
Abstract
Experience with and management of stress has implications for adolescents’ behavioral and socioemotional development. This study examined the relationship between adolescents’ physiological response to an acute laboratory stressor (i.e., Trier Social Stress Test; TSST) and anger regulation and interpersonal competence in a sample of 175 low-income urban adolescents (51.8% girls). Findings suggested that heightened reactivity as indicated by cortisol, heart rate, and blood pressure was associated with increased interpersonal competence and anger regulation. However, these findings were context dependent such that, for youth high in self-reported child maltreatment, heightened reactivity was associated with decreased interpersonal competence and anger regulation. Results highlight the importance of considering how context may condition the effect of stress reactivity on functioning during adolescence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anger regulation and interpersonal competence are important indicators of socioemotional adjustment during adolescence (Buhrmester 1990; Nicholas et al. 2008). Anger regulation is a defining element of externalizing problems (Bradley 2000); whereas interpersonal competence is important in forming and maintaining peer relationships (Demir and Urberg 2004). Within western culture, two of the most important developmental tasks that adolescents must accomplish are avoiding externalizing behaviors and forming and maintaining peer relationships (Roisman et al. 2004). Problems with anger regulation and interpersonal competence in adolescence have been associated with increased physical and psychological problems during adulthood (Harold et al. 2004; Roisman et al. 2004). Thus, examining influences on anger regulation and interpersonal competence is paramount given their likely role in helping adolescents successfully transition into adulthood.
Many factors may contribute to anger regulation and interpersonal competence during adolescence and include both physiological states and environmental influences (Dodge and Pettit 2003; Reiss et al. 2000). Heightened reactivity in response to a stressor has been associated with both maladaptive behavior and healthy, adaptive functioning during adolescence (Boyce and Ellis 2005; Obradovic et al. 2010; Susman 2006). Ellis and Boyce (2008) have suggested that a heightened stress response is only a vulnerability in highly stressful contexts (such as in the context of child maltreatment by caregivers) but that in less stressful, supportive environments (such as supportive family environments) heightened reactivity is associated with positive functioning. To explore this theory, the current study examined whether the relationship between stress reactivity to an acute laboratory based stressor (TSST) and two important indicators of adolescent’s socioemotional functioning, anger regulation and interpersonal competence, was affected by adolescents’ recall and/or perception of maltreatment (e.g., physical and/or emotional abuse, neglect) in a sample of low-income urban youth. Examining how child maltreatment may modify the impact of stress reactivity on youth’s functioning helps illuminate the conditions under which reactivity contributes to maladaptive and adaptive functioning during adolescence.
Stress Reactivity and Adjustment
A growing body of literature finds that variability in adolescents’ stress response both in the hypothalamic- pituitary- adrenal axis (HPA) and the autonomic nervous system (ANS) is associated with adolescent functioning (Adam and Kumari 2009; van Goozen et al. 2007). The ability to activate the stress response system is a normative response by the body that is necessary for survival and serves an adaptive function in the short-term. However, chronic activation of the HPA and ANS may contribute to impairments in affective, behavioral, and cognitive functioning (McEwen 2007). Much of the literature on stress response and adjustment suggests that heightened reactivity to stress is a risk factor for negative adjustment during adolescence, both in regards to problems managing anger and in interpersonal relationships (Granger et al. 1996; Kobak et al. 2009; Miller et al. 2006). However, highly reactive children may only experience negative outcomes when reared in adverse environments, suggesting an important role of context, defined here as environmental rearing conditions (past or present), in the relationship between stress reactivity and adolescent outcomes (Ellis and Boyce 2008).
Biological Sensitivity to Context: Child Maltreatment
Heightened stress reactivity may have negative and positive associations with psychological functioning that are context dependent. Ellis and Boyce (2008) propose that individual differences in reactivity, developed as a result of the interaction between genetic and early environmental experiences, increase reactive individuals’ susceptibility to both adverse and positive environments, which in turn increases vulnerability for developing negative outcomes under adverse conditions and positive outcomes under supportive conditions. Specifically, heightened reactivity in adverse environments is exacerbated and leads to upregulation of reactivity to stress in other environmental situations resulting in increased wariness in children and problems managing anger and difficulties in interpersonal relationships. Alternatively, for reactive youth who are reared in more supportive, less stressful environments, children may use that heightened arousal response to benefit from the social environment and develop good emotion regulation skills and social competence (Ellis et al. 2005; Boyce and Ellis 2005). It may be that reactive children are more reflective and conscious of self and, thus, could potentially benefit more from supportive environments by taking advantage of what that environment has to offer. To some extent, heightened reactivity may be typical during the period of adolescence and only a problem under conditions of environmental adversity with those individuals that experience trauma during this period or earlier developmental periods being vulnerable to developing dysregulated negative affect (Casey et al. 2010). Therefore, the context in which youth develop is important to consider when examining the relationship between stress reactivity and adjustment.
Research has examined the role of different environmental conditions in the relationship between reactivity and outcomes, but this research has predominately focused on children. For example, research has demonstrated that children who are both physiologically reactive and have low father or mother involvement are most at risk for mental health problems during childhood, with the lowest rates of mental health problems among children who were reactive and report low maternal depression (Boyce et al. 2006). Furthermore, heightened reactivity has been associated with positive adjustment under conditions of low adversity but with externalizing problems under conditions of high adversity (Obradovic et al. 2010). The current study will contribute to this growing body of research by examining Boyce and Ellis (2005) theory during adolescence and by focusing on child maltreatment.
Children who experience child maltreatment often develop in contexts where there is a lack of warmth and support, as well as high levels of violence, both of which increase exposure to uncontrollable stress and upregulate stress reactivity (Bell and Belsky 2007; van Voorhees and Scarpa 2004). In turn, when youth are faced with acute stressors in other contexts they may become overly aroused and thus experience problems regulating emotions and being competent in interpersonal relationships (Obradovic et al. 2010). Thus, child maltreatment may create a context under which youths’ reactivity to stressors is developed and/or exasperated, which in turn, is associated with maladjustment (Cicchetti and Rogosch 2001).
Child maltreatment may be particularly problematic for the development of socio-emotional problems for children who are biologically reactive (Hart et al. 1996). Despite the extensive amount of research on the relationship between child maltreatment and socio-emotional problems, specifically externalizing problems, and the research on stress reactivity and socio-emotional problems, little to no research has been done on the interaction of maltreatment and stress reactivity on socio-emotional problems and thus marks an important area for future research (van Voorhees and Scarpa 2004). There has been research during infancy and childhood, however, suggesting that behaviorally or biologically reactive children, as compared to less reactive children, show the worst outcomes under conditions of contextual adversity (e.g., low parental warmth) and the best outcomes in supportive environments (Ellis et al. 2011; Obradovic et al. 2010). The current study extends this research by examining whether current heightened reactivity to an acute stressor in a laboratory setting coupled with reports of past child maltreatment is associated with difficulties with anger regulation and interpersonal competence during adolescence.
Hypotheses
There is accumulating evidence that youths’ stress response contributes to psycho-social functioning during adolescence. However, the conditions under which heightened reactivity is associated with maladaptive functioning are not well understood. Thus, the current study examines whether the nature of the relationship between current stress reactivity to an acute stressor and adolescents’ adjustment varies in the context of childhood maltreatment. Specifically, we hypothesized that greater stress reactivity to an acute stressor is associated with more anger regulation difficulties and lower interpersonal competence but only when youth report higher levels of child maltreatment and conversely greater stress reactivity to an acute stressor is associated with less anger regulation difficulties and higher interpersonal competence when youth report lower levels of child maltreatment.
Past research suggests that gender differences may exist in the relationship between adolescents’ stress response and social and behavioral outcomes (Chaplin et al. 2010; Natsuaki et al. 2009). Research generally has been mixed with some studies finding a stronger relationship between stress reactivity and outcomes for girls (Natsuaki et al. 2009) and some studies finding a stronger relationship for boys (Tout et al. 1998). Thus, all models controlled for gender to account for these potential relationships.
Methods
Participants
This study utilized data from a longitudinal project that examined development in high-risk low income urban families who had been followed since birth, with twice yearly assessments (N = 371). Families were originally recruited over a 5 year period from women registering for prenatal care at a Women’s center of a large urban hospital in the Northeast and from women in a delivery ward who had not received prenatal care. During adolescence, a subsample of the larger sample who were aged 14 ½ to 16 years and who met the present study’s eligibility criteria (no acute psychiatric condition, no serious medical condition, not pregnant, and IQ > 80) were invited to participate in the present laboratory based study of the effects of stress of adolescents’ functioning. Based on these criteria, only 11 adolescents were excluded from participation. The 175 youth who participated were not different from the overall sample on demographic characteristics (sex, race, and mother education level). Adolescents were predominately African American (86.9%) and 51.8% of participants were girls. No mothers had greater than high school educations. Adolescents’ primary caregivers were mostly biological mothers (80%). At the time of data collection adolescents were roughly 15 ½ years of age (M = 15.36, SD = 1.01).
Procedures
Youth completed four sessions, spaced roughly 1 week apart. During the first two sessions youth completed questionnaires (e.g., Childhood Trauma Questionnaire), computer tasks, and interviews that assessed adjustment. Youth also participated in a laboratory-based stress session during session three. Data from session four was not used for the current study. All sessions lasted roughly 3 h and both parental consent and adolescent asset were obtained for the sessions. Adolescents and parents were told that participation in all sessions was optional and that they had the right to refuse any part of the assessments and payment would still be awarded.
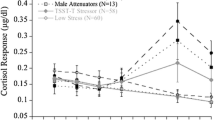
The Trier Social Stress Test conducted during session three (TSST-C; Buske-Kirschbaum et al. 1997) was used to examine adolescents’ stress reactivity to an acute stressor. All laboratory sessions began at 4:15 pm as there is less variation in cortisol at that time of day (Blackhart et al. 2007). The first part of the session involved a relaxation period, which lasted 40 min, at which pretest measures of blood pressure, pulse, cortisol, and self-reported emotion were taken. The relaxation period consisted of a trained research assistant guiding participants through breathing exercises and muscle relaxation, which lasted on average 7 min. Following the relaxation period, youth participated in the TSST-C. The TSST-C was used to induce social stress in adolescents by asking youth to prepare and relay a story (i.e., give a speech) to two unfamiliar adult “judges.” The adolescent was given a story stem and asked to prepare the rest of the story for 5 min. After this, adolescents are asked to give this speech for 5 min while standing in front of the two judges. After the 5 min are finished youth were asked to complete a math task out loud in front of the judges. Judges maintain a neutral expression and do not help adolescents during the task. The TSST-C is one of the most widely used and valid tests for eliciting a stress response in adolescents (Kudielka et al. 2004). Adolescents were debriefed regarding the TSST-C 20 min after the end of the task.
Physiological and self-report assessments assessing stress response were taken during the TSST-C (for HR), immediately after the TSST-C, and then every 15 min through 1 h of recovery. Adolescents were compensated $50 for participation in each session, with an additional bonus payment for completing all sessions. Most adolescents completed all sessions and thus there was very little missing data (i.e., no measure used in the current study had more than 15 participants missing data).
Measures
Stress Response
Salivary cortisol levels were measured as a biomarker of HPA axis activation. Salivary cortisol is a well-established non-invasive measure of HPA axis functioning that is highly correlated with plasma cortisol (Adam and Kumari 2009). To obtain cortisol, saliva was collected using a cotton swab that participants were asked to place between their cheek and tongue for approximately 2 min. The swab was put in a tube and placed directly on ice and stored at −20C before being assayed in duplicate at a University laboratory. The intra-assay coefficients of variation for the assay kits ranged from 3.0 to 5.1%. Samples were taken during the relaxation period, at baseline following the relaxation period (40 min into the session), right before adolescents prepared the story (47 min into the session), immediately following the speech and math tasks (+65), and every 15 min during recovery (+80, +95, +110, +125). To examine adolescents’ stress response to the TSST-C, baseline cortisol (40) was subtracted from peak cortisol at 80 min. Forty minutes was chosen as baseline, as opposed to assessments taken within the first 15–30 min of the session, because presumably adolescents have acclimated to the laboratory setting during the relaxation period. Furthermore, data indicated that on average cortisol was at its lowest value 40 min into the session. Eighty minutes was chosen as “peak” because salivary cortisol levels increase about 15 min after acute stressors. Baseline minus peak is a valid measure of adolescents’ stress response to an acute stressor.
To examine cardiovascular response, another important indicator of stress reactivity, a Critikon Dinamap 120 Patient monitor was used to assess systolic blood pressure (SBP) and diastolic blood pressure (DBP). A pulse sensor also was attached to the participant’s finger to provide continuous heart rate (HR) measurement. Blood pressure and heart rate were measured at baseline (+40), at task preparation (+47), after the TSST-C (+65), and 15 min after the task (+80). Additionally, HR was measured on two occasions during the TSST-C (+55 & +60). To examine adolescents’ stress response, three measures of cardiovascular reactivity were computed: (a) SBP peak (at +65) minus baseline, (b) DBP peak (at +65) minus baseline at 65 min, and (c) HR peak (an average of the 55 and 60 time points) minus baseline.
Anger Regulation
The Self-Report Adolescent component of the Behavior Assessment Scale for Children Self-Report of Personality (BASC-SRP; Reynolds and Kaphaus 2002) was used to assess anger regulation and interpersonal competence. The BASC-SRP is a highly valid instrument for assessing both competence and maladjustment among adolescents (Stein et al. 2007). The Anger Control subscale includes 14 items intended to assess adolescents’ competency in controlling their anger. Participants respond to both true/false items and on a 4-point scale ranging from 1 (Never) to 4 (Almost Always) to questions such as “When I get angry I can’t think about anything else.” and “When I am angry I want to hurt someone.” Higher scores indicated less anger regulation.
Interpersonal Competence
The 7-item Interpersonal Relations Subscale from the BASC-SRP was used to measure interpersonal competence among adolescents and included a combination of true/false items and a responses on 4-point scale ranging from 1 (Never) to 4 (Almost Always). Sample items included “I am slow to make new friends.” and “My classmates don’t like me.” Higher scores reflect more interpersonal competence. The BASC-SRP is a widely-used measure and these subscales show good internal consistency, with alpha coefficients on subscales exceeding .80 (Reynolds 2010; Stein et al. 2007).
Childhood Maltreatment
Adolescents’ experiences of childhood maltreatment were assessed with the Childhood Trauma Questionnaire-short form (CTQ-SF; Bernstein et al. 1994). The CTQ short-form contains five subscales and 28-items that assess youths’ perceptions of physical and emotional maltreatment (neglect and abuse) and sexual abuse during childhood and adolescence. Because reports of sexual abuse was rare, only the four subscales assessing physical and emotional maltreatment were used; thus resulting in 20 items. Participants were asked to think about their experiences growing up as a child and teenager and respond on a scale from 1 (Never True) to 5 (Very Often True) to questions such as “I felt unloved” and “I was punished with a belt, a board, a cord, or some other object.” A sum score was computed across the subscales, with higher scores indicating more perceived maltreatment (α = .73). Within our sample scores ranged from 20–62 out of a possible range of 20–100 (M = 33.47, SD = 8.41). For analyses, we computed a dichotomous variable for high versus low CTQ scores. Following recommendations from the manual, youth falling below a score of 32 were classified in as low maltreatment (51% of youth) and youth who scored above 32 as high in maltreatment (49% of youth; Bernstein and Fink 1998). The CTQ has been found to be a reliable and valid measure of childhood maltreatment in adolescent samples. Specifically, adolescent reports on the CTQ have been found to have good test–retest reliability, predictive validity, and correlate with official reports of child maltreatment (Bernstein et al. 2003; Wolfe et al. 2001).
Analytic Strategy
The AMOS 18.0 structural equation modeling (SEM) program was used to test the relationship between stress reactivity and adolescents’ adjustment by maltreatment history. Models included peak minus baseline scores as measures of stress reactivity. Preliminary analyses attempted to run growth curve models of the full trajectory of stress response (from baseline to peak to recovery); however, these models did not identify, potentially because of small sample size and multicollinearity among the data points. Thus, below we only present findings using peak minus baseline as the measure of stress reactivity. Furthermore, preliminary confirmatory factor analyses in AMOS indicated that a latent stress reactivity variable did not fit the data well, and thus indicators of stress reactivity were modeled as manifest variables in separate path models.
Preliminary confirmatory factor analyses in AMOS indicated that a latent stress reactivity variable did not fit the data well, and thus indicators of stress reactivity were modeled as manifest variables in separate path models. Models were estimated separately because of concerns of power due to a smaller sample size and, furthermore, we were not interested in examining the relative effects of different measures of stress reactivity on adolescents’ outcomes (Kline 2005). Model fit for all path models were examined using the Chi-square goodness of fit statistic, the comparative fit indices (CFI), and the root mean square error of approximation (RMSEA). A nonsignificant Chi-square indicated a good model fit (Byrne 2001). CFI values of .90 indicated adequate fit of the data and RMSEA values ranging from .05 to .08 indicated adequate model fit (Thompson 2000). The significance threshold for all models was set at p < .05. The full information maximum likelihood estimation procedure (FIML) was used to address missing values because FIML produces less biased estimates than does listwise case deletion or mean substitution (Acock 2005).
To test for moderating effects of child maltreatment, a multiple-group path analysis was conducted with two groups: those reporting high maltreatment and those reporting low maltreatment. Multiple-group models are a commonly used technique for testing moderation within path analysis (Tomarken and Waller 2005). We used a dichotomous moderator and ran a multiple group model, as opposed to estimating a continuous interaction, because it is very difficult to detect moderating effects with continuous variables and we wanted to maximize power to detect potential group differences (McClelland and Judd 1993; Henseler and Fassott 2010). To test for differences across groups, two models were compared, one in which all parameters were constrained to be equal and the other in which the structural loadings were allowed to vary across the two groups. Change in the Chi-square was examined for statistical significance at the p < .05 level. A significant change in Chi-square between the models suggests that group differences in the freed structural pathways exist, and critical ratios above 1.96 were examined to locate specific, significant group differences (Byrne 2001). We chose to use SEM because it offers several advantages over multiple regression that were pertinent to the current study. Specifically, within SEM researchers have the ability to assess the relationship between individual constructs as well as overall model fit, the ability to take into account error on the dependent variables, and the ability to address missing data with FIML.
Results
Descriptive Statistics
Data were examined for normality. The cortisol data was skewed. To address this, values that were greater than 3 standard deviations above the mean were reassigned a value equal to three standard deviations above the mean (following Susman et al. 2007). All other variables fell within the range of normality and did not require transformation. Correlations among study variables, as well as means and standard deviations are presented in Table 1.
Gender was controlled for in all analyses. Gender was not significantly associated with any of the four indicators of acute stress reactivity but was significantly associated with anger regulation such that boys reported lower levels of anger regulation than girls, β = −.18, p < .05.
To get a better sense of current functioning across the two groups (high child maltreatment and low child maltreatment), we also examined mean differences in demographics, protective factors within the family and at school, perceived stress, adolescents’ functioning, and stress response (Table 2). Analyses indicated that youth low in child maltreatment reported more positive relationships with parents, less perceived stress, and fewer problems at school than youth high in child maltreatment. These descriptive results provide preliminary evidence that youth in the child maltreatment group were currently experiencing multiple stressors within their lives as compared to youth in the non-maltreated group.
Stress Reactivity and Adolescents’ Adjustment
We first examined the relationship between four different indicators of stress reactivity and interpersonal competence and anger regulation for the full sample of youth (Fig. 1). Models were estimated separately for the different stress responses of heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), and cortisol. Chi- square was highly non-significant for all models indicating good model fit. Furthermore, CFI and RMSEA values from all models ranged from .91 to .94 and .07 to .08, respectively, indicating adequate model fit. Heart rate reactivity (i.e., an increase in heart rate from baseline to peak) was significantly associated with interpersonal competence (β = .16, p < .05), and cortisol reactivity (i.e., an increase in cortisol from baseline to peak) was associated with interpersonal competence but only reached a trend level of significance (β = .14, p = .09). Higher DBP reactivity (i.e., an increase in DBP from baseline to peak) was associated with less problems with anger regulation (β = −.18, p < .05). Results from these models suggested that adolescents with higher stress reactivity, as indicated by heart rate reactivity and DPB, were more likely to report interpersonal competence and less likely to report problems with anger regulation.

Stress reactivity and adolescents’ adjustment. Although represented here in the same figure, separate models were estimated for the four different indicators of stress reactivity. Standardized betas are presented and * indicates significance at p < .05 level. Dashed lines indicate non-significant associations. All analyses controlled for gender
Child Maltreatment, Stress Reactivity and Adolescents’ Adjustment
Adolescents low and high in child maltreatment differed on their associations between stress reactivity and anger regulation and interpersonal competence. Specifically, results from the omnibus group difference tests in all four models indicated that there were significant changes in Chi-squares, ranging from 14.59 to 24.87, when the paths were allowed to differ for adolescents low and high in child maltreatment (Fig. 2). In terms of anger regulation, when the effect of cortisol reactivity on adolescents’ adjustment was examined across groups, critical ratios indicated that the relationship between cortisol reactivity and anger regulation difficulties was significant and positive for those high in child maltreatment, β = .32, p < .01 and significant and negative for those low in child maltreatment, β = −.26, p = .02. When the relationship of SBP reactivity and anger regulation problems was examined across groups there was a significant and positive relationship for those high in child maltreatment, β = .17, p < .05; this relationship was significant and negative for youth low in child maltreatment, β = −.32, p < .001. The pattern of findings between heart rate and anger regulation were similar, with higher heart rate reactivity associated with less anger regulation problems among youth low in child maltreatment, β = −.23, p < .01 and non-significant and positive for youth high in child maltreatment, β = .10, p = .28. DBP followed a similar but slightly different pattern with higher DBP reactivity associated with less anger regulation problems among youth low in child maltreatment, β = −.26, p < .01 and non-significant and negative for youth high in child maltreatment, β = −.13, p = .20.

Stress response adolescents’ adjustment, and child maltreatment. Although represented here in the same figure, separate models were estimated for the four different indicators of stress reactivity. Those low in child maltreatment are to the left and youth high in child maltreatment are to the right of the diagonal. Standardized betas are presented and * indicates significance at p < .05 level. Models control for gender
There also were significant differences between groups for the relationship between stress reactivity and interpersonal competence. Critical ratios indicated that three of the structural pathways differed for those low and high in child maltreatment. The pathway from heart rate reactivity to interpersonal competence was significant and positive for youth low in child maltreatment, β = .31, p < .001 but was non-significant and negative for youth high in child maltreatment, β = −.07, p = .46. Furthermore, the pathway from SBP reactivity, as well as the path from DBP reactivity to interpersonal competence were significant and positive for youth low in child maltreatment, β = .21, p < .05 and β = .20, p < .05, respectively but non-significant for those high in child maltreatment, β = −.01, p = .99 and β = .07, p = .51, respectively.
Discussion
The effect of child maltreatment on the relationship between adolescents’ stress reactivity and adjustment is an important but understudied topic. This study contributes to the literature by providing support for Ellis and Boyce’s (2008) premise that heightened reactivity to stress is only a vulnerability in highly stressful contexts but that in less stressful, contexts heightened arousal is associated with positive functioning. Furthermore, we contribute to the literature by demonstrating empirically that child maltreatment conditions the relationship between stress reactivity and adolescents’ functioning in a sample of urban youth. Specifically, we found that heightened reactivity to a acute stressor was associated with adaptive functioning in less adverse environments. Conversely, heightened reactivity was a risk factor for decreased anger regulation and decreased interpersonal competence in more adverse environments.
This is one of the first studies to examine the relationship between stress reactivity and anger regulation and interpersonal competence in a low income urban sample of adolescents. Findings from the sample as a whole suggested that heightened reactivity to an acute stressor (defined as change in heart rate, cortisol, and blood pressure) was associated with increased interpersonal competence and anger regulation but the associations were only modest. Modest associations are consistent with previous research findings on the relationship between physiological reactivity and adolescent outcomes (Granger and Kivlighan 2003; Obradovic et al. 2010). Furthermore, few studies have been conducted with predominately low income urban samples of youth, and the robustness of the stress response and associations of the stress response and adolescent functioning may vary based on the race, SES, and location of the sample (Jackson et al. 1999). Thus, it will be important in future research to examine whether associations between stress reactivity to an acute stressor and adjustment are comparable to the associations found in less urban environments with predominately middle and upper class European American youth. Another potential reason for the modest associations is that within youth there is variability in contextual influences that might affect the relationship between stress reactivity and functioning. Examining potential factors that may affect the nature of the relationship between stress reactivity and youths’ functioning is a critical yet understudied topic of research that may help explain the discrepancies in current research.
To this end and consistent with work done by Ellis and Boyce (2008) and Gunnar et al. (2000), our findings suggested that heightened stress reactivity may be adaptive for those low income urban youth who reported low levels of childhood maltreatment. It may be that responding to social evaluative stressors like the TSST with heightened reactivity is typically a healthy response for youth, allowing them to be aroused appropriately when needed, which may translate into better emotion regulation and interpersonal success. In contrast, for youth with relatively high levels of recalled or perceived past maltreatment, we found either a lack of association between stress response and adaptive outcomes or a negative association. When youth show heightened stress responses in the context of a non-supportive, maltreating environment, the consequences on emotion regulation may be negative with youth being less able to control emotion. This explanation is consistent with Ellis’s and Boyce’s theory, as well as empirical work that finds heightened reactivity to be only be a risk factor for maladjustment in adverse environments (Essex et al. 2011; Obradovic et al. 2010). Our findings were suggestive of this pattern but, contrary to expectations, significant associations only emerged for the relationship between heightened reactivity and anger regulation. It is noteworthy, that the significant associations we see occur for anger regulation and not interpersonal competence. Few studies have been done that look explicitly at interpersonal competence. Perhaps heightened reactivity is less problematic for behaviors that are more dyadic and have less of an emotional regulation component. Future research examining interpersonal competence during adolescence is important given the salience of peer relationships during this developmental period (Roisman et al. 2004).
It is also plausible that a lack of findings within the maltreated group occurred because youth who experience chronic maltreatment and chronic stress arousal over many years may develop a numbing or blunting of their stress arousal response (Gunnar and Vazquez 2001), leading to reduced range in stress response and ability to detect findings in this group. However, in the present study, we did not find that youth in the high maltreatment group showed decreased levels or range of stress response than the low maltreatment group. Nonetheless, emotional blunting in maltreated youth will be an important factor to consider in future studies of links between physiological arousal response and socio-emotional adjustment in maltreated youth.
Drawing on these findings, programs aimed to improve emotion regulation and interpersonal competence should target those youth with high stress reactivity who also have experienced maltreatment or other potential adverse experiences. Prevention approaches directed toward helping parents learn more adaptive emotional regulatory skills may also reduce the incidence of early maltreatment and/or neglect and thus impact adolescent development through impacting parental care and overall early environmental nurturing conditions.
Limitations
This study is not without limitations. Most notably, data were only collected at one point in time, and thus we cannot make claims regarding causality and direction of effects. This limits our ability to evaluate the claim from Boyce and Ellis’s theory that a trait-like reactivity develops as a product of both genetic and environmental conditions that shape individual differences in reactivity in other settings and developmental periods. To date, very few studies have examined the associations between stress reactivity and adolescents’ adjustment longitudinally and as such this area of research is a priority. We also were not able to assess at what point in time child maltreatment occurred because the CTQ asks youth to report on maltreatment experiences growing up as a child. Thus, we do not know if the context in which adolescents were currently in was one in which they were experiencing child maltreatment. Examining at what point in time maltreatment occurs is important because past research has suggested that the impact of child maltreatment on functioning may depend on the timing of maltreatment (Ireland et al. 2002; van Voorhees and Scarpa 2004). The use of retrospective reports also has been questioned as a valid assessment of child maltreatment (Hardt and Rutter 2004). However, the use of the CTQ during adolescence has been found to correlate highly with official reports of child maltreatment (Wolfe et al. 2001) and may not be as susceptible to recall bias as reports collected several years later during adulthood (Everson et al. 2008). Nonetheless, future research should collect more objective measures of child maltreatment, as well as assess the timing and duration of maltreatment for youth.
In the current study, we were interested in evaluating the premise that heightened reactivity may be associated with positive adjustment under supportive conditions and negative adjustment under adverse conditions. We did not, however, specifically examine whether adolescents who reported more supportive environments evidenced heightened reactivity that was associated with positive functioning. Thus, our findings may only be tapping into an absence of risk as opposed to assessing differences in supportive environments. Our results (Table 2) do indicate that those youth who reported lower child maltreatment also reported more positive parent–child relationships, less problems at school, and less perceived stress, which suggests that in our sample youth who reported less child maltreatment also experienced more supportive environments than those youth who reported more maltreatment.
We only modeled heightened stress reactivity as a function of peak-baseline, and thus did not model the entire stress response (baseline through recovery) nor did we examine blunted reactivity. Examining different patterns and trajectories of stress response (e.g., blunted vs. hyper-reactivity and peak vs. baseline and recovery) is an important area of research that may have implications for understanding the disparate findings on acute stress response and adjustment (Gunnar et al. 2009). As stated in the “Methods” section, we did attempt to run growth curve models of the full trajectory of stress response; however, these models did not statistically identify, potentially because of small sample size and multicollinearity among the data points. Future studies, with larger samples should examine different patterns and trajectories of acute stress response and the association with adolescents’ functioning.
Finally, a relatively small sample size may have resulted in underpowered multiple group models. SEM typically requires larger samples to obtain valid parameters, with recommendations of 100 participants needed to obtain reliable results (Thompson 2000). Our sample size per group was less than 100 (n’s = 86, 87). However, path models are not as complex as SEM models and may not need as many participants as fewer parameters are generally estimated. The rule of thumb for SEM is that valid parameters can be obtained with ratios of participants to parameters at a minimum of 5:1 (Thompson 2000). Following this, our sample size of 175 is adequate to allow estimation of 35 parameters. In our multiple group models, only 26 parameters were estimated (13 per group); thus, we were adequately powered.
Conclusion
This study broadens our understanding of how contextual influences interact with biological systems (e.g., stress response system) to affect adolescents’ adjustment. Findings suggest that heightened reactivity to stress is more of a vulnerability in highly stressful environments here children report child maltreatment but that in less stressful, environments heightened arousal is associated with interpersonal competence and anger regulation. Integration of biological, social, and clinical domains is important for pushing the field of adolescent development forward (Dahl 2004). Furthermore, findings from this study shed light on the role of child maltreatment in the relationship between heightened stress reactivity and adolescent adjustment. By studying potential moderators that impact the effect of stress reactivity on adjustment, we can inform intervention efforts by identifying at what level to intervene and for which youth intervention is needed.
References
Acock, A. C. (2005). Working with missing values. Journal of Marriage and Family, 67, 1012–1028.
Adam, E. K., & Kumari, M. (2009). Assessing salivary cortisol in large-scale, epidemiological research. Psychoneuroendocrinology, 34, 1423–1436.
Bell, B. G., & Belsky, J. (2007). Parenting and children’s cardiovascular functioning. Child: Care, Health and Development, 34, 194–203.
Bernstein, D. P., & Fink, L. (1998). Childhood trauma questionnaire: A retrospective self-report questionnaire and manual. San Antonio, TX: The Psychological Corporation.
Bernstein, D. P., Fink, L., Handelsman, L., Foote, J., Lovejoy, M., Wenzel, K., et al. (1994). Initial reliability and validity if a new retrospective measure of child abuse and neglect. American Journal of Psychiatry, 151, 1132–1136.
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., et al. (2003). Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse and Neglect, 27, 169–190.
Blackhart, G. C., Eckel, L. A., & Tice, D. M. (2007). Salivary cortisol in response to acute social rejection and acceptance by peers. Biological Psychology, 75, 267–276.
Boyce, W. T. (1996). Biobehavioral reactivity and injuries in children and adolescents. In M. H. Bornstein & J. Genevro (Eds.), Child development and behavioral pediatrics: Toward understanding children and health. Mahwah, NJ: Erlbaum.
Boyce, W. T., & Ellis, B. J. (2005). Biological sensitivity to context: I. An evolutionary- developmental theory of the origins and functions of stress reactivity. Development and Psychopathology, 17, 271–301.
Boyce, W. T., Essex, M. J., Alkon, A., Goldsmith, H. H., Kraemer, H. C., & Kupfer, D. J. (2006). Early father involvement moderates biobehavioral susceptibility to mental health problems in middle childhood. Journal of the American Academy of Child & Adolescent Psychiatry, 45, 1510–1520.
Bradley, S. J. (2000). Affect regulation and the development of psychopathology. New York: Guilford.
Buhrmester, D. (1990). Intimacy of friendship, interpersonal competence, and adjustment during preadolescence and adolescence. Child Development, 61, 1101–1111.
Buske-Kirschbaum, A., Jobst, S., Wustmans, A., Kirschbaum, C., Rauh, W., & Hellhammer, D. (1997). Attenuated free cortisol response to psychosocial stress in children with atopic dermatitis. Psychosomatic Medicine, 59, 419–426.
Byrne, B. M. (2001). Structural equation modeling with AMOS: Basic concepts, applications, and programming. Mahwah, NJ: Erlbaum.
Casey, B., Jones, R. M., Levita, L., Libby, V., Pattwell, S. S., Ruberry, E. J., Soliman, F., & Somerville, L. H. (2010). The storm and stress of adolescence: insights from human imaging and mouse genetics. Developmental Psychobiology, 52, 225–235.
Chaplin, T. M., Freiburger, M. B., Mayes, L. C., & Sinha, R. (2010). Prenatal cocaine exposure, gender, and adolescent stress response: A prospective longitudinal study. Neurotoxicology and Teratology, 32, 595–604.
Cicchetti, D., & Rogosch, F. A. (2001). The impact of child maltreatment and psychopathology on neuroendocrine functioning. Development and Psychopathology, 13, 783–804.
Dahl, R. E. (2004). Adolescent brain development: a period of vulnerabilities and opportunities. Annual New York Academy of Sciences, 1021, 1–22.
Demir, M., & Urberg, K. (2004). Friendship and adjustment among adolescents. Journal of Experimental Child Psychology, 88, 68–82.
Dodge, K. A., & Pettit, G. S. (2003). A biopsychosocial model of the development of chronic conduct problems in adolescence. Developmental Psychology, 39, 349–371.
Ellis, B. J., & Boyce, W. T. (2008). Biological sensitivity to context. Current Directions in Psychological Science, 17, 183–187.
Ellis, B. J., Essex, M. J., & Boyce, W. T. (2005). Biological sensitivity to context: II. Empirical explorations of an evolutionary-developmental theory. Development and Psychopathology, 17, 303–328.
Ellis, B. J., Shirtcliff, E. A., Boyce, W. T., Deardorff, J., & Essex, M. J. (2011). Quality of early family relationships and the timing and tempo of puberty: Effects depend on biological sensitivity to context. Development and Psychopathology, 23, 85–99.
Essex, M. J., Armstrong, J. M., Burk, L. R., Goldsmith, H. H., & Boyce, W. T. (2011). Biological sensitivity to context moderates the effects of the early teacher-child relationship on the development of mental health by adolescence. Development and Psychopathology, 23, 149–161.
Everson, M. D., Smith, J. B., Hussey, J. M., English, D., Litrownik, A. J., Dubowitz, H., et al. (2008). Concordance between adolescent reports of childhood abuse and child protective service determinations in an at-risk sample of young adolescents. Child Maltreatment, 13, 14–26.
Granger, D. A., & Kivlighan, K. T. (2003). Integrating biological, behavioral, and social levels of analysis in early child development: Progress, problems, and prospects. Child Development, 74, 1058–1063.
Granger, D. A., Weisz, J. R., McCracken, J. T., Ikeda, S. C., & Douglas, P. (1996). Reciprocal influences among adrenocortical activation, psychosocial processes, and the behavioral adjustment of clinic-referred children. Child Development, 67, 3250–3262.
Gunnar, M. R., & Vazquez, D. M. (2001). Low cortisol and a flattening of expected daytime rhythm: Potential indices of risk in human development. Development and Psychopathology, 13, 515–538.
Gunnar, M., Bruce, J., & Donzella, B. (2000). Stress physiology, health, and behavioral development. In A. Thronton (Ed.), The well-being of children and families: Research and data needs (pp. 188–212). Ann Arbor, MI: University of Michigan Press.
Gunnar, M. R., Frenn, K., Wewerka, S. S., & Ryzin, M. J. (2009). Moderate versus severe early life stress: Associations with stress reactivity and regulation in 10–12 year-old children. Psychoneuroendocrinology, 34, 62–75.
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45, 260–273.
Harold, G. T., Shelton, K. H., Goeke-Morey, M. C., & Cummings, E. M. (2004). Marital conflict, child emotional security about family relationships and child adjustment. Social Development, 13, 350–376.
Hart, J., Gunnar, M., & Cicchetti, D. (1996). Altered neuroendocrine activity in maltreated children related to symptoms of depression. Development and Psychopathology, 8, 201–214.
Henseler, J., & Fassott, G. (2010). Testing moderating effects in PLS path models: An illustration of available procedures. In V. Esposito, J. Chin, & H. Wang (Eds.), Handbook of partial least squares: Concepts, methods, and applications. Berlin: Springer.
Ireland, T. O., Smith, C. A., & Thornberry, T. P. (2002). Developmental issues in the impact of child maltreatment on later delinquency and drug use. Criminology, 40, 359–400.
Jackson, R. W., Treiber, F. A., Turner, J. R., Davis, H., & Strong, W. B. (1999). Effects of race, sex, and socioeconomic status upon cardiovascular stress responsively and recovery in youth. International Journal of Psychophysiology, 31, 111–119.
Kline, R. B. (2005). Principles and practice of structural equation modeling. New York, NY: Guilford Press.
Kobak, R., Zajac, K., & Levine, S. (2009). Cortisol and antisocial behavior in early adolescence: The role of gender in an economically disadvantaged sample. Developmental and Psychopathology, 21, 579–591.
Kudielka, B. M., Buske-Kirschbaum, A., Hellhammer, D. H., & Kirschbaum, C. (2004). Differential heart rate reactivity and recovery after psychosocial stress (TSST) in healthy children, younger adults, and elderly adults: The impact of age and gender. International Journal of Behavioral Medicine, 2, 116–121.
McClelland, G. H., & Judd, C. M. (1993). Statistical difficulties of detecting interactions and moderator effects. Psychological Bulletin, 114, 376–390.
McEwen, B. S. (2007). Physiology and Neurobiology of stress and adaptation: Central role of the brain. Physiological Review, 87, 873–904.
Miller, A. L., Seifer, R., Stroud, L., Sheinkopf, S. J., & Dickstein, S. (2006). Bio behavioral indices of emotion regulation relate to school attitudes, motivation, and behavior problems in a low-income preschool sample. Annals of the New York Academy of Sciences, 1094, 325–329.
Natsuaki, M. N., Klimes-Dougan, B., Xiaojia, G., Shirtcliff, E. A., Hastings, P. D., & Zahn-Waxler, C. (2009). Early pubertal maturation and internalizing problems in adolescence: Sex differences in the role of cortisol reactivity to interpersonal stress. Journal of Clinical Child and Adolescence Psychology, 38, 513–524.
Nicholas, T. R., Mahadeo, M., Bryant, K., & Botvin, G. J. (2008). Examining anger as a predictor of drug use among multiethnic middle school students. Journal of School Health, 78, 480–486.
Obradovic, J., Bush, N. R., Stamperdahl, J., Adler, N. E., & Boyce, W. T. (2010). Biological sensitivity to context: The interactive effects of stress reactivity and family adversity on socioemotional behavior and school readiness. Child Development, 81, 270–289.
Reiss, D., Neiderhiser, J. M., Hetherington, E. M., & Plomin, R. (2000). The relationship code: Deciphering genetic and social influences on adolescent development. Cambridge, MA: Harvard University Press.
Reynolds, C. R. (2010). Behavior assessment system for children. Corsini encyclopedia of psychology. Hoboken, NJ: Wiley.
Reynolds, C. R., & Kaphaus, R. W. (2002). The clinician’s guide to the behavior system for children (BASC). New York: Guilford.
Roisman, G. I., Masten, A. S., Coatsworth, J. D., & Tellegen, A. (2004). Salient and emerging developmental tasks in the transition to adulthood. Child Development, 75, 123–133.
Stein, S., Watson, S. T., & Wickshom, K. (2007). Review of the behavior assessment system for children. Mental measurements yearbook, 18. Retrieved on-line http://web.ebscohost.com/ehost/detail?vid=3&hid=112&sid=1bc62445-0879-4e14-9fd4-e8f5a56df88b%40sessionmgr104&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=mmt&AN=TIP18193503.
Susman, E. J. (2006). Psychobiology of persistent antisocial behavior: Stress early vulnerabilities and the attenuation hypothesis. Neuroscience and Biobehavioral Review, 30, 376–389.
Susman, E. J., Dockray, S., Dorn, L. D., Schiefelbein, V. L., Herwehe, S., & Heaton, J. A. (2007). Morningness/eveningness, morning–to–afternoon cortisol ratio, and antisocial behavior problems during puberty. Developmental Psychology, 43, 811–822.
Thompson, B. (2000). Ten commandments of structural equation modeling. In L. G. Grimm & P. R. Yarnold (Eds.), Reading and understanding more multivariate statistics (pp. 261–285). Washington, DC: American Psychological Association.
Tomarken, A. J., & Waller, N. (2005). Structural equation modeling: Strengths, limitations, and misconceptions. Annual Review of Clinical Psychology, 1, 31–65.
Tout, K., Haan, M., Campbell, E. K., & Gunnar, M. R. (1998). Social behavior correlates of cortisol activity in child care: Gender differences and time-of-day effects. Child Development, 69, 1247–1262.
van Goozen, S. H. M., Fairchild, G., Snoek, H., & Harold, G. T. (2007). The evidence for a neurobiological model of childhood antisocial behavior. Psychological Bulletin, 133, 149–182.
van Voorhees, E., & Scarpa, A. (2004). The effects of child maltreatment on the hypothalamic- pituitary-adrenal axis. Trauma Violence Abuse, 5, 333–352.
Wolfe, D. A., Scott, K., Wekerle, C., & Pittman, A. (2001). Child maltreatment: Risk of adjustment problems and dating violence in adolescence. Journal of American Academy of Child and Adolescent Psychiatry, 40, 282–289.
Acknowledgments
Support for this project and time working on this manuscript was provided by the National Institutes of Health (NIH) through grants T32DA019426 (Cook), K01-DA-024759 (Chaplin), P50-DA-16556 (Sinha), R01-DA-06025 (Mayes), R01-DA-017863 (Mayes), KO5-DA-020091 (Mayes), and a grant from the Gustavus and Louise Pfeiffer Research Foundation (Mayes). The study sponsors had no involvement in the study design; collection, analysis, and interpretation of data; the writing of the manuscript; or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cook, E.C., Chaplin, T.M., Sinha, R. et al. The Stress Response and Adolescents’ Adjustment: The Impact of Child Maltreatment. J Youth Adolescence 41, 1067–1077 (2012). https://doi.org/10.1007/s10964-012-9746-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-012-9746-y