennessee) that did not report fetal deaths less than 500 g were excluded from portions of the analysis. All data were analyzed using state of residence at delivery.
Gestational age and birth weight were obtained from the birth certificate or fetal death record; time to death was obtained from the death certificate. Gestational age in completed weeks was computed from the interval between the first day of the last normal menstrual period (LMP) and the date of birth. Records with missing date of LMP were imputed by NCHS when there was a valid month and year. Clinical estimate of gestation was used in the imputation of gestational age in cases when no valid month and year of LMP was reported. Records with implausible or missing values for birth weight or gestational age and records with a birth weight value inconsistent with the gestational age were deleted. Procedures for imputing data and determining gestational age-birth weight inconsistency have been described in detail elsewhere [15].
The fetal mortality rate was defined as fetal deaths per 1,000 deliveries; less than 24 h (<24 h) rate was those deaths occurring within 24 h of birth per 1,000 live births. We defined the combined perinatal mortality rate as all fetal deaths plus <24 h infant deaths per 1,000 deliveries. The US has adopted the WHO definitions of live birth and fetal death as shown in Table 1a. This definition of live birth does not define a minimal gestational age or birth weight. However, states have varying definitions of fetal death and most define minimum gestational age and/or birth weight requirements, as shown in Table 1b [7].
To estimate the variation in outcomes classification by state we restricted our population to include all fetal deaths and all <24 h deaths since these very early infant deaths were most likely to be misclassified. We determined the ratio of <24 h infant deaths to fetal deaths for each state and used logistic regression to determine odds ratios for the risk of fetal death compared to live births resulting in death <24 h. Finally, the odds ratios were adjusted for maternal race and age. All states were included in the model, using North Carolina as the reference group. North Carolina was chosen as the reference group because it had an infant to fetal death ratio of approximately one and a large birth population. Analyses were conducted using SAS v9.1 and SPSS v17.0.
Results
We identified 37,813 singleton deliveries of greater than 20 weeks gestational age and with a birth weight of less than 500 g. Over 50% (51.9%) of these deliveries were fetal deaths. Among the infant deaths, 89.7% occurred during the first 24 h of birth, 97.7% occurred during the neonatal period and 94.7% during the first 7 days of life (Table 2).
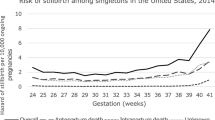
Table 3 provides the state-specific fetal, <24 h, and combined perinatal mortality rates. States with lower fetal mortality rates generally had higher <24 h and neonatal mortality rates. Figure 1 displays box plots of mortality rates per 1,000 deliveries at least 20 weeks gestational age and <500 g for each of the 48 states reporting fetal deaths in this range. The mean perinatal mortality rate (fetal + all infant deaths) was 917 per 1,000 deliveries [SD = 56] and the rate ranged from a low of 706 to a high of 1,000; the combined fetal plus <24 h mortality rate had a mean of 715 [SD = 57] and had a low of 523 and a high of 819. The mean infant mortality rate across all states was 415 per 1,000 live births [SD = 92] and ranged from a low of 176 to a high of 661; the mean <24 h mortality rate was 213 [SD = 70] and ranged from 58.8 to 427.4; and the mean fetal mortality rate was 501 [SD = 94] and ranged from 245.8 to 666.7.

State death rate by classification period. Death rates per 1,000 fetal deaths + live births under 500 g by state for the 48 states reporting fetal deaths in this birthweight category. States outside of the 1.5 inter-quartile range are identified as outliers (filled circle)
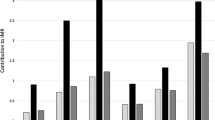
For subsequent analyses, we restricted our population to the 33,164 fetal and <24 h infant deaths for the regression. The ratio of fetal deaths to <24 h deaths varied by state from a low of 0.59 to a high of 9.0 (Table 3). The unadjusted logistic regression (data not shown) demonstrated similar variation in the odds ratios for classification of a fetal death by state, ranging from 0.38 (95% CI = 0.24–0.59) to 3.26 (95% CI = 1.21–8.84) compared to the reference state of North Carolina. Adjustments for maternal race and age did not substantially change the relative comparisons across the states (Fig. 2). Overall, 14 states had an odds ratio greater than 1 with a level of significance less than 0.05. Only six states (Rhode Island, Delaware, Kansas, Maine, Connecticut, and Maryland) had odds ratios less than 1 indicating that when adjusted for maternal age and race, these states had a lower risk of having deliveries classified as fetal deaths compared to <24 h deaths. For example, as shown in Fig. 2, deliveries in Rhode Island had an adjusted odds ratio of 0.31 (95% CI = 0.20–0.48), meaning that Rhode Island deliveries had a 69% decreased risk of being classified as fetal deaths compared to <24 h deaths.

Adjusted odds ratio, with 95% confidence intervals, of fetal deaths among the cohort of fetal plus <24 h infant deaths for each state with North Carolina as the reference group
Discussion
We used 4 years of national vital statistics data to explore the hypothesis that states across the US differ in their classification of fetal and infant death for deliveries less than 500 grams. Because fetal deaths and live births are most likely to be misclassified, we restricted our study to these two group in order to determine the classification pattern for the US overall and the 48 individual states reporting outcomes in <500 g category. This analysis revealed a broad variation in the classification patterns across states and we identified six states (Rhode Island, Delaware, Kansas, Maine, Connecticut, and Maryland) where the odds favored the report of a delivery as a live birth/infant death rather than a fetal death. However, most states were as or more likely to report these deliveries as fetal deaths.
Differential state-level classification of fetal versus infant death is more likely the result of differences in the application of the definition of live birth rather than differences in the underlying biology of the fetuses. Differences in state reporting requirements may account for some variation in outcomes reporting between states; however, we minimized this potential effect by restricting our analysis to deliveries with a gestational age of at least 20 weeks, considering only deliveries classified as live births who died within 24 h, and excluding the states that do not report fetal deaths under 500 g. Additionally, legal standards for vital registration of a fetal death differ among those states whose ratios appear to be outliers (Table 1b), arguing against varying legal standards as the main explanation for this phenomenon. We note that the states at either end of the spectrum tend to be states with smaller populations. Therefore, variation in state-level classification may reflect hospital-specific vital records reporting practices. A few number of hospitals in a state is more likely to affect the state-level patterns of reporting.
Variation in classification as a fetal death versus a live birth/infant death can distort birth weight-specific mortality rates for very low birth weight babies. As suggested in an examination of Alabama data from the 1990s, temporal trends favoring classification of outcomes as live births may obscure improvements in birthweight specific mortality rates by including a greater number of non-viable infants [14]. Although the absolute number of live births under 500 g is small, these events contribute significantly to the total number of infant and fetal deaths and to the overall infant mortality rate. Therefore, the pattern of classification as a fetal death versus live birth/infant death potentially could have a significant impact on overall infant mortality and fetal death rates. For example, a small upward trend in infant mortality rates reported in Canada has been attributed to increased numbers of infants less than 500 g classified as live births [12]. Changing classification patterns were also suggested as an underlying factor in the apparent increase in the infant mortality rate in the U.S. from 2001 to 2002 [16].
This study was subject to several limitations. The quality of reporting on the population-based vital records, including accuracy and completeness of reporting of fetal deaths, may account for some differences between states. Previous work has noted the problems associated with these secondary data, including missing data, out-of-range data (biologically implausible), and inconsistencies between birth weight and gestational age [17, 18].
Some heterogeneity may have resulted from analysis of data by state of residence rather than state occurrence as registration of vital events follow reporting regulations of the state of occurrence rather than the state of residence to which the death is attributed. States with significant numbers of very low birth weight deliveries to mothers living across state lines may have their outcomes influenced by reporting standards of neighboring states. We do not believe the variability resulting from these patterns account for the overall patterns observed in our analysis because they would be expected to dilute the observed effects.
Given the nature of the available data, the causes of the differences observed across states could not be fully explored in this study. Six states in our analysis favored classification as an infant death rather than a fetal death. One potential explanation is that institutions in these states more strictly follow the WHO definition of a live birth. Rhode Island, for example, is obligated by state law to follow a strict legal definition of a live birth and this requirement is consistent with our findings of low odds of fetal death in that state. A number of these states are small and have fewer obstetrical facilities, with a large proportion of deliveries occurring in tertiary hospitals; therefore variations in community practice patterns are not averaged across multiple institutions. Other states were more likely to classify these deliveries as fetal deaths. Local or regional practices may be influenced by attitudes toward pregnancy termination, neonatal resuscitation, resources, and parental or provider expectations of survival of very low birth weight infants. These decisions may also be related to factors such as social, economic, and religious views.
The findings from this study have important health policy implications and suggest caution when comparing individual state fetal and infant mortality rates. Comparisons may not be appropriate, especially across states with differing patterns of vital event reporting. Instead, comparing perinatal mortality rates may be more meaningful, as demonstrated by our finding of less variability in this measure across states. Future research should explore hospital-specific reporting patterns, both over time and across the range of birth weight and gestational age, to better understand the implications of these findings.
References
Lee, K. S., Khoshnood, B., Hsieh, H., Kim, B. I., Schreiber, M. D., & Mittendorf, R. (1995). Which birthweight groups contributed most to the overall reduction in the neonatal mortality rate in the United States from 1960 to 1986? Paediatric and Perinatal Epidemiology, 9(4), 420–430.
Martin, J. A., Kochanek, K. D., Strobino, D. M., Guyer, B., & MacDorman, M. F. (2005). Annual summary of vital statistics—2003. Pediatrics, 115(3), 619–634.
Hamilton, B. E., Minino, A. M., Martin, J. A., Kochanek, K. D., Strobino, D. M., & Guyer, B. (2007). Annual summary of vital statistics: 2005. Pediatrics, 119(2), 345–360.
Joseph, K. S., Kramer, M. S., Allen, A. C., Cyr, M., Fair, M., Ohlsson, A., et al. (2000). Gestational age- and birthweight-specific declines in infant mortality in Canada, 1985–94. Fetal and infant health study group of the canadian perinatal surveillance system. Paediatric and Perinatal Epidemiology, 14(4), 332–339.
Paul, D. A., Mackley, A., Locke, R. G., Stefano, J. L., & Kroelinger, C. (2009). State infant mortality: An ecologic study to determine modifiable risks and adjusted infant mortality rates. Maternal and Child Health Journal, 13(3), 343–348.
Centers for Disease Control and Prevention. (2004). Racial/ethnic trends in fetal mortality—United States, 1990–2000. MMWR Morbidity and Mortality Weekly Report, 53(24), 529–532.
MacDorman, M. F., Hoyert, D. L., Martin, J. A., Munson, M. L., & Hamilton, B. E. (2007). Fetal and perinatal mortality, United States, 2003. National Vital Statistics Reports, 55(6), 1–17.
MacDorman, M. F., Munson, M. L., & Kirmeyer, S. (2007). Fetal and perinatal mortality, United States, 2004. National vital statistics reports. Hyattsville, MD: National Center for Health Statistics.
MacDorman, M. F., & Kirmeyer, S. (2009). Fetal and perinatal mortality, United States, 2005. National Vital Statistics Reports, 57(8), 1–19.
Kochanek, K. D., & Martin, J. A. (2005). Supplemental analyses of recent trends in infant mortality. International Journal of Health Services, 35(1), 101–115.
Martin, J. A., Kung, H. C., Mathews, T. J., Hoyert, D. L., Strobino, D. M., Guyer, B., et al. (2008). Annual summary of vital statistics: 2006. Pediatrics, 121(4), 788–801.
Joseph, K. S., & Kramer, M. S. (1996). Recent trends in Canadian infant mortality rates: effect of changes in registration of live newborns weighing less than 500 g. CMAJ, 155(8), 1047–1052.
Joseph, K. S., & Kramer, M. S. (1997). Recent trends in infant mortality rates and proportions of low-birth-weight live births in Canada. Cmaj, 157(5), 535–541.
Phelan, S. T., Goldenberg, R., Alexander, G., & Cliver, S. P. (1998). Perinatal mortality and its relationship to the reporting of low-birthweight infants. American Journal of Public Health, 88(8), 1236–1239.
Alexander, G. R., Himes, J. H., Kaufman, R. B., Mor, J., & Kogan, M. (1996). A United States national reference for fetal growth. Obstetrics and Gynecology, 87(2), 163–168.
MacDorman, M. F., Martin, J. A., Mathews, T. J., Hoyert, D. L., & Ventura, S. J. (2005). Explaining the 2001–2002 infant mortality increase in the United States: Data from the linked birth/infant death data set. International Journal of Health Services, 35(3), 415–442.
Petersen, D. J., & Alexander, G. R. (1997). Threats to accurate interpretation of secondary data. In J. B. Kotch (Ed.), Maternal and child health: Programs, problems and policy in public health (pp. 395–404). Gaithersburg: Aspen Press.
Alexander, G. R., Petersen, D. J., Wingate, M. S., & Kirby, R. S. (2005). Research issues in maternal and child health. In J. B. Kotch (Ed.), Maternal and child health: Programs, problems and policy in public health (2nd ed., pp. 493–533). Sudbury: Jones and Bartlett.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was performed without any financial support.
Rights and permissions
About this article
Cite this article
Ehrenthal, D.B., Wingate, M.S. & Kirby, R.S. Variation by State in Outcomes Classification for Deliveries Less Than 500 g in the United States. Matern Child Health J 15, 42–48 (2011). https://doi.org/10.1007/s10995-010-0566-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-010-0566-y