
Abstract
United Methodist clergy have been found to have higher than average self-reported rates of obesity, diabetes, asthma, arthritis, and high blood pressure. However, health diagnoses differ from physical health functioning, which indicates how much health problems interfere with activities of daily living. Ninety-five percent (n = 1726) of all actively serving United Methodist clergy in North Carolina completed the SF-12, a measure of physical health functioning that has US norms based on self-administered survey data. Sixty-two percent (n = 1074) of our sample completed the SF-12 by self-administered formats. We used mean difference tests among self-administered clergy surveys to compare the clergy SF-12 Physical Composite Scores to US-normed scores. Clergy reported significantly better physical health composite scores than their gender- and age-matched peers, despite above average disease burden in the same sample. Although health interventions tailored to clergy that address chronic disease are urgently needed, it may be difficult to elicit participation given pastors’ optimistic view of their physical health functioning.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The number of clergy in the United States (US) is likely somewhere between the US Bureau of Labor’s estimate of 404,000 clergy of all faiths in 2006 (Bureau of Labor Statistics 2009) and the Yearbook of American and Canadian Churches estimate of 622,727 clergy serving church traditions (e.g., Catholic, Orthodox, Mainline Protestant, Evangelical, Latter-day Saints, Jehovah’s Witnesses) in 2007 (Lindner 2009). To put these numbers in perspective, in 2006 in the US there were an estimated 633,000 physicians and surgeons, 361,000 fire fighters, and 166,000 psychologists (Bureau of Labor Statistics 2009). Thus, the number of clergy is substantial. Moreover, these clergy serve an estimated 339,000 churches with more than 152 million confirmed members (Lindner 2009)—approximately 50.1% of the US population at the end of 2007 (US Census Bureau 2009).
The clergy vocation is unique in a number of ways. It is well known that clergy engage in pastoral activities such as prayer, worship, and preaching, as well as visiting sick congregants and performing weddings and funerals. In addition, clergy engage in administrative activities such as budget oversight and staff coordination (Carroll 2006), and they further serve as mentors, leaders, spokespersons, and liaisons (Kuhne and Donaldson 1995). Clergy are often at the front line of family deaths and crises, including mental health crises, and these crises put them “on call.” Frequently, clergy (e.g., solo pastors) are the only one at their institution able to respond to crisis calls. The workday of clergy is notably busy, fragmented, and varied, with little predictability (Kuhne and Donaldson 1995). Further, clergy occupy a highly visible role, granting them little privacy (Rowatt 2001), although also allowing them to advance community goals.
Despite the rather unique combination of clergy roles and experiences, the health of clergy has been under-studied, with the exception of a small but growing literature on clergy stress and a handful of studies on clergy mortality rates. In a review of the literature on clergy stress, Morris and Blanton (1994) cited the following five stressors as the most salient for clergy: mobility, low financial compensation, inadequate social support, high time demands, and intrusions on family boundaries. There is some evidence that burnout and dissatisfaction with ministry, at least among clergy families, is increasing (Rowatt 2001). Clergy report that these combined stressors decrease their engagement in healthy behaviors and negatively impact their overall health (Proeschold-Bell et al. 2009).
Studies on standardized mortality rates (SMRs) for clergy generally compare specific religious groups of White, male clergy to other geographically similar White males. Using data spanning four centuries and ten countries, King and Bailar (1969) found that uniformly the SMRs for clergy were substantially lower than those for their non-clergy counterparts. Major contributors to the lower mortality rates were less tuberculosis, syphilis, accidents, and suicide. However, not all disease-specific SMRs were lower for clergy. In 1950, coronary disease was high for US clergy, and diabetes also contributed to higher mortality among US clergy aged 20–64. More recently, Flannelly et al. reviewed 12 studies of the SMRs of clergy and found that in all but one study, the SMR was below 90%, in other words, favorable to clergy (Flannelly et al. 2002). However, they also reported differences in disease-specific SMR by denomination, with Presbyterian (102%) and Episcopal (126%) clergy exhibiting higher SMRs for diabetes than clergy from other churches. Thus, despite impressively low historical overall mortality rates, diseases such as diabetes and coronary disease have been large contributors to mortality for clergy.
The United States has experienced striking changes in overall health status, most notably in obesity and chronic disease. Among adults aged 20 and above, the prevalence of obesity doubled between 1980 and 2002 (Flegal et al. 2002; Hedley et al. 2004). The prevalence of diabetes rose by 33% between 1990 and 1998 (Mokdad et al. 2000). Also, after declining for decades, the prevalence of hypertension rose from 20.4% in 1988–1991 to 28.6% in 1999–2002 (Hajjar et al. 2006). Cardiovascular disease continues to be the leading cause of death among Americans (Neyer et al. 2007).
A recent study compared self-reported chronic disease prevalence rates between United Methodist clergy in North Carolina (NC) and their fair comparison North Carolinian counterparts (people aged 35–64, White, insured, and employed in the past year) (Proeschold-Bell and LeGrand 2010). Over 41% of United Methodist clergy in NC reported height and weight data that would qualify them for obesity, 36% reported having high blood pressure, 34% reported having arthritis, 14% reported having asthma, and 13% reported having diabetes. These rates were significantly higher for NC clergy than for North Carolinians in general. The prevalence rates for clergy were higher by 10.3% for obesity, 4.3% for high blood pressure, 4.1% for asthma, 3.3% for diabetes, and 2.5% for arthritis. We could find only one other study on clergy chronic disease rates. The Evangelical Lutheran Church in America reported a 34% obesity rate for their clergy compared to a US national average of 22% (Halaas 2002). Unlike the study by Proeschold-Bell and LeGrand, they did not adjust for gender (74% male) and age (mean = 50), which may have inflated rates. Nevertheless, there is evidence that clergy are experiencing chronic disease at alarming rates.
The high chronic disease burden experienced by clergy raises the question of whether health problems are disrupting the ability of clergy to perform their unique leadership roles. Health functioning (also known as health-related quality of life) is a commonly measured construct assessing how health affects one’s work activities, socialization activities, and ability to care for oneself. We were unable to find any studies on clergy health functioning. This study used health functioning data from the United Methodist clergy study (described earlier) that reported high chronic disease rates, thereby enabling us to examine physical health functioning in the context of high disease rates. Assessing the degree of physical health functioning among clergy is a first step in understanding the possible repercussions of the high rates of chronic disease among clergy.
Methods
Data Collection
Data were collected as part of the Duke Divinity School Clergy Health Initiative. Through the United Methodist Church (UMC) conference directories, we obtained the names of UMC clergy in the North Carolina and the Western North Carolina Annual Conferences. All currently serving UMC clergy in NC were offered study participation. This census included all full-time and part-time pastors (elders, local, and student pastors) appointed to churches, district superintendents, bishops, extension ministers, currently serving deacons, and retired pastors who had come out of retirement for a church appointment (n = 1,820).
Westat, a contract research organization to the Duke Divinity School, collected data between July and November 2008. We desired a mix of data collection modes (phone, web, paper) in order to consider mode effects when comparing clergy data with that of other studies. Westat randomized clergy in advance to telephone (33%) or self-administered (67%) web conditions.
Westat sent all eligible clergy an advance letter introducing the survey along with a prepaid incentive of $25. Clergy assigned to the web condition were emailed a web link and password to access the survey securely online. Web surveys took approximately 61 min. Westat prompted clergy four times before mailing a paper copy of the survey. If the survey still was not completed, staff contacted clergy and offered to conduct a telephone interview.
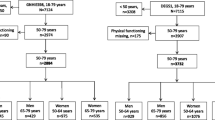
Of the clergy first assigned to the self-administered web version, 83% completed the survey by web, 6% by mail, and 6% by telephone, for a response rate of 95%. The telephone interview response rate was also 95%. Thus, the overall study response rate was 95% with a total of 1,726 participants. Combined, telephone interviews composed 38% (n = 652), web surveys 58% (n = 999), and paper surveys 4% (n = 75). To control for mode effects, this study uses the self-administered data only (n = 1,074).
All procedures were approved by the Duke University and Westat Institutional Review Boards.
Measures
Medical Outcomes Study (MOS) Short Form (SF)-12
The MOS SF-12 is a 12-item health functioning measure that generates scores including a Physical Health Composite Score. Subscales are scored on a 0–100 scale with 50 indicating average health and standard deviations of 10, with norms for the US population and specific subgroups available for the SF-12 version 1 (Ware et al. 1998), used in this study, as well as the slightly newer SF-12 version 2 (Ware et al. 2002). Higher scores indicate better functioning. The SF-12 has been shown to provide good reliability, internal consistency and construct validity (Ware et al. 2002), with its summary scales discriminating between symptomatic and non-symptomatic groups (Andrews et al. 2001; Ciechanowski et al. 2000; Sanderson et al. 2001).
Demographics
Demographic items from the survey included gender, age, ethnicity, education level, marital status, and health insurance status. Ministry salary (not including housing allowance or other household income) was ascertained from the conference directories. Because both age and gender relate strongly to health, SF-12 scores were calculated in aggregate and separately for males and females and by age group. We selected three age groups corresponding to national norm data for the SF-12: ages 35–44 (n = 252); 45–54 (n = 602); and 55–64 (n = 561).
Statistical Analyses
SF-12 Physical Composite Scores were calculated and compared with US-normed scores published in the SF-12 manuals (Ware et al. 1998, 2002). Because this study used version 1, scores are most comparable to the SF-12 version 1 norms. We include comparison of the clergy scores to US-normed scores for the SF-12 version 2 because those norms are more recent and stratify age and gender together. The differences between versions of the SF-12 are small, with minor changes in wording and the winnowing of six response options to five on some items. Mean difference tests were conducted for clergy means versus US means.
Results
Table 1 depicts the demographic characteristics of the clergy sample which provided data via web or paper surveys. The sample is 76.5% male, 91.1% White, highly educated with 77.8% holding either a masters or doctoral degree, and older (mean age = 52.3).
Table 2 displays physical health functioning scores of the clergy sample compared with the available US norms for the SF-12 by age and gender. For 7 of the 11 comparisons, clergy reported significantly better physical health functioning. The largest differences occurred in the age group 55–64. Using version 1 of the SF-12, clergy scores were 3.60 higher than those of their US peers. Using version 2 of the SF-12, clergy scores for men were 3.14 higher, and for women were 4.28 higher, than their US peers. Higher scores indicate better physical health functioning.
Discussion
This study is the first to rigorously compare clergy health functioning status to that of their population counterparts. We used the same data from a census of United Methodist clergy, in which clergy reported high rates of obesity, arthritis, diabetes, asthma, and high blood pressure. Thus, one would expect these clergy to have worse physical health functioning than their general population counterparts. However, despite simultaneously reporting higher rates of chronic disease, clergy reported better physical health functioning than their US peers.
One might wonder whether SF-12 scores that are 2 to 4 points higher indicate an experience of better health functioning, as opposed to being statistically significant but not clinically meaningful. Hundreds of studies have utilized the SF-12 and have found differences in physical health functioning by health condition. For example, studies have found that those with musculoskeletal complaints report physical health functioning scores that are 2.0 points lower than those that do not have these difficulties (Ware et al. 2002). Similarly, asthmatic groups and those with irritable bowel syndrome both average 2.7 points lower than those who do suffer from these conditions (Ware et al. 2002). An example of a health condition averaging 4.2 points lower than people who do not have the condition is osteoarthritis (Ware et al. 2002). Thus, these higher physical health functioning scores reported by clergy likely indicate less disruption of work and socialization activities and the ability to care for themselves, despite reports of higher than average prevalence rates of chronic disease.
We can only speculate as to why this is. First, it may be the work itself. It is possible that the sedentary nature of clergy tasks mitigates the impact on physical health functioning in a way that is not experienced by gender- and age-matched peers who have lower rates of chronic disease but more physically demanding vocations. If clergy had to dig ditches or mine coal, their responses may indicate worse physical health functioning. Likewise, it is possible that sedentary work activities allow clergy to focus on their spiritual well-being. Such focus may actually lead clergy to ignore physical health limitations, which may be of lesser concern to them, as well.
Alternatively, it may be that the calling to their vocation is so strong that clergy overcome physical impediments to answer their call, and that their physical functioning scores reflect an extreme dedication to work. In other words, clergy may persist in their work activities even in the face of arthritic pain or exhaustion from diabetes and high blood pressure. This explanation is consistent with literature indicating that clergy put the needs of others before their own (Proeschold-Bell et al. 2009). In fact, this self-sacrificing mindset may play a role in causing poor clergy health in the first place. In their work to serve God, clergy may prioritize the daily needs and also crises of their congregants, and fail to engage in exercise and healthy eating habits. Clergy may also postpone seeking preventative and acute health care in the process of attending to their calling. Further research in this area is needed.
Clergy may also experience better physical health functioning due to abstaining from tobacco use. In previously unreported data, a strikingly low proportion–4.2%–of United Methodist clergy in NC aged 35–64 reported current smoking, in comparison with 18.3% of North Carolinians the same age. This finding is consistent with other studies that have also documented less alcohol, tobacco, and drug use among clergy (Chatters 2000; Ellison and Levin 1998; Koenig 2001). Smoking and other substance use would likely take a toll on physical health functioning.
It is also possible that the difference in physical health functioning scores could be explained by the higher than average levels of education and income that clergy possess. Both income and education are related to better health (Pappas et al. 1993). Because we were comparing to national SF-12 norm data, we were not able to adjust for education and income. This lack of adjustment was also true of the Proeschold-Bell and LeGrand (2010) study, however, in which they found worse rates of chronic disease. One might expect even greater disparities in chronic disease if these factors were taken into account.
One strength of this study is the sample itself. All currently serving UMC clergy in NC were offered participation, and 95% completed the survey. However, an important limitation of this study is that its sample is limited to UMC clergy in NC. One must be cautious in generalizing to clergy of other faiths, denominations, and geographic locations. Future health studies among clergy of other faiths and denominations are needed. Another limitation is the use of version 1 of the SF-12, on which the national norm data are 14 years older than our data. Given the increase in chronic disease rates in the last two decades, however, one would expect the general population to indicate worse physical health functioning over time, thereby increasing the gap between clergy and the general population. Unfortunately, age and gender stratified norms are not available for version 1. Based on version 2 norms, it appears that older clergy, aged 55–64, experience the greatest benefit in physical health functioning, despite the highest rates of chronic disease in the article by Proeschold-Bell and LeGrand (2010). Additional understanding of clergy health by age group is needed.
In conclusion, this study suggests that, despite an urgent need for health interventions for clergy, it may be difficult to entice clergy to participate in health interventions given their optimistic view of their physical health functioning. Increased understanding of the discrepancy between high clergy disease rates and better perceived clergy physical health functioning is needed. Such understanding may assist in targeting health interventions to clergy while providing insight into how deeply religious individuals attend to their physical health, or, indeed, function in spite of experiencing chronic diseases.
References
Andrews, G., Henderson, S., & Hall, W. (2001). Prevalence, comorbidity, disability and service utilization: Overview of the Australian national mental health survey. British Journal of Psychiatry, 178, 145–153.
Bureau of Labor Statistics US Department of Labor. (2009). Occupational outlook handbook, 2008–2009 edition. Retrieved 6 Nov 2009, from http://www.bls.gov/oco/.
Carroll, J. W. (2006). God’s potters: Pastoral leadership and the shaping of congregations. Grand Rapids, MI: William B. Eerdmans Pub.
Chatters, L. M. (2000). Religion and health: Public health research and practice. Annual Review of Public Health, 21, 335–367.
Ciechanowski, P. S., Katon, W. J., & Russo, J. E. (2000). Depression and diabetes: Impact of depressive symptoms on adherence, function, and costs. Archives of Internal Medicine, 160(21), 3278–3285.
Ellison, C. G., & Levin, J. S. (1998). The religion-health connection: Evidence, theory, and future directions. Health Education & Behavior, 25(6), 700–720.
Flannelly, K. J., Weaver, A. J., Larons, D. B., & Koenig, H. G. (2002). A review of mortality research on clergy and other religious professionals. Journal of Religion and Health, 41(1), 57–67.
Flegal, K. M., Carroll, M. D., Ogden, C. L., & Johnson, C. L. (2002). Prevalence and trends in obesity among US adults, 1999–2000. Journal of the American Medical Association, 288(14), 1723–1727.
Hajjar, I., Kotchen, J. M., & Kotchen, T. A. (2006). Hypertension: Trends in prevalence, incidence, and control. Annual Review of Public Health, 27, 465–490.
Halaas, G. W. (2002). Ministerial health and wellness, 2002, Evangelical Lutheran Church in America. IL: Chicago.
Hedley, A. A., Ogden, C. L., Johnson, C. L., Carroll, M. D., Curtin, L. R., & Flegal, K. M. (2004). Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. Journal of the American Medical Association, 291(23), 2847–2850.
King, H., & Bailar, J. C., I. I. I. (1969). The health of the clergy: A review of demographic literature. Demography, 6(1), 27–43.
Koenig, H. G. (2001). Religion and medicine II: Religion, mental health, and related behaviors. International Journal of Psychiatry in Medicine, 31(1), 97–109.
Kuhne, G. W., & Donaldson, J. F. (1995). Balancing ministry and management: An exploratory study of pastoral work activities. Review of Religious Research, 37(2), 147–163.
Lindner, E. W. (2009). Yearbook of American & Canadian churches. Nashville, TN: Abingdon Press.
Mokdad, A. H., Ford, E. S., Bowman, B. A., Nelson, D. E., Engelgau, M. M., Vinicor, F., et al. (2000). Diabetes trends in the US: 1990–1998. Diabetes Care, 23(9), 1278–1283.
Morris, M. L., & Blanton, P. W. (1994). The influence of work-related stressors on clergy husbands and their wives. Family Relations, 43(2), 189–195.
Neyer, J. R., Greenlund, K. J., Denny, C. H., Keenan, N. L., Labarthe, D. R., & Croft, J. B. (2007). Prevalence of heart disease—United States, 2005. Journal of the American Medical Association, 297(12), 1308–1309.
Pappas, G., Queen, S., Hadden, W., & Fisher, G. (1993). The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. New England Journal of Medicine, 329(2), 103–109.
Proeschold-Bell, R. J., & LeGrand, S. (2010). High rates of chronic disease and obesity among United Methodist clergy. Obesity, doi:10.1038/oby.2010.102.
Proeschold-Bell, R. J., LeGrand, S., James, J., Wallace, A., Adams, C., & Toole, D. (2009). A theoretical model of the holistic health of United Methodist clergy. Journal of Religion and Health, doi 10.1007/s10943-009-9250-1.
Rowatt, W. (2001). Stress and satisfaction in ministry families. Review & Expositor, 98(4), 523–543.
Sanderson, K., Andrews, G., & Jelsma, W. (2001). Disability measurement in the anxiety disorders: Comparison of three brief measures. Journal of Anxiety Disorders, 15(4), 333–344.
US Census Bureau. (2009). Question & answer center. Retrieved 5 Nov2009 from http://www.census.gov/population/www/index.html.
Ware, J. E., Kosinski, M., & Keller, S. D. (1998). SF-12: How to score the SF-12 physical and mental health summary scales (3rd ed.). Lincoln, RI: QualityMetric Inc.
Ware, J. E., Kosinski, M., Turner-Bowker, D. M., & Gandek, B. (2002). SF-12v2: How to score version 2 of the SF-12 health survey (with a supplement documenting version 1). Lincoln, RI: QualityMetric Inc.
Acknowledgments
The authors thank John James, MA, of the Duke Divinity School for his help with the United Methodist conference directory data, and Keith Meador, MD, ThM, MPH, and Robert Millikan, PhD, MPH, for their insightful comments. We thank Brian Pence, Ph.D. for his statistical consults and Christopher Adams, Ph.D., M.A., for clergy stress insights. We thank David Toole, PhD, MTS, for his leadership as Principal Investigator of the Clergy Health Initiative. This study was funded by a grant from the Rural Church Program Area of The Duke Endowment.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Proeschold-Bell, R.J., LeGrand, S. Physical Health Functioning Among United Methodist Clergy. J Relig Health 51, 734–742 (2012). https://doi.org/10.1007/s10943-010-9372-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-010-9372-5