
Abstract
This study determined the effect of a cognitive behavioral group therapy (CBGT) program administered to infertile women on infertility-related stress, depressive and anxious thoughts, and general health state. A randomized controlled design was used for this study. The study was conducted with 107 infertile women: 55 in the experimental group and 52 in the control group. The CBGT was administered to the experimental group for 11 weeks. The pretest, posttest, and trimester follow-up results of this group were compared with those of the control group. The experimental group’s Fertility Problem Inventory pretest mean score was 188.47 ± 30.699, posttest mean score was 135.84 ± 22.571, and follow-up mean score was 140.61 ± 20.16. A statistically significant difference was found between the experimental and control groups’ pretest, posttest, and follow-up mean scores on depressive and anxious cognitions (CCL), FPI and its subscales, and the General Health Questionnaire-28 and its subscales (p < 0.05). The CBGT intervention reduced the infertility-related psychosocial problems experienced by infertile women and promoted improvement in their depressive and anxious cognitions, and their mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Infertility is the inability of sexually active couples to achieve or continue pregnancy despite having unprotected intercourse at least three times a week for 12 or more months (Zegers and Adamson 2009). Infertility affects more than 80 million people and its prevalence ranges between 5 and 30% (Sezgin and Hocaoğlu 2014). The infertility experience, also defined as an “infertility crisis,” is accompanied by physical, economic, and social stresses (Sexton et al. 2010). Infertility can even be considered one of the most stressful situations in infertile peoples’ lives. Infertile women feel more psychological stress and pressure than their husbands, and the prevalence of anxiety and depression among them are higher (McNaughton-Cassill et al. 2002; El Kissi et al. 2013; Maroufizadeh et al. 2017). Studies show that 50% of infertile women consider this process to be the most stressful experience of their lives (Herrmann et al. 2011) and the psychosocial agony they experience is similar to those with a life-threatening disease such as cancer or heart failure (Domar et al. 1993). Previous studies report that unseen losses (loss of dreams, genetic continuity, perception of oneself as a fertile individual, successful pregnancy and childbearing experiences, breastfeeding experience, relationships, and hope for being a potential grandmother) experienced by infertile women increase their stress level and mental health problems (Lohrmann 1995; Günay et al. 2005; Karaca and Ünsal 2015).
The importance of psychological support systems in addition to biological treatments for infertility is increasingly recognized. Studies in recent years sought to reduce psychological symptoms such as high levels of stress, anxiety, or depression caused by infertility. Individual, couple, or group based psychological support and intervention programs positively affect both birth rates and psychological health for patients with infertility (Domar et al. 2000; Facchinetti et al. 2004; Pasha et al. 2013). In such programs both behavioral and cognitive techniques are used, which are the mainstay of cognitive behavioral therapy (CBT). Some studies show psychotherapy is a reliable alternative to pharmacotherapy for reducing anxiety and improving the mental health of infertile women (Faramarzi et al. 2008; Pasha et al. 2013). Czamanski-Cohen et al. (2016) conducted a study to examine the effect of CBT on pregnancy rates. They showed that CBT programs administered during in vitro fertilization (IVF) treatment reduced the perceived level of stress, and that they increased the rate of pregnancy compared to the control group.
CBT is effective in the treatment of many mental problems, and it is widely used by mental health professionals. However, a relatively limited number of studies examine the effectiveness of CBT as a psychosocial intervention in infertility. Although the number of studies on the psychosocial effects of infertility has increased recently, no psychosocial intervention studies specifically addressing this question have been conducted. The present study evaluated the effectiveness of a cognitive behavioral group therapy (CBGT) program developed specifically for Turkey.
Infertility being the most challenging crisis that couples experience, it is necessary for mental health and reproductive health professionals to cooperate within the team. Mental health professionals can be the bridge between providing psychotherapy services and clarifying complex medical procedures (Hart 2002). The authors of this study are reproductive health and mental health professionals and they have sought to emphasize the importance of team cooperation for infertility with this study.
This study aimed to determine the effect of the CBGT program administered to (1) women with infertility on the levels of stress due to infertility, (2) their negative depressive and anxious automatic thoughts, (3) general health state.
Methods
Sample
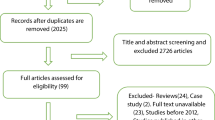
This randomized controlled study was conducted in the infertility and assisted reproductive techniques unit of a university hospital. A total of 332 women who were diagnosed with infertility and subsequently referred to the infertility and assisted reproductive techniques unit between June 2017 and September 2017 were included in the study. An obstetrics and gynecology specialist and a fertility nurse informed the women who came to the hospital for treatment about the study. The patients who agreed to participate in the study and met the inclusion criteria (n = 110) were referred by the fertility nurse to the researcher (psychiatric nurse/therapist), who conducted the sessions. The experimental and control groups were created using propensity score matching, randomization methods using a computer software that randomly assigned the participants to one of the groups, taking into consideration factors like age, education level, duration of infertility, and suspected etiology of infertility. The inclusion criteria for the participants were as follows: females younger than 45 years, who were at least literate, who were diagnosed with infertility for at least 1 year, who were married, who did not receive psychotherapy or psychiatric treatment before, who did not participate in any psychological/social support group before, who spoke Turkish, and who volunteered to participate in the study. Four experimental groups were created which consisted of 12 or 13 participants in each one. The group therapy sessions lasted for 11 weeks. During the intervention, four participants left the group because they became pregnant, and one participant left the group because of relocation. Five participants in the experimental group were not included in the follow-up session because they got pregnant. In the control group, three participants were not included because of pregnancy, and one participant was not included because of relocation. Therefore, in total the experimental group consisted of 55 participants, and the control group consisted of 52 participants (Fig. 1). The participants in the control group were assigned to a waiting list, and they all received the same CBGT program as the active treatment group at the termination of the study.

Test Administration Stages
Procedure
The study was conducted between September 2017 and May 2018. A CBT-trained psychiatrist prepared the sessions based on the CBT approach, and organized the sessions. These sessions were held in the meeting room of the infertility and assisted reproductive techniques unit. The groups were closed groups, and no additional participants were taken until the group sessions were completed. Make-up sessions were conducted by a group therapist for those who could not participate in the session for any reason.
The experimental group was offered 11 weekly CBT sessions delivered in a group format. Except for the first and the last therapy sessions, which lasted for 140 min to allow an additional 20 min to fill out the study questionnaires, all sessions lasted for 120 min. A nurse experienced in CBT led the therapy, and an obstetrics and gynecology specialist joined her in the first session, during which psychoeducation about the techniques and treatment options for infertility was discussed with the participants for 20 min. The therapy sessions followed a syllabus, which started with psychoeducation about the CBT approach. The next two sessions focused on the cognitive model of psychopathology and an individualized case conceptualization for the participants. Later, behavioral techniques to overcome depression, anxiety, and stress were introduced, where progressive muscle relaxation, controlled breathing, activity scheduling, problem solving, and other stress management techniques were discussed. At the same time, the therapist also provided information on the concept of negative cognitions, and ways to challenge them. Underlying assumptions and deeper schemata were also discussed during these sessions, and the participants were taught ways to identify and challenge their negative cognitions and how to incorporate a more balanced way of thinking into their daily lives. Participants were also encouraged to identify any unhelpful strategies they had been employing to overcome their depression or anxiety, and more adaptive ways of coping were discussed. These sessions formed the core component of the therapy, and they consisted of six sessions. All sessions also included between-session homework assignments to strengthen the learning process, which generally correlated with the particular week’s agenda. The tenth session was specifically reserved for the sexual problems of the participants. The last session was a summary of all the topics covered during the previous weeks, and a blueprint for relapse prevention was offered. The therapist’s fidelity to the CBT protocol and her competence in delivering the therapy techniques were monitored and assessed by an independent rater using the Cognitive Therapy Scale (Young and Beck 1980).
Three tests were administered to the participants in the study: pretest, posttest, and follow-up test. The scales used in the pretest were completed in the first session and those in the posttest were completed in the last session. For the follow-up session, the experimental and control group was invited again to complete the tests. Attention was paid to simultaneously administer the tests to both groups. The fertility nurse played an active role to make sure that the test was completed by the participants.
Data Collection Tools
The study data were collected using the Personal Information Form, the Fertility Problem Inventory (FPI), the General Health Questionnaire (GHQ-28), and the Cognitions Checklist (CCL).
Personal Information Form The researchers prepared this form, and it included questions about the demographic data of the women and the clinical characteristics of their infertility.
Fertility Problem Inventory (FPI) The FPI was developed by Newton et al. in 1999 to measure the infertility-related global stress level of an individual. This is a self-assessment scale consisting of 46 items (Newton et al. 1999). Eren (2008) tested the validity and reliability of the Turkish version of this scale. The Cronbach’s alpha score of the scale in the present study was 0.920. This scale can be used for both women and men who have either primary or secondary infertility. The scale is composed of five subscales including social concerns, sexual concerns, marital concerns, need for parenthood, and rejection of a childless lifestyle. These subscales determine the infertility-related stress in specific fields. Higher scores indicate increased stress related to infertility. The mean standard global stress score obtained was 134.4 ± 33.8.
General Health Questionnaire (GHQ-28) This questionnaire was developed by Goldberg in 1972 (Goldberg and Williams 2000). Kılıç tested the validity and reliability of the Turkish version in 1996 (Kılıç 1996). Kılıç found that the reliability of the GHQ-28 (Cronbach’s alpha) was 0.94, and its sensitivity at the cut-off score of 5 was 73.7%. The questionnaire consists of four subscales with seven questions in each: somatic symptoms, anxiety and sleep disorders, social dysfunction, and severe depression. Studies have found that the subscales are correlated with each other.
Cognition Checklist (CCL) This self-assessment scale includes 26 items that measure the frequency of depression and anxiety. In this 5-point Likert-type scale, the scores range from 0 to 4, where 0 indicates “never”, and 4 indicates “always”. This scale includes two subscales: depressive cognitions and anxious cognitions. The mean score on the depression subscale ranged from 0 to 56, and the mean score on the anxiety subscale ranged from 0 to 48 (Beck et al. 1987). Batmaz et al. tested the validity and reliability of the Turkish version of this scale in 2015 (Batmaz et al. 2015).
Statistical Analysis
We did a a priori power analysis in order to determine the minimum number of participants needed for the study using G*Power 3.1.9.2 (Faul et al. 2007), and the analysis showed that in order to identify an effect size of 0.50 (moderate effect size), with an alpha of 0.05 and 0.80 power, we would need a total of 51 participants per group. All the remaining analyses were performed by using IBM SPSS Statistics version 22 (IBM Corp., 2013) software package. The data were analyzed using frequency distribution for categorical variables and descriptive statistics (mean ± SD) for numeric variables. The Kolmogorov–Smirnov test for normality was administered for the scales and their subscales to decide on the analyses to be performed. The test results showed that all scores met the assumptions of normality; therefore, parametric tests were used for comparison. We performed independent sample t test to determine whether there was a difference between two independent (e.g. experimental and control) groups in terms of their scores. We performed repeated measures analysis of variance to detect whether there was a difference between more than two dependent groups and also performed the Bonferroni tekeeping pretest scores under controlst to detect which groups presented differences. The researchers used an analysis of covariance (ANCOVA) to determine whether there was a difference between posttest and follow-up scores that were modified according to pretest scores between the experimental and control groups.
Ethical Considerations
Written permission (2017/86) was obtained from the Ethics Committee of Düzce University Non-Invasive Health Studies. The research was performed considering the “Informed Consent Principle,” “Volunteering Principle,” and “Confidentiality Principle,” which are the ethical principles for the protection of the individual rights of people. After the research was completed, a CBGT program was provided for the participants in the control group.
Results
The study examined coefficients of skewness and kurtosis of scale and subscale scores to determine the analyses to be performed. The coefficients of skewness and kurtosis were found to be in a range of + 2, therefore, parametric tests were used for their comparisons.
Table 1 shows the demographic and clinical characteristics of the participants in the experimental and control groups. The mean age of the women included in the study was 30.46 ± 5.72 (18–43) years, and the groups were homogeneous for their mean age (p > 0.05). No significant difference was found between the groups for the women’s education level, work status, income level, family type, and treatment result (whether pregnancy occurred at the end of the treatment or not) (p > 0.05, Table 1).
Table 2 shows a statistically significant difference between the mean scores of whole scale and subscale periods as a result of repeated measures analysis of variance that was performed for the experimental group. Accordingly, while the CCL, GHQ, FPI, and their subscales’ pretest mean scores were significantly higher than their posttest and follow-up mean scores, follow-up mean scores were significantly lower than their posttest mean scores.
While the study found no statistically significant difference between the mean scores of the “rejection of a childless lifestyle” and “need for parenthood” subscale periods (p > 0.05), repeated measures analysis of variance for the control group showed that there was a statistically significant difference between the mean scores of the CCL, GHQ, FPI, and their social, sexual, marital subscale periods (p < 0.01).
The study found a statistically significant difference between the mean posttest and follow-up scores for GHQ and its subscales in the experimental and control groups as a result of independent t-test, as shown in Table 3 (t = − 11.026, t = − 6.708, t = − 12.384, t = − 8.445; p < 0.001, respectively). Independent t-test showed that was a statistically significant difference between the mean posttest and follow-up scores for FPI and its subscales in the experimental and control groups (t = − 9.400, t = − 14.394, t = − 3.556, t = − 8.407, respectively; p < 0.001). Accordingly, it can be concluded that the experimental group’s mean posttest and follow-up scores for FPI and its subscales are significantly lower than those of the control group.
The mean posttest follow-up scores and those that were modified based on pretest scores are presented in Table 4. The modified mean posttest and follow-up scores were calculated by controlling for pretest scores. The study found a statistically significant difference between the mean posttest and follow-up scores for FPI and its subscales that were modified based on pretest scores and applied to the experimental and control groups as a result of performed ANCOVA (F = 90.813, F = 76.457, respectively; p < 0.001). The study found a statistically significant difference between the mean posttest and follow-up scores on the “severe depression” subscale of the GHQ that were modified based on pretest scores and applied to the experimental and control groups as a result of ANCOVA (F = 59.263; p < 0.001). The study also found a statistically significant difference between the mean posttest and follow-up scores on the “social problems and rejection of a childless lifestyle” subscales of the FPI that were modified based on pretest scores and applied to the experimental and control groups (F = 313.822, F = 56.928, respectively; p < 0.001).
When the time and group interaction results in Table 5 are examined, they show a statistically significant difference between whole scale and subscale periods (pretest, posttest, follow-up) and groups (p < 0.001). Accordingly, there was a significant decrease in the posttest and follow-up scores from the pretest scores of the experimental group, while there was a significant increase in the posttest and follow-up scores of the control group.
Discussion
This study determined the effect of a CBGT program on infertility-related stress, depressive and anxious cognitions and general health state. The study results showed that CBGT positively affected all three areas.
The participants had high pretest scores on the FPI, global stress, depressive and anxious cognitions and general health state. Many previous studies showed that women with infertility had high levels of stress and were likely to develop mental health problems, depression, and anxiety (Gulseren et al. 2006; Weinger 2009; Kahyaoglu Sut and Balkanli Kaplan 2015; Maroufizadeh et al. 2017). Infertility-related mental health problems are widely observed, and minimizing these mental health problems and stress levels increases potential birth rates (Yorulmaz and Sütcü 2016).
This study found the experimental group’s posttest and follow-up mean scores on the global stress and all of its subscales were significantly lower than the control group’s posttest and follow-up mean scores. Furthermore, the posttest and follow-up scores for the CBT intervention group on global stress and all of its subscales decreased compared to the pretest score. Faramarzi et al. (2013) compared CBT with fluoxetine, and found that although the CBT group’s mean scores on social concerns, sexual concerns, marital concerns, rejection of a childless lifestyle, and need for parenthood decreased significantly compared to the pretest scores, only the sexual concerns mean score decreased significantly in the fluoxetine group. Thus, CBGT intervention was a highly effective method for infertility-related problems in women. Table 2 indicated the need for parenthood subscale of the FPI had the highest subscale score (47.85 ± 7.483). Although the posttest and follow-up test scores decreased significantly, these scores were higher than the pretest scores of the other subscales. In previous studies, the reasons why infertile women had high levels of stress varied. However, desire for experiencing the feeling of motherhood and ability to reproduce were primary reasons (Benyamini et al. 2008; Podolska and Bidzan 2011). Inability to be a mother may be considered equivalent to the loss of reproductivity and womanhood, and results in other losses such as pregnancy, childbearing, and breastfeeding experiences and loss of genetic continuity (Lohrmann 1995; Bidzan et al. 2011). In a study conducted in Turkey, 96.2% of women reported that they wanted to have children to “experience the feeling of motherhood” (Karaca and Unsal 2015). In another study conducted in the USA, women considered the inability to have children as a threat to their personal identity (Gonzalez 2000). The social concerns subscale of the global stress scale ranked second (39.37 ± 8.619). However, a considerable decrease was observed in the posttest and follow-up test scores after the CBT intervention. Motherhood is considered a primary role for women, particularly in traditional cultures. Therefore, women feel substantial social pressure and are stigmatized, which results in their avoidance of social relationships and activities (Remennic 2000; Fido and Zahid 2004; Weinger 2009; Karaca and Unsal 2015). Studies conducted in Turkey with women who have infertility reported that women frequently resorted to social avoidance, and that they felt severely stigmatized (Akyüz et al. 2014; Özdemir 2006; Karaca and Unsal 2015). Therefore, the effect of CBGT intervention on decreasing social concerns is a significant result for the present study.
Recent studies showed that 50% of women with infertility defined their infertility as the most stressful situation in their lives (Herrmann et al. 2011). Therefore, controlling the stress level might reduce mental health problems in women, and increase the potential birth rates (Yorulmaz and Sütcü 2016). Facchinetti et al. examined the effect of CBT for women with infertility on stress (2004), and found that under the same stressing situations, the CBT group had lower blood pressure and heart rate levels than the control group. Mosalanejad et al. (2012) observed a statistically significant decrease in the posttest scores of the CBT group on psychological stress, anxiety, and depression. In the present study, the global stress score of the CBT intervention group decreased both in the posttest and follow-up tests, and there was a significant difference between this group and the control group. Thus, CBT was shown as an effective method to reduce infertility-related stress levels.
This study found a statistically significant difference between the experimental and control groups’ pretest, posttest, and follow-up mean scores on the CCL, and its subscales (depressive and anxious thoughts) (p < 0.05). This finding implies that CBGT intervention was an effective method to address depressive and anxious cognitions. Anxiety and depression are the most frequently encountered mental disorders in the general population (Kroenke et al. 2009). Individuals with infertility experience twice as much anxiety and depression than the general population (Kahyaoglu Sut and Balkanli Kaplan 2015; Maroufizadeh et al. 2018). A study conducted in Iran in 2018 found the prevalence of anxiety in individuals with infertility was 49.6%, and depression was 33.0%. This study also found that anxiety symptoms were observed 2.26 times more in women than in men (Maroufizadeh et al. 2018). Long-term studies showed that CBT was effective as a therapy method for the treatment of depressive and anxious cognitions and disorders (Twomey et al. 2014; Andersen et al. 2016; Springer et al. 2018). The effectiveness of CBGT intervention for the mental health problems such as depression and anxiety of women with infertility has been a focus of research for the last 10 years. However, the researchers did not find any study in which CBGT specifically assessed infertile women’s cognition in the related literature. A study that assessed the automatic cognitions of infertile women determined that they frequently had difficulties handling their anxiety (Karaca 2018). It is thought that women’s cognitions that changed with CBGT will play a protective role in handling infertility-related problems. The posttest and follow-up test scores on the GHQ-28 in total and all its subscales (somatic symptoms, anxiety and sleep disorders, social dysfunction, and severe depression) of the women with infertility were significantly lower than their pretest scores, and the decrease was significant compared to the control group. Faramarzi et al. (2008) compared the effectiveness of fluoxetine, CBT, and the control group in their study. In the CBT group, they found a significant decrease in GHQ and all its subscale scores. However, there was a significant decrease in the subscales other than psychosocial symptoms in the fluoxetine group. They also found a significant decrease in the depression levels of the women with infertility in the CBT group. In the present study, the pretest mean score on the severe depression subscale was 2.02, the posttest mean score was 0.00, and the follow-up mean score was 0.11, which showed the effectiveness of the CBT intervention on the depression symptoms. Domar et al. (2000) found a significant decrease in the CBT group compared to the psychological support group and control group. Pasha et al. (2013) reported that depression scores for both antidepressant and CBT groups decreased significantly compared to the control group, which showed that CBT was the most effective treatment. Faramarzi et al. (2008) found that the CBT intervention group had significantly decreased depression and anxiety scores compared to the drug and control groups. A statistically significant decrease was observed in the CBT group’s posttest anxiety and depression scores. In the present study, anxiety, social dysfunction, and sleep disorder symptoms were improved in the CBT intervention group, which was in line with other studies’ results (Tarabusi et al. 2004; Hosaka et al. 2002; McNaughton-Cassill et al. 2002; Mosalanejad et al. 2012).
In conclusion, a multidisciplinary collaboration between specialists in reproductive and assisted fertility techniques and mental health professionals is essential for the treatment of infertility. This study has added new evidence that multidisciplinary collaboration positively affects some mental health parameters of women with infertility. The participation of gynecologists who perform assisted reproduction treatment in some sessions can be seen as a strength of the study. Participants had the opportunity to obtain comprehensive information/consultation about infertility treatments and the problems they encountered with their cooperation during sessions. CBGT needs to be tested on larger and different samples. However, these findings offer hope for men and women who stress over infertility, and for mental health and reproductive health professionals.
As infertility is a couple’s problem, the fact that this study was conducted with women only can be seen as a limitation. Future studies using CBGT should be conducted with more diverse samples for intervention in problems caused by being infertile. The effectiveness of CBGT with couples should be assessed because infertility often causes marital and sexual problems. In the meantime, studies that compare individualistic CBT and CBGT can be recommended to researchers.
The CBT program administered in this study may be recommended to fertility clinics in Turkey by mental health professionals. Educational programs for medical personnel can be planned as a dissemination activity for CBGT use at infertility clinics.
References
Akyüz, A. S., Şahiner, G., Seven, M., & Bakır, B. (2014). The effect of marital violence on infertility distress among a sample of Turkish women. International Journal of Fertility and Sterility, 8, 67.
Andersen, P., Toner, P., Bland, M., & McMillan, D. (2016). Effectiveness of transdiagnostic cognitive behaviour therapy for anxiety and depression in adults: A systematic review and meta-analysis. Behavioural and cognitive psychotherapy, 44(6), 673–690. https://doi.org/10.1017/S1352465816000229.
Batmaz, S., Yuncu, O. A., & Kocbiyik, S. (2015). Assessing negative automatic thoughts psychometric properties of the Turkish version of the cognition checklist. Iranian journal of psychiatry and behavioral sciences, 9(4), 3444. https://doi.org/10.17795/ijpbs-3444.
Beck, A. T., Brown, G., Steer, R. A., Eidelson, J. I., & Riskind, J. H. (1987). Differentiat-ing anxiety and depression: A test of the cognitive content-spec-ificity hypothesis. Journal of Abnormal Psychology, 96(3), 179–183.
Benyamini, Y., Bardarıan, Y. G., Gozlan, M., Tabıv, G., Shiloh, S., & Kokıa, E. (2008). Coping specificity: The case of women coping with infertility treatments. Psychology and Health, 23, 221–241. https://doi.org/10.1080/14768320601154706.
Bidzan, M., Podolska, M., Bidzan, L., & Smutek, J. (2011). Personality traits and the feeling of loneliness of women treated for infertility. Ginekologia Polska, 82(7), 508–513.
Domar, AD., Clapp, D., Slawsby, E., Kessel, B., Orav, J., & Freizinger, M. (2000). The impact of group psychological interventions on distress in infertile women. Health Psychology, 19(6), 568. http:dx.doi.org/10.10370278-6!33.19.6.568.
Domar, A. D., Zuttermeister, P. C., & Friedman, R. (1993). The psychological impact of infertility: a comparison with patients with other medical conditions. Journal of Psychosomatic Obstetrics and Gynaecology, 45, 42.
El Kissi, Y., Romdhane, A. B., Hidar, S., Bannour, S., Ayoubi Idrissi, K., Khairi, H., et al. (2013). General psychopathology, anxiety, depression and self-esteem in couples undergoing infertility treatment: A comparative study between men and women. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 167, 185–189. https://doi.org/10.1016/j.ejogrb.2012.12.014.
Eren, N. (2008). The effect of perceived social support in infertile couples on infertility–related stress and marriage harmony (doktoral thesis). Ankara: Gazi University.
Facchinetti, F., Tarabusi, M., & Volpe, A. (2004). Cognitive-behavioral treatment decreases cardiovascular and neuroendocrine reaction to stress in women waiting for assisted reproduction. Psychoneuroendocrinology, 29, 162–173.
Faramarzi, M., Alipor, A., Esmaelzadeh, S., Kheirkhah, F., Poladi, K., & Pash, H. (2008). Treatment of depression and anxiety in infertile women: cognitive behavioral therapy versus fluoxetine. Journal of Affective Disorders, 108(1–2), 159–164. https://doi.org/10.1016/S0306-4530(02)00170-1.
Faramarzi, M., Pasha, H., Esmailzadeh, S., Kheirkhah, F., Heidary, S., & Afshar, Z. (2013). The effect of the cognitive behavioral therapy and pharmacotherapy on ınfertility stress: a randomized controlled trial. International Journal of Fertility and Sterility, 7, 199–206.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
Fido, A., & Zahid, M. A. (2004). Coping with infertility among Kuwaiti women: cultural perspectives. International Journal of Social Psychiatry, 50, 294–300. https://doi.org/10.1177/0020764004050334.
Goldberg, DP, & Williams, PA. (2000). General health questionnaire (GHQ). Swindon: nferNelson.
Gonzalez, L. (2000). Infertility as a transformational process: A framework for psychotherapeutic support of infertile women. Issues in Mental Health Nursing, 21, 619–633. https://doi.org/10.1080/01612840050110317.
Gulseren, L., Cetinay, P., Tokatlioglu, B., Sarikaya, O. O., Gulseren, S., & Kurt, S. (2006). Depression and anxiety levels in infertile Turkish women. Journal of Reproductive Medicine, 51, 421–426.
Hart, A. V. (2002). İnfertilite and the role of psychotherapy. İssues İn Mental Health Nursing, 23, 31–41.
Herrmann, D., Scherg, H., Verres, R., Von, Hagens C., Strowitzki, T., & Wischmann, T. (2011). Resilience in infertile couples acts as a protective factor against infertility-specific distress and impaired quality of life. Journal of Assisted Reproduction and Genetics, 10, 1111–1117. https://doi.org/10.1007/s10815-011-9637-2.
Hosaka, T., Matsubayashi, H., Sugiyama, Y., Izumi, S. I., & Makino, T. (2002). Effect of psychiatric group intervention on natural-killer cell activity and pregnancy rate. General Hospital Psychiatry, 24, 353–356. https://doi.org/10.1016/S0163-8343(02)00194-9.
Kahyaoglu Sut, H., & Balkanli Kaplan, P. (2015). Quality of life in women with infertility via the FertiQoL and the hospital anxiety and depression scales. Nursing and Health Sciences, 17(1), 84–89. https://doi.org/10.1111/nhs.12167.
Karaca, A. (2018). Infertile women’s automatic negative thoughts and coping strategies: Qualitative study. In 5th International Conference Quality and Its Perspectives, with the subtitle: Multidisciplinary Approach to Patient Care, April, pp. 35–42.
Karaca, A., & Unsal, G. (2015). Psychosocial problems and coping strategies among Turkish women with infertility. Asian Nursing Research, 9(3), 243–250. https://doi.org/10.1016/j.anr.2015.04.007.
Kılıç, C. (1996). General health questionnaire: Validity and reliability. Turkish Psychiatry Review, 7, 3–9.
Kroenke, K., Spitzer, R. L., Williams, J. B., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50, 613–621.
Lohrmann, JA. (1995). A psychological investigation of women’s experience of successfully coping with infertility (doctoral thesis). Cincinnati: Union Institute.
Maroufizadeh, S, Ghaheri, A, Almasi-Hashiani, A, Mohammadi, M, Navid, B, Ezabadi, Z, & Samani, R. O. (2018). The prevalence of anxiety and depression among people with infertility referring to Royan Institute in Tehran, Iran: A cross-sectional questionnaire study. Middle East Fertility Society Journal. 23(2):103–106. http://creativecommons.org/licenses/by-nc-nd/4.0/
Maroufizadeh, S., Ghaheri, A., & Omani, Samani. (2017). Factors associated with poor quality of life among Iranian infertile women undergoing IVF. Psychology, health and medicine, 22(2), 145–151. https://doi.org/10.1080/13548506.2016.1153681.
McNaughton-Cassill, M. E., Bostwick, J. M., Arthur, N. J., Robinson, R. D., & Neal, G. S. (2002). Efficacy of brief couples support groups development to manage the stress of in vitro fertilization treatment. Mayo Clinic Proceedings, 77, 1060–1066. https://doi.org/10.4065/77.10.1060.
Mosalanejad, L., Khodabakshi Koolaee, A., & Jamali, S. (2012). Effect of cognitive behavioral therapy in mental health and hardiness of infertile women receiving assisted reproductive therapy (ART). Iranian Journal of Reproductive Medicine, 10, 483–488.
Newton, C. R., Sherrard, W., & Glavac, I. (1999). The Fertility Problem Inventory: measuring perceived infertility–related stress. Fertility and Sterility, 72, 54–62.
Özdemir, A. Ç. (2006). Psychological projections of infertility. American Journal of Orthopsychiatry, 2(47), 34–40.
Pasha, H., Faramarzi, M., Esmailzadeh, S., Kheirkhah, F., & Salmalian, H. (2013). Comparison of pharmacological and nonpharmacological treatment strategies in promotion of infertility self-efficacy scale in infertile women: A randomized controlled trial. Iranian journal of reproductive medicine, 11(6), 495.
Podolska, M. Z., & Bidzan, M. (2011). Infertility as a psychological problem. Ginekologia Polska, 82, 44–49.
Remennic, L. (2000). Childless in the land of imperative motherhood: Stigma and coping among infertile Israeli women. Sex Role, 11, 821–841.
Sexton, M. B., Byrd, M. R., O’Donohue, W. T., & Jacobs, N. N. (2010). Web-based treatment for infertility-related psychological distress. Archives of Women’s Mental Health, 13, 347–358. https://doi.org/10.1007/s00737-009-0142-x.
Sezgin, H., & Hocaoğlu, Ç. (2014). Psychiatric aspect of infertility. Current Approaches in Psychiatry, 6(2), 165–184.
Springer, K. S., Levy, H. C., & Tolin, D. F. (2018). Remission in CBT for adult anxiety disorders: A meta-analysis. Clinical psychology review, 61, 1–8. https://doi.org/10.1016/j.cpr.2018.03.002.
Tarabusi, M., Volpe, A., & Facchinetti, F. (2004). Psychological group support attenuates distress of waiting in couples scheduled for assisted reproduction. Journal of Psychosomatic Obstetrics and Gynecology, 25, 273–279. https://doi.org/10.1080/01674820400017905.
Twomey, C., O’Reilly, G., & Byrne, M. (2014). Effectiveness of cognitive behavioural therapy for anxiety and depression in primary care: a meta-analysis. Family practice, 32(1), 3–15. https://doi.org/10.1093/fampra/cmu060.
Weinger, S. (2009). Infertile Cameroonian women: social marginalization and coping strategies. Qualitative Social Work, 8, 45–64. https://doi.org/10.1177/1473325008100425.
Yorulmaz, E. G., & Sütcü, S. T. (2016). Effectiveness of cognitive behavioral group therapy in infertility: A systematic review. Current Approaches in Psychiatry. 8:144–156. http://dx.doi.org/10.18863/pgy.24953.
Young, J., & Beck A. (1980). Cognitive therapy scale: Rating manual. Unpublished manuscript, Center for Cognitive Therapy, Philadelphia, PA.
Zegers, H. F., & Adamson, G. D. (2009). International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology. https://doi.org/10.1093/humrep/dep343
Acknowledgements
The authors would like to thank to all participants in this study. They also thank the nurses and secretaries in the infertility outpatient clinic for their support.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
Study design: AK, AY, SB; data collection: AÇ, AK, AY; article drafting: AK, SB, AY and data interpretation and revision and final approval of the article: all authors.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Karaca, A., Yavuzcan, A., Batmaz, S. et al. The Effect of Cognitive Behavioral Group Therapy on Infertility Stress, General Health, and Negative Cognitions: A Randomized Controlled Trial. J Rat-Emo Cognitive-Behav Ther 37, 375–394 (2019). https://doi.org/10.1007/s10942-019-00317-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10942-019-00317-3