
Abstract
Contemporary prevention science has focused on the application of cultural adaptations of evidence-based prevention programs for minority youth populations. Far less is known about culturally grounded methods that are intended to organically develop prevention programs within specific populations and communities. This article systematically reviews recent literature on culturally grounded interventions used to prevent health disparities in ethnic minority youth populations. In this review, we assessed 31 peer-reviewed articles published in 2003 or later that fit inclusionary criteria pertaining to the development and evaluation of culturally grounded prevention programs. The evaluated studies indicated different approaches toward cultural grounding, as well as specific populations, geographic regions, and health issues that have been targeted. Specifically, the findings indicated that most of the studies focused on the development and evaluation of culturally grounded HIV/STI and substance abuse prevention programs for Mexican–American, African American, and American Indian/Alaska Native youth residing in the South or Southwestern US. These studies largely relied on community-based participatory or qualitative research methods to develop programs from the “ground up.” This review has implications for the development of future culturally grounded and culturally adapted prevention programs targeting underserved minority youth populations and geographic regions. Specifically, it identifies populations and regions where culturally grounded prevention efforts are underdeveloped or non-existent, providing some scientific direction for the future development of these types of programs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the past two decades, there has been an increased focus on incorporating culturally specific content in prevention programs in order to address health disparities and promote health equity in marginalized populations (Barrera, Castro, Strycker, & Toobert, 2013). Research has suggested that prevention interventions that meaningfully incorporate the values and norms of targeted cultural groups promote both cultural “fit” and program effectiveness for those populations (Castro, Barrera, & Martinez, 2004; Okamoto et al., 2014). While social and behavioral intervention research has largely endorsed the value of cultural specificity, it has also described multiple methods by which culture can be infused into prevention curricula (Okamoto, Kulis, Marsiglia, Holleran Steiker, & Dustman, 2014; Resnicow, Soler, Braithwaite, Ahluwalia, & Butler, 2000). Further, while the prevention literature has described the theoretical use of and scientific value behind some of these methods to develop culturally focused prevention interventions (Barrera et al., 2013; Castro, Barrera, & Holleran Steiker, 2010; Castro et al., 2004; Resnicow et al., 2000), relatively little is known about the use of approaches that build prevention curricula from the “ground up” (i.e., culturally grounded prevention; Okamoto et al., 2014). As a result, little is known about the contexts in which this type of approach should be used and the populations that may benefit most from these approaches. The purpose of this article is to provide a systematic review of published literature pertaining to culturally grounded prevention for ethnic minority youth, which is intended to elucidate how this approach has been used with different populations and in different settings. This review has implications for the future use of culturally grounded approaches to prevention development with specific youth populations and within specific contexts.
Literature Review
Definition of Culturally Grounded Prevention
Culturally grounded prevention programs utilize collaborative approaches toward their development and evolve from the “ground up” (Lee, Vu, & Lau, 2013; Okamoto et al., 2014). The “ground up” or “bottom up” nature of these approaches indicate that they start from the values, behaviors, norms, and worldviews of the populations they are intended to serve, and therefore are most closely connected to the lived experiences and core cultural constructs of the targeted populations and communities (Okamoto et al., 2014). Central to culturally grounded approaches, researchers work collaboratively with members of the target community in order to create a program from inception to implementation, beginning with a community needs assessment to identify priorities for prevention (Lee et al., 2013). Lee and colleagues distinguished culturally grounded prevention from another bottom up approach—the indigenous approach—by which a single (or few) community stakeholder(s) develop a curriculum without the collaboration of researchers or the community-at-large.
Lee et al. (2013) and Okamoto, Kulis, Marsiglia, Holleran Steiker, and Dustman (2014) further differentiate culturally grounded from culturally adapted prevention. Currently, there is more empirical and theoretical literature describing the development and effectiveness of culturally adapted interventions than of culturally grounded interventions (Okamoto et al., 2014). In contrast to culturally grounded approaches, cultural adaptations are defined as the modification of an existing intervention, such as changing the language and cultural references in curricular lessons, in order to make the intervention compatible with a specific population (Bernal, Jiménez-Chafey, & Domenech Rodríguez, 2009; Resnicow, Baranowski, Ahluwalia, & Braithwaite, 1999). Cultural adaptations often rely upon a top–down approach, in which investigator-driven research based on theories about a specific problem within a cultural group is used to modify an intervention (Lee et al., 2013). In sum, there are subtle distinctions in the ways in which culturally grounded approaches are used to develop social and behavioral interventions, compared with other approaches that are used to infuse cultural content in these interventions. Overall, the results of culturally grounded approaches are prevention programs with a high degree of social and cultural validity and “fit.”
Methodological Approaches to Culturally Grounded Prevention
There are several approaches in the design and implementation of culturally grounded prevention interventions. Okamoto et al. (2006) described the use of an ecologically based assessment that can serve as the foundation for such interventions. Ecologically based assessment involves the elucidation of specific environmental and cultural correlates of community problems, and is important for the development of prevention programs. This approach can build upon protective factors for minority youth populations, including indigenous youth (Okamoto et al., 2006). For example, as part of an ecologically based assessment, Napoli, Marsiglia, and Kulis (2003) surveyed a large subsample of indigenous youth in the Southwest US, and found that a strong sense of belonging in school provided a protective effect against drug use.
Community-based participatory research (CBPR) methods are another means toward developing a foundation for culturally grounded prevention programs. CBPR is an applied collaborative approach involving both researchers and community members in the research process (Horowitz, Robinson, & Seifer, 2009). Specific to culturally grounded prevention, CBPR provides one avenue toward promoting culturally appropriate preconception health care for American Indian youth (Richards & Mousseau, 2012). Richards and Mousseau’s use of CBPR was intended to increase the effectiveness of health promotion and prevention programs by involving the target community in the design, implementation, and evaluation of the programs. Through their use of CBPR, the investigators identified and created different methods for delivering a prevention message. They also used focus groups in the development of key media messages to increase community members’ knowledge of preconception health (Richards & Mousseau, 2012). Another form of community-based participatory research includes community-based participatory action research (PAR), in which both researchers and community members create prevention components with a focus towards social change. The purpose of PAR is to empower marginalized communities through their active involvement in the research process (Baum, MacDougall, & Smith, 2006). Helm et al. (2015) described the use of this method in the development of the Puni Ke Ola substance use prevention program for rural Native Hawaiian youth. Their approach to PAR utilized social action in support of Hawaiian approaches to community- and family-based wellness. Using a photovoice methodology, Hawaiian youth are currently developing prevention components in collaboration with researchers. These components are based largely on community landmarks, images, and references, their cultural significance, and how they can be used for psychosocial protection against substance use and abuse.
Relevance of the Study
Research has suggested that prevention programs may need to be culturally grounded for certain youth ethnic groups, such as indigenous youth, because the content or delivery of existing prevention programs are not as effective for these populations as for other youth ethnic groups (Dixon et al., 2007). The challenge of cultural grounding is that it is time consuming and expensive relative to cultural adaptations (Holleran Steiker et al., 2008; Okamoto et al., 2014). This is a particular concern for communities that have severe health disparities and require a more immediate public health response, and is particularly problematic in times of severe budget constraints. Our study is relevant because we provide some scientific direction for the use of culturally grounded methods for specific populations and regions, specifically pointing to the populations and regions where cultural grounding might be indicated. Further, culturally grounded prevention interventions have the potential to anchor culturally focused prevention within certain regions and with certain populations, addressing health disparities for targeted youth populations, while also providing a conceptually shorter adaptational bridge for programs focused on related populations and regions (Okamoto et al., 2014).
Using this logic, culturally grounded prevention programs developed for Native Hawaiian youth, for example, would have more applicability for adaptation to other indigenous youth (particularly those within the Pacific region) than programs developed for youth on the continental US, and could also serve as a template for adaptations to other Pacific Islander youth. This systematic review examines the characteristics of programs developed using culturally grounded approaches and can help to develop future youth prevention programs of this nature. Using specific inclusionary criteria, we provide specific information related to youth populations and regions using culturally grounded methods, as well as the means toward developing culturally grounded programs. This information can point to youth populations and regions underserved by grounded programs, allowing preventionists to respond to specific health-related needs. As such, this systematic literature review contributes to the alleviation of population-specific health disparities, and will aid in the creation of future culturally focused interventions for youth.
Method
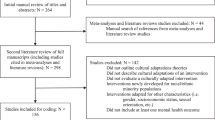
Figure 1 illustrates a flowchart of the process of identifying articles for this systematic review. In Step 1, the two primary authors conducted a computerized search of online databases including PsycNet, PubMed, EBSCO, and SocIndex. In each database, we used a combination of terms to search for related articles. These terms included “culturally grounded,” “prevention,” “youth,” “intervention,” “rural,” “adaptation,” and “culture.” During these searches, we used other related terms such as “adolescents” and “children” to expand the search perimeter. We also identified articles related to culturally grounded prevention programs for youth in several online registries [i.e., National Registry of Evidence-based Programs and Practices (NREPP), the Cochrane Library, and Blueprints for Healthy Youth Development]. In order to highlight recent studies, we limited these online database and registry searches to peer-reviewed articles published since 2003. The literature search in Step 1 yielded a total of 4340 articles. After cross-checking the databases and eliminating any duplicate articles, we reduced the total number of articles to 3276.

Method for literature review. This figure illustrates our process for identifying and reducing the number of articles included this review
In Step 2, the two primary authors read and evaluated all abstracts based on the inclusionary and exclusionary criteria for this study. Articles were included in this study if (1) they pertained to the development or evaluation of culturally grounded prevention programsFootnote 1 across multiple areas, such as substance abuse, suicide, and HIV; (2) they focused on non-majority youth (e.g., ethnic and/or sexual minority youth) who were ages 18 years or younger; and (3) they described an empirically based (data driven) approach toward the development of prevention programs. Articles were excluded in this study if (1) they focused on non-adapted or culturally adapted prevention programsFootnote 2 across multiple areas, such as substance abuse, suicide, and HIV; (2) they were non-empirical in nature (i.e., those in which data were not collected nor analyzed); (3) they focused on majority youth (e.g., White, middle class youth), or non-youth populations; (4) they focused exclusively on indigenous program development (e.g., grassroots programs; Lee et al., 2013); and (5) they were not peer reviewed. Based on our initial assessment using these criteria, we reduced the number of articles to 252. In Step 3, the two primary authors screened the full text of the remaining 252 articles using the inclusionary and exclusionary criteria, which further reduced the total number of articles to 55.
Finally, Step 4 of the process consisted of a further evaluation and validation of the remaining 55 articles. Additional co-authors screened and discussed the full text of each remaining article to determine whether or not it fully fit the inclusionary criteria. Through this process, we eliminated additional articles after further investigation showed that they did not fit these criteria. For example, we eliminated Brody, Yu, Chen, Kogan, and Smith (2012), because the authors focused on an adaptation of an existing group-based parenting skills training intervention for rural African American preadolescents that was originally developed by investigators from the same research team. Other studies were eliminated based on lack of evidence of cultural grounding (e.g., Pantin et al., 2009; Prado et al., 2007). Articles were also eliminated when we found that they took on a more indigenous approach to prevention described by Lee et al. (2013) or that they used the terms “cultural grounding” when, in fact, they used an adaptational approach (e.g., Colby et al., 2013). Upon completion of the validation process, 24 additional articles were excluded, resulting in a total of 31 articles for inclusion in this study.
Results
The 31 peer-reviewed articles which met the inclusionary criteria for this study are outlined in Table 1. The articles are summarized in terms of the research designs used in the studies, the demographics of the populations examined in the studies, and culturally grounded program characteristics and study outcomes.
Research Design
Of the 31 studies, 65 % focused on program efficacy or effectiveness, 29 % focused on pre-prevention or prevention program development, and 6 % focused on program implementation. Studies employed a variety of research methods, including randomized control trial designs (44 %), qualitative approaches (22 %), mixed methods (16 %), and quasi-experimental, correlational, or descriptive approaches (18 %). The majority of studies employed surveys or scales to measure program effects (65 %), while 30 % of these studies used focus groups in the development or evaluation of their programs. In regards to the delivery method, over half of the studies used a community-based approach. For example, the development of the Strong African American Families program involved seven consecutive weekly meetings held in community facilities with rural youth and families in Georgia (Brody, Chen, Kogan, Murry, & Brown, 2010). Thirty-two percent of the studies described a school-based approach toward delivering the prevention program, while 16 % used a mixture of both community-based and school-based approaches.
Study Demographics
The two most represented ethnicities in the studies were Mexican or Mexican–Americans and African Americans (29 and 23 %, respectively), followed by studies focused on North American indigenous groups (American Indians, Alaskan Natives, and Canadian Aboriginals; 19 %). An equal number of studies focused on Asian and/or Pacific Islander groups and African youth (13 % each). In terms of predominant study locations, 29 % took place in Arizona while another 23 % were conducted in Georgia (see Fig. 2). Further, a majority of the studies (58 %) occurred in rural areas, while roughly one-third took place in urban locations. The majority of youth participating in the research studies were between the ages of 10–12 years (38 %) and 13–15 years (36 %). Additionally, three-fourths of the studies focused solely on youth populations (74 %), and 23 % focused primarily on parents of youth in our target age range.

Location of studies. This figure summarizes the geographic focus of culturally grounded prevention studies included in this review
Program Characteristics and Outcomes
The majority of the studies in this review focused on three prevention programs–The Strong African American Families Program (SAAF; 23 %), keepin’ it R.E.A.L.Footnote 3 (23 %), and Ho‘ouna Pono (14 %; see Table 1). The majority of the prevention studies targeted substance use or abuse (33 %), followed by HIV/AIDS and STIs (22 %). The remaining studies focused on other health-related or behavioral issues, such as diabetes, teen dating violence, and pregnancy prevention. Thirty-seven percent of the studies used community-based participatory research (CBPR) as means for grounding (see Fig. 3). For example, Shaibi et al. (2012) collaborated with a local community clinic which serves uninsured Latino families and with a metropolitan YMCA in creating a culturally grounded diabetes prevention program. The three most frequent intervention components described in the studies were skills training (29 %), guided discussions and activities (27 %), and education (20 %).

Methods for grounding prevention programs. This figure illustrates the types of methods described in studies to “ground” prevention interventions
The two primary study outcomes were improved targeted behaviors related to the intervention (48 %) and increased cultural pride and/or awareness (14 %). As an example of the behavioral changes, Murry et al. (2011) found that the Strong African American Families Program demonstrated program-induced changes in parenting behaviors at approximately 5 year follow-up, such as improved parent–child communication. Goodkind, LaNoue, Lee, Lance Freeland, and Freund (2012) found an increase in positive coping strategies and social adjustment, as well as an increase in connectedness to a tribal affiliation, for American Indian and Alaskan Native youth participating in a mental health promotion program. In terms of cultural aspects and enculturation, Markus (2012) used photovoice to facilitate narratives related to elders’ storytelling and tribal histories, which in turn strengthened youth participants’ cultural identity and self-esteem.
Sixty-five percent of the articles included in this review focused specifically on program efficacy or effectiveness. This subset of studies was coded based on three types of program outcomes found to be significant in each study—(1) changes in knowledge of risky behaviors (e.g., an increase in understanding information related to unsafe sexual practices or substance use), (2) changes in attitudes related to risky behaviors (e.g., an increase in feelings or beliefs that supported anti-drug use or safe sex norms), and (3) changes in risk behaviors (e.g., a decrease in risky sexual behaviors or substance use). The majority of the efficacy or effectiveness studies included in this review found significant positive effects on youths’ behaviors and attitudes (55 %), followed by youths’ behaviors (25 %) and youths’ attitudes (10 %).
Discussion
The two programs with the most published research were the Strong African American Families Program (SAAF) and keepin’ it R.E.A.L. These programs focused on African American and Mexican–American youth, respectively, and accounted for most of the research on these populations included in this review. Numerous studies have reported on the development and testing of SAAF and keepin’ it R.E.A.L. since 2003, whereas other programs, such as MEMA kwa VijanaFootnote 4 or the Mpondombili Project, appear to have been studied for several years but have substantially fewer studies associated with them. Research related to other culturally grounded programs, such as Ho‘ouna Pono or Wind River UNITY Photovoice for Healthy Relationships, have been published more recently and appear to be in earlier stages of program development and evaluation. The numerous studies analyzing different aspects of SAAF and keepin’ it R.E.A.L. provide greater depth into reasons behind their effectiveness compared to the other programs included in this review, and highlight the conditions that contribute to behavioral and attitudinal changes within the target populations as a result of participation in the programs. Common characteristics of these effective programs include a focus on building skills for health-promoting behaviors (e.g., positive parenting practices and drug resistance skills), a focus on specific ethnocultural and regional values, beliefs, and worldviews, and the use of interactive techniques (e.g., discussions and activities) to convey the prevention message.
A significant portion of the studies in this review also focused on North American indigenous groups (i.e., American Indians, Alaskan Natives, and Canadian Aboriginals); however, these studies focused on a variety of different prevention programs rather than on only one or two programs. The diversity of programs targeting these populations reflects the diversity of indigenous populations in general, but the relative shortage of studies on each of these different programs suggests a lack of depth in understanding reasons for their effectiveness in addressing various health disparities for indigenous youth populations. This suggests the need for more research related to measuring and identifying effective prevention principles and practices for indigenous youth populations.
Populations that were not the focus of as many culturally grounded studies included Native Hawaiians and other Pacific Islanders, Asians or Asian Americans, and Africans. Populations absent from any culturally grounded studies in this review included those from the Middle East and Southeast Asia. The lack or absence of culturally grounded research with these populations suggests directions for future development in culturally grounded prevention programs within specific regions and ethnic groups. Culturally grounded prevention research may serve to anchor prevention programs within these specific contexts, providing a foundation for culturally and regionally specific program adaptations to related youth populations (Okamoto et al., 2014).
The majority of sampled youth included in the studies ranged from ages 10 to 15 years, which corresponded to grades 5–9. Study investigators and program developers might have targeted this age range in order to address youth risk behaviors before or close to their onset. Recent epidemiological research has illustrated sharp increases in self-reported alcohol consumption and sexual intercourse between grades 7 and 8 (Center for Disease Control and Prevention, 2011). Prevention programs may have been timed to address these behaviors at their onset through the use of culturally relevant skills and strategies to deal with them.
The large majority of the culturally grounded programs in this review were implemented and evaluated in rural locations. The norms of rural communities align with the development of culturally grounded interventions, because they both expect active stakeholder investment and collaboration (Okamoto et al., 2014). In comparison, the diversity of values and cultures across urban communities could make grounding prevention programs into one unified culture difficult for developers in these settings. There may be a greater sense of social diversity and disorganization in urban settings that could hinder the grounding process, while common goals, values, and a greater sense of community involvement in rural settings may serve to support the process. These characteristics of rural communities may serve to promote and sustain culturally grounded efforts over lengthy time periods, which may have contributed to the number of studies occurring in these types of communities.
All the studies in this review described close collaboration with the target populations and their communities in order to create culturally grounded prevention interventions. Over half of the studies described how extensive information from community stakeholders and consumers was collected through the use of focus groups, community-based participatory research (CBPR), and participatory action research (PAR) strategies, and how this information could be used for grounding programs. This suggests that close collaboration with the target community or population is critical to the development of culturally grounded prevention programs. CBPR and PAR strategies incorporate qualitative methods such as focus groups and interviews, and facilitate collective opportunities for the target population to analyze and determine the culturally grounded intervention methods that work best within their communities. As an example, Gosin and colleagues explain how CBPR principles were used in the development of the keepin’ it R.E.A.L. program in order to make the program non-threatening, interactive, and fun for the youth (Gosin, Marsiglia, & Hecht, 2003; Gosin, Dustman, Drapeau, & Harthun, 2003). Further, related research on the development of the program highlighted the importance of youth participants’ narratives, because they described the influence of youths’ cultural values on their reactions to drug offers (Gosin et al., 2003).
Finally, studies included in this review used a variety of research designs in the development and evaluation of culturally grounded programs, including randomized controlled trial designs, qualitative designs, and quasi-experimental designs. While this demonstrates that there are various empirical approaches to develop and evaluate these types of programs, it also suggests that researchers and program developers may need to be flexible in the designs that are used in culturally grounded prevention research. Specifically, Whitbeck, Walls, and Welch (2012) discuss the conflict that often arises between cultural values and research methods, such as how “gold standard” research designs (i.e., randomized controlled trials) involve withholding a potentially effective intervention to a portion of the target population who believe they have ownership and rights to the use of the program. The heterogeneity of different research designs used in the studies suggest that researchers involved in the development of culturally grounded programs need to be methodologically flexible, in order to balance community expectations and needs with the demand for scientific rigor.
Limitations of the Study
There were several limitations to this study. One is that this literature review was restricted to recent published articles only. Thus, community-based, culturally grounded programs in the early (pre-publication) stages of development and/or validation, or unpublished programs of this nature, were not captured in this review. Another limitation was the lack of specific information related to program development in several of the published articles. Specifically, several of these articles included descriptions of culturally focused prevention curricula, but did not describe the methods used to develop those curricula (e.g., Carter, Straits, & Hall, 2007; Prado et al., 2007). These programs may or may not have utilized a grounded approach to program development. To be conservative in our review, these articles were excluded from our analysis. As a result, our findings may not constitute a complete representation of all the culturally grounded prevention methods being utilized.
Conclusion
Despite its utilization over the past decade, culturally grounded prevention is an under-acknowledged approach to developing culturally specific prevention programs. This review of published literature on culturally grounded prevention has highlighted the application of this approach, including the methods of developing and evaluating these programs to address health disparities in minority youth populations. The majority of the studies in this review focused on programs targeting health disparities in African American, Mexican–American, and American Indian/Alaska Native youth and on programs developed with rural communities. Future research might target populations or regions that are underserved by culturally grounded prevention programs, such as those within the Middle East and Southeast Asia, as well as expand upon research in the Pacific and Africa, in order to anchor culturally focused prevention within those areas. More research may also be needed to measure the effectiveness of existing culturally grounded prevention programs with few studies, particularly those targeting American Indian youth.
Notes
In this study, we defined culturally adapted prevention programs as those that were tailored for a cultural group that were different from the group(s) for whom the original intervention was developed (Okamoto et al., 2014).
“R.E.A.L.” stands for “Refuse,” “Explain,” “Avoid,” and “Leave.” These are the primary drug resistance skills taught in the curriculum (Hecht, 2006).
The full name of the program in Swahili is “Mpango wa Elimu na Maadili ya Afya (MEMA) kwa Vijana,” which roughly translates to “program of education for health-related behavior for young people” (Hayes et al., 2005).
References
References marked with an asterisk indicate studies that were included in this literature review.
Barrera, M., Castro, F. G., Strycker, L. A., & Toobert, D. J. (2013). Cultural adaptations of behavioral health interventions: A progress report. Journal of Consulting and Clinical Psychology, 81(2), 196–205.
Baum, F., MacDougall, C., & Smith, D. (2006). Participatory action research. Journal of Epidemiology and Community Health, 60(10), 854–857.
Bernal, G., Jiménez-Chafey, M. I., & Domenech Rodríguez, M. M. (2009). Cultural adaptation of treatments: A resource for considering culture in evidence-based practice. Professional Psychology: Research and Practice, 40(4), 361–368.
*Brody, G. H., Chen, Y. F., Kogan, S. M., Murry, V. M., & Brown, A. C. (2010). Long-term effects of the strong African American families program on marked list youths’ alcohol use. Journal of Consulting and Clinical Psychology, 78(2), 281–285.
*Brody, G. H., Kogan, S. M., Chen, Y. F., & McBride Murry, V. (2008). Long-term effects of the strong African American families program on youths’ conduct problems. Journal of Adolescent Health, 43(5), 474–481.
*Brody, G. H., Murry, V. M., Kogan, S. M., Gerrard, M., Gibbons, F. X., Molgaard, V., et al. (2006). The Strong African American Families Program: A cluster-randomized prevention trial of long-term effects and a mediational model. Journal of Consulting and Clinical Psychology, 74(2), 356–366.
*Brody, G. H., Murry, V. M., McNair, L., Chen, Y. F., Gibbons, F. X., Gerrard, M., et al. (2005). Linking changes in parenting to parent-child relationship quality and youth self-control: The Strong African American Families program. Journal of Research on Adolescence, 15(1), 47–69.
Brody, G. H., Yu, T., Chen, Y. F., Kogan, S. M., & Smith, K. (2012). The adults in the making program: Long-term protective stabilizing effects on alcohol use and substance use problems for rural African American emerging adults. Journal of Consulting and Clinical Psychology, 80(1), 17–28.
Carter, S., Straits, K. J. E., & Hall, M. (2007). Project venture: Evaluation of an experiential, culturally based approach to substance abuse prevention with American Indian youth. Journal of Experiential Education, 29(3), 397–400.
Castro, F. G., Barrera, M., & Holleran Steiker, L. K. (2010). Issues and challenges in the design of culturally adapted evidence-based interventions. Annual Review of Clinical Psychology, 6, 213–239.
Castro, F. G., Barrera, M., & Martinez, C. R. (2004). The cultural adaptation of prevention interventions: Resolving tensions between fidelity and fit. Prevention Science, 5(1), 41–45.
Center for Disease Control and Prevention. (2011). Youth online: Middle school YRBS, 2011 Results. http://apps.nccd.cdc.gov/youthonline/.
Colby, M., Hecht, M. L., Miller-Day, M., Krieger, J. L., Syvertsen, A. K., Graham, J. W., et al. (2013). Adapting school-based substance use prevention curriculum through cultural grounding: A review and exemplar of adaptation processes for rural schools. American Journal of Community Psychology, 51(1–2), 190–205.
Dixon, A. L., Yabiku, S. T., Okamoto, S. K., Tann, S. S., Marsiglia, F. F., Kulis, S., et al. (2007). The efficacy of a multicultural prevention intervention among urban American Indian youth in the southwest U.S. The Journal of Primary Prevention, 28(6), 547–568.
*Gerrard, M., Gibbons, F. X., Brody, G. H., Murry, V. M., Cleveland, M. J., & Wills, T. A. (2006). A theory-based dual-focus alcohol intervention for preadolescents: The Strong African American Families Program. Psychology of Addictive Behaviors, 20(2), 185–195.
*Goodkind, J., LaNoue, M., Lee, C., Freeland, L., & Freund, R. (2012). Feasibility, acceptability, and initial findings from a community-based cultural mental health intervention for American Indian Youth and their families. Journal of Community Psychology, 40(4), 381–405.
*Gosin, M., Marsiglia, F. F., & Hecht, M. L. (2003). keepin’ it R.E.A.L.: A drug resistance curriculum tailored to the strengths and needs of pre-adolescents of the southwest. Journal on Drug Education, 33(2), 119–142.
*Guilamo-Ramos, V., Soletti, A. B., Burnette, D., Sharma, S., Leavitt, S., & McCarthy, K. (2012). Parent–adolescent communication about sex in rural India: US–India collaboration to prevent adolescent HIV. Qualitative Health Research, 22(6), 788–800.
*Hayes, R. J., Changalucha, J., Ross, D. A., Gavyole, A., Todd, J., Obasi, A. I., et al. (2005). The MEMA kwa Vijana project: Design of a community randomised trial of an innovative adolescent sexual health intervention in rural Tanzania. Contemporary Clinical Trials, 26(4), 430–442.
*Hecht, M. L. (2006). The principle of cultural grounding in school-based substance abuse prevention: The Drug Resistance Strategies Project. Journal of Language and Social Psychology, 25(3), 301–319.
Helm, S., Lee, W., Hanakahi, V., Gleason, K., McCarthy, K., & Haumana. (2015). Using photovoice with youth to develop a drug prevention program in a rural Hawaiian community. American Indian and Alaska Native Mental Health Research, 22(1), 1–26.
Holleran Steiker, L. K., Castro, F. G., Kumpfer, K., Marsiglia, F. F., Coard, S., & Hopson, L. M. (2008). A dialogue regarding cultural adaptation of interventions. Journal of Social Work Practice in the Addictions, 8(1), 154–162.
Horowitz, C. R., Robinson, M., & Seifer, S. (2009). Community-based participatory resarch from the margin to the mainstream: Are researchers prepared? Circulation, 119, 2633–2642.
*Isaak, C. A., Campeau, M., Katz, L. Y., Enns, M. W., Elias, B., & Sareen, J. (2009). Community-based suicide prevention research in remote on-reserve First Nations communities. International Journal of Mental Health and Addiction, 8(2), 258–270.
*Kaufman, C. E., Mitchell, C. M., Beals, J., Desserich, J. A., Wheeler, C., Keane, E. M., et al. (2010). Circle of life: Rationale, design, and baseline results of an HIV prevention intervention among young American Indian adolescents of the Northern Plains. Prevention Science, 11(1), 101–112.
*Kulis, S., Marsiglia, F. F., Elek, E., Dustman, P., Wagstaff, D. A., & Hecht, M. L. (2005). Mexican/Mexican American adolescents and keepin’ it R.E.A.L.: An evidence-based subsance use prevention program. Children & Schools, 27(3), 133–145.
Lee, R., Vu, A., & Lau, A. (2013). Culture and evidence-based prevention programs. In F. Paniagua & A.-M. Yamada (Eds.), Handbook of Multicultural Mental Health (pp. 525–564). Oxford: Elsevier Inc.
*Mantell, J. E., Harrison, A., Hoffman, S., Smit, J. A., Stein, Z. A., & Exner, T. M. (2006). The Mpondombili Project: Preventing HIV/AIDS and unintended pregnancy among rural South African school-going adolescents. Reproductive Health Matters, 14(28), 113–122.
*Markus, S. F. (2012). Photovoice for healthy relationships: Community-based participatory HIV prevention in a rural American Indian community. American Indian and Alaska Native Mental Health Research, 19(1), 102–123.
*Marsiglia, F. F., Kulis, S., Wagstaff, D. A., Elek, E., & Dran, D. (2005). Acculturation status and substance use prevention with Mexican and Mexica–American Youth. Journal of Social Work Practice in the Addictions, 5(1–2), 85–111.
*Marsiglia, F. F., Yabiku, S., Kulis, S., Nieri, T., & Lewin, B. (2010). Influences of school Latino composition and linguistic acculturation on a prevention program for youths. Social Work Research, 34(1), 6–19.
*Moran, J. R., & Bussey, M. (2006). Results of an Alcohol Prevention Program with Urban American Indian Youth. Child and Adolescent Social Work Journal, 24(1), 1–21.
*Murry, V. M., Berkel, C., Brody, G. H., Gerrard, M., & Gibbons, F. X. (2007). The Strong African American Families program: Longitudinal pathways to sexual risk reduction. Journal of Adolescent Health, 41(4), 333–342.
*Murry, V. M., Berkel, C., Chen, Y. F., Brody, G. H., Gibbons, F. X., & Gerrard, M. (2011). Intervention induced changes on parenting practices, youth self-pride and sexual norms to reduce HIV-related behaviors among rural African American youths. Journal of Youth Adolescence, 40(9), 1147–1163.
Napoli, M., Marsiglia, F. F., & Kulis, S. (2003). Sense of belonging in school as a protective factor against drug abuse among Native American urban adolescents. Journal of Social Work Practice in the Addictions, 3(2), 25–41.
*Obasi, A. I., Cleophas, B., Ross, D. A., Chima, K. L., Mmassy, G., Gavyole, A., et al. (2006). Rationale and design of the MEMA kwa Vijana adolescent sexual and reproductive health intervention in Mwanza Region, Tanzania. AIDS Care, 18(4), 311–322.
*Okamoto, S. K., Helm, S., Giroux, D., & Kaliades, A. (2011). “I no like get caught using drugs”: Explanations for refusal as a drug resistance strategy for rural Native Hawaiian youths. Journal of Ethnic & Cultural Diversity in Social Work, 20(2), 150–166.
*Okamoto, S. K., Helm, S., Giroux, D., Edwards, C., & Kulis, S. (2010a). The development and initial validation of the Hawaiian Youth Drug Offers Survey (HYDOS). Ethnicity and Health, 15(1), 73–92.
Okamoto, S. K., Helm, S., Pel, S., McClain, L. L., Hill, A. P., & Hayashida, J. K. P. (2014a). Developing empirically based, culturally grounded drug prevention interventions for indigenous youth populations. Journal of Behavioral Health Services & Research, 41(1), 8–19.
*Okamoto, S. K., Helm, S., Poa-Kekuawela, K., Chin, C. I. H., & Nebre, L. H. (2010b). Exploring culturally specific drug resistance strategies of Hawaiian youth in rural communities. Journal of Alcohol and Drug Education, 54(1), 56–75.
Okamoto, S. K., Kulis, S., Marsiglia, F. F., Holleran Steiker, L. K., & Dustman, P. A. (2014b). A continuum of approaches toward developing culturally focused prevention interventions: From adaptation to grounding. The Journal of Primary Prevention, 35, 103–112.
Okamoto, S. K., LeCroy, C. W., Tann, S. S., Rayle, A. D., Kulis, S., Dustman, P., et al. (2006). The implications of ecologically based assessment for primary prevention with indigenous youth populations. The Journal of Primary Prevention, 27(2), 155–170.
*Okamoto, S. K., Pel, S., Helm, S., & Valdez, J. K. (2014c). Gender differences in the use of drug resistance strategies: An analysis of rural Asian/Pacific Islander youth. Health Promotion Practice, 15(4), 568–574.
Pantin, H., Prado, G., Lopez, B., Huang, S., Tapia, M. I., Schwartz, S. J., et al. (2009). A randomized controlled trial of Familias Unidas for Hispanic adolescents with behavior problems. Psychosomatic Medicine, 71(9), 987–995.
*Plummer, M. L., Wight, D., Obasi, A. I., Wamoyi, J., Mshana, G., Todd, J., et al. (2007). A process evaluation of a school-based adolescent sexual health intervention in rural Tanzania: The MEMA kwa Vijana programme. Health Education Research, 22(4), 500–512.
Prado, G., Pantin, H., Briones, E., Schwartz, S. J., Feaster, D., Huang, S., et al. (2007). A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. Journal of Consulting and Clinical Psychology, 75(6), 914–926.
Resnicow, K., Baranowski, T., Ahluwalia, J. S., & Braithwaite, R. L. (1999). Cultural sensitivity and public health: Defined and demystified. Ethnicity and Disease, 9, 10–21.
Resnicow, K., Soler, R., Braithwaite, R., Ahluwalia, J. S., & Butler, J. (2000). Cultural sensitivity in substance use prevention. Journal of Community Psychology, 28(3), 271–290.
*Richards, J., & Mousseau, A. (2012). Community-based participatory research to improve preconception health among Northern Plains American Indian adolescent women. American Indian & Alaska Native Mental Health Research, 154–185.
*Shaibi, G. Q., Konopken, Y., Hoppin, E., Keller, C. S., Ortega, R., & Castro, F. G. (2012). Effects of a culturally grounded community-based diabetes prevention program for obese Latino adolescents. The Diabetes Educator, 38(4), 504–512.
Whitbeck, L. B., Walls, M. L., & Welch, M. L. (2012). Substance abuse prevention in American Indian and Alaska Native communities. The American Journal of Drug and Alcohol Abuse, 38(5), 428–435.
*Warren, J. R., Hecht, M. L., Wagstaff, D. A., Elek, E., Ndiaye, K., Dustman, P., et al. (2006). Communicating prevention: The effects of the keepin’ it REAL classroom videotapes and televised PSAs on middle-school students’ substance use. Journal of Applied Communication Research, 34(2), 209–227.
*Williams, L. R., Adams, H. L., & Altamirano, B. N. (2012). Mexican American adolescents’ perceptions of dating violence programs: Recommendations for effective program design and implementation. Qualitative Social Work, 11(4), 395–411.
*Yabiku, S., Kulis, S., Marsiglia, F. F., Lewin, B., Nieri, T., & Hussaini, S. (2007). Neighborhood effects on the efficacy of a program to prevent youth alcohol use. Substance Use and Misuse, 42(1), 65–87.
Acknowledgments
Resources used in preparation of this study were funded by the National Institutes of Health/National Institute on Drug Abuse under Grant R34 DA031306. The authors wish to acknowledge Ms. Jessica Mabanag and Ms. Kaycee Bills for their assistance with manuscript preparation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to report in the publication of this manuscript.
Rights and permissions
About this article

Cite this article
Lauricella, M., Valdez, J.K., Okamoto, S.K. et al. Culturally Grounded Prevention for Minority Youth Populations: A Systematic Review of the Literature. J Primary Prevent 37, 11–32 (2016). https://doi.org/10.1007/s10935-015-0414-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10935-015-0414-3