
Abstract
The transition to middle school can be a significant stressor for young adolescents, leading to increases in depression for those who are vulnerable. The current study examined how perceived support from mothers, fathers, and teachers independently and interactively predicted developmental patterns of depressive symptoms during adolescents’ transition to middle school, and gender differences in these effects of social support. Four timepoints of data were collected from 1,163 participants (48.5 % boys) enrolled in an ethnically diverse suburban middle school in the Midwest between 1.25 and 20.50 months after these participants entered the 7th grade. The results from growth curve modeling indicated that levels of depressive symptoms decreased over time for boys but remained stable for girls during the developmental period examined. There is also evidence that support from mothers, fathers, and teachers independently and inversely predicted levels of depressive symptoms at the beginning of the 7th grade, and support from both mothers and fathers predicted changes in these symptoms. Effects of mothers’ support and teachers’ support, but not the effect of fathers’ support, remained significant in reducing levels of depressive symptoms at 20.50 months from middle school entry. Furthermore, the protective effect of mothers’ support was stronger for girls than for boys. Finally, mothers’ support interacted with fathers’ support and teachers’ support to predict levels of depressive symptoms. Specifically, the protective effect of mothers’ support was more salient when fathers’ support was low, and vice versa. In contrast, support from mothers and teachers had an amplifying, synergistic effect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Early adolescence marks a time of increased emotional turmoil associated with stress related to the many changes during this developmental period. One significant stressor in early adolescence is the transition to a new school environment. In particular, the transition to middle school is related to many negative outcomes for youth, including lower self-efficacy, academic motivation and achievement (Eccles et al. 1993; Ryan and Patrick 2001), and greater internalizing difficulties (Roeser et al. 1998). In addition, early adolescence is a time period during which depressive symptoms begin to show gender differences (Ge et al. 2001; Hankin and Abramson 2001), with girls experiencing higher levels of depressive symptoms than boys (Ge et al. 1994; Hankin et al. 1998; Kessler et al. 1993). At a time when students are moving into a new school, the structure of the school environment changes and relationships with teachers often change, with an increase in number of teachers and higher demands and expectations of autonomy for students (Eccles et al. 1991; 1993a, b). These changes in the school environment coupled with the onset of puberty and associated emotional and academic strife could lead to significant challenges in adjustment during this developmental period. Identifying protective factors that may prevent the development of depressive symptoms during this difficult transition, as well as understanding potential gender differences, will be vitally important to guide prevention efforts.
Social support from parents has been found to be an important protective factor in the development of depression (e.g., Meadows et al. 2006; Stice et al. 2004; Young et al. 2005). Although youth seemingly want to rely less on parents for support, support from parents has been clearly documented as having continued importance in the lives of young adolescents (Levitt et al. 1993). In addition, the literature supports the positive impact of teachers on young adolescents, not only on their academic adjustment (Malecki and Demaray 2003; Wigfield et al. 2006) but also on social-emotional adjustment (De Wit et al. 2011; Reddy et al. 2003). Further, researchers are increasingly considering the effects of multiple sources of support to understand the independent effects of support from mothers, fathers, and teachers (Jia et al. 2009; Rueger et al. 2010); however, less is known about the interactive effects of these adult sources of support. Bronfenbrenner’s theory of human development (1979) emphasizes the importance of the immediate environment in the life of a youth, and the interaction between different environments. As such, this theory highlights the importance of testing adolescents’ experiences in different contexts, such as home and school, and the ways in which the effects of support from various sources interact to offer protection. Finally, gender differences in the effects of social support on depressive symptoms have been mixed, with some studies demonstrating support for differences across gender (e.g., Colarossi and Eccles 2003) and others demonstrating consistency across gender (e.g., Jia et al. 2009). Thus, a closer investigation of the independent and interactive protective effects of support from mothers, fathers, and teachers throughout the middle school years and gender differences in these effects would add to the literature, and inform intervention efforts at a time of unique vulnerability.
Social Support as a Protective Factor to Depression
Social Support from Parents
Research is unequivocal in demonstrating that parents continue to play an important role in this developmental time period. An inverse association between support from parents and depressive symptoms during adolescence has been consistently supported, both concurrently (Helsen et al. 2000; Patten et al. 1997) and longitudinally (Colarossi and Eccles 2003; Patten et al. 1997; Rueger et al. 2010). There is also evidence that lower levels of parental support predict the onset of a major depressive episode (Stice et al. 2004; Young et al. 2005). Investigations of trajectories of depression over multiple timepoints (Costello et al. 2008; Needham 2008; Meadows et al. 2006) are consistent with longitudinal studies using only two timepoints in demonstrating the protective effects of supportive parents on depressive symptoms over time. For example, in a large representative epidemiological study, support from both mothers and fathers was found to predict initial levels and decreases in depressive symptoms over a seven-year period (Needham 2008).
Further, there has been growing interest in the social support literature on the independent contributions made by mothers and fathers; however, results from these studies seem to be mixed. Some evidence suggests that support from both mothers and fathers is important in reducing levels of depressive symptoms during adolescence (Meadows et al. 2006; Niemiec et al. 2006), whereas others indicate that support from mothers might be more strongly related to their children’s internalizing behavior compared to support from fathers (Colarossi and Eccles 2003; Ge et al. 1994). More longitudinal research comparing the effects of support from mothers and fathers on both levels of and developmental changes in depressive symptoms is needed to gain a more nuanced understanding of the important role that parents continue to play in this developmental period.
Social Support from Teachers
In addition to the considerable study on support from parents and the home environment, researchers have increasingly begun to investigate the role of social support in other important contexts, such as the school (e.g., Blum et al. 2002), to have a better understanding of youth depression. This research has confirmed that support from non-familial sources takes on growing importance during adolescence. For example, a study focused on non-familial adult support sources demonstrated that a majority of adolescents in the U.S. report having a non-parental adult, such as teachers, in their lives (Chen et al. 2003). Ninety percent of those teens deemed these adults as important sources of support, with one-third of these teens indicating these non-familial sources as “truly key person[s].”
Perceived support from teachers has been inversely associated with depressive symptoms, both cross-sectionally (Jia et al. 2009) and longitudinally (Colarossi and Eccles 2003; Roeser et al. 1998). However, there is limited information on the effect of teacher social support on changes in depressive symptoms over multiple timepoints. In one of the few studies focused on effects of teachers’ support on depressive symptoms over time, Reddy et al. (2003) found that support from teachers in 6th grade predicted depressive symptoms in 6th grade, but did not predict change in depressive symptoms from 6th to 8th grade. Another study of early adolescents similarly found that support from teachers in 9th grade did not predict change in depressive symptoms from 9th to 10th grade (De Wit et al. 2011). More work is needed to elucidate the impact that teachers’ support can have in the lives of early adolescents over time.
Independent and Interactive Effects of Parental and Teachers’ Support
An important set of questions to address is whether support from mothers, fathers, and teachers have additive benefits to young adolescents, or whether there is an interactive relationship among these sources of support. The unique effect of support from parents above and beyond the effects of support from teachers has been consistently demonstrated in the literature (Colarossi and Eccles 2003; Jia et al. 2009; Rueger and Malecki 2011). However, it is not clear if the same is true for teachers’ support. Some research suggests that support from teachers offers protection above and beyond the effects of support from parents (Colarossi and Eccles 2003; Jia et al. 2009) but other research has failed to demonstrate independent effects of teachers’ support as a protective factor (Ezzell et al. 2000; Rueger et al. 2010).
It is possible that a consideration of the interactive relationship between support from parents and teachers may help explain these inconsistent results. Studies have demonstrated that the caring support of even one non-familial adult, including teachers, can be protective when support from parents is lacking. For example, a cross-sectional study of 5th through 11th graders demonstrated that teachers’ support was associated with fewer depressive symptoms when parental support was low, but not when parent support was high (Conners-Burrow et al. 2009). Similarly, a long-term follow-up from childhood into adulthood of 65 offspring of alcoholics demonstrated that the high-risk individuals who were able to overcome the childhood adversities of being raised in an alcoholic family experienced higher levels of support from other adult sources compared to those who experienced coping problems (Werner and Johnson 2004). Thus, it is likely that the lack of consideration of the interaction effects between support from parents and other adult sources, such as teachers, might lead to inconsistent findings across studies. Therefore, it is important to continue to focus on and compare the interactive as well as independent effects of support from mothers and fathers with teachers, especially over multiple timepoints, to have a better understanding of the role that significant familial and non-familial adults continue to play in the lives of early adolescents.
Gender Differences in Effects of Social Support
It has been well-documented that girls experience higher levels of depressive symptoms than do boys during adolescence (Hankin and Abramson 2001; Kessler et al. 1993). The onset of this gender difference in the level of depressive symptoms occurs during early adolescence (Ge et al. 2001; Hankin et al. 1998), and the difference is maintained through adulthood (Kessler et al. 1993). In addition, research suggests that there are gender differences in the ways in which youth use social support as a coping strategy: girls are more likely than boys to seek out support (Frydenberg and Lewis 1991, 1993).
Interestingly, there are more consistencies than differences in perceptions of social support from adult sources, such as parents (Demaray and Malecki 2002; Rueger et al. 2010) and teachers (Rueger et al. 2008). The same is true for gender differences in the effects of support on depressive symptoms: Support from parents and teachers have been demonstrated as protective for both boys and girls. More specifically, support from mothers, fathers, and teachers were all uniquely associated with depressive symptoms in a cross-sectional analysis of a large sample of middle school students in the U.S. and China, and no gender differences were demonstrated (Jia et al. 2009). Consistency across gender was also demonstrated, in both concurrent and longitudinal relationships between parental support and depressive symptoms in early adolescence (Rueger et al. 2010). This pattern of findings suggests that socialization factors may influence how boys and girls interact socially and utilize social resources in different ways, but that young adolescent boys and girls have the same basic social needs. However, this conclusion has yet to be confirmed in longitudinal studies examining gender differences in the effects of social support on developmental trajectories of depressive symptoms, which requires the use of multiple timepoints of data.
Research with older adolescents similarly demonstrates consistency across gender to the effects of support, but there are some notable gender differences. While research continues to show that boys and girls benefit from mothers’ support (Colarossi and Eccles 2003; Niemiec et al. 2006; Piko et al. 2009) and teachers’ support (Colarossi and Eccles 2003; De Wit et al. 2011; Reddy et al. 2003) in mid to late adolescence, several studies have highlighted the particular importance that mothers may play in adolescent girls’ well-being. Some studies demonstrate stronger (Colarossi and Eccles 2003; Meadows et al. 2006) or more widespread positive effects (Niemiec et al. 2006) of support from mothers for daughters than for sons, whereas other studies document significant effects only between mothers and daughters (Ge et al. 1994). On the other hand, there is also evidence that fathers’ support may be more influential for boys than girls (Colarossi and Eccles 2003; Piko et al. 2009) in this later age range. Combined, these results highlight the potential for each of the three adult sources to have a unique influence on the well-being of adolescents, especially among same-sex parent–child pairs. It is possible that some of these gender differences are operative only in later adolescence; alternatively, it is possible that these differences begin to develop earlier in adolescence. More work considering possible gender differences in future studies focused on social support and depression in early adolescence would help to bring clarity to this issue.
Current Investigation
The literature clearly supports the continued importance of perceived support from parents and teachers in early adolescence. However, a lack of research on the unique or interactive effects of support from these adult sources, especially over multiple timepoints, limits interpretation and application of previous findings to intervention efforts. In addition, although previous research suggests that there are more similarities than differences across gender in the effects of social support on levels of depression, limited studies have considered gender differences in the longitudinal effects of social support on developmental trajectories of depression. Further, research highlights the growing importance of same-sex parent–child pairs in late adolescence, but little work has been done to explore these questions in early adolescence. Thus, the current investigation aims to add to the literature by using multiple timepoints of data to examine the independent and interactive effects of social support from mothers, fathers, and teachers in predicting developmental patterns of depressive symptoms during the middle school years, and gender differences in these effects of social support.
Three research questions guided the investigation. The first question addressed the unique effects of support from significant adult sources: Does social support from mothers, fathers, and teachers independently predict levels of and changes in depressive symptoms during the transition to middle school? The second question addressed potential gender differences in these effects: Do the effects of social support from mothers, fathers, and teachers on levels of and changes in depressive symptoms differ for boys and girls? The third question addressed potential interactive relationships between the three adult sources of support: Does social support from mothers, fathers, and teachers interact with each other to predict levels of and changes in depressive symptoms? Addressing these empirical questions will bring clarity to inconsistencies in the literature, and add to our understanding of the protective role that social support from adult sources continue to play through the transition to middle school.
Methods
Participants and Procedures
Four waves of data were collected for two separate studies across two consecutive school years from 2005 to 2007 at a racially/ethnically and socioeconomically diverse suburban middle school in the Midwest consisting of 7th and 8th graders (age ranging from 12 to 15 across the study). In the 2005–2006 school year, enrollment was 859 students, with 40 % of the students reporting a non-Caucasian ethnicity/race, and 24 % students meeting criteria for low income status, which includes families receiving public aid, children in foster homes with public funds, and families eligible to receive free or reduced-price lunches. In addition, there was a 10 % mobility rate and .2 % chronic truancy rate during that school year.
The first two waves of data were collected as part of a study that occurred during the 2005–2006 school year (Rueger et al. 2010). The first wave of data was collected in the fall, approximately 1 month into the school year (N = 801), and the second wave of data was collected in the spring, approximately 1 month from the end of the same school year (N = 759). Data for the first study were collected as part of a school-wide assessment; thus, in accordance with school district policy, parents were notified of the assessment and were given the option to withdraw their child from participating in the assessment. One parent asked that their child do not participate in the assessment. Once the school-wide assessment was complete, the researchers obtained Institutional Review Board approval to use the extant data for research purposes.
The third and fourth waves of data were collected as part of another study that occurred during the 2006–2007 school year (Rueger and Malecki 2011). The third wave of data was collected approximately 1 month after winter break the following school year (N = 529), and the fourth wave of data was collected approximately 1 month from the end of the same school year (N = 528). Data for the second study were collected after all procedures were approved by the Institutional Review Board and parental consent and student assent were collected. Across all four waves of data collection, participants completed self-administered surveys in multi-class groups in the school cafeteria.
A total of N = 1,163 youth participated in the four waves of data collection described above. The final sample was evenly distributed in gender (51.6 % male) and was racially/ethnically diverse, with 53.5 % non-Hispanic Caucasian, 28.1 % Hispanic, 5.6 % African American, 5.6 % Asian American, and 2.3 % Other (e.g., Native American). During the 2005–2006 school-wide assessment, 20 % of the students in the sample reported that their family met the requirements for low-income status, which aligns with the 24 % low income rate based on the school-wide data.
Our analytical sample included N = 1,119 participants who provided reports for measures of depressive symptoms and social support in at least one of the four waves of the study and who had no missing data in gender and race/ethnicity. A major advantage of the statistical model used in the present study (i.e., the multilevel model for change) is that participants can be included in analyses as long as they have complete data in at least one of the four waves of the study. Specifically, under the framework of multilevel modeling, incomplete data are analyzed using the maximum likelihood method to provide unbiased parameter estimates. There is evidence that this estimation method of multilevel analysis handles incomplete data more efficiently than imputation methods (Twisk 2006; Twisk and de Vente 2002). Participants who had missing data in study constructs across all four waves (N = 44; <4 % of the total sample) were handled using listwise deletion as multilevel modeling is unable to incorporate them in analyses. Data for these participants were not imputed, as multiple imputations offer little advantage when the proportion of missing data is <10 % (Cummings 2013).
Of the participants included in the final sample, 16 % provided only one wave of data, 63 % provided data across only two waves of the data, and 21 % had three or more waves of data. Because of its flexible treatment of the time predictor, the multilevel model for change can effectively accommodate such unbalanced data (i.e., data with varying numbers of waves across participants) without sacrificing the accuracy of the fixed effect estimation (Singer and Willett 2003). To examine whether patterns of depressive symptoms vary systematically across participants with different waves of data, a multilevel model was fitted with depressive symptoms as the dependent variable and the waves of data contributed by each participant as the predictor. Findings indicated that participants with one (b = .511, p < .001) or two (b = .207, p < .01) wave of data reported higher levels of depressive symptoms than participants with three or more waves of data. Although differences in levels of depressive symptoms were observed, we note that the multilevel model for change enables us to control for between-individual differences in patterns of depressive symptoms (please see the Plan of Analysis section for further details), so that these differences will not bias the estimation of the fixed effects.
Measures
Gender, Race, and Ethnicity
Gender was coded as 0 = male and 1 = female for analyses. To control for race, dummy-coded variables were developed for Hispanic, African American, Asian American, and other race, using non-Hispanic Caucasian as the reference or comparison group.
Time from Middle School Entry
Time from middle school entry when participants were surveyed were coded as the number of months after adolescents entered 7th grade. Across the four waves of the study, participants provided data at 1.25, 5.00, 8.50, 13.25, 17.00, and 20.50 months from middle school entry.
Depressive Symptoms
Adolescent depressive symptoms were assessed with the Depression subscale of the Behavior Assessment System for Children—Self Report of Personality, Second Edition (BASC-2 SRP; Reynolds and Kamphaus 2004), which is a self-report rating scale that measures the personality and self-perceptions of students ages 12–21. There are two types of questions in the scale. Ten items require a True or False response (e.g., “I don’t seem to do anything right”), while four items are rated on a 4-point frequency scale, ranging from “0 = Never” to “3 = Almost Always” (e.g., “I feel depressed”). Raw scores were summed and converted to a T-score using the BASC-2 scoring software. The internal consistency for the depression subscale ranged from .87 to .88 across the four waves of the study. The final scores of depressive symptoms were slightly skewed and were transformed using a square root transformation prior to analysis.
Perceived Social Support
Perceived levels of support from mothers, fathers, and teachers were assessed using the Teacher subscale and a modified Parent subscale from the Child and Adolescent Social Support Scale (CASSS; Malecki et al. 2003). Specifically, youth were asked to rate 12 items assessing levels of social support from teachers (e.g., “my teacher(s) care about me”), and another 12 items assessing levels of support from parents, with separate ratings for mothers and fathers (e.g., “my mother/father listens to me when I need to talk”; “my mother/father makes suggestions when I don’t know what to do”). Responses were given on a 6-point frequency scale ranging from “1 = Never” to “6 = Always.” Scores for support from these three sources were created by summing the frequency ratings, with possible scores ranging from 6 to 72 for each subscale. The internal consistency of the Mother (αs ranged from .93 to .94), Father (αs ranged from .94 to .96), and Teacher (αs ranged from .90 to .94) subscales was excellent across the four waves of the study. Measures of social support were significantly and positively correlated across the four waves of the study, with the correlations between the Mother and Father subscales (rs ranged from .52 to .57) being stronger than the correlations between the Mother and Father subscales with the Teacher subscale (rs ranged from .27 to .39).
Plan of Analysis
The multilevel model for change, namely growth curve modeling (Singer and Willett 2003), was used to examine the research questions of the present study. A total of five hierarchical models predicting depressive symptoms were tested using SPSS. Three models were tested in initial analyses to set up the baseline model for examining effects of social support on developmental trajectories of depressive symptoms and gender differences in these effects. Model 1 is an unconditional means model examining significance of between-individual and within-individual variance of depressive symptoms. Model 2, the unconditional growth model, estimated the initial level and the linear change of depressive symptoms. Specifically, time from middle school entry was used as the time variable whose effect indicates the rate of change of depressive symptoms over time. Equation 1 summarizes analyses conducted in Model 2:
where i represents the 1,119 participants, j represents the six timepoints assessed (1.25, 5.00, 8.50, 13.25, 17.00, and 20.50 months from middle school entry), and the components in the bracket are raw residuals associated with the within-individual differences between the predicted and observed values of depressive symptoms (εij) and the between-individual variability in the initial level (ζ0i) and the rate of change (ζ1i) of depressive symptoms with variances equal to σ 2ε , σ 20 , σ 21 respectively. The time variable was centered at 1.25 months so that the intercept coefficient (γ00) indicates adolescents’ levels of depressive symptoms at 1.25 months from entry into middle school, and the coefficient/effect of the time variable (γ10) describes the rate of change of these symptoms between 1.25 and 20.50 months from entry into middle school.
Model 3 considering gender differences in the initial level and the rate of change of depressive symptoms controlling for race/ethnicity is expressed in Eq. 2:
The main effect of gender in the model (γ05) tests gender differences in the initial level of depressive symptoms, whereas the interaction effect of gender and the time variable (γ11) examines gender differences in the rate of change of these symptoms (i.e., the moderating effect of gender on the effect of the time variable). As both variables included in the interaction term can be treated as the moderator, the gender by time interaction can also be interpreted as changes in gender differences in levels of depressive symptoms over time (i.e., the moderating effect of the time variable on the effect of gender). Interaction terms between race/ethnicity and the time variable were not included in Model 3 as they were not significant. As four waves of data were available for the present study, we also tested the significance of the quadratic change of depressive symptoms. Analyses examining the quadratic function of the time variable (i.e., Time2) as well as the interaction between gender and the quadratic function of the time variable provided no evidence supporting the curvilinear change of depressive symptoms. Therefore, Model 3 was used as the baseline model for subsequent analyses.
In the next step, to address the first research question, the longitudinal effects of mothers’ support, fathers’ support, and teachers’ support on depressive symptoms controlling for the effects of race/ethnicity and gender were examined simultaneously, and the significant effects revealed in this analysis were reported in Model 4 which is expressed in Eq. 3:
The interaction between teachers’ support and the time variable was not significant and therefore was excluded from the model. Similar to the test of gender effects, the main effects of social support in the model reveal the effects of social support on the initial level of depressive symptoms, whereas the interaction effects between social support and the time variable address the effects of social support on the rate of change of depressive symptoms (i.e., the moderating effects of social support on the effect of the time variable) as well as changes in effects of social support on levels of depressive symptoms over time (i.e., the moderating effects of the time variable on the effects of social support).
Lastly, to address the 2nd and 3rd research questions, the interaction effects between gender and measures of social support as well as the interaction effects among measures of social support were explored. None of the examined interaction effects on the rate of change of depressive symptoms were significant. Gender interacted with mothers’ support, but not fathers’ and teachers’ support, to predict levels of depressive symptoms. In addition, the interaction effects between mothers’ support with teachers’ support and fathers’ support, but not the interaction effect between teachers’ support and fathers’ support, on levels of depressive symptoms were statistically significant. Finally, the three-way interaction between gender, mothers’ support, and fathers’ support as well as the three-way interaction between gender, mothers’ support, and teachers’ support on levels of depressive symptoms were not significant, indicating that the interactions effects between mothers’ support with fathers’ support and teachers’ support on levels of depressive symptoms did not differ for boys and girls. A final mode (Model 5) reported the significant interactions revealed in these analyses along with all effects examined in Model 4. The final model is expressed in Eq. 4:
For all analyses, standardized scores of depressive symptoms and measures of social support were used so that standardized regression coefficients could be reported for effects of social support. Therefore, measures of social support were also centered at their grand mean (means of scale scores across all four timepoints) in analysis. The variance of depressive symptoms explained by each model was calculated using a Pseudo-R 2. The models were compared using Δχ 2 tests. In addition, using the regression coefficients, degrees of freedom, and covariance statistics retrieved from SPSS outputs, follow-up analyses (e.g., significant region tests, regression coefficients of the focal variables at the conditional values of the moderators) explored significant interactions with the assistance of an online computational utility developed for interpreting interaction effects under the framework of multilevel modeling (Preacher et al. 2006).
Results
Preliminary Analyses
The descriptive statistics on the main study constructs (depressive symptoms, and support from mothers, fathers, and teachers) are reported in Table 1 and the correlation statistics between depressive symptoms and social support for each timepoint are reported in Table 2. The correlation statistics provided evidence for statistically significant negative relationships between depressive symptoms and all measures of social support in the total sample. Using Steiger’s Z test, we found that the correlation between mothers’ support and depressive symptoms was significantly stronger than the correlation between fathers’ support and depressive symptoms at 1.25, 8.5, and 13.25 months from middle school entry; mothers’ support was also more strongly correlated with depressive symptoms than was teachers’ support at 1.25, 5, 8.5, and 13.25 months from middle school entry. Gender differences in the reported correlations were explored using Fisher’s Z test. The correlation between mothers’ support and depressive symptoms was stronger for females than for males at 5, 8.5, and 17 months from middle school entry. In addition, support from teachers and fathers were more strongly correlated with depressive symptoms for females than for males at 5 and 17 months from middle school entry, respectively.
Growth Curve Modeling Analyses
Unconditional Model (Model 1)
Variance components of the unconditional model (Model 1; χ2 = 6,383.539) revealed statistically significant within-individual (σ 2ε = .383, p < .001) and between-individual (σ 20 = .673, p < .001) variability in measures of depressive symptoms. The intra-class correlation coefficient indicated that 64 % of the variance in these symptoms existed between individuals, and the remaining variance was due to within-individual differences.
Unconditional Growth Curve Model (Model 2) and Gender Differences Model (Model 3)
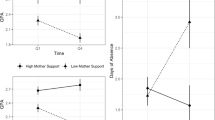
Parameter estimates from Model 2 (χ2 = 6,369.391; Δχ2 = 14.148, Δdf = 3, p < .01; Persudo R2 within person = 7.6 %) indicated that changes in depressive symptoms between 1.25 and 20.50 months from middle school entry were not statistically significant in the total sample (γ10 = −.004, p = ns). In the next step, we tested gender differences in the initial level and the rate of change of depressive symptoms (Model 3) controlling for race/ethnicity. The results from these analyses are reported in Table 3. The findings from Model 3 indicated that Hispanic (γ02 = .243, p < .001) and Asian (γ03 = .220, p < .05) youth as well as youth with Other (γ04 = .367, p < .05) racial/ethnic backgrounds reported higher levels of depressive symptoms than their Caucasian counterparts, whereas levels of these symptoms did not differ significantly between African American and Caucasian youth (γ01 = .166, p = ns). Racial/ethnic differences in the rate of change of depressive symptoms were not statistically significant, and therefore were not included in Model 3. The most noteworthy finding of Model 3 is that boys and girls did not differ in their initial levels of depressive symptoms (γ05 = .013, p = ns), but they did differ in the rate of change of these symptoms as indicated by the significant interaction between gender and the time variable (γ11 = .019, p < .001). Developmental trajectories of depressive symptoms by gender are plotted in Fig. 1a. Levels of depressive symptoms decreased significantly over time for boys (γrate of change = −.014, p < .001) but remained stable for girls (γrate of change = .005, p = ns). The significant interaction between gender and the time variable also implied that the time variable moderated the effect of gender on levels of depressive symptoms. In other words, gender differences in levels of depressive symptoms changed over the time period examined. The significant region tests revealed that gender differences in levels of depressive symptoms became significant between 6 and 7 months from entry into middle school, after which girls consistently exhibited significantly higher levels of depressive symptoms than boys as shown in Fig. 1a.

Prototypical plots for developmental trajectories of depressive symptoms by gender and levels of social support: a gender differences, b mother support, c father support, and d teacher support
Effects of Each Source of Social Support (Model 4)
The first research question (Does social support from mothers, fathers, and teachers independently predict levels of and changes in depressive symptoms during the transition to middle school?) was addressed in the next step: the effects of support from mothers, fathers, and teachers on the initial level and the rate of change of depressive symptoms were examined simultaneously, controlling for the effects of race/ethnicity and gender. The significant effects revealed in the analysis are reported in Model 4 (see Table 3). Controlling for social support from other adult sources examined, all three measures of social support predicted the initial level of depressive symptoms (γ06 = −.278, p < .001; γ07 = −.140, p < .001; γ08 = −.074, p < .001). In addition, the significant interactions between mothers’ support and fathers’ support with the time variable indicated that both mothers’ support (γ12 = .006, p < .05) and fathers’ support (γ13 = .005, p < .05) predicted the rate of change of depressive symptoms. The regression coefficients of each measure of social support were compared using t statistics computed using the equation: t = (γvariable 1-γ variable 2)/SE(γvariable 1-γ variable 2), where SE(γvariable 1-γ variable 2) = SQRT[Var(γvariable 1) + Var(γ variable 2)-2*Cov(γvariable 1, γ variable 2)] (DeMaris 2004). The effect of mothers’ support on the initial level of depressive symptoms was stronger than those of fathers’ support (t[2,464] = 2.09, p < .05) and teachers’ support (t[2,464] = 4.45, p < .001), whereas the latter two effects did not differ significantly from each other. In addition, no significant differences were found between the effects of mothers’ support and fathers’ support on the rate of change of depressive symptoms.
Figure 1b, c exhibit the prototypical plot for developmental trajectories of depressive symptoms at a high (−1 SD) and a low level (1 SD) of mothers’ support and fathers’ support, respectively. Adolescents reporting high levels of parental support showed lower levels of depressive symptoms at 1.25 months from middle school entry than those who reported low levels of parental support. Additional analyses examining the rate of change of depressive symptoms by levels of parental support indicated that levels of depressive symptoms decreased more rapidly over time for adolescents with low (low mothers’ support: γrate of change = −.026, p < .001; low fathers’ support: γrate of change = −.025, p < .001) versus high levels (high mothers’ support: γrate of change = −.014, p < .001; high fathers’ support: γrate of change = −.015, p < .001) of parental support. The significant interactions between mothers’ support and fathers’ support with the time variable also suggested that the effects of support from mothers and fathers on levels of depressive symptoms changed over time (i.e., the moderating effects of the time variable on the effects of mothers’ and fathers’ support). Analyses re-centering the time variable at the last timepoint of the study (i.e., 20.50 months from middle school entry) revealed that the effect of mothers’ support on levels of depressive symptoms remained significant at 20.50 months from middle school entry (γmothers’ support = −.167, p < .001), although its magnitude was smaller than the effect of mothers’ support on the initial level of depressive symptoms. In contrast, the effect of fathers’ support on the final level of depressive symptoms was no longer significant (γfathers’ support = −.027, p = ns). The significant region tests found that the effect of mothers’ support on levels of depressive symptoms remained significant across the time period studied; in contrast, the effect of fathers’ support on levels of these symptoms became non-significant between 16 and 17 months from middle school entry.
The longitudinal effects of teachers’ support on depressive symptoms were plotted in Fig. 1d following the same strategy described above. Higher levels of teachers’ support were consistently associated with lower levels of depressive symptoms during the time period studied. The effect of teachers’ support on the rate of change of depressive symptoms (i.e., the interaction effect between teachers’ support and the time variable) was not significant and therefore was excluded from Model 4. The lack of interaction between teachers’ support and the time variable also implied that the effect of teachers’ support on levels of depressive symptoms did not change across the time period examined (i.e., the time variable did not moderate the effect of teachers’ support).
Interaction Analyses (Model 5)
A final set of analyses examining the interaction effects between gender and measures of social support as well as the interaction effects among measures of social support addressed the second (Do the effects of social support from mothers, fathers, and teachers on depressive symptoms differ for boys and girls?) and third (Does social support from mothers, fathers, and teachers interact with each other to predict depressive symptoms) research questions. The results from these analyses revealed significant interaction effects between gender and mothers’ support, but not fathers’ or teachers’ support. In addition, results demonstrated significant interactions between mothers’ support and fathers’ support, and between mothers’ support and teachers’ support on levels of depressive symptoms. These interaction effects are reported in Model 5 (see Table 3).
Gender Differences in Effects of Mothers’ Support
The interaction effect between gender and mothers’ support reported in Model 5 suggested significant gender differences in the effect of support from mothers on levels of depressive symptoms (γ09 = −.135, p < .001). Follow-up analyses found that although mothers’ support was inversely associated with levels of depressive symptoms for both boys (1.25 months: γmothers’ support = −.195, p < .001; 5.00 months: γmothers’ support = −.181, p < .001; 8.50 months: γmothers’ support = −.167, p < .001; 13.25 months: γmothers’ support = −.150, p < .001; 17.00 months: γmothers’ support = −.136, p < .001; 20.50 months: γmothers’ support = −.122, p < .01) and girls (1.25 months: γmothers’ support = −.329, p < .001; 5.00 months: γmothers’ support = −.315, p < .001; 8.50 months: γmothers’ support = −.302, p < .001; 13.25 months: γmothers’ support = −.284, p < .001; 17.00 months: γmothers’ support = −.270, p < .001; 20.50 months: γmothers’ support = −.257, p < .001) across the time period examined, it consistently had a stronger protective effect for girls than for boys.
Interaction Effects of Mothers’ Support and Fathers’ Support
The interaction effect of mothers’ support and fathers’ support on levels of depressive symptoms (γ010 = .032, p < .05) was explored with follow-up analyses that estimated the regression coefficients of mothers’ support predicting levels of depressive symptoms at a low (−1 SD) and a high level (+ SD) of fathers’ support, as well as the regression coefficients of fathers’ support predicting levels of depressive symptoms at a low (−1 SD) and a high (+ SD) level of mothers’ support. Results indicated that the effects of support from mothers on both the initial level (at low levels of fathers’ support: γmothers’ support = −.226, p < .001; at high levels of fathers’ support: γmothers’ support = −.163, p < .001) and the final level of depressive symptoms (at low levels of fathers’ support: γmothers’ support = −.154, p < .05; at high levels of fathers’ support: γmothers’ support = −.091, p < .05) were stronger among youth reporting low versus high levels of fathers’ support. Similarly, the effect of support from fathers on the initial level of depressive symptoms (at low levels of mothers’ support: γfathers’ support = −.169, p < .001; at high levels of mothers’ support: γfathers’ support = −.106, p < .001) was stronger among youth reporting low versus high levels of mothers’ support. The effects of fathers’ support on the final level of depressive symptoms was not significant at both low and high levels of mothers’ support (at low levels of mothers’ support: γfathers’ support = −.047, p = ns; at high levels of mothers’ support: γfathers’ support = .017, p = ns).
Interaction Effects of Mothers’ Support and Teachers’ Support
The interaction effect of mothers’ support and teachers’ support (γ011 = −.053, p < .001) on levels of depressive symptoms was explored following the same strategy described above. The results indicated that support from mothers had a stronger effect on both the initial level (at low levels of teachers’ support: γmothers’ support = −.142, p < .001; at high levels of teachers’ support: γmothers’ support = −.247, p < .001) and the final level of depressive symptoms (at low levels of teachers’ support: γmothers’ support = −.070, p = ns; at high levels of teachers’ support: γmothers’ support = −.175, p < .001) for youth reporting high versus low levels of teachers’ support. On the other hand, the effect of support from teachers on levels of depressive symptoms was significant at high levels of mothers’ support (γteachers’ support = −.132, p < .001) but not at low levels of mothers’ support (γteachers’ support = −.027, p = ns). As the interaction between teachers’ support and the time variable was excluded from the Model 5, the regression coefficients of teachers’ support predicting levels of depressive symptoms at low and high levels of mothers’ support did not change across the developmental period examined.
Discussion
The goal of the current study was to extend the literature on the relationship between social support and depression by investigating the independent and interactive effects of support from important adult sources on depressive symptoms during the middle school years and gender differences in these effects. Consistent with the literature, the results from this study showed that girls and boys were at similar risk for depressive symptoms during the transition into middle school, but girls were at greater risk later in their middle school years. Although there were no significant differences in depressive symptoms between boys and girls at the beginning of 7th grade, boys’ depressive symptoms began to improve over the course of the middle school years, whereas girls’ symptoms remained stable. More specifically, gender differences in depressive symptoms began to emerge between 6 and 7 months after beginning 7th grade, after which girls consistently exhibited significantly higher levels of depressive symptoms than boys. The study also demonstrated the importance of support from mothers, fathers, and teachers as protective factors for both boys and girls as they transition into middle school. Perceived support from each of the three adult sources uniquely predicted levels of depressive symptoms above and beyond the effects of the other two sources as youth entered middle school. In addition, support from mothers and fathers uniquely predicted the rate of change of depressive symptoms over the two-year period. Finally, support from mothers was highlighted as particularly important in relation to support from fathers and teachers, and the protective effect of mothers’ support in reducing depressive symptoms was stronger for girls than for boys.
The findings demonstrating significant independent effects of both parents and teachers on depressive symptoms are consistent with previous research focused on early adolescents (Jia et al. 2009; Rueger et al. 2010) and mid to late adolescents (Colarossi and Eccles 2003). Further, support from mothers and fathers also predicted the rate of change of depressive symptoms. Although levels of depressive symptoms declined more rapidly for youth reporting lower levels of mothers’ support and fathers’ support, support from mothers was negatively associated with levels of these symptoms across the developmental period examined; support from fathers also had a protective effect on depressive symptoms during the first 16 months from middle school entry. On the other hand, our study is one of the first to demonstrate that the effects of mothers’ support and fathers’ support on levels of depressive symptoms reduced over time. Specifically, the effects of mothers’ support on levels of depressive symptoms were weaker at the end of the study in comparison to its effects on levels of depressive symptoms at the beginning of middle school entry; in addition, fathers’ support no longer predicted depressive symptoms after 16–17 mothers from middle school entry. This is consistent with patterns reported in the literature (e.g., Meadows et al. 2006), as adolescents’ social circle and circle of influence are growing. In spite of this, the effects of mothers’ support on levels of depressive symptoms remained significant at the end of middle school, although effects of fathers’ support became non-significant. Interestingly, while the effect of teachers’ support on initial levels of depressive symptoms was the weakest among the three sources of adult social support examined, it remained stable over time, and continued to predict lower levels of depressive symptoms at the end of middle school. Thus, by the end of middle school, both support from mothers and teachers continued to demonstrate unique protective effects. These results highlight the importance for future research to examine changes in effects of social support on depressive symptoms by using multiple timepoints of data.
The current study also demonstrated some significant interactions that are worth noting. First, although support from mothers was protective for both boys and girls, the interaction between gender and mothers’ support suggests that support from mothers is more strongly protective for girls. In addition, the interaction between mothers’ support and fathers’ support suggests that support from mothers is particularly important when there is a lack of fathers’ support, and support from fathers is particularly important when there is a lack of mothers’ support. Finally, the interaction between mothers’ support and teachers’ support suggests that support from mothers is more protective for those with higher levels of teachers’ support; similarly, effects of support from teachers may be protective only at high levels of mothers’ support.
The results from this study were consistent with the existing literature that demonstrates the important role played by both mothers and fathers in protecting their sons and daughters from increases in depressive symptoms during early adolescence (Jia et al. 2009; Needham 2008). In addition, results suggest that mothers might be more strongly related to their children’s well-being compared to support from fathers in early adolescence, as has been found in mid to late adolescence (Colarossi and Eccles 2003; Niemiec et al. 2006; Piko et al. 2009). Further, support from mothers was also found to be particularly important in this study in relation to teachers’ support as it served to amplify the effects of support from teachers. Finally, consistent with previous concurrent and longitudinal research (Jia et al. 2009; Rueger et al. 2010), there was more consistency across gender than differences in the relationship between social support and depressive symptoms over multiple timepoints in our study. Although there is evidence that girls benefitted more than boys from a supportive relationship with their mothers, mothers’ support was inversely related to levels of depressive symptoms for both boys and girls across the developmental period examined. Furthermore, the protective effects of fathers’ support and teachers’ support in reducing levels of depressive symptoms did not differ for boys and girls. Being one of the first longitudinal studies considering gender differences in effects of social support on depressive symptoms across multiple timepoints, our results provide strong evidence in support of the growing literature that demonstrates a similar basic need for social resources across gender in spite of differences in how boys and girls interact socially.
Also consistent with previous research, the current study demonstrated growing gender differences in levels of depressive symptoms during the middle school years. Interestingly, the gender differences demonstrated in the current study resulted from boys’ decrease in depressive symptoms rather than girls’ increase in depressive symptoms. These findings suggest that boys may have more easily adjusted to the new school environment, with an accompanying improvement in depressive symptoms over time. It is possible that boys may be better able to “bounce back” from the stress of the transition to middle school more so than girls. If there are differences in how boys and girls adjust to middle school, it will also be important for teachers and school personnel to be aware of these differences. Particularly relevant to schools is the finding that the effect of teachers’ support remained stable over time; thus, it will be important for teachers to understand the importance of showing students support throughout the middle school years. As students enter their last year of middle school, many teachers are in the mindset that they need to prepare students for high school, thus may be pushing students to be more independent. Withdrawing their support to students may be detrimental to student’s emotional health, particularly since support from teachers lost its protective effect when mothers’ support was low. Though teachers’ support could not compensate for low mothers’ support, if a student was experiencing low levels of support from both teachers and mothers they may be more at risk for depression.
The finding in the current study that depressive symptoms decreases during the middle school years goes against a widely accepted finding that depression and emotional distress increases during the period of time (Chen et al. 2011; Natsuaki et al. 2009). However, the findings from this study are consistent with the stage-environment fit theory (Eccles et al. 1993a, b). It is possible that there were protective benefits of being in a supportive middle school environment during a developmental stage full of new challenges and stressors. There is research to suggest that middle schools differ from junior high schools, and that students who attend a middle school (i.e., smaller groups of students, more contact between student and teacher, less ability-based tracking, more emphasis on objective grading) are less likely to have difficulties with the transition (Eccles et al. 1991). In the current study, the school was a true “middle school,” separated into core teams designed to allow more personal attention from teachers to students. Depressive symptoms were higher at the beginning of the transition to middle school, when transition stress was high, but declined as students adjusted to their new environment. In general, it would be reasonable to suggest that the initial transition to a new school would be related to greater distress than consecutive years. After a year of adjusting to the new school environment, students in subsequent years in the same building may experience relief of some emotional distress related to that transition. The fact that the current school was a true middle school might also be a factor in the continued impact that teachers had on the social-emotional well-being of the middle school students. Research on stage-environment fit argues for the continuation of school environments with strong supports in place during middle school (Eccles and Roeser 2011), and the findings from this study support this recommendation.
There are several strengths of the current investigation worth noting, as well as limitations that suggest avenues for future research. First, there are very few longitudinal investigations in the current literature focused on the effects of social support on depression that utilize more than two timepoints. The current study, with its use of four time points during the middle school years adds depth to our understanding of the importance of social support in the etiology of depressive symptoms by bringing new insights into the ways in which social support influences changes in depression during early adolescence. Second, the measure of social support utilized in the current study has excellent psychometric properties (see Malecki et al. 2003; Rueger et al. 2010), and includes a range of different types of support for a comprehensive measurement of social support. In addition, the fact that the same instrument was used to assess social support from mothers, fathers, and teachers allows for more confidence that assessment has resulted in comparable measurement of the same construct. A third strength is the diverse sample, ethnically and racially as well as socioeconomically, that was evenly distributed across gender, which increases generalizability of the findings to a general population. Related, with the use of a multilevel model for change, we were able to use the full sample of students across all four timepoints, increasing power in our study. However, we also note that there are limitations in the use of this procedure: although imbalanced data have little influences on the estimation of fixed effects, they may affect the estimation of variance components (Singer and Willett 2003). As variance explained by each model, which was indicated by the pseudo R2 reported, was computed using estimates of variance components, it should be interpreted with caution.
In addition, while the CASSS is a psychometrically robust instrument, it is possible that the positive effect of teachers’ support might have been suppressed by the way that this support was measured. More specifically, the CASSS asks students to think about their teachers collectively rather than focusing on individual teachers. It is possible that perceptions of support from a specific teacher could have revealed a stronger impact than was detected in the current study. An older line of research (e.g., Brock et al. 1996; Davis et al. 1998; Sarason et al. 1994) suggests that there are different relationships between well-being and global versus relationship-specific social support. Another line of research has found youth’s report of support from one non-parental adult is linked with improved social and academic outcomes (e.g., Chen et al. 2003). The combination of these two areas in the literature might suggest that an assessment of perceptions of support from a particular teacher may demonstrate a greater effect on social-emotional functioning than focusing on global perceptions of support from a group of teachers. Relatedly, another limitation in the current study is the exclusive focus on adult support sources. Adolescence is a time for increasing dependence on and importance of peer relationships, and while adult support clearly remains important, a consideration of the role of adult support in relation to peer support would further our understanding of the developmental course of depression in adolescence and the protective role that social support might play. There are indications that support from parents (Colarossi and Eccles 2003; Helsen et al. 2000; Rueger et al. 2010) and teachers (e.g., Colarossi and Eccles 2003; De Wit et al. 2011) is protective for adolescents, even when considering support from peers. However, other studies have demonstrated important interactive effects between adult and peer sources (Helsen et al. 2000; Young et al. 2005). Future research should continue to consider the protective role played by parents, as well as specific non-parental adults and peers during early adolescence to have a better understanding of protective factors related to depressive symptoms in early adolescence.
Conclusion
The current investigation adds to the literature by examining the unique and interactive effects of support from mothers, fathers and teachers on depressive symptoms over multiple timepoints with a consideration for gender differences. Results documenting the emergence of gender differences in depressive symptoms during the course of the middle school years were consistent with the literature in showing that girls and boys are at similar risk for depression during the transition into middle school, but girls are at greater risk later in their middle school years. In addition, the protective role of mothers, fathers, and teachers was supported by this research, indicating that these adult sources of support take on new importance in the lives of young adolescents as they mature and transition to environments that offer gradually increasing independence. Although youth seemingly want to rely less on adults, such as parents or teachers, for support, the results from the current study adds to the growing literature that clearly documents the continued importance of adults in the lives of young adolescents. Support from mothers was particularly salient throughout this time period, especially when support from fathers was lacking, and was especially potent in conjunction with high levels of support from teachers, as each source of support served to amplify the protective benefits of the other source. Finally, although gender differences were evident with all three sources of support in correlational analyses, the only gender difference that emerged from growth curve analyses was with mothers’ support. Although support from mothers was significant for both boys and girls, its protective effects in reducing levels of depressive symptoms was significantly stronger for girls than for boys during the middle school years. Taken together, our results suggest that future research should continue to focus on the independent and interactive effects of support from multiple sources and gender differences in these effects longitudinally using multiple timepoints of data during this potentially challenging time period in order to inform prevention and interventions efforts both at home and in the schools.
References
Blum, R. W., McNeely, C. A., & Rinehart, P. M. (2002). Improving the odds: The untapped power of schools to improve the health of teens. Minneapolis, MN: Center for Adolescent Health and Development, University of Minnesota.
Brock, D. M., Sarason, I. G., Sarason, B. R., & Pierce, G. R. (1996). Simultaneous assessment of perceived global and relationship-specific support. Journal of Social and Personal Relationships, 13(1), 143–152. doi:10.1177/0265407596131008.
Bronfenbrenner, U. (1979). Contexts of child rearing: Problems and prospects. American Psychologist, 34(10), 844–850. doi:10.1037/0003-066X.34.10.844.
Chen, C., Greenberger, E., Farruggia, S., Bush, K., & Dong, Q. (2003). Beyond parents and peers: The role of important non-parental adults (VIPS) in adolescent development in China and the United States. Psychology in the Schools, 40(1), 35–50. doi:10.1002/pits.10068.
Chen, A. C., Haas, S., Gillmore, M. R., & Kopak, A. (2011). Trajectories of depressive symptoms from adolescence to young adulthood: Chinese Americans versus non-Hispanic whites. Research in Nursing and Health, 34(3), 176–191. doi:10.1002/nur.20429.
Colarossi, L. G., & Eccles, J. S. (2003). Differential effects of support providers on adolescents’ mental health. Social Work Research, 27(1), 19–30. doi:10.1093/swr/27.1.19.
Conners-Burrow, N., Johnson, D. L., Whiteside-Mansell, L., McKelvey, L., & Gargus, R. A. (2009). Adults matter: Protecting children from the negative impacts of bullying. Psychology in the Schools, 46(7), 593–604. doi:10.1002/pits.20400.
Costello, D. M., Swendsen, J., Rose, J. S., & Dierker, L. C. (2008). Risk and protective factors associated with trajectories of depressed mood from adolescence to early adulthood. Journal of Consulting and Clinical Psychology, 76, 173–183. doi:10.1037/0022-006X.76.2.173.
Cummings, P. (2013). Missing data and multiple imputation. JAMA Pediatrics, 167(7), 656–661. doi:10.1001/jamapediatrics. 2013.1329.
Davis, M. H., Morris, M. M., & Kraus, L. A. (1998). Relationship-specific and global perceptions of social support: Associations with well-being and attachment. Journal of Personality and Social Psychology, 74, 468–481. doi:10.1037/0022-3514.74.2.468.
De Wit, D. J. D., Karioja, K., Rye, B. J., & Shain, M. (2011). Perceptions of declining classmate and teacher support following the transition to high school: Potential correlates of increasing student mental health difficulties. Psychology in the Schools, 48(6), 556–572. doi:10.1002/pits.20576.
Demaray, M. K., & Malecki, C. K. (2002). Critical levels of social support associated with student adjustment. School Psychology Quarterly, 17, 213–241.
DeMaris, A. (2004). Regression with social data: Modeling continuous and limited response variables (1st ed.). NJ: Wiley-Interscience.
Eccles, J. S., Lord, S., & Midgley, C. (1991). What are we doing to early adolescents? The impact of educational contexts on early adolescents. American Journal of Education, 99(4), 521–542. doi:10.1086/443996.
Eccles, J. S., Midgley, C., Wigfield, A., Buchanan, C. M., Reuman, D., Flanagan, C., et al. (1993a). Development during adolescence: The impact of stage-environment fit on young adolescents’ experiences in schools and in families. American Psychologist, 48(2), 90–101. doi:10.1037/0003-066X.48.2.90.
Eccles, J. S., & Roeser, R. W. (2011). Schools as developmental contexts during adolescence. Journal of Research on Adolescence, 21(1), 225–241. doi:10.1111/j.1532-7795.2010.00725.x.
Eccles, J. S., Wigfield, A., Midgley, C., & Reuman, D. (1993b). Negative effects of traditional middle schools on students’ motivation. The Elementary School Journal, 93(5), 553–574. doi:10.1086/461740.
Ezzell, C. E., Swenson, C. C., & Brondino, M. J. (2000). The relationship of social support to physically abused children’s adjustment. Child Abuse and Neglect, 24, 641–651. doi:10.1016/S0145-2134(00)00123-X.
Frydenberg, E., & Lewis, R. (1991). Adolescent coping: The different ways in which boys and girls cope. Journal of Adolescence, 14, 119–133.
Frydenberg, E., & Lewis, R. (1993). Boys play sports and girls turn to others: Age, gender and ethnicity as determinants of coping. Journal of Adolescence, 16, 253–266.
Ge, X., Conger, R. D., & Elder, G. H. J. (2001). Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental Psychology, 37(3), 404–417. doi:10.1037/0012-1649.37.3.404.
Ge, X., Lorenz, F. O., Conger, R. D., Elder, G. H., & Simons, R. L. (1994). Trajectories of stressful life events and depressive symptoms during adolescence. Developmental Psychology, 30(4), 467–483. doi:10.1037/0012-1649.30.4.467.
Hankin, B. L., & Abramson, L. Y. (2001). Development of gender differences in depression: An elaborated cognitive vulnerability–transactional stress theory. Psychological Bulletin, 127(6), 773–796. doi:10.1037/0033-2909.127.6.773.
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., McGee, R., & Angell, K. E. (1998). Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107(1), 128–140. doi:10.1037/0021-843X.107.1.128.
Helsen, M., Vollebergh, W., & Meeus, W. (2000). Social support from parents and friends and emotional problems in adolescence. Journal of Youth and Adolescence, 29(3), 319–335. doi:10.1023/A:1005147708827.
Jia, Y., Way, N., Ling, G., Yoshikawa, H., Chen, X., Hughes, D., et al. (2009). The influence of student perceptions of school climate on socioemotional and academic adjustment: A comparison of Chinese and American adolescents. Child Development, 80(5), 1514–1530. doi:10.1111/j.1467-8624.2009.01348.x.
Kessler, R. C., McGonagle, K. A., Swartz, M., & Blazer, D. G. (1993). Sex and depression in the national comorbidity survey: I. Lifetime prevalence, chronicity and recurrence. Journal of Affective Disorders, 29(2–3), 85–96. doi:10.1016/0165-0327(93)90026-G.
Levitt, M. J., Guacci-Franco, N., & Levitt, J. L. (1993). Convoys of social support in childhood and early adolescence: Structure and function. Developmental Psychology, 29(5), 811–818. doi:10.1037/0012-1649.29.5.811.
Malecki, C. K., & Demaray, M. K. (2003). What type of support do they need? Investigating student adjustment as related to emotional, informational, appraisal, and instrumental support. School Psychology Quarterly, 18(3), 231–252. doi:10.1521/scpq.18.3.231.22576.
Malecki, C. K., Demaray, M. K., & Elliott, S. N. (2003). A working manual on the development of the child and adolescent social support scale (2000). Dekalb: Unpublished manuscript, Northern Illinois University.
Meadows, S. O., Brown, J. S., & Elder, G. H, Jr. (2006). Depressive symptoms, stress, and support: Gendered trajectories from adolescence to young adulthood. Journal of Youth and Adolescence, 35(1), 93–103. doi:10.1007/s10964-005-9021-6.
Natsuaki, M. N., Biehl, M. C., & Ge, X. (2009). Trajectories of depressed mood from early adolescence to young adulthood: The effects of pubertal timing and adolescent dating. Journal of Research on Adolescence, 19(1), 47–74. doi:10.1111/j.1532-7795.2009.00581.x.
Needham, B. L. (2008). Reciprocal relationships between symptoms of depression and parental support during the transition from adolescence to young adulthood. Journal of Youth and Adolescence, 37(8), 893–905. doi:10.1007/s10964-007-9181-7.
Niemiec, C. P., Lynch, M. F., Vansteenkiste, M., Bernstein, J., Deci, E. L., & Ryan, R. M. (2006). The antecedents and consequences of autonomous self-regulation for college: A self-determination theory perspective on socialization. Journal of Adolescence, 29(5), 761–775. doi:10.1016/j.adolescence.2005.11.009.
Patten, C. A., Gillin, C. J., Farkas, A. J., Gilpin, E. A., Berry, C. C., & Pierce, J. P. (1997). Depressive symptoms in California adolescents: Family structure and parental support. Journal of Adolescent Health, 20(4), 271–278. doi:10.1016/S1054-139X(96)00170-X.
Piko, B., Kovacs, E., & Fitzpatrick, K. M. (2009). What makes a difference? Understanding the role of protective factors in Hungarian adolescents’ depressive symptomatology. European Child and Adolescent Psychiatry, 18(10), 617–624. doi:10.1007/s00787-009-0022-y.
Preacher, K. J., Curran, P. J., & Bauer, D. J. (2006). Computational tools for probing interaction effects in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31, 437–448.
Reddy, R., Rhodes, J. E., & Mulhall, P. (2003). The influence of teacher support on student adjustment in the middle school years: A latent growth curve study. Development and Psychopathology, 15(1), 119–138. doi:10.1017/S0954579403000075.
Reynolds, C. R., & Kamphaus, R. W. (2004). BASC-2: Behavior assessment system for children, second edition manual. Circle Pines, MN: American Guidance Service.
Roeser, R. W., Eccles, J. S., & Sameroff, A. J. (1998). Academic and emotional functioning in early adolescence: Longitudinal relations, patterns, and prediction by experience in middle school. Development and Psychopathology, 10(2), 321–352. doi:10.1017/S0954579498001631.
Rueger, S. Y., & Malecki, C. K. (2011). Effects of stress, attributional style and perceived parental support on depressive symptoms in early adolescence: A prospective analysis. Journal of Clinical Child and Adolescent Psychology, 40(3), 347–359. doi:10.1080/15374416.2011.563461.
Rueger, S. Y., Malecki, C. K., & Demaray, M. K. (2008). Gender differences in the relationship between perceived social support and student adjustment during early adolescence. School Psychology Quarterly, 23, 496–514.
Rueger, S. Y., Malecki, C. K., & Demaray, M. K. (2010). Relationship between multiple sources of perceived social support and psychological and academic adjustment in early adolescence: Comparisons across gender. Journal of Youth and Adolescence, 39(1), 47–61. doi:10.1007/s10964-008-9368-6.
Ryan, A. M., & Patrick, H. (2001). The classroom social environment and changes in adolescents’ motivation and engagement during middle school. American Educational Research Journal, 38(2), 437–460. doi:10.3102/00028312038002437.
Sarason, I. G., Sarason, B. R., & Pierce, G. R. (1994). Social support: Global and relationship-based levels of analysis. Journal of Social and Personal Relationships, 11(2), 295–312. doi:10.1177/0265407594112008.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis: Modeling change and event occurrence. New York: Oxford University Press.
Stice, E., Ragan, J., & Randall, P. (2004). Prospective relations between social support and depression: Differential direction of effects for parent and peer support? Journal of Abnormal Psychology, 113(1), 155–159. doi:10.1037/0021-843X.113.1.155.
Twisk, J. (2006). Applied multilevel analysis (1st ed.). NY: Cambridge University Press.
Twisk, J., & de Vente, W. (2002). Attrition in longitudinal studies: How to deal with missing data. Journal of Clinical Epidemiology, 55(4), 329–337.
Werner, E. E., & Johnson, J. L. (2004). The role of caring adults in the lives of children of alcoholics. Substance Use and Misuse, 39(5), 699–720. doi:10.1081/JA-120034012.
Wigfield, A., Eccles, J. S., Schiefele, U., Roeser, R. W., & Davis-Kean, P. (2006). Development of achievement motivation. In N. Eisenberg, W. Damon, & R. M. Lerner (Eds.), (pp (pp. 933–1002). Hoboken, NJ: John Wiley & Sons Inc.
Young, J. F., Berenson, K., Cohen, P., & Garcia, J. (2005). The role of parent and peer support in predicting adolescent depression: A longitudinal community study. Journal of Research on Adolescence, 15(4), 407–423. doi:10.1111/j.1532-7795.2005.00105.x.
Acknowledgments
We would like to thank the students and staff at this middle school for their participation. We also would like to acknowledge Christine Malecki Ph.D., Michelle Demaray Ph.D., and their research labs at Northern Illinois University for their support during these data collections.
Author contributions
SR conceived of the study, collected the data, participated in the design and coordination of the study, and drafted sections of the manuscript. PC participated in the design of the study, performed the statistical analysis, and drafted sections of the manuscript. LJ participated in the design and helped to draft sections of the manuscript. HJC coordinated aspects of the literature review and helped to draft sections of the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rueger, S.Y., Chen, P., Jenkins, L.N. et al. Effects of Perceived Support from Mothers, Fathers, and Teachers on Depressive Symptoms During the Transition to Middle School. J Youth Adolescence 43, 655–670 (2014). https://doi.org/10.1007/s10964-013-0039-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-013-0039-x