
Abstract
A descriptive cross-sectional survey was conducted over 5 months in two tertiary hospitals in Riyadh, Saudi Arabia. The 5-month period was from November 2014 to March 2015. The survey instrument used was a Short-Form Health Survey SF-36 (the RAND 36-item) questionnaire that measure QOL of the caregivers. Our study subjects included 289 randomly selected Saudi caregivers. Almost all the mean scores were increased (higher than 50) with the exception of levels of energy/fatigue. Role functioning/physical scored the highest (81.02 ± 35.33) followed by physical functioning (76.34 ± 29.83). Other domains of QOL scored (71.02 ± 35.33) for the role functioning/emotional; pain (71.15 ± 28.48), emotional well-being (60.58 ± 18.44); social functioning (58.39 ± 25.83), and general health (54.32 ± 17.08). In multivariate regression analysis, the model predicts that the contributions of age, gender, and the cancer type of patients were a statistically significant predictor with the QOL domains of caregivers. Cancer caregivers in Saudi Arabia caring for patients more than 1 year after diagnosis reported favorable QOL. Factors associated with QOL domains included age, gender of the caregivers, and the types of cancer patients. These findings are encouraging as a baseline for providing more information to future studies in QOL of caregivers.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Health-related quality of life refers to aspects of a person’s self-concept of well-being that are affected by disease or treatment (Mercedes et al. 2011). Cancer is a disease that negatively impacts the health-related quality of life (HRQOL) of patients as well as family caregivers (Clark et al. 2003, 2013; Rummans et al. 2006). Tending to cancer patients poses psychological, emotional, and physical challenges for caregivers (Shahi et al. 2014). Caring for patients with chronic diseases such as cancer requires considerable time, effort and emotional expenditure, which could lead to highly stressful and burdensome quality of life for caregivers (Amendola et al. 2011). Studies show that a family caregiver looking after a cancer patient is likely to have significant levels of anxiety and depression (Badger et al. 2007; Mantani et al. 2007; Wilson et al. 2007). Aside from psychological issues, family caregivers also experience physical health problems such as fatigue, lack of self-care, and sleep deprivation (Mosher et al. 2013; Schulz and Sherwood 2008). Furthermore, several studies also show that caregivers have a higher risk of mortality and physical and mental problems than non-caregivers (Song et al. 2011; Rhee et al. 2008). The impact of cancer on the HRQOL of family caregivers may also have a negative effect on their ability to care for and support their patients (Khanjari et al. 2014). This population who are considered as a key actor in the provision of health care among cancer patients are often goes unnoticed. Caregivers are considered the “hidden patients” and are usually the unseen victims of the disease (Wilkinson and Lynn 2005).
Health-related quality of life (HRQOL) refers to a multidimensional assessment of physical, emotional, and social domains of a caregiver’s health or disease status (CDC 2014). The subjectively perceived quality of life of caregivers is often evaluated using health-related quality of life (HRQOL) questionnaires. Various studies in different countries have measured HRQOL to determine the perceived health status of a caregiver (Awadalla et al. 2007; Sjolander et al. 2012; Yang et al. 2012). Measuring and analyzing HRQOL can identify the burden of preventable disease and injuries as well as it can also provide helpful insights into the relationships between HRQOL and risk factors (CDC 2014).
Previous studies done on measuring HRQOL of family caregivers have been conducted during palliative care which starts from the patient’s diagnosis to the point where the patient is close to death or has died (Persson et al. 2008; Ringdal et al. 2004). Several tools were also developed and tested in order to measure HRQOL such as the European Organization for Research and Treatment of Cancer Quality of Life Questionnaires (QLQs), 36-Item Short-Form Health Survey (SF-36), and Caregiver Quality of Life Index-Cancer (CQOLC), Eastern Cooperative Oncology Group (ECOG) Performance Status Rating (PSR) (Duan et al. 2015; Edwards and Ung 2002; Oliver and Greenberg 2009; Li et al. 2003; van AndelG et al. 2008). These questionnaires are the most widely and increasingly used in clinical practice and clinical trials in this population.
Family caregivers play a crucial role in the palliative care of cancer patients. They provide care for their loved one and deal with a huge challenge in coping with a variety of physical, social, and economic problems during the caregiving process. Various research has been done among cancer patients but less is known with their family caregivers. In the Kingdom of Saudi Arabia, no study has been done determining the HRQOL among family caregivers. Since the family system is considered the most important social institution in the Saudi Arabia, which maintain primary responsibility for the care of those afflicted with this long-term disease. We considered that it would be ideal to identify issues affecting HRQOL of the family caregivers, who are the key actors in supporting cancer patients and in the palliative treatment of care. Identifying these issues will provide and raise the awareness of healthcare professionals for the primary caregivers of people with cancer. This will also help in formulating a policy that will provide support and interventions for caregivers. Furthermore, with the increasing rate of cancer in the Kingdom, the burden associated with being primary caregivers for cancer patients is expected to increase in 2030 among middle-aged and elderly (Ibrahim et al. 2008). As a result of this increase, the health-related quality of life in caregivers may also be at risk. We hypothesized that younger caregivers who provided help to their relatives would report poorer functioning levels of QOL. We also hypothesized that there is no association between the caregivers’ quality of life and the demographic characteristics as well as patients’ type of cancer.
In light of the emotional toll exacted on caregivers of cancer patients, this study was designed to identify health-related quality of life (HRQOL) of caregivers of Saudi cancer patients more than 1 year after diagnosis.
Methods
Design and Setting
A descriptive cross-sectional survey was conducted at two hospitals (King Khalid University Hospital and King Fahad Medical City Hospital) in Riyadh, Saudi Arabia. These hospitals are considered the largest in Riyadh, Saudi Arabia. Ethical approval was obtained from the Ethics Committee of King Saud University, Riyadh, Saudi Arabia (CAMS 15/3536). The approval of the Institutional Review Board (IRB) committee of each hospital was also obtained prior to distribution of the survey.
Participants
To be eligible, participants had to be 18 or older, possess the ability to speak and understand either Arabic or English language, and have a relative diagnosed with cancer at least 1 year ago. Non-Saudis and those unwilling to participate were excluded from the study.
Procedure
The survey was conducted from November 2014 to March 2015. Patients’ information was taken from the existing database of each hospital. The patients were randomly selected and contacted by nurses working under the supervision of family medicine physicians. Patients had to be willing to give information about their closest family member or primary caregivers. The chosen caregiver was then invited to participate in the study. Each participant was asked for his or her next schedule of hospital or primary healthcare center visits. A trained researcher was contracted to distribute the questionnaire and interact with the participants. Verbal/written informed consent was obtained prior to inclusion. Included participants were informed prior to filling out the survey that they could decline and had an option of not completing the questionnaire. All participants were also informed that they could choose to remain anonymous and no names were needed to ensure confidentiality.
Instruments
A Short-Form Health Survey SF-36 (the RAND 36-item) instrument was used to measure HRQOL of the family caregivers (Lowrie et al. 2003). This instrument is one of the most widely used tool to assess HRQOL which consists of 36 items that measure the self-reported levels of physical functioning, bodily pain, role limitations due to physical condition, energy/fatigue, role limitation due to emotional condition, social functioning, emotional well-being, and perceptions of general health of caregivers. The questions about physical health were represented by the Physical Component Summary (PCS), physical functioning, and role limitations due to physical problems, body pain, and general health. Questions related to mental health were represented by the Mental Component Summary Score (MCS), which consists of social functioning, vitality, role limitations due to emotional problems, and mental health. The questionnaire was an Arabic language translated and was supplemented with a scoring manual which was followed by the researchers. Arabic language version is reliable, and it is similar to the English language version (Lazenby and Khatib 2012). Each response of the participants was recorded and transformed through a description in order to give score between 0 and 100. Items in the same scale are averaged together to create the eight scales (physical functioning, and role limitations due to physical problems, body pain and general health, social functioning, vitality, role limitations due to emotional problems and mental health). Average of the scale scores represents the answer of the respondent. A high score defines a more favorable health state, thus higher level of function.
Data Analysis
Statistical analyses were carried out using SPSS 22.0 for Windows software (SPSS Inc., Chicago, IL, USA). The eight scales of QOL were calculated according to the given standard SF-36 algorithms. All raw scores were coded, re-calibrated, summated, and transformed from 0 to 100 for each item, with higher scores indicating better QOL. Linear regression was done to assess the significance of predictors and compute the coefficient of determination. A p value <0.05 was considered statistically significant.
Results
Demographics Characteristics
A total of 289 caregivers participated in this study. Table 1 presents the demographic characteristics of the caregivers. In this cross-sectional study, there was a predominance of female caregivers (65.1 %), and the majority of the caregivers (55.4 %) had completed a secondary education. The mean age of the caregivers was 31.22 ± 10.9 (M ± SD). Thirty-six percent of the participants earned 3000–5000 Saudi Riyal which consider in a minimum wage of a Saudi national. Of the 289 participants, 86.5 % of the caregivers were patient related: 36.3 % were patients’ son/daughter, 23.2 % husband/wife, 22.5 % father/mother, and 4.5 % grandson/daughter. 13.5 % are cared professionals such as nurses. The majority of the patients were female (60.2 %) and had a mean age of 52.82 (SD 10.3). Breast cancer was the most common (23.5 %) cancer among the patients followed by colon cancer (19 %) and other diagnosis (16.3 %) such as non-Hodgkin’s lymphoma. Fifty percent of the patients had an advanced cancer stage.
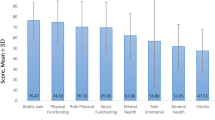
Quality of Life of Caregivers
Table 2 shows the component scores of the quality of life of the caregivers. The higher scores of quality of life domains indicate better functioning. Energy/fatigue scored (49.91 ± 23.80) the lowest among the domains of quality of life followed by the general health (54.32 ± 17.08). Role functioning/physical scored the highest (81.02 ± 35.33) then physical functioning (76.34 ± 29.83) indicating better functioning of the caregivers. Furthermore, the role functioning/emotional scored (71.02 ± 35.33); emotional well-being (60.58 ± 18.44); social functioning (58.39 ± 25.83); and pain (71.15 ± 28.48).
Factors Associated with QOL Scale Scores
Tables 3 and 4 present the factors associated with QOL scale scores. In multivariate regression analysis, the model predicts that gender was a statistically significant predictor of role functioning (P = 0.011), energy/fatigue (P = 0.003), and social functioning (P = 0.030). Differences in means of physical functioning were significant among categories of age (P = 0.001), educational level (P = 0.004), and cancer type (P = 0.000). In other words, greater difficulty in physical functioning was noticed across the caregivers’ age, educational level, and patient’s cancer diagnosis. The regression analysis also found that emotional well-being (P = 0.000), social functioning, and general health (P = 0.002) of the caregiver were a statistically significant predictor of the patient relationship. Furthermore, gender (P = 0.030) and age (P = 0.000) were found a significant predictor of social functioning (P = 0.05). Female caregivers had significantly less functioning scores than male caregivers in terms of the role of emotional, energy/fatigue, emotional well-being, pain, and general health. Older caregivers had significantly lower functioning scores in the physical component summary. The results also found that cancer type was a significant predictor in domains of health change in the caregivers (P = 0.049). Other demographic factors were not found to be significant predictors in QOL in this study.
Discussion
Several studies show that the effect of caregiving for cancer patients has a deleterious effect on the quality of life of the caregivers (Obaidi and Al-Atiyyat 2013; Vrettos et al. 2012). The present study provides an overview of the quality of life of caregivers in Saudi Arabia. The results of the present study indicate that cancer caregivers in 1 year after diagnosis of cancer displayed better functioning levels of QOL. Almost all the mean scores were increased (higher than 50) with the exception of levels of energy/fatigue. Our findings were similar to the study done in the USA that reported the QOL of life in primary caregivers at 2 years after the diagnosis (Kim and Spillers 2010). The low level of energy found in our study is also in agreement with a study carried out in Australia among home caregivers of persons with advanced cancer (Aranda and Hayman-White 2001).
A number of factors may explain the results found in the present study. First, the extended family pattern: In Saudi Arabia, the patient is considered as one member of the larger family, and the family is responsible for the patients. The treatment of patients is usually consented to by the family to avoid distressing the patient emotionally. Such a practice helps family members feel that they are protecting and supporting the patient as well as securing his or her well-being (Choong and Chandia 2013). For example, futile treatment or a continued delivery of medical care even if there is no reasonable hope of a cure or benefit, is often advocated by many and requested by relatives (O’Kelly et al. 2011). Based on Islamic law, a family member is permitted to withdraw or withhold futile treatment or disproportionate treatment, allowing death to take its natural course (Choong and Chandia 2013; Sachedina 2005; Zahedi et al. 2007). Second, the health system in the Kingdom, where health services are free, can improve domains of QOL of the caregivers. Since some aspects of the present study were associated with improved QOL, it is notable to heighten the level of energy/fatigue among caregivers. Future investigated studies are needed for energy/fatigue of caregivers over the course of cancer in over 1 year after diagnosis as well as at 5 years and late stage of diagnosis. In a comparative study between caregivers of cancer patients in the palliative and curative phase, it was found that caregivers caring for patients in the palliative phase reported lower QOL than caregivers in the curative phase (Valeberg and Grov 2013).
Other highlights of the present study were the predictor that may affect the QOL of caregivers for the person diagnosed with cancer at least 1 year ago. We examined demographic and QOL domains of the caregivers. Our findings show the significant contribution of gender, age, educational level, income–patient relationship, and cancer type of patients to domains of QOL. The contributions of age, gender, and the cancer types of patients with the domains QOL of caregivers highlight the present study. The type of cancer ailing patients is a significant predictor that may affect the QOL of patients. We also found evidence that cancer stage of patients is shown as a predictor that may affect physical QOL as well as health behavior of caregivers (Lu et al. 2010). Furthermore, the present study found that gender as significant predictors in caregivers QOL. Previous studies show that female caregivers are more affected involving social functioning while male caregivers, particularly husbands of patients, are more distressed about work related and financial issues (Kim et al. 2006). In addition, gender, particularly females’ caregivers had greater influence on the association between depressive symptoms and QOL (Kim et al. 2015). Since cancer exerts a significant burden on the QOL of caregivers, it only suggests that both cancer patients and their caregivers should be included in programs that are sensitive to the role of gender and will enhance their ability in dealing and managing the disease. It is also worth mentioning that monthly income elucidate significant contributions to the domains of role functioning/emotional, even though, the medical expenses of the patients were supported by the government.
Regarding the age of caregivers, a significant relation was found among the domains of physical functioning, energy/fatigue, social functioning, pain, general health, and levels of health change in the caregivers. One of the reasons may be due to the fact that the majority of the caregivers are at the age of 30 years old, and most of them are under less pressure to worry about the family responsibilities and medical expenses because they were sons/daughters of the patient.
The role of caregivers is essential and considered as one of the components of effective cancer management (Given et al. 2001). Most physicians include family caregivers in the course of treatment of the patients, such as treatment planning, decision making, and implementation (Glajchen 2004; Hudson et al. 2004). QOL of caregivers is often neglected by putting the patients’ needs first. In addition, caregivers, particularly family caregivers, usually begin their roles without training and are expected to meet many demands without much support and assistance. This reason may induce greater distress and depression and low QOL of the caregivers. Counseling or educational programs are needed to increase the level of competence of these caregivers.
The study is limited in terms of the design of the survey. The cross-sectional design of the study precludes the causation of the findings. Secondly, the present study is limited in terms of sample size which is not fully a representative of the country. Third, the study is based on self-response that may introduce biases from participants. Lastly, we examined only basic demographics of caregivers and QOL domains, and the effect size in the regression model was small to modest. It will also be worthwhile for future studies to investigate caregivers caring for patients at advanced and late stages of diagnosis and include other predictors of QOL such as behavior (e.g., healthy diet) and physical activity such as exercise. However, the author does believe that this study can help and be considered as a baseline findings for future studies in monitoring the QOL of caregivers.
Conclusion
Cancer caregivers in Saudi Arabia reported favorable quality of life. They showed better functioning on QOL domains of emotional well-being, role functioning/emotional, pain, social functioning, physical functioning, general health, and role functioning/physical. Energy/fatigue was the lowest score among the QOL domains indicating caregivers may be at risk of poorer quality of life when the time and the disease will advance. Cancer has been considered as a chronic disease, long-term impact of this disease on caregivers QOL should be monitored.
Regarding the predictors of QOL, the present study revealed that certain socio-demographic and clinical characteristics of patients can predict and have statistically significant effects on the QOL of caregivers. Age and gender of caregivers coupled with the type of cancer afflicting the patients affect most of the QOL of the caregivers. This study provides an overview of the caregivers QOL whose caring for patients at 1 year after diagnosis. It will also be important to conduct further studies among caregivers caring for cancer patients in advanced and late stage of cancer.
References
Amendola, F., Oliveira, M. A., & Alvarenga, M. R. (2011). Influence of social support on the quality of life of family caregivers while caring for people with dependence. Revista da Escola de Enfermagem da USP, 45(4), 884–889.
Aranda, S. K., & Hayman-White, K. (2001). Home caregivers of the person with advanced cancer: An Australian perspective. Cancer Nursing, 24, 300–307.
Awadalla, A. W., Ohaeri, J. U., Gholoum, A., Khalid, A. O., Hamad, H. M., & Jacob, A. (2007). Factors associated with quality of life of outpatients with breast cancer and gynecologic cancers and their family caregivers: A controlled study. BMC Cancer, 7, 102.
Badger, T., Segrin, C., Dorros, S. M., Meek, P., & Lopez, A. M. (2007). Depression and anxiety in women with breast cancer and their partners. Nursing Research, 56, 44–53.
Centers for Disease Control and Prevention (CDC). Health-related quality of life (HRQOL) concepts. Accessed Nov 2014. http://www.cdc.gov/hrqol/concept.htm.
Choong, K., & Chandia, M. (2013). Technology at the end of life: “Medical futility” and the Muslim PVS patient. International Review of Law, 2013, 9. doi:10.5339/irl.2013.9.
Clark, M. M., Bostwick, J. M., & Rummans, T. A. (2003). Group and individual treatment strategies for distress in cancer patients. Mayo Clinic Proceedings, 78(12), 1538–1543.
Clark, M. M., Rummans, T. A., Atherton, P. J., Cheville, A. L., Johnson, M. E., Frost, M. H., et al. (2013). Randomized controlled trial of maintaining quality of life during radiotherapy for advanced cancer. Cancer, 119(4), 880–887.
Duan, J., Fu, J., Gao, H., Chen, C., Fu, J., Shi, X., & Liu, X. (2015). Factor analysis of the caregiver quality of life index-cancer (CQOLC) scale for chinese cancer caregivers: A preliminary reliability and validity study of the CQOLC-Chinese version. PLoS One 10(2), e0116438. http://doi.org/10.1371/journal.pone.0116438.
Edwards, B., & Ung, L. (2002). Quality of life instruments for caregivers of patients with cancer: A review of their psychometric properties. Cancer Nursing, 25(5), 342–349.
Given, B. A., Given, C. W., & Kozachik, S. (2001). Family support in advanced cancer. CA: A Cancer Journal for Clinicians, 51, 213–231. doi:10.3322/canjclin.51.4.213.
Glajchen, M. (2004). The emerging role and needs of family caregivers in cancer care. Journal of Supportive Oncology, 2(2), 145–155.
Hudson, P. L., Aranda, S., & Kristjanson, L. J. (2004). Meeting the supportive needs of family caregivers in palliative care: Challenges for health professionals. Journal of Palliative Medicine, 7(1), 19–25.
Ibrahim, E., Bin, S., Banjar, L., Awadalla, S., & Abomelha, M. S. (2008). Current and future cancer burden in Saudi Arabia: Meeting the challenge. Hematology/Oncology and Stem Cell Therapy, 1, 210–215.
Khanjari, S., Langius-Eklöf, A., Oskouie, F., & Sundberg, K. (2014). Family caregivers of women with breast cancer in Iran report high psychological impact 6 months after diagnosis. European Journal of Oncology Nursing,. doi:10.1016/j.ejon.2014.06.002.
Kim, Y., Loscalzo, M. J., Wellisch, K., & Spillers, R. L. (2006). Gender differences in caregiving stress among caregivers of cancer survivors. Psycho-Oncology, 15, 1086–1092. doi:10.1002/pon.1049.
Kim, Y., & Spillers, R. L. (2010). Quality of life of family caregivers at 2 years after a relative’s cancer diagnosis. Psychooncology, 19(4), 431–440. doi:10.1002/pon.1576.
Kim, Y., van Ryn, M., Jensen, R. E., Griffin, J. M., Potosky, A., & Rowland, J. (2015). Effects of gender and depressive symptoms on quality of life among colorectal and lung cancer patients and their family caregivers. Psychooncology, 24(1), 95–105. doi:10.1002/pon.3580.
Lazenby, M., & Khatib, J. (2012). Associations among patient characteristics, health-related quality of life, and spiritual well-being among Arab Muslim cancer patients. Journal of Palliative Medicine, 15(12), 1321–1324. doi:10.1089/jpm.2012.0208.
Li, L., Wang, H. M., & Chen, Y. S. (2003). Chinese SF-36 health survey: Translation, culture adaption, validation, and normalisation. Journal of Epidemiology and Community Health, 57(4), 259–263.
Lowrie, E. G., Curtin, R. B., LePain, N., & Schatell, D. (2003). Medical outcomes study short form-36: A consistent and powerful predictor of morbidity and mortality in dialysis patients. American Journal of Kidney Diseases, 41(6), 1286–1292.
Lu, L., Pan, B., Sun, W., Cheng, L., Chi, T., & Wang, L. (2010). Quality of life and related factors among cancer caregivers in China. Psychiatry and Clinical Neurosciences, 64, 505–513. doi:10.1111/j.1440-1819.2010.02131.
Mantani, T., Saeki, T., Inoue, S., Okamura, H., Daino, M., Kataoka, T., & Yamawaki, S. (2007). Factors related to anxiety and depression in women with breast cancer and their husbands: Role of alexithymia and family functioning. Supportive Care in Cancer, 15(7), 859–868.
Mercedes, M. P., Raquel, B. G., Cinthya, R. C., & Gloria, R. G. (2011). Assessment of health-related quality of life: The Cinderella of peritoneal dialysis? International Journal of Nephrology, 2011, 8. doi:10.4061/2011/528685.
Mosher, C. E., Bakas, T., & Champion, V. L. (2013). Physical health, mental health, and life changes among family caregivers of patients with lung cancer. Oncology Nursing Forum, 40(1), 53–61. doi:10.1188/13.ONF.53-61.
O’Kelly, C. D., Urch, C., & Brown, E. A. (2011). The impact of culture and religion on truth telling at the end of life Nephrol. Dialysis & Transplantation, 26, 3838–3842.
Obaidi, J. G., & Al-Atiyyat, N. M. (2013). Quality of life among primary caregivers of women with breast cancer: A review. Middle East Journal of Cancer, 4, 45–49.
Oliver, A., & Greenberg, CC. (2009). Measuring outcomes in oncology treatment: The importance of patient-centered outcomes. The Surgical Clinics of North America, 89(1), 17–vii. http://doi.org/10.1016/j.suc.2008.09.015.
Persson, C., Ostlund, U., Wennman-Larsen, A., Wengstrom, Y., & Gustavsson, P. (2008). Health-related quality of life in significant others of patients dying from lung cancer. Palliative Medicine, 22, 239–247.
Rhee, Y. S., Yun, Y. H., Park, S., Shin, D. O., Lee, K. M., Yoo, H. J., et al. (2008). Depression in family caregivers of the elderly: The feeling of burden as a predictor of depression. Journal of Clinical Oncology, 26, 5890–5895.
Ringdal, G. I., Ringdal, K., Jordhoy, M. S., Ahlner-Elmqvist, M., Jannert, M., & Kaasa, S. (2004). Health-related quality of life (HRQOL) in family members of cancer victims: Results from a longitudinal intervention study in Norway and Sweden. Palliative Medicine, 18, 108–120.
Rummans, T. A., Clark, M. M., Sloan, J. A., Frost, M. H., Bostwick, J. M., Atherton, P. J., et al. (2006). Impacting quality of life for patients with advanced cancer with a structured multidisciplinary intervention: A randomized controlled trial. Journal of Clinical Oncology, 24(4), 635–642.
Sachedina, A. (2005). End-of-life: The Islamic view. Lancet, 366, 774–779.
Schulz, R., & Sherwood, P. R. (2008). Physical and mental health effects of family caregiving. The American Journal of Nursing, 108(9 Suppl), 23–27. doi:10.1097/01.NAJ.0000336406.45248.4c.
Shahi, V., Lapid, M. I., Kung, S., Atherton, P. J., Sloan, J. A., Clark, M. M., & Rummans, T. A. (2014). Do age and quality of life of patients with cancer influence quality of life of the caregiver? Journal of Geriatric Oncology, 5(3), 331–336. doi:10.1016/j.jgo.2014.03.003.
Sjolander, C., Rolander, B., Järhult, J., Mårtensson, J., & Ahlstrom, G. (2012). Health-related quality of life in family members of patients with an advanced cancer diagnosis: A one-year prospective study. Health and Quality of Life Outcomes, 10, 89. doi:10.1186/1477-7525-10-89.
Song, J. I., Shin, D. W., Choi, J. Y., Kang, J., Baik, Y. J., Mo, H., et al. (2011). Quality of life and mental health in family caregivers of patients with terminal cancer. Supportive Care in Cancer, 19(10), 1519–1526.
Valeberg, B. T., & Grov, E. K. (2013). Symptoms in the cancer patient: Of importance for their caregivers’ quality of life and mental health? European Journal of Oncology Nursing, 17(1), 46–51. doi:10.1016/j.ejon.2012.01.009.
van AndelG, Bottomley A., Fossa, S. D., Efficace, F., Coens, C., Guerif, S., et al. (2008). An international field study of the eEORTCQLQ-PR25: A questionnaire for assessing the health-related quality of life of patients with prostate cancer. European Journal of Cancer, 44, 2418–2424.
Vrettos, I., Kamposioras, K., Kontodimopoulos, N., Pappa, E., Georgiadou, E., Haritos, D., et al. (2012). Comparing health-related quality of life of cancer patients under chemotherapy and of their caregivers. The Scientific World Journal,. doi:10.1100/2012/135283.
Wilkinson, A. M., & Lynn, J. (2005). Caregiving for advanced chronic illness patients. Techniques in Regional Anesthesia and Pain Management, 9, 122–132.
Wilson, K. G., Chochinov, H. M., Graham Skirko, M., Allard, P., Chary, S., Gagnon, P. R., et al. (2007). Depression and anxiety disorders in palliative cancer care. Journal of Pain and Symptom Management, 33, 118–129.
Yang, X., Hao, Y., George, S. M., & Wang, L. (2012). Factors associated with health-related quality of life among Chinese caregivers of the older adults living in the community: A cross-sectional study. Health and Quality of Life Outcomes, 10, 143. doi:10.1186/1477-7525-10-143.
Zahedi, F., Larijani, B., & Tavakoly Bazzaz, J. (2007). End of life ethical issues and Islamic views. Iranian Journal of Allergy, Asthma and Immunology, 6, 5–15.
Acknowledgments
The authors would like to extend their sincere appreciation to the Deanship of Scientific Research at King Saud University for funding this Research group No (RG# 1435-024).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Ethical Approval
Approval from the ethical research committee of the King Saud University (CAMS 15/3536) and the hospitals (King Khalid University Hospital and King Fahad Medical City Hospital) was sought prior to the beginning of the study. All procedures performed were in accordance with the ethical standards of the institution and the 1964 Helsinki declaration.
Rights and permissions
About this article

Cite this article
Almutairi, K.M., Alodhayani, A.A., Alonazi, W.B. et al. Assessment of Health-Related Quality of Life Among Caregivers of Patients with Cancer Diagnosis: A Cross-Sectional Study in Saudi Arabia. J Relig Health 56, 226–237 (2017). https://doi.org/10.1007/s10943-016-0261-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-016-0261-4