
Abstract
Long-term longitudinal studies that examine whether there are distinct trajectories of at-risk depressive symptoms and alcohol use across the high school years (e.g., high co-occurrence) are rare in normative samples of adolescent boys and girls; yet, this assessment is of critical importance for developing effective prevention and intervention strategies. Moreover, the role of self-regulation and novelty-seeking behavior in differentiating among distinct subgroups of adolescents is not clear. To address these gaps, the present study sought to identify subgroups of adolescent boys and girls that indicated at-risk trajectories across the high school years for both depressive symptoms and alcohol use, and examined the role of delay of gratification and novelty seeking at baseline in differentiating among the subgroups. Canadian adolescents (N = 4,412; 49 % female) were surveyed at four time points (grades 9, 10, 11, and 12). Parallel process latent class growth analyses revealed four distinct subgroups for both boys and girls, encompassing high co-occurrence, depressive symptoms only, alcohol use only, and low co-occurrence. Across gender, delay of gratification at baseline differentiated among the four subgroups, with the High Co-Occurrence Group group scoring the lowest and the Low Co-Occurrence Group the highest. Lower novelty-seeking scores at baseline were associated more with being in the Depressive Symptoms Only Group relative to the other groups, particularly the Alcohol Use Only Group for boys. Thus, delay of gratification and novelty seeking may be useful in identifying youth at risk for co-occurring depressive symptoms and alcohol use trajectories, as well as at-risk trajectories for only one of these behaviors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adolescence often is associated with the onset of internalizing behaviors such as depressive symptoms (Rohde et al. 2009) as well as significant increases in risk behaviors such as alcohol use (Measelle et al. 2006), making it a sensitive age period for investigating these behaviors. While many studies have been conducted on adolescent depressive symptoms and alcohol use, research is limited on the co-occurrence of at-risk levels of these two behaviors within the same individual. Moreover, of the studies on co-occurrence that have been conducted, many have focused on early adolescent, clinical, or adult samples (e.g., Chen and Simons-Morton 2009; Cranford et al. 2011), and/or have not included a long-term longitudinal focus on the trajectories of both of these behaviors over time (e.g., Rohde et al. 1996, 2013; Windle and Davies 1999). Importantly, research also is limited on the role of self-regulation and novelty-seeking behaviors as predictors of the co-occurrence of at-risk depressive symptoms and alcohol use trajectories (although see Eisenberg et al. 2001 for a study with children). The current study addresses this gap by examining trajectories of depressive symptoms and alcohol use across the high school years, and by investigating the role of self-regulation and novelty-seeking behaviors in differentiating among subgroups of adolescent boys and girls that exhibit distinct trajectories over time on both problem behaviors.
Although most of the research on depressive symptoms and alcohol use among adolescents has examined these behaviors separately, positive correlations have been found between depressive symptoms and alcohol use in this age group (e.g., Marmorstein 2010). As a result, researchers increasingly have attempted to understand why the two behaviors might be linked (e.g., Swendsen and Merikangas 2000). One focus has been on exploring common risk factors. For example, a great deal of attention has been paid in recent years to the role that self-regulation and novelty-seeking behaviors might play in adolescent problem behaviors (e.g., Steinberg 2010). Although self-regulation has been defined in a number of ways, the most pertinent to this study are effortful control and delay of gratification. Effortful control has been described as the efficiency of executive function, including the ability to inhibit a dominant response while activating a subdominant response (Rothbart and Bates 2006). Similarly, delay of gratification is defined as showing a preference for a delayed more valuable reward versus an immediate but less valuable one (Mischel et al. 1989). In contrast, novelty-seeking behaviors are conceived as the tendency to explore and to actively seek out new situations (Windle and Lerner 1986). In the present study, we specifically focus on the role of delay of gratification and novelty seeking in predicting distinct trajectories of depressive symptoms and alcohol use.
According to the Dual Systems Model (Steinberg 2010), increases in problem behaviors such as alcohol use in adolescence may be the result of a temporal gap between an early maturing socio-emotional system (hypothesized to be a result of increases in the sensitivity and efficiency of the dopaminergic system, perhaps linked to puberty, leading to increases in approach motivation and novelty-seeking behaviors), and a slower maturing self-regulatory system (hypothesized to be led by the prefrontal cortex, associated with delay of gratification, which may not be fully mature until the mid-20 s). In other words, the greater maturity of the socio-emotional system in early adolescence is thought to lead to increased novelty-seeking behaviors that may challenge the still developing cognitive control system, such that the ability to self-regulate is compromised (Spear 2000; Steinberg 2010). Evidence in support of this hypothesis comes from longitudinal studies that have shown that novelty-seeking behaviors (e.g., sensation seeking) increase from age 12–15 and then remain relatively stable across adolescence until slowly declining in the 20 s, while self-regulation (e.g., impulsivity) tends to be highest in childhood and then declines steadily across the adolescent and young adult years (Harden and Tucker-Drob 2011; Steinberg et al. 2008).
Importantly, the focus on novelty seeking and self-regulation in the Dual Systems Model also can help explain individual differences in problem behavior across adolescents. For example, research consistently has demonstrated that adolescents with lower levels of self-regulation are more likely to engage in problem behaviors than their peers (e.g., Ernst et al. 2006; Spear 2000; Wills and Stoolmiller 2002). Block and Block (1980; Block and Kremen 1996) also support the assertion that individuals low in self-regulation may be prone to problem behaviors. However, Block and Block also suggest that self-regulation might lie on a spectrum from over-control to under-control, in which each end of the spectrum is associated with different problem behaviors. Specifically, they characterize over-controlled individuals as being low in approach motivation and novelty-seeking behaviors, and having a propensity to overly self-regulate or delay gratification. In such a case, over-controlled individuals might indiscriminately inhibit positive as well as negative emotions, putting them at greater risk than their peers for depressive symptoms. Support for this hypothesis has been found in a number of studies (Murray and Kochanska 2002; Wilson et al. 2009). For example, Murray and Kochanska (2002) examined differences in self-regulation (low, moderate, high effortful control) with respect to internalizing (i.e., depressive symptoms) and externalizing problem behaviors (i.e., conduct problems) in a sample of children aged 2.5–5.5 years. Their results indicated that the low effortful control group (i.e., under-controlled) had the highest number of externalizing behaviors, the high effortful control group (i.e., over-controlled) had the highest number of internalizing behaviors, and the moderate effortful control group had the fewest problem behaviors. Wilson et al. (2009), in a sample of children aged 8–11, found the same pattern of results. Moreover, the finding for internalizing behaviors also has some support from research on brain function among adolescents who are depressed, which reveals decreased striatal reactivity (an area related to approach motivation and novelty-seeking processing) but increased medial prefrontal cortex reactivity (an area linked to self-regulation) to monetary reward stimuli, suggesting possible overregulation of reward processing in this population in comparison to a sample of healthy adolescents (Forbes et al. 2009).
In contrast, Smoski et al. (2009) also found decreased striatal reactivity among individuals reporting depression, but did not find support for overregulation of reward processing. In fact, similar to alcohol use, some researchers have suggested that low self-regulation is a risk factor for emotional problems, (e.g., Moriya and Tanno 2008). Specifically, low effortful control has been shown to predict internalizing behaviors such as depressive symptoms in both preadolescents and adolescents (Verstraeten et al. 2009; Wang et al. 2012), providing some support for the assertion that alcohol use and depressive symptoms may share the common risk factor of low self-regulation.
Interestingly, other researchers such as Tice et al. (2001) suggest that adolescents who exhibit depressive symptoms, in an effort to reduce emotional distress, may be more likely to focus on the immediate present and short-term rewards than they are to prioritize long-term goals. As a result, adolescents with depressive symptoms may turn to activities that promise immediate pleasure, such as alcohol use, in an effort to enhance their mood. In other words, individuals may exhibit co-occurrence of depressive symptoms and alcohol use because depressive symptoms are thought to be alleviated by alcohol use (i.e., the self-medication hypothesis). Alternatively, other researchers hypothesize that consistent high alcohol use might affect brain chemistry, which in turn may affect self-regulatory skills (Crews et al. 2000; López-Caneda et al. 2013), and thereby lead to increased depressive symptoms over time. There have been mixed findings in the literature with regard to the direction of effects between alcohol use and depressive symptoms among adolescents (Hooshmand et al. 2012; Windle et al. 2008), although many of these studies have included composite variables encompassing several health-risk behaviors (e.g., alcohol, smoking, and marijuana use; Measelle et al. 2006), rather than just alcohol use.
One study explicitly tested the direction of effects between depressive symptoms and alcohol use using a longitudinal sample of high school students, but found no support for the self-medication hypothesis or for the alternate hypothesis that alcohol use leads to greater depressive symptoms over time (Hooshmand et al. 2012). In fact, most adolescents increased their frequency and amount of alcohol use over the high school years, regardless of their levels of depressive symptoms in grade 9. Increases in alcohol use tend to be normative across high school and drinking often occurs during social activities such as parties (Hooshmand et al. 2012; Needham 2007). As a result, drinking alcohol for some youth may be associated with enhanced social networks and feelings of belongingness. Of course, some youth may engage in alcohol use for self-medication reasons, but depressive symptoms also often are associated with social withdrawal (i.e., less approach motivation and novelty seeking behaviors; Windle and Davies 1999); thus, some adolescents with higher depressive symptoms may be less likely than their peers to participate in the social situations that co-occur with alcohol use (Fleming et al. 2008; Lewinsohn et al. 2003).
In fact, it may be that some youth engage in alcohol use because they are depressed, and therefore impulsively use alcohol to self-medicate, but it also may be that other youth engage in alcohol use only as a means of socializing with their friends and their alcohol use is not related to any depressive symptomatology. Similarly, it could be that some adolescents exhibit depressive symptoms as a result of alcohol use, but other adolescents display depressive symptoms that are not related to any alcohol use. In other words, some youth may report both depressive symptoms and alcohol use, while there might be others who exhibit only alcohol use or only depressive symptoms. To explore this question, person-centred analyses that specifically account for heterogeneity (i.e., individual differences) among adolescents in the pattern of these behaviors over time are needed. Person-centered analyses specifically assess subgroup heterogeneity (i.e., is there a group of youth who exhibit co-occurring alcohol use and depressive symptom behaviors over time, a group of youth who exhibit depressive symptoms only, and a group of youth who exhibit alcohol use only)? To the best of our knowledge, there are no long-term longitudinal studies that examine different trajectories of depressive symptoms and alcohol use across the high school years, in order to compare individuals exhibiting the co-occurrence of at-risk depressive symptoms and alcohol use trajectories to individuals with at-risk trajectories on only one of these behaviors. Furthermore, research is limited on how self-regulation and novelty-seeking behavior might be associated with different trajectories of depressive symptoms and alcohol use over time among adolescents.
It also is not clear whether trajectories of depressive symptoms and alcohol use might differ across boys and girls. Indeed, it has been well established in the literature that gender differences exist in the frequency of depressive symptoms, with girls exhibiting higher rates of depression than boys (Lewinsohn et al. 1993; Ruchkin et al. 2006). In contrast, older adolescent boys tend to engage in more at-risk alcohol use than girls (e.g., Miller et al. 2007). Thus, the assessment of gender differences is an important factor to assess when examining the co-occurrence of depressive symptoms and alcohol use in adolescence.
The Current Study
The study addressed two primary goals. First, we assessed the prevalence of distinct trajectories of depressive symptoms and alcohol use across the high school years. Depressive symptoms and alcohol use tend to have their onset in adolescence and increase during the high school years (Kandel and Davies 1982; Measelle et al. 2006), but the prevalence of trajectories that show co-occurrence of these behaviors within the same individual, across the high school years, is less clear for a normative high school sample. We hypothesized that we might find High Co-Occurrence, Depressive Symptoms Only, Alcohol Use Only, and Low Co-Occurrence Groups, but this analysis was exploratory given the lack of long-term longitudinal research addressing this issue in a normative adolescent population.
Second, we assessed whether delay of gratification (a form of self-regulation) and novelty seeking, both assessed at baseline, would differentiate among the different subgroups of individuals exhibiting distinct trajectories of depressive symptoms and alcohol use. We hypothesized that lower delay of gratification and higher novelty seeking at baseline would be more consistent with an Alcohol Use Only Group, relative to their peers, consistent with past research (e.g., Wills and Stoolmiller 2002; Windle and Davies 1999) and in congruence with the dual systems model (Steinberg 2010). A Low Co-Occurrence Group was expected to report the most positive scores on delay of gratification at baseline. It was not clear what delay of gratification and novelty-seeking behaviors might look like for a High Co-Occurrence Group or a Depressive Symptoms Only Group, however, given the mixed findings for depressive symptoms and the more limited research on co-occurrence. Finally, we investigated whether there would be gender differences in the results. Two demographic variables, parental education and at-risk background factors (e.g., parental divorce, learning disability, etc.), also were included as covariates in all analyses, given that both depression and alcohol use are associated with socio-economic status (e.g., Huckle et al. 2010; Lorant et al. 2003).
Methods
Sample
Students (N = 4,412, 49 % females; mean age in grade 9 = 14.3) from eight high schools encompassing a school district in Ontario, Canada, were surveyed in each grade of high school. This study was part of a larger longitudinal study on youth lifestyle choices. The overall participation rate ranged from 83 to 86 % across all the waves of data collection. Non-participation was due to student absenteeism (average of 13.5 %), parental refusal (average of .06 %), or student refusal (average of 1.4 %). Consistent with the broader Canadian population (Statistics Canada 2006), 92.4 % of the participants were born in Canada, and the most common ethnic backgrounds reported other than Canadian were Italian (31 %) and French (18 %). Data on socioeconomic status indicated mean levels of education for mothers and fathers falling between “some college, university or apprenticeship program” and “completed a college/apprenticeship/technical diploma” (5 % of parents did not complete high school and 25 % were university graduates). Furthermore, 70 % of the respondents reported living with both birth parents, 12 % with one birth parent and a stepparent, 15 % with one birth parent (mother or father only), and the remainder with other guardians (e.g., other relatives, foster parents, etc.).
Procedure
Active informed assent was obtained from the adolescent participants. Parents were provided with written correspondence mailed to each student’s home prior to the survey administration outlining the study; this letter indicated that parents could request that their adolescent not participate in the study. An automated phone message about the study also was left at each student’s home phone number. This procedure was approved by the participating school board and the University Research Ethics Board. At all time periods, the questionnaire was administered to students in classrooms by trained research staff. Students were informed that their responses were completely confidential.
Measures
Depressive symptoms and alcohol use were assessed in all four grades. Gender, parental education, at-risk background, delay of gratification, and novelty seeking were assessed in grade 9.
Gender
Gender of participants was assessed (1 = boy, 2 = girl).
Covariates
Parental education (one item per parent, averaged for those reporting on both parents, r = .45) was assessed. Higher scores indicated greater parental education (1 = did not finish high school to 6 = professional degree). At-risk background was measured as the number of risk factors that participants reported (i.e., participants were asked to indicate yes or no to whether they have a learning disability, are living or have lived in foster care, started using marijuana prior to age 13, have parents/guardians who engaged in narcotic use, had a teen mother, have parents who were or are depressed, or have parents who divorced). Higher scores indicate a greater number of risks.
Depressive Symptoms
Depressive symptoms were measured in grades 9 through 12 using the Center for Epidemiological Studies Depression Scale-Revised (CESD-R) (Eaton et al. 2004; Radloff 1977, 1991; Van Dam and Earleywine 2011). Participants indicated how often they experienced 20 symptoms (e.g., “I could not get going”) using a 5-point scale, with 0 = none of the time to 4 = most of the time. The scale has been shown to have good reliability with adolescent samples (e.g., Kim and Ge 2000; Radloff 1991). Ratings were rescored so that the CESD-R has the same range (0–60) as the original CESD (see htttp://cesd-r.com/cesdr/), and summed such that higher scores indicate greater depressive symptoms. Cronbach’s alphas across grades 9, 10, 11, and 12 ranged from .90 to .93 for boys, and .92 to .03 for girls.
Alcohol Use
Alcohol use was measured in grades 9 through 12 by frequency of use with an 8-pt scale, with 0 = never to 7 = every day, and average consumption per drinking episode was assessed with a 6-point scale, with 0 = less than 1 drink to 5 = 4 or more drinks (Adlaf et al. 1997; Willoughby et al. 2004). The scores on the 8-pt scale were re-coded to a 6-pt scale and then the two items were averaged. Correlations between frequency of use and average consumption per episode in grades 9, 10, 11, and 12 were .69, .70, .65, .68 for boys and .74, .71, .68, .66, for girls, respectively. Higher scores represent higher alcohol use.
Delay of Gratification
Delay of gratification was measured in grade 9 with five items (e.g., “I usually do what I want when I want to, I don’t think about what it will mean to me later”; I have difficulty saving money to buy something several weeks later”), on a 5-point scale, 1 = usually to 5 = never (adapted from Chen et al. 2004; Simons and Carey 2002; Wills et al. 2001). Cronbach’s alphas were .74 for boys and .77 for girls. Higher scores represent more delay of gratification.
Novelty Seeking
Novelty seeking was measured in grade 9 with five items from the approach subscale (e.g., “I am interested in new objects shown to me”; “I like trying new things”) of the Dimensions of Temperament Questionnaire (Windle and Lerner 1986), using a 4-point scale of 1 = never to 4 = always. Previous research has shown that the approach subscale is correlated with novelty seeking (e.g., Wills et al. 1998). Cronbach’s alphas were .71 for boys and .70 for girls. Higher scores represent higher novelty seeking.
Missing Data
There were missing data because some participants did not complete a wave of data collection due to absenteeism or because they moved to a school in another region, and because some students did not finish the entire questionnaire (10 % of data, consistent with other longitudinal survey studies, e.g., Hyde and Petersen 2009). We included three versions of the survey at each time period so that the same scales were not always near the end of the survey. Participants who completed the survey at all time periods were not significantly different from participants missing one, two, or three waves on any of the study measures, with the exception that participants who completed the survey at all four time periods reported significantly less alcohol use in grade 9 than their peers (Wilks λ < .001; η2 = .015; mean difference of .08, .15, and .10 for comparisons with three-wave, two-wave, and one-wave participants, respectively). Missing values were imputed using the EM (expectation-maximum) algorithm, with all demographic and study measures used in the imputation process. EM is an iterative maximum-likelihood (ML) procedure in which a cycle of calculating means and covariances followed by data imputation is repeated until a stable set of estimated missing values is reached. Methodological research has demonstrated that ML estimation is preferable to pair-wise deletion, list-wise deletion, or means substitution (Schafer and Graham 2002).
Plan of Analysis
Preliminary analyses included descriptive statistics for all variables. For all primary analyses, parental education and at-risk background were included as covariates. Analyses were conducted using MPlus (Version 7.0; Muthén and Muthén 1998–2012). Alpha level was set at .01 for all analyses given the large sample size. Growth curve analyses were first conducted to test if average change over time for depressive symptoms and alcohol use was linear or non-linear, and whether the growth shape was similar across boys and girls. A well-specified model fit was indicated by a comparative fit index (CFI) of >.95 and a root-mean-square error of approximation (RMSEA) of <.06 simultaneously (Hu and Bentler 1999).
A parallel-process latent class growth analysis (Nagin 2005) then was conducted simultaneously on the best fitting growth curve models for depressive symptoms and for alcohol use to identify if there were distinct co-occurring trajectories over time. Latent class growth modeling is a person-centered analysis that specifically explores subgroup heterogeneity in change over time in frequency of the behaviors. In order to determine which number of trajectory groups were best represented by the data, several criteria were considered: (a) interpretability of the classes, (b) Bayesian information criterion (BIC), such that smaller values of BIC indicate a better fit model, (c) significance of the Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMR-LRT) and/or the Bootstrap Likelihood Ratio Test (BLRT), which compare a particular model to a model with one fewer classes (i.e., a significant p value indicates that the estimated model provides a better fit to the data than the model with fewer classes), and (d) average latent class posterior probabilities close to 1.00 (Nylund et al. 2007). Entropy (an index of confidence that individuals belong to the correct class and that adequate separation between latent classes exists) also was examined; scores >.80 are good but there is no set cut-off criterion for entropy (Jung and Wickrama 2008). Finally, membership in the different trajectory groups was used as an outcome in multinomial logistic regression analyses with the covariates, delay of gratification, and novelty seeking included as predictors.
Results
Preliminary Analyses
All variables demonstrated acceptable skewness and kurtosis. Table 1 presents the means and standard deviations of the variables. On average, depressive symptoms and alcohol use increased over time. There were no gender differences in grade 9 for alcohol use, delay of gratification, or novelty seeking. However, girls reported higher depressive symptoms than boys, F(1, 4410) = 167.35, p < .001, η 2 = .037. For grades 10, 11, and 12, girls also reported significantly greater depressive symptoms than boys (all ps < .001, η 2 ranged from .005 to .044, with the larger effect sizes occurring in grades 9 and 10), but boys reported significantly greater alcohol use than girls (all ps < .001, η 2 ranged from .012 to .044, with the larger effect sizes occurring in grades 11 and 12).
Primary Analyses
Univariate Growth Trajectories
Prior to conducting the latent class growth analyses, univariate latent growth curve (LGC) models were conducted to test for linearity, and were first conducted separately for boys and girls to ensure that their growth shapes were similar (Muthén 2005). Separate growth models were identified for depressive symptoms and alcohol use by (a) first testing each variable on a linear growth model, in which the paths from the slope factor to the measured variables were fixed in a linear progression (i.e., 0 = grade 9; 1 = grade 10; 2 = grade 11; 3 = grade 12), (b) next testing a model for each variable in which the slope factor was replaced with a shape factor in order to test for non-linearity (Duncan et al. 2006), in which the loadings were set to 0 in grade 9, 1 in grade 12, and freely estimated in grades 10 and 11, and (c) then testing a quadratic model in which a quadratic factor was added to a linear slope factor, again to test for non-linearity. The Chi square difference test for depressive symptoms indicated that the model with the shape slope factor best fit the data for boys in comparison to the linear model, χ2 diff (2) = 35.40, p < .001, while the quadratic model best fit the data for girls, χ2 diff (4) = 67.83, p < .001. Boys increased in depressive symptoms over time, with a steeper increase between grade 10 and grade 11 than between the other grades, while girls had a smaller increase over time, with little change in the senior grades. The fit for the models was well-specified for both boys, CFI = .997; RMSEA = .038 (.018–.060) and girls, CFI = .998; RMSEA = .066 (.034–.105). Chi square difference tests for alcohol use revealed that the quadratic model best fit the data for both boys and girls (boys: χ2 diff (4) = 757.85, p < .001, girls: χ2 diff (4) = 812.05, p < .001), in comparison to the linear model. Furthermore, the fit for the quadratic model was well-specified for boys, CFI = 1.00; RMSEA = .020 (.000–.051), and for girls, CFI = .998; RMSEA = .046 (.026–.069). Examination of the best fitting models revealed that the estimated variances of the intercepts and slope factors in the models were all different significantly from zero. This finding indicated that there was significant variability in individual trajectories, and therefore substantiated the use of latent class growth analyses (Nagin 2005) to examine subgroup heterogeneity. Given that the growth shapes for depressive symptoms were different between boys and girls, separate latent class growth analyses were conducted for boys and girls (see Muthén 2005). The best fitting growth curve models for boys and girls were used in the latent class growth analyses.
Parallel-process latent class growth analyses
Fit indices for model comparisons are shown in Table 2. For boys, the four-class solution was considered the optimal model. The LMR-LRT became non-significant at five classes, indicating that adding the fifth class did not significantly improve the model. The entropy value for four classes was .83, and the average latent class posterior probabilities ranged from .88 to .92, indicating that a high proportion of boys were correctly classified. There also was good distinction among the four classes and they were consistent with our expectations. Finally, the drop in the BIC from four to five classes was much smaller than the drop from three to four classes, again suggesting that the four class solution best fit the data. Figure 1 shows the trajectories of the four classes, which included (a) a High Co-Occurrence Group [scores on the depressive symptoms measure indicated risk for depressive disorder (i.e., a cutoff of 28 on the CESD-R has been suggested by Radloff 1991)], and an at-risk level of alcohol use [i.e., on average, binge drinking level and high frequency of alcohol use (i.e., once a week)—see Willoughby et al. 2004); (b) a Depressive Symptoms Only Group (scores on the depressive symptoms measure indicated risk for depressive disorder but scores on the alcohol measure did not indicate at-risk levels of alcohol use); (c) an Alcohol Use Only Group (scores on the depressive symptoms measure did not indicate risk for depressive disorder but scores on the alcohol measure indicated at-risk levels of alcohol use); and (d) a Low Co-Occurrence Group (scores on both the depressive symptoms and alcohol use measures were at low levels and did not indicate at-risk levels).

Sub-group trajectories for depressive symptoms and alcohol use across 4 years of high school for boys. Notes Dep = Depressive Symptoms; Alc = Alcohol Use
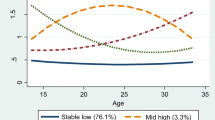
For girls, the LMR-LRT became non-significant at four classes, indicating that adding the fourth class did not significantly improve the model. Examination of the three class model indicated good distinction among the three classes but a Depressive Symptoms Only Group did not emerge. This was unexpected given that girls are more likely than boys to report depressive symptoms and to exhibit lower alcohol use. In contrast, examination of the four class model included a Depressive Symptoms Only Group model and also indicated good distinction among the classes. The entropy value for the fourth class increased to .86 from .85 in the third class, and the average latent class posterior probabilities ranged from .90 to .95 (identical to the third class model), indicating that a high proportion of girls were correctly classified. Finally, the drop in the BIC from three to four classes was still large, in contrast to the smaller drop in the BIC from four to five classes, again suggesting that the four class solution might be the best fitting model. As the four class model was more interpretable (see Jung and Wickrama 2008, Nylund et al. 2007), we chose the four class model as the final solution. Figure 2 shows the trajectories of the four classes, which included (a) a Moderately High Co-Occurrence Group [scores on the depressive symptoms measure indicated close to at-risk levels for depressive disorder (scores ranged from 26 to 27 but the recommended cutoff for at-risk levels is at 28—see Radloff 1991), and scores on the alcohol measure indicated high levels of alcohol use]; (b) a Depressive Symptoms Only Group (scores on the depressive symptoms measure indicated risk for depressive disorder but scores on the alcohol measure did not indicate at-risk levels of alcohol use); (c) an Alcohol Use Only Group (scores on the depressive symptoms measure did not indicate risk for depressive disorder but scores on the alcohol measure indicated moderate levels of alcohol use); (d) a Low Co-Occurrence Group (scores on both the depressive symptoms and alcohol use measures were at low levels).

Sub-group trajectories for depressive symptoms and alcohol use across 4 years of high school for girls. Notes: Dep = Depressive Symptoms; Alc = Alcohol Use
To check whether the High Co-Occurrence Groups might have higher alcohol use or depressive symptoms than the Depressive Symptoms Only and Alcohol Use Only Groups, repeated measures ANOVAs comparing alcohol scores across grades between the High Co-Occurrence and Alcohol Use Only Groups, as well as depressive symptom scores across grades between the High Co-Occurrence and Depressive Symptoms Only Groups, were conducted. For boys, there was no significant difference in alcohol use between the High Co-Occurrence and Alcohol Use Only Groups, but there was a significant main effect for group with depressive symptoms, F(1, 550), p < .001, η 2 = .11. The High Co-Occurrence Group had higher overall depressive symptoms scores (M = 30.57) than the Depressive Symptoms Only Group (M = 27.04), although it is important to note that the Depressive Symptoms Only Group had at-risk scores in the senior grades.
For girls, there was a significant interaction between group and grade for depressive symptoms, F(3, 1773) = 11.512, p < .001, η 2 = .02, with the Moderately High Co-Occurrence Group reporting lower depressive symptoms scores than the Depressive Symptoms Only Group, with the differences wider in the middle grades (see Fig. 2; although again the scores on the depressive symptoms measure for the Moderately High Co-Occurrence Group indicated very close to at-risk levels). There also was a significant interaction between group and grade for alcohol use, F(3, 3330) = 44.825, p < .001, η 2 = .04, with the Moderately High Co-Occurrence Group reporting higher alcohol use scores than the Alcohol Use Only Group, with the differences wider at the lower grades.
Multinomial Logistic Regression Group Comparisons
Means and standard deviations for the study measures (i.e., delay of gratification, novelty seeking, at-risk background, and parental education) across the different co-occurring groups are shown in Table 3 for boys and Table 4 for girls. Both delay of gratification (p < .001) and novelty seeking (p = .002) significantly differentiated among the four groups for boys. Boys with higher delay of gratification scores at baseline had increased odds of being in the Low Co-Occurrence Group in comparison to the High Co-Occurrence, OR = 4.881, p < .001 (95 % CI = 3.652–6.523), Depressive Symptoms Only, OR = 2.730, p < .001 (95 % CI = 2.085–3.575), and Alcohol Use Only, OR = 2.844, p < .001 (95 % CI = 2.292–3.530) Groups. In turn, higher delay of gratification scores at baseline also was associated with increased odds of being in the Depressive Symptoms Only and Alcohol Use Only Groups in comparison to the High Co-Occurrence Group [OR = 1.788, p < .001 (95 % CI = 1.304–2.450), and OR = 1.716, p < .001 (95 % CI = 1.312–2.245, respectively)]. In terms of novelty seeking, the only significant finding was that individuals with higher novelty-seeking scores at baseline had increased odds of being in the Alcohol Use Only Group in comparison to the Depressive Symptoms Only Group, OR = 1.755, p < .001 (95 % CI = 1.291–2.385) Groups.
Both delay of gratification and novelty seeking also significantly differentiated among the four groups for girls, ps < .001. Identical to boys, girls with higher delay of gratification scores at baseline had increased odds of being in the Low Co-Occurrence Group in comparison to the Moderately High Co-Occurrence, OR = 11.224, p < .001 (95 % CI = 8.434–14.936), Depressive Symptoms Only, OR = 4.813, p < .001 (95 % CI = 3.643–6.358), and Alcohol Use Only Groups, OR = 3.071, p < .001 (95 % CI = 2.493–3.784). In turn, higher delay of gratification scores at baseline also was associated with increased odds of being in the Depressive Symptoms Only and Alcohol Use Only Groups in comparison to the Moderately High Co-Occurrence Group, [OR = 2.332, p < .001 (95 % CI = 1.744–3.118); OR = 3.655, p < .001 (95 % CI = 2.844–4.696, respectively)], and being in the Alcohol Use Only Group relative to the Depressive Symptoms Only Group, OR = 1.567, p = .001 (95 % CI = 1.213–2.024). Finally, lower novelty-seeking scores at baseline was associated with increased odds of being in the Depressive Symptoms Only Group in comparison to the Low Co-Occurrence, OR = 1.941, p < .001 (95 % CI = 1.414–2.664), Alcohol Use Only, OR = 2.437, p < .001 (95 % CI = 1.790–3.319), and Moderately High Co-Occurrence, OR = 1.950, p < .001 (95 % CI = 1.351–2.815) Groups.
Discussion
Although past studies indicate that depressive symptoms and alcohol use tend to increase in adolescence and are positively correlated (Kandel and Davies 1982; Marmorstein 2010; Measelle et al. 2006), the longitudinal examination of the co-occurrence of these behaviors within the same individual, across the high school years, is limited. Yet, identifying whether problem behaviors co-occur may be critical for developing effective prevention and intervention strategies. The present study addressed this gap by examining the prevalence of distinct trajectories of depressive symptoms and alcohol use (e.g., high co-occurrence, high alcohol use only, etc.) across grades 9–12 in a normative adolescent sample, and by examining the predictive role of self-regulation (i.e., delay of gratification) and novelty-seeking behavior, assessed at baseline, in differentiating among these distinct trajectories.
Our data identified four distinct trajectories of depressive symptoms and alcohol use across the high school years, for both boys and girls. Ten percent of boys and 14 % of girls were classified as being in a High Co-Occurrence Group, while 15 % of boys and 14 % of girls were classified as being in a Depressive Symptoms Only Group. In contrast, prevalence rates for the Alcohol Use Only Groups were 32 % for boys and 37 % for girls (although mean levels of alcohol use levels were at a moderate level for girls, rather than at a high level as with the boys), and similar to the rates of Low Co-Occurrence Groups, which were 44 % for boys and 36 % for girls. These findings support extensive research outlining the prevalence of alcohol use among adolescents (e.g., see Hooshmand et al. 2012), but also highlight the significance of depressive symptoms among this group of adolescents, both concurrently with at-risk alcohol use and also independent of at-risk alcohol use.
Importantly, delay of gratification at baseline significantly differentiated among the four groups for both boys and girls. The greatest difference on delay of gratification was seen between the High Co-Occurrence and Low Co-Occurrence Groups, with the Depressive Symptoms Only and Alcohol Use Only Groups in the middle. Moreover, the pattern of findings generally was consistent across gender, and was found for girls even though the Moderately High Co-Occurrence Group had lower depressive symptoms that the Depressive Symptoms Only Group. This finding supports the hypothesis that lower delay of gratification is a common risk factor for depressive symptoms and alcohol use in adolescence (Tice et al. 2001; Wills and Stoolmiller 2002), and confirms the expectations outlined by the Dual Systems Model (Steinberg 2010) that individual differences in self-regulation should predict higher levels of problem behavior among adolescents. Critically, delay of gratification differentiated between individuals with two co-occurring problem behaviors and individuals with one problem behavior. Indeed, the assessment of delay of gratification may be particularly relevant for the consideration of adolescent boys and girls who are at risk for co-occurring depressive symptoms and alcohol use. Delay of gratification, however, also significantly differentiated the Depressive Symptoms Only and Alcohol Use Only Groups from the Low Co-Occurrence Group. An important implication of these results, therefore, is that developing programs for adolescents that focus on improving delay of gratification may be particularly helpful for reducing co-occurring depressive symptoms and alcohol use, but even for reducing at-risk depressive symptoms and alcohol use that occur independently of each other. Moreover, the measure of delay of gratification used in the current study is related to the broader concept of self-regulation, which is thought to encompass many characteristics, such as planning, impulsivity, and effortful control, among others. Prevention and intervention programs that address multiple characteristics of self-regulation, therefore, may be particularly effective.
In no case was higher delay of gratification at baseline associated with higher depressive symptoms (i.e., over-control), in contrast to findings reported by Murray and Kochanska (2002) and Wilson et al. (2009). While the present study used a person-centered analysis and a similar conceptualization of delay of gratification as that used in these previous studies, it varied in the methodology used and the age range of participants (adolescents vs children). In particular, the present study used self-report measures whereas Murray and Kochanska (2002) and Wilson et al. (2009) used parent and teacher reports for problem behaviors (e.g., depressive symptoms). Inferring depressive symptoms from mother or teacher reports may be more difficult than using self-report measures as depressive symptoms can be challenging to accurately observe. Future research, however, should explore these conflicting findings further in a longitudinal study that examines the role of delay of gratification in depressive symptoms across both childhood and adolescence.
An interesting finding in the present study was that there were limited differences between the Depressive Symptoms Only and Alcohol Use Only Groups on the study measures, with the exception of novelty seeking, indicating that novelty seeking might be one way to discriminate between these two groups. Partial support was given to our hypothesis that higher novelty-seeking scores would be associated more with the Alcohol Use Only Group than with the other groups. Specifically, we found this result only for boys, and it was only the Depressive Symptoms Only Group that had lower novelty-seeking scores than the Alcohol Use Only Group. For girls, the Depressive Symptoms Only Group had lower novelty-seeking scores than all of the other groups, with no other differences among the groups. These findings suggest that, in our sample, novelty seeking appears to be negatively related to depressive symptoms more so than positively and uniquely related to alcohol use. Furthermore, these results are consistent with research on brain function among adolescents who are depressed that has found decreased striatal reactivity (an area related to novelty seeking processing) to monetary reward stimuli (e.g., Forbes et al. 2009; Smoski et al. 2009), as well as research that has indicated that depressive symptoms often are associated with social withdrawal (Fleming et al. 2008; Lewinsohn et al. 2003; Windle and Davies 1999). Given that alcohol use typically occurs in social situations, social withdrawal might explain why individuals in the Depressive Symptoms Only Group engaged in low levels of alcohol use in comparison to their peers.
In contrast, given their high scores on both depressive symptoms and alcohol use, the individuals in the High Co-Occurrence Groups, in particular, may drink alcohol in order to self-medicate, rather than only as a way to socialize with friends. Alternatively, it also is possible that high levels of alcohol use in the High Co-Occurrence Groups may have led to greater depressive symptoms over time (e.g., see Fergusson et al. 2009). Again, research findings are mixed in terms of the direction of effects between alcohol use and depressive symptoms during the adolescent years, with some studies finding no effects (e.g., Hooshmand et al. 2012), some studies finding support for depressive symptoms leading to greater alcohol use over time (i.e., self-medication; e.g., Measelle et al. 2006), some studies finding support for alcohol use leading to greater depressive symptoms over time (e.g., Fergusson et al. 2009), and other studies finding support for bidirectional associations (e.g., Locke and Newcomb 2001). Given the results of the present study, an important avenue for future research will be to explicitly test the direction of effects hypotheses in a longitudinal study specifically with individuals exhibiting high-co-occurrence of depressive symptoms and alcohol use. Testing the direction of effects with this population will enhance our understanding of why these two behaviors are linked for these individuals, and will facilitate our ability to develop significant prevention and intervention strategies.
The current study is not without limitations. First, we relied on self-report assessments of depressive symptoms and alcohol use, and would have benefited from a corroborating clinical assessment of risk (e.g., major depressive disorder or alcohol abuse). Second, it would be interesting to see if measuring novelty seeking and delay of gratification with behavioral tasks (e.g., see Eisenberg et al. 2013; Mischel et al. 1989) rather than self-report might result in different findings. Third, while the findings from the current study support the hypothesis of delay of gratification and novelty seeking as common risk factors for problem behavior in adolescence, these measures were only assessed at one time point—grade 9. It is important for future studies to include longitudinal assessments of delay of gratification and novelty seeking. Establishing trajectories of these measures across the high school years could provide additional information regarding the development of co-occurring problem behaviors, as well as the developmental progression of delay of gratification and novelty seeking. Fourth, while we controlled for several important covariates, there are many other biological and social factors that were not accounted for in this study (e.g., peer relationships). Finally, the participants came from a relatively homogeneous sample. Thus, these results may not generalize to populations from other regions with greater ethnic diversity. For example, drinking may not be normative, and depressive symptoms may be reported differently for individuals with cultural or religious backgrounds that are more prohibitive or that carry greater stigma for mental illness.
Conclusions
Overall, between 10 and 14 % of adolescents exhibited high co-occurrence of depressive symptoms and alcohol use, while 14–15 % displayed depressive symptoms only. In contrast, the prevalence of individuals who reported at-risk alcohol use only was higher, at 32–37 %. Importantly, an assessment of delay of gratification significantly differentiated among the groups (particularly between adolescents in the High Co-Occurrence and Low Co-Occurrence Groups), while lower novelty seeking was associated more with adolescents reporting depressive symptoms only relative to other three groups, but particularly relative to the Alcohol Use Only Group for boys. If delay of gratification and novelty seeking can successfully predict group membership in a normative adolescent sample, it is likely that they may be crucial even more for clinical samples. Finally, developing programs for adolescents that focus on improving delay of gratification and self-regulation in general may be particularly helpful for reducing co-occurring depressive symptoms and alcohol use, but even for reducing at-risk depressive symptoms and alcohol use that occur independently of each other.
References
Adlaf, E. M., Ivis, F. J., & Smart, R. G. (1997). Ontario student drug use survey, 1977–1997. Toronto, Ontario: Addiction Research Foundation.
Block, J., & Block, J. H. (1980). The role of ego-control and ego-resiliency in the organization of behavior. In W. A. Collins (Ed.), Development of cognition, affect, and social relations: The Minnesota symposia on child psychology. NJ: Erlbaum.
Block, J. H., & Kremen, A. M. (1996). IQ and ego-resiliency: Conceptual and empirical connections and separateness. Journal of Personality and Social Psychology, 70, 349–361. doi:10.1037/0022-3514.70.2.349.
Chen, K., Sheth, A., Elliott, D., & Yeager, A. (2004). Prevalence and correlates of past-year substance use, abuse, and dependence in a suburban community sample of high-school students. Addictive Behaviors, 29, 413–423. doi:10.1016/j.addbeh.2003.08.013.
Chen, R., & Simons-Morton, B. (2009). Concurrent changes in conduct problems and depressive symptoms in early adolescents: A developmental person-centered approach. Development and Psychopathology, 21, 285–307. doi:10.1017/S0954579409000169.
Cranford, J. A., Nolen-Hoeksema, S., & Zucker, R. A. (2011). Alcohol involvement as a function of co-occurring alcohol use disorders and major depressive episode: Evidence from the National Epidemiological Survey on Alcohol and Related Conditions. Drug and Alcohol Dependence, 117, 145–151. doi:10.1016/j.drugalcdep.2011.01.011.
Crews, F. T., Braun, C. J., Hoplight, B., Switzer, R. C., & Knapp, D. J. (2000). Binge ethanol consumption causes differential brain damage in young adolescent rats compared with adult rats. Alcoholism, Clinical and Experimental Research, 24, 1712–1723. doi:10.1111/j.1530-0277.2000.tb01973.x.
Duncan, T. E., Duncan, S. C., Strycker, L. A., Li, F., & Alpert, A. (2006). An introduction to latent variable growth curve modeling: Concepts, issues, and applications (2nd ed.). NJ: Erlbaum.
Eaton, W. W., Muntaner, C., Ybarra, M., Smith, C. B., & Tien, A. Y. (2004). Revision of the Center for Epidemiologic Studies Depression (CESD) scale. In M. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment. NJ: Erlbaum.
Eisenberg, N., Cumberland, A., Spinrad, T. L., Fabes, R. A., Shephard, S. A., Reiser, M., et al. (2001). The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Development, 72, 1112–1134. doi:10.1111/1467-8624.00337.
Eisenberg, N., Edwards, A., Spinrad, T. L., Sallquist, J., Eggum, N. D., & Reiser, M. (2013). Are effortful and reactive control unique constructs in youth children? Developmental Psychology, 49, 2082–2094. doi:10.1037/a0031745.
Ernst, M., Luckenbaugh, D. A., Moolchan, E. T., Leff, M. K., Allen, R., Eshel, N., et al. (2006). Behavioral predictors of substance-use initiation in adolescence with and without attention deficity/hyperactivity disorder. Pediatrics, 117, 2030–2039. doi:10.1542/peds.2005-0704.
Fergusson, D. B., Boden, J. M., & Horwood, L. J. (2009). Tests of causal links between alcohol use or dependence and major depression. Archives of General Psychiatry, 66, 260–266. doi:10.1001/archgenpsychiatry.2008.543.
Fleming, C. B., Mason, W. A., Mazza, J. J., Abbott, R. D., & Catalano, R. F. (2008). Latent growth modeling of the relationship between depressive symptoms and substance use during adolescence. Psychology of Addictive Behaviors, 22, 186–197. doi:10.1037/0893-164X.22.2.186.
Forbes, E. E., Hariri, A. R., Martin, S. L., Silk, J. S., Moyles, D. L., Fisher, P. M., et al. (2009). Altered striatal activation predicting real-world positive affect in adolescent major depressive disorder. American Journal of Psychiatry, 166, 64–73. doi:10.1176/appi.ajp.2008.07081336.
Harden, K. P., & Tucker-Drob, E. M. (2011). Individual differences in the development of sensation seeking and impulsivity during adolescence: Further evidence for a dual systems model. Developmental Psychology, 47, 739–746. doi:10.1037/a0023279.
Hooshmand, S., Willoughby, T., & Good, M. (2012). Does the direction of effects in the association between depressive symptoms and health-risk behaviors differ by behavior? A longitudinal study across the high school years. Journal of Adolescent Health, 50, 140–147. doi:10.1016/j.jadohealth.2011.05.016.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. doi:10.1080/10705519909540118.
Huckle, T., You, R. Q., & Casswell, S. (2010). Socio-economic status predicts drinking patterns but not alcohol-related consequences independently. Addiction, 105, 1192–1202. doi:10.1111/j.1360-0443.2010.02931.x.
Hyde, J. S., & Petersen, J. L. (2009). A longitudinal investigation of peer sexual harassment victimization in adolescence. Journal of Adolescence, 32, 1173–1188. doi:10.1016/j.adolescence.2009.01.011.
Jung, T., & Wickrama, K. (2008). An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass, 2, 302–317. doi:10.1111/j.1751-9004.2007.00054.x.
Kandel, D. B., & Davies, M. (1982). Epidemiology of depressive mood in adolescents: An empirical study. Archives of General Psychiatry, 39, 1205–1212.
Kim, S. Y., & Ge, X. (2000). Parenting and adolescent depressive symptoms in Chinese American families. Journal of Family Psychology, 14, 420–435. doi:10.1037/0893-3200.14.3.420.
Lewinsohn, P. M., Hops, H., Roberts, R. E., Seeley, J. R., & Andrews, J. A. (1993). Adolescent psychopathology: I. Prevalence of incidence of depression and other DSM -III -R disorders in high school students. Journal of Abnormal Psychology, 102, 133–144.
Lewinsohn, P. M., Pettit, G. S., Joiner, J., Thomas, E., & Seeley, J. R. (2003). The symptomatic expression of major depressive disorder in adolescents and young adults. Journal of Abnormal Psychology, 112, 244–252. doi:10.1037/0021-843X.112.2.244.
Locke, T. F., & Newcomb, M. D. (2001). Alcohol involvement and dysphoria: A longitudinal examination of gender differences from late adolescence to adulthood. Psychological and Addictive Behaviors, 15, 227–236. doi:10.1037/0893-164X.15.3.227.
López-Caneda, E., Holquin, S. R., Cadaveia, F., Corral, M., & Doallo, S. (2013). Impact of alcohol use on inhibitory control (and vice versa) during adolescence and young adulthood: A review. Alcohol and Alcoholism,. doi:10.1093/alcalc/agt168.
Lorant, V., Deliége, D., Eaton, W., Robert, A., Philippt, P., & Ansseau, M. (2003). Socioeconomic inequalities in depression: A meta-analysis. American Journal of Epidemiology, 157, 98–112. doi:10.1093/aje/kwf182.
Marmorstein, N. R. (2010). Longitudinal associations between depressive symptoms and alcohol problems: The influence of comorbid delinquent behavior. Addictive Behaviors, 35, 564–571. doi:10.1016/j.addbeh.2010.01.004.
Measelle, J. R., Stice, E., & Hogansen, J. M. (2006). Developmental trajectories of co- occurring depressive, eating, antisocial, and substance abuse problems in female adolescents. Journal of Abnormal Psychology, 115, 524–538. doi:10.1037/0021-843X.115.3.524.
Miller, J. W., Naimi, T. S., Brewer, R. D., & Jones, S. E. (2007). Binge drinking and health risk behaviors among high school students. Pediatrics, 119, 76–85. doi:10.1542/peds.2006-1517.
Mischel, W., Shoda, Y., & Rodriguez, M. L. (1989). Delay of gratification in children. Science, 244, 933–938.
Moriya, J., & Tanno, Y. (2008). Relationships between negative emotionality and attentional control in effortful control. Personality and Individual Differences, 44, 1348–1355. doi:10.1016/j.paid.2007.12.003.
Murray, K. T., & Kochanska, G. (2002). Effortful control: Factor structure and relation to externalizing and internalizing behaviors. Journal of Abnormal Child Psychology, 30, 503–514.
Muthén, B. O. (2005). Retrieved from http://www.statmodel.com/discussion/messages/14/738.html?1130249370.
Muthén, L. K., & Muthén, B. O. (1998–2012). Mplus user’s guide (7th ed.). Los Angeles, CA: Muthén & Muthén.
Nagin, D. S. (2005). Group-based modelling of development. Cambridge: Harvard Press.
Needham, B. L. (2007). Gender differences in trajectories of depressive symptomatology and substance use during the transition from adolescence to young adulthood. Social Science and Medicine, 65, 1166–1179.
Nylund, K. L., Asparouohov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A monte carlo simulation study. Structural Equation Modeling, 14, 535–569.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Radloff, L. S. (1991). The use of the Center for Epidemiological Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence, 20, 149–166.
Rohde, P., Beevers, C. G., Stice, E., & O’Neil, K. (2009). Major and minor depression in female adolescents: Onset, course, symptom presentation, and demographic associations. Journal of Clinical Psychology, 65, 1339–1349. doi:10.1002/jclp.20629.
Rohde, P., Lewinsohn, P. M., Klein, D. N., Seeley, J. R., & Gau, J. M. (2013). Key characteristics of major depressive disorder occurring in childhood, adolescence, emerging adulthood, and adulthood. Clinical Psychological Science, 1(41), 53. doi:10.1177/2167702612457599.
Rohde, P., Lewinsohn, P. M., & Seeley, J. R. (1996). Psychiatric comorbidity with problematic alcohol use in high school students. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 101–109. doi:10.1097/00004583-199601000-00018.
Rothbart, M. K., & Bates, J. E. (2006). Temperament. In N. Eisenberg & W. Damon (Eds.), Handbook of child psychology: vol 3. Social, emotional, and personality development (6th ed., pp. 99–166). NY: Wiley.
Ruchkin, V., Sukhodolsky, D. G., Vermeiren, R., Koposov, R. A., & Schwab-Stone, M. (2006). Depressive symptoms and associated psychopathology in urban adolescents: A cross-cultural study of 3 countries. The Journal of Nervous and Mental Disease, 194, 106–113. doi:10.1097/01.nmd.0000198142.26754.18.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7, 147–177. doi:10.1037/1082-989X.7.2.147.
Simons, J. S., & Carey, K. B. (2002). Risk and vulnerability for marijuana use problems: The role of affect dysregulation. Psychology of Addictive Behaviors, 16, 72–75. doi:10.1037/0893-164X.16.1.72.
Smoski, M. J., Felder, J., Bizzell, J., Green, S. R., Ernst, M., Lynch, T. R., et al. (2009). fMRI of alterations in reward selection, anticipation, and feedback in major depressive disorder. Journal of Affective Disorders, 118, 69–78. doi:10.1016/j.jad.2009.01.034.
Spear, J. P. (2000). The adolescent brain and age-related behavioral manifestations. Neuroscience and Biobehavioral Reviews, 24, 417–463. doi:10.1016/S0149-7634(00)00014-2.
Statistics Canada. (2006). Population by ethnic origin [Online]. Available at http://www12.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/demo26a-eng.htm.
Steinberg, L. (2010). A dual systems model of adolescent risk-taking. Developmental Psychobiology, 52, 216–224. doi:10.1002/dev.20445.
Steinberg, L., Albert, L., Cauffman, E., Banich, M., Graham, S., & Woolard, J. (2008). Age differences in sensation seeking and impulsivity as indexed by behavior and self-report: Evidence for a dual systems model. Developmental Psychology, 44(6), 1764–1778. doi:10.1037/a0012955.
Swendsen, J. D., & Merikangas, K. R. (2000). The comorbidity of depression and substance use disorders. Clinical Psychology Review, 20, 173–189. doi:10.1016/S0272-7358(99)00026-4.
Tice, D. M., Bratslavsky, E., & Baumeister, R. F. (2001). Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! Journal of Personality and Social Psychology, 80, 53–67. doi:10.1037/0022-3514.80.1.53.
Van Dam, N. T., & Earleywine, M. (2011). Validation of the Center for Epidemiologic Studies Depression Scale-Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Research, 186, 128–132. doi:10.1016/j.psychres.2010.08.018.
Verstraeten, K., Vasey, M., Raes, F., & Bijttebier, P. (2009). Temperament and risk for depressive symptoms in adolescence: Mediation by rumination and moderation by effortful control. Journal of Abnormal Child Psychology, 37, 349–361. doi:10.1007/s10802-008-9293-x.
Wang, M. T., Brinkworth, M., & Eccles, J. (2012). Moderating effects of teacher–student relationship in adolescent trajectories of emotional and behavioral adjustment. Developmental Psychology,. doi:10.1037/a0027916.
Willoughby, T., Chalmers, H., & Busseri, M. (2004). Where is the syndrome? Examining co-occurrence among multiple problem behaviors in adolescence. Journal of Consulting and Clinical Psychology, 72, 1022–1037.
Wills, T. A., Cleary, S., Filer, M., Shinar, O., Mariani, J., & Spera, K. (2001). Temperament related to early-onset substance use: Test of a developmental model. Prevention Science, 2, 145–163. doi:10.1023/A:1011558807062.
Wills, T. A., & Stoolmiller, M. (2002). The role of self-control in early escalation of substance use: A time-varying analysis. Journal of Consulting and Clinical Psychology, 70, 986–997. doi:10.1037/0022-006X.70.4.986.
Wills, T. A., Windle, M., & Cleary, S. D. (1998). Temperament and novelty seeking in adolescent substance use: Convergence of dimensions of temperament with constructs from Cloninger’s theory. Journal of Personality and Social Psychology, 74, 387–406.
Wilson, A. C., Lengua, L. J., Tininenko, J., Taylor, A., & Trancik, A. (2009). Physiological profiles during delay of gratification: Associations with emotionality, self-regulation, and adjustment problems. Journal of Applied Developmental Psychology, 30, 780–790. doi:10.1016/j.appdev.2009.05.002.
Windle, M., & Davies, P. T. (1999). Depression and heavy alcohol use among adolescents: Concurrent and prospective relations. Development and Psychopathology, 11, 823–844.
Windle, M., & Lerner, R. M. (1986). Reassessing the dimensions of temperamental individuality across the life span: The Revised Dimensions of Temperament Survey (DOTS-R). Journal of Adolescent Research, 1(2), 213–230.
Windle, M., Spear, L. P., Fuligni, A. J., Angold, A., Brown, J. D., Pine, D., et al. (2008). Transitions into underage and problem drinking: Summary of developmental processes and mechanisms: Ages 10–15. Pediatrics, 121, S273–S289. doi:10.1542/peds.2007-2243C.
Acknowledgments
Funding for this longitudinal project was provided by the Social Sciences and Humanities Research Council of Canada to Teena Willoughby.
Author contributions
T.W conceived of the study, participated in the design and coordination of the study, performed the statistical analyses, collected the data, and participated in the drafting of the manuscript; A.F participated in the design, performed the statistical analyses, and participated in the drafting of the manuscript. Both authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Willoughby, T., Fortner, A. At-Risk Depressive Symptoms and Alcohol Use Trajectories in Adolescence: A Person-Centred Analysis of Co-Occurrence. J Youth Adolescence 44, 793–805 (2015). https://doi.org/10.1007/s10964-014-0106-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-014-0106-y