
Abstract
Project Northland was a randomized community trial to prevent or delay alcohol use among adolescents. Students in the intervention communities were exposed to a multi-component prevention program in early adolescence and high school. This paper examines the impact of Project Northland on the trajectories of four scales of the adolescent form of the Minnesota Multiphasic Personality Inventory (MMPI-A). Students in the intervention communities demonstrated lower rates of growth of family problems and alcohol/drug use proneness than students in the delayed-program control communities. The results were more robust for baseline non-drinkers. Editors’ Strategic Implications: This experimental study extends the scope of the impact of Project Northland, already recognized as a model substance abuse prevention program by the Substance Abuse and Mental Health Services Administration. The results suggest that focused prevention programs have the potential to impact young adolescents’ lives more broadly. Replication and further examination of the mechanisms by which risk factors and outcomes are modified is necessary, but school administrators and public health officials could learn from this promising program and evaluation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Adolescent alcohol use is one of the most difficult behaviors to change because alcohol use is so widely accepted in U.S. culture (Institute of Medicine 2004). In fact, moderate alcohol use is prescribed for adults as a way to prevent cardiovascular diseases (Murray et al. 2002), while it is proscribed for children and adolescents. These mixed messages about alcohol use create a scenario that is quite different than for cigarette smoking or illicit drug use, where there are clearer messages about health consequences and illegality, respectively, and makes prevention efforts to reduce adolescent alcohol use considerably more challenging.
Alcohol is the most commonly used psychoactive drug among adolescents (Guo et al. 2000), with 41% of 8th graders, 63% of 10th graders, and 75% of 12th graders reporting ever having used alcohol in 2005 (Johnston et al. 2005). Still, early adolescent alcohol use is precocious and associated with multiple social, behavioral, and developmental problems (Ellickson et al. 2003; Grant and Dawson 1997; Greenblatt 2000; Gruber et al. 1996; Hingson et al. 2002; Hingson et al. 2003). Early alcohol use is associated with heavier use of alcohol and problem behaviors in later adolescence including alcohol-related violence, injuries, drinking and driving, other drug use and absenteeism from work or school (Gruber et al. 1996). Youth who drink before age 15 are estimated to be four times more likely to develop alcohol dependence in adulthood than those who begin drinking at age 18 or older (Grant and Dawson 1997; Substance Abuse and Mental Health Services Administration 2004). Clearly, alcohol use prevention programs that target young adolescents and successfully address potent risk factors for early use are of critical public health importance.
The school and family are particularly important social contexts for early adolescent alcohol use and provide the primary social risk and protective factors for alcohol use onset and progression (Resnick et al. 1997). The school setting incorporates the peer group, and alcohol use by friends, perceptions of use, and the association with peers who engage in deviant behavior are strongly associated with earlier alcohol use onset (Donovan et al. 2004; Hipwell et al. 2005; Iannotti et al. 1996; Kosterman et al. 2000; Marshal and Chassin 2000). Cross-sectional data from the National Longitudinal Study of Adolescent Health indicate that school factors, particularly school connectedness, account for 4–6% of the variability in alcohol use among 7th through 12th grade students; family factors such as family connectedness and household access to alcohol, account for 9% of the variability in alcohol use among 7th and 8th grade students, and 6% of the variability among 9th through 12th grade students (Resnick et al. 1997). In particular, parental monitoring appears to be protective, with low levels of parental monitoring in childhood and early adolescence consistently associated with an increase in alcohol use (Bray et al. 2001; Donovan et al. 2004; Guo et al. 2001; Kaplow et al. 2002; Li et al. 2000). Unsupportive and demanding family environments, permissiveness, family dysfunction, and parental alcohol abuse are also associated with increased risk of early alcohol use (Colder and Chassin 1999; Donovan et al. 2004; Jackson et al. 1999).
While there has been considerable work on how school and family factors influence adolescent alcohol use, far less attention has been given to the impact of reducing adolescent alcohol use on school and family functioning. Randomized trials of adolescents with substance use disorders have shown that reductions in drug use were associated with improvements in other contexts such as school and family (Henggeler et al. 2002; Liddle et al. 2001). Still, few alcohol prevention programs have examined their impact beyond behaviors targeted directly by the interventions and their mediating psychosocial factors (Botvin et al. 1995; Ellickson et al. 2003; Spoth et al. 1999).
Project Northland was an alcohol use prevention program for 6th through 12th grade students that was undertaken in northeastern Minnesota from 1991–1998 (Perry et al. 1993). The project was a randomized community trial with 24 school districts and 28 surrounding communities randomized to intervention and delayed-program control conditions. The project targeted the Class of 1998 beginning in their 6th grade year (Komro et al. 1999; Perry et al. 1993; Perry et al. 2000; Perry et al. 1996; Williams et al. 1995a). The project was successful in significantly reducing the onset and prevalence of alcohol by 8th grade (Perry et al. 1996), and altering the normative trajectories of alcohol use in 6th through 8th and 10th through 12th grades, during the active intervention phases (Perry et al. 2002). Significant mediators of the intervention effects for the early adolescent phase included: peer influence to use, functional meanings of use, proneness to alcohol use such as stimulus-seeking, parent-child communication, and self-efficacy to handle alcohol use offers (Komro et al. 2001). A recent analysis of projects funded by the State Incentive Grant mechanism reinforced the effectiveness of Project Northland among young adolescents (Flewelling et al. 2005). Project Northland was named one of the first “model” substance abuse prevention programs in the country as designated by the federal Substance Abuse and Mental Health Services Administration (see www.modelprograms.samhsa.gov).
Included in Project Northland’s annual survey of alcohol use behaviors and related psychosocial factors administered each year, from 6th to 12th grades, to the Project Northland cohort, were 110 items from the 478 item Minnesota Multiphasic Personality Inventory-Adolescent (MMPI-A) (Butcher and Williams 1992), a widely used objective measure of psychopathology during adolescence. The 110 items included in the Project Northland student survey allowed for the scoring of five MMPI-A scales that assess behavioral and emotional problems at school and in the family, as well as substance abuse. These MMPI-A scales were selected for their potential utility in determining the broader impact of a preventive intervention like Project Northland (Williams et al. 1999). To date, no other universal prevention programs have assessed program outcomes using clinically valid measures from the MMPI-A to assess changes in adolescents over time.
The MMPI-A scales were examined at the end of the early adolescent phase of Project Northland, using mixed model analyses of covariance, and there were differences between treatment conditions on the Alcohol/Drug Problems Proneness scale (Williams et al. 1999). It seemed important, given the uniqueness of this data set, to further assess the impact of Project Northland by examining the trajectories of each of the selected MMPI-A scales over time for both the early adolescent and high school phases of the project, using growth curve models, to determine how Project Northland may have impacted the trajectories of growth in multiple important areas of adolescents’ lives.
Methods
The aim of the current study is to determine whether the Project Northland intervention had an impact on selected MMPI-A scales measuring clinically relevant problems. It was hypothesized that students who were exposed to Project Northland would have fewer behavioral and emotional difficulties within their families and at school, would report fewer indicators of alcohol and other drug-related disorders, and would demonstrate a lower probability of being substance abusers compared to students in the delayed-program control condition who were not exposed to Project Northland.
Study Design and Intervention Programs
Project Northland was conducted from 1991 to 1998 in six counties in northeastern Minnesota and involved mostly white, rural, lower-middle class to middle-class communities. Twenty-four school districts were recruited to participate in the study in 1990. Four school districts were very small and so were combined with adjacent school districts prior to randomization in order to have sufficient sample sizes in each unit. One school district dropped out during the cohort’s 9th grade, but re-joined the study in the cohort’s 11th grade after a change in school district administration. The 20 combined school districts and adjoining communities were randomly assigned to intervention or delayed-program control conditions at baseline and remained in those conditions throughout the study period. The primary study sample is the Class of 1998 (N = 3151), followed from 6th through 12th grades.
The intervention program is discussed in detail in other publications (Komro et al. 1999; Perry et al. 1993; Perry et al. 2000; Perry et al. 1996; Williams et al. 1995a). The intervention had three phases, an early adolescent phase (6–8th grades), an interim phase (9–10th grades), and a high school phase (11–12th grades) (Perry et al. 2002). The interim phase was less intensive because of funding constraints. The delayed-program control schools received Project Northland training and program materials following the active study phases in 1994 and 1998; otherwise they participated in their usual alcohol and drug use prevention programs.
The intervention program for the early adolescent and follow-up phase consisted of four years of behavioral curricula implemented by teachers and peer leaders in the classrooms (when the cohort was in 6th through 9th grades), and three years of parental involvement and education, peer leadership opportunities, and community task force activities (when the cohort was in the 6th through 8th grades). There were no intervention programs when the cohort was in the 10th grade. Full descriptions of these intervention programs can be found in other reports (Perry et al. 1996; Williams et al. 1999). The early adolescent phase was successful in reducing past week and past month alcohol use among all students, and additionally, tobacco and marijuana use among baseline non-users of alcohol (Perry et al. 1996).
The intervention program for the high school phase consisted of a one-year classroom curriculum (when the cohort was in the 11th grade), and two years of parental education and involvement via print media, community-wide media campaigns and print media distributions, peer action teams to encourage alcohol-free activities and high school events, and community action teams to promote policy change concerning access to alcohol (when the cohort was in the 11th and 12th grades). Greater detail on the high school phase programs can be found elsewhere (Perry et al. 2000; Perry et al. 2002). The high school phase was successful in reducing the trajectories of alcohol use behavior and intentions as well as binge drinking over the course of 10–12th grades (Perry et al. 2002).
Study Sample
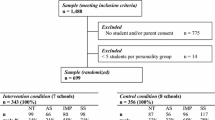
Students in the intervention and delayed-program control school districts were administered the selected MMPI-A items at baseline in fall 1991, and follow-up each year in spring 1992–1998. The sample size for the entire study was 3151, which included students who had participated in at least one wave of surveys. There were 198 students who moved between school districts during the seven years of data collection and these students were dropped from the analyses, reducing the sample size to 2953. Students who had three or more inconsistent responses in a survey were dropped from that data point. On average, 0.01% of students were dropped each year due to inconsistent responses. Students also had to meet validity criteria for MMPI-A responses using an abbreviated version of the Variable Response Inconsistency (VRIN) scale (Williams et al. 1999). Values for students not meeting these criteria were set to missing in the analyses (about 1% of the sample, n = 33).
Two samples of students were used for the analyses to examine intervention effects: (1) those who participated in the early adolescent and follow-up phase, and (2) those who participated in the high school phase. The first sample included students who had (a) baseline data in 1991 (6th grade), (b) at least one data point between 1992 and 1994 (6–8th grades), and (c) had at least one data point between 1995 and 1996 (9–10th grades). This assured that the sample consisted of students who had been exposed to the early adolescent phase of the project and follow-up period. The first sample had a sample size of 1857.
The second high school sample included participants in the analyses who had (a) baseline data in 1991 (6th grade), (b) at least one data point between 1992 and 1994 (6th–8th grades), and (c) at least one data point between 1997 and 1998 (11–12th grades). This assured that the sample consisted of students who had been exposed to the early adolescent and high school phases of the study. The second sample had a sample size of 1701. Within the two samples, baseline users of alcohol included those students who reported ever having had a drink of alcohol at baseline in 6th grade, while baseline non-users reported never having had a drink.
There were no gender differences between those who were included versus those who were excluded by condition. There was a significant race difference, however, so that students who were in the intervention condition but excluded from the analyses were more likely to be non-whites than those who were included, χ2 (3, 2953) = 89.62, P < .001).
Measures
Because of time constraints, the entire MMPI-A could not be administered to the cohort. The four MMPI-A scales evaluated for these analyses included two of the MMPI-A Content Scales (Williams et al. 1992): the 35 item Family Problems Scale (A-fam) and 20 item School Problems Scale (A-sch). Also included were two scales developed to measure alcohol and drug problems (Weed et al. 1994): the 13 item Alcohol/Drug Problem Acknowledgement Scale (ACK) and the 36 item Alcohol/Drug Problems Proneness Scale (PRO). One additional scale was administered to the students, the Low Aspirations Content Scale, which is associated with poor achievement and limited school participation, but was excluded from the current analyses because A-sch is more highly associated with serious behavior problems in the school setting and because of some overlap between ACK and the other scales (Forbey and Ben-Porath 2003; Williams et al. 1992).
The psychometric characteristics of A-fam and A-sch were previously presented (Williams et al. 1992), and subsequent studies provided further support for their external validity (Forbey and Ben-Porath 2003; Rinaldo and Baer 2003; Williams et al. 1995b). High scores on A-fam signify multiple and serious problems within the young person’s family, including a wide variety of both acting out behaviors (e.g., aggression, running away), emotional symptoms (e.g., depression, withdrawal), and reports of abuse. High scores on A-sch indicate numerous problems in school including poor grades, suspensions, truancy, underachievement, dropping out, and cheating or lying.
Additional research has also supported the external validity of the two MMPI-A Alcohol/Drug Problems scales, ACK and PRO (e.g., Micucci 2002; Stein and Graham 2001, 2005; Williams 1995b). ACK consists of 13 obvious items related to substance abuse (e.g., fighting while drinking, descriptions of blackouts, drinking excessively, marijuana use). Similar to PRO, it has been shown to discriminate between adolescents in general population, substance abuse treatment, and psychiatric treatment samples (Weed et al. 1994). Both scales have also been shown to discriminate within an inpatient psychiatric sample those adolescents with comorbid substance abuse disorders from those who do not have them (Micucci 2002) and to detect substance abuse in juvenile correctional settings (Stein and Graham 2001, 2005). High scorers on ACK report multiple indicators of substance abuse disorders, and have a higher probability of having a substance abuse diagnosis than low scorers.
PRO was developed as an empirical, rather than content-based, MMPI-A measure for identifying adolescents likely to abuse alcohol or other drugs, but who do not endorse obvious items of problematic use (Weed et al. 1994). Empirically-derived scales like PRO are thought to be more resistant to under-reporting of problems (Stein and Graham 2005; Weed et al. 1994). PRO item content includes several of the risk factors for early adolescent alcohol use (e.g., negative peer group influences, less involvement with parents, deviant behaviors like stealing and lying, rule breaking, stimulus seeking, less achievement orientation). Although it is not as direct or strong a measure of substance abuse problems as is ACK, there is some evidence of its relationship to substance abuse problems (Micucci 2002; Stein and Graham 2001; Weed et al. 1994). High scores on PRO indicate a higher probability that given individuals are more like youth in residential treatment for alcohol and drug problems than those with lower scores. In addition, there are also indications that PRO may be measuring a constellation of risk factors and/or consequences of substance abuse problems. For example, Williams et al. (1995b) found that both PRO and ACK were related to measures of peer influence and self-efficacy to turn down offers of alcohol in young adolescents.
Analysis Methods
Differences in changes over time between the intervention and delayed-program control conditions were tested using mixed-effects regression models for repeated measures data (i.e., growth curve models). Growth curve analysis allows one to identify patterns of growth or change over time and test whether these patterns differ between subgroups (e.g., intervention conditions). Mixed-effects regression models can accommodate fixed effects, random effects and correlated observations within study units. One of the strengths of this approach is its ability to flexibly and appropriately model the structure of the data, including data arising from a cluster sampling scheme and unbalanced, or missing data. The mixed effects regression model is also particularly useful because it not only models the process of change for the population, but also the process of change for individuals, who can differ in idiosyncratic ways (Raudenbush and Bryk 2002; Singer and Willett 2003).
Two sets of growth curve analyses were conducted, for the early adolescent and follow-up phase (6–10th grades), and the high school phase (10–12th grades). Analyses were conducted separately for each of the four MMPI-A scales: A-fam, A-sch, ACK, and PRO. For the early adolescent and follow-up phase (6–10th grades), examination of the observed growth curves on the four scales showed that the curves had nonlinear shapes. These shapes are consistent with several adolescent problem behaviors, such as tobacco and alcohol use, that show a marked increase in prevalence in early adolescence (middle or junior high school), followed by a change in growth rates in high school (Perry et al. 2002). Based on the shapes of the curves, then, and smaller BIC statistics (data not shown), a cubic model (rather than a linear or quadratic model) was used in the analyses. A cubic model represents a growth curve with two “bends” in the line, or two changes in direction. Therefore, in regards to the fixed effects in these models, the estimate associated with the linear term (i.e., time, or “linear time” as in Table 2) represents the rate of growth immediately following the centering point (at the beginning of 6th grade); while the quadratic term (i.e., time2 or “quadratic time” as in Table 2) represents the first “bend,” or curve, in the line, which signifies acceleration (a positive coefficient) or deceleration (a negative coefficient) in growth. Inclusion of a cubic term (i.e., time3 or “cubic time” as in Table 2) generates a second stationary point of change in the curve, representing a shift, or change, in the acceleration or deceleration of the line (Singer and Willett 2003). For the high school phase, where there were three waves of data (10–12th grades), a linear time model was appropriate for the analyses.
Three potential sources of variability were considered for inclusion as random effects matched with all of the fixed effects in the models: (1) variation within a student over time (“level 1” variability), (2) variation between students within a school district (“level 2” variability), and (3) variation between school districts (“level 3” variability). Thus 3-level growth models were used in these analyses to appropriately account for these fixed effects. To test whether growth curves significantly differed between the intervention and the delayed-program control groups, interactions between these three fixed effects and intervention condition (i.e., time*group, time2*group, and time3*group) were entered in the models. Analyses were conducted separately for baseline alcohol users and non-users to examine whether there were differential intervention effects for these two groups. All analyses used MULTILEV in LISREL 8.72 (Joreskog and Sorbom 2005).
Results
Early Adolescent and Follow-up Phase (1991–1996)
Table 1 presents means of raw scores of the four MMPI-A scales for the intervention and control conditions separately for the total sample (N = 1,857) and the two sub-samples of baseline nonusers (n = 1161, 63%) and baseline users (n = 683, 37%). Overall, the mean scores for each increase as the cohort ages from fall, 6th grade through spring, 10th grade although the PRO, A-fam, and A-sch scales appear to peak in 9th grade, particularly for the students in the intervention condition. Results of the growth curve analyses on each of the four subscales, including the intercept and effect sizes, are presented in Table 2. For the total sample, there were significant growth curve differences (i.e., significant cubic X group effects, quadratic X group effects, and/or linear time X group effects) between the intervention and delayed-program control groups for the A-fam and PRO scales. There were no significant differences between groups in the growth curves on the A-sch and ACK scales. For the two scales where significant differences were found, evaluation of the coefficient estimates indicated that the intervention group had a lower initial rate of change, or linear growth (indicating lower risk), had a higher rate of acceleration (higher risk), and then a steeper rate of deceleration (lower risk) compared to the delayed-program control group (Raudenbush and Bryk 2002; Singer and Willett 2003). Examination of the predicted mean trajectories (see Fig. 1) showed that, for the most part, for all scales, the intervention group growth curves remained below or lower than the delayed-program group through 8th grade (1994), so that the initial significant change (linear time X group effects) appears to have essentially delayed the onset of acceleration of family problems and drug use proneness among intervention group students.

Growth curves for selected mmpi-a scales from project northland by intervention condition
As in the earlier studies (Perry et al. 1996; Williams et al. 1999) program effects were significant among the sub-sample of 6th grade students who reported being baseline non-users. There were significant cubic X group, quadratic X group, and linear time X group effects on the A-fam and PRO scales (data available on request from first author). These were all in the same direction as discussed for all students (above). Additionally, significant linear time X group effects were detected on A-sch and ACK, indicating lower risk for the intervention group. Thus, similar patterns of growth curves were found for the non-users as for the total sample, with the addition of the significant linear X time interaction for the ACK and A-sch scales among the baseline non-users, suggesting that for baseline non-users the intervention had an impact on delaying the development of school problems and more serious alcohol or other drug abuse. There were no significant growth curve differences between the two conditions on any of the four MMPI-A scales for the smaller sub-sample of students who were baseline users, those who had already reported some lifetime alcohol use at the beginning of 6th grade.
The High School Phase (1996–1998)
Table 3 presents means of the raw scores of the four MMPI-A scales for the two intervention conditions separately for the High School phase sample (N = 1,701) during the 11th and 12th grades (10th grade was presented in Table 1). For the High School phase, there were no significant slope differences between the intervention and delayed-program control groups on any of the four MMPI-A scales for the growth curve analyses (examining students from 10th through 11th or 12th grades). Examination of the estimates and predicted slopes indicated that the two groups had similar scores and remained stable over time on the PRO and A-sch scales. Significant linear time effects on the A-fam (estimate = −0.72, P < .001) and A-sch scales (estimate = −0.15, P < .05) indicate that students in both conditions showed slight decreases in A-fam and A-sch scores over time.
During the High School phase, there was one significant time X intervention effect for baseline alcohol users. There was a significant linear time X group effect for the A-sch (estimate = 0.36; P < 0.04). A significant linear time effect was found on the A-fam scale (estimate = −0.62, P < .001) for the baseline non-users and on A-fam (estimate = −0.80, P < .001) and A-sch scales (estimate = −0.27; P < .03) for the baseline users. This indicated that overall for the baseline non-users, there was a slight decrease in the A-fam score over time, whereas for the alcohol users there was an overall slight decrease on the A-fam and A-sch scores over time. Thus the high school students generally reduced their risk for family and school problems. The reduction in school problems was less among high school intervention students than delayed-program control students.
Discussion
Project Northland is an alcohol use prevention program aimed at adolescents in 6th through 12th grades. The project was successful in changing the prevalence and trajectories of alcohol use among those involved in the intervention, so that the increase in alcohol use among students in the intervention districts was less than those of students in the delayed-program control districts (Perry et al. 1996; Perry et al. 2002). The current study adds another important dimension to the potential of successful primary prevention programs such as Project Northland. Students in the intervention school districts had lower initial increases on important and relevant measures of family problems and drug use proneness as measured by the significant linear X group interactions of the trajectories of A-fam and PRO during the early adolescent phase of the study. The significant quadratic X group and cubic X group interactions also suggest that the curvature of the trajectories differed between groups, as can be seen in Fig. 1, with greater acceleration and deceleration among students in the intervention condition. Thus, after the initial relative decrease in these scales, the intervention group appeared to begin to catch up with the delayed-program control group. However, the intervention group was also significantly more likely to decelerate about 9th grade, so that the early delay resulted in a shorter acceleration period. Importantly, the data suggest that the Project Northland intervention positively impacted students’ family problems and drug use proneness throughout early adolescence. In particular, not only are family problems a potent risk factor for the development of alcohol use and other problem behaviors, family problems appear to be able to be reduced by an intervention aimed at alcohol use prevention among young adolescents. Given the changes in behaviors as measured by the MMPI-A A-fam and PRO scales, Project Northland may have delayed or decreased the probability of more serious substance abuse disorders developing.
It is of interest to note that the intervention had an impact on the MMPI-A scales, but that this impact was most robust among baseline non-users of alcohol, in the early adolescent (rather than high school) phase. These results somewhat mirror the outcomes for alcohol use, where reductions in alcohol use were not found in separate analyses with baseline alcohol users in either phase of Project Northland (Perry et al. 1996). In the high school phase of Project Northland, modest reductions in the trajectories of alcohol use were found (Perry et al. 2000), but these were not as powerful as in the early adolescent phase. Thus the lack of outcomes for the high school phase in this study is disappointing but consistent with the alcohol use outcomes (Perry et al. 2002). These findings underscore the need for prevention programs aimed at students in high school where few successful interventions have taken place. The findings also suggest that the intervention should be more potent than the high school phase of Project Northland, perhaps spanning 3–4 years, and with substantial parent involvement. A special focus on early users of alcohol may be needed so that problems in school are not exacerbated by the intervention. It appears, then, that Project Northland had an important initial impact on multiple areas of young adolescents’ lives, particularly family problems and drug use proneness, and that this initial impact shortened the early adolescent period of acceleration, and that deceleration was also then greater among the intervention students. This is particularly notable since family problems are a key predictive factor for alcohol use throughout adolescence.
Project Northland appears, then, to have been a particularly powerful intervention for young adolescents, their proneness to use alcohol and drugs, and their families. The family intervention in the early adolescent phase consisted of peer-led, home-based activities that were required as homework (Williams et al. 1995a; Williams et al. 1999); students were rewarded for completion of activities. The family intervention also included family nights in the 6th and 7th grades, and mailed material to parents (Perry et al. 1996). Parents were encouraged and recruited to join the community task forces in their communities. Overall, the parent programs, especially in the 6th grade, had very high participation rates (Williams 1995a), with nearly 90% of parents participating in the home-based activity program, the Slick Tracy Home Team, during the 6th grade. Importantly, parent-child communication was a significant mediator of the Project Northland outcomes in early adolescence (Komro et al. 2001), although, among the MMPI-A scales, only the PRO scale was a significant mediator (not the A-fam) in the main outcome analyses. Students who participated in the family intervention programs also had lower increases in alcohol use than those who did not participate in these programs (Stigler et al. 2006). Thus, it appears that the Project Northland family intervention programs may not only have been important for the outcomes of the main study, alcohol use, but also may have had a direct impact on family problems experienced by young adolescents.
The results reported in the current study suggest that rather than family factors simply functioning as risk or protective factors for adolescent alcohol use, the influence is bidirectional: adolescents whose risk of drinking was lowered by their participation in a prevention program also report fewer family problems, and less probability of developing an alcohol and drug abuse disorder than control group adolescents. This is consistent with the findings of developmental scientists studying the bidirectional influences among parents and children that explain the development of psychopathology (Cicchetti and Cohen 1995; Sroufe and Rutter 1984). The mechanisms through which participation in Project Northland resulted in reports of fewer family problems cannot be disentangled fully, but it seems plausible that these might include protective mechanisms such as: increased parental awareness of teen alcohol use, increased parental ability to monitor teen activities and set appropriate consequences for teen alcohol use, and increased supervision of teen activities either in school or through sponsored activities in the community. Furthermore, the increased skills learned in the home-based activities that facilitated effective communication about alcohol use might have encouraged the use of better parenting strategies for other potential areas of problem development during adolescence.
The generalizability of the findings from this study is limited because Project Northland involved primarily White adolescents in rural and small towns in northeastern Minnesota. However, one important aspect of the findings of this study is that prevention programs in early adolescence can have a broad impact on adolescents’ lives. This may be particularly appealing to parents and to school districts as they consider whether and why to adopt an evidence-based substance use prevention program. If our prevention programs have an impact on family problems or behaviors related to drug proneness, for example, in a cohort of young adolescent students, then this should be particularly relevant for school administrators, teachers and staff. Likewise, parental support may be able to be garnered for the enactment of a prevention program, when allocation of resources is being examined. Thus, the use of measures, like the four MMPI-A scales used in this study, that more broadly assess the impact of prevention programs in key arenas of young people’s lives may not only broaden our understanding of the impact of these programs, but also their potential for dissemination.
References
Botvin, G. J., Baker, E., Dusenbury, L., Botvin, E. M., & Diaz, T. (1995). Long-term follow-up results of a randomized drug abuse prevention trial in a white middle-class population. Journal of the American Medical Association, 273(14), 1106–1112.
Bray, J. H., Adams, G. J., Getz, J. G., & Stovall, T. (2001). Interactive effects of individuation, family factors, and stress on adolescent alcohol use. American Journal of Orthopsychiatry, 71(4), 436–449.
Butcher, J. N., & Williams, C. L. (1992). Essentials of MMPI-2 and MMPI-A interpretation. Minneapolis, MN: University of Minnesota Press.
Cicchetti, D., & Cohen, D. (1995). Developmental psychopathology. New York: Wiley.
Colder, D. R., & Chassin, L. (1999). The psychosocial characteristics of alcohol users versus problem users: Data from a study of adolescents at risk. Development and Psychopathology, 11, 311–348.
Donovan, J. E., Leech, S. L., Zucker, R. A., Loveland-Cherry, C. J., Hester, J. M., Fitzgerald, H. E., et al. (2004). Really underage drinkers: Alcohol use among elementary students. Alcoholism. Clinical and Experimental Research, 28(7), 341–349.
Ellickson, P. L., McCaffrey, D. F., Ghosh-Dastidar, B., & Longshore, D. L. (2003). New inroads in preventing adolescent drug use: results from a large-scale trial of project ALERT in middle schools. American Journal of Public Health, 93(11), 1830–1836.
Ellickson, P. L., Tucker, J. S., & Klein, D. J. (2003). Ten-year prospective study of public health problems associated with early drinking. Pediatrics, 111(5), 949–955.
Flewelling, R. L., Austin, D., Hale, K., LaPlante, M., Liebig, M., Piaseki, L., et al. (2005). Implementing research-based substance abuse prevention in communities: Effects of a coalition-based prevention initiative in Vermont. Journal of Community Psychology, 33(3), 333–353.
Forbey, J. D., & Ben-Porath, Y. S. (2003). Incremental validity of the MMPI-A content scales in a residential treatment facility. Assessment, 10(2), 191–202.
Grant, B. F., & Dawson, D. A. (1997). Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. Journal of Substance Abuse, 9, 103–110.
Greenblatt, J. C. (2000). Patterns of alcohol use among adolescents and associations with emotional and behavioral problems. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration.
Gruber, E., DiClemente, R. J., Anderson, M. M., & Lodico, M. (1996). Early drinking onset and its association with alcohol use and problem behavior in late adolescence. Preventive Medicine, 25(3), 293–300.
Guo, J., Collins, L. M., Hill, K. G., & Hawkins, J. D. (2000). Developmental pathways to alcohol abuse and dependence in young adulthood. Journal of Studies on Alcohol, 61(6), 799–808.
Guo, J., Hawkins, J. D., Hill, K. G., & Abbott, R. D. (2001). Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. Journal of Studies on Alcohol, 62(6), 754–762.
Henggeler, S. W., Clingempeel, W. G., Brondino, M. J., & Pickrel, S. G. (2002). Four-year follow-up of multisystemic therapy with substance-abusing and substance-dependent juvenile offenders. Journal of the American Academy of Child Adolescent Psychiatry, 41(7), 868–874.
Hingson, R., Heeren, T., Levenson, S., Jamanka, A., & Voas, R. (2002). Age of drinking onset, driving after drinking, and involvement in alcohol related motor-vehicle crashes. Accident; Analysis & Prevention, 34(1), 85–92.
Hingson, R., Heeren, T., Winter, M. R., & Wechsler, H. (2003). Early age of first drunkenness as a factor in college students’ unplanned and unprotected sex attributable to drinking. Pediatrics, 111(1), 34–41.
Hipwell, A. E., White, H. R., Loeber, R., Southamer-Loeber, M., Chung, T., & Sembower, M. A. (2005). Young girls’ expectancies about the effects of alcohol, future intentions and patterns of use. Journal of Studies on Alcohol, 66(5), 630–639.
Iannotti, R. J., Bush, P. J., & Weinfurt, K. P. (1996). Perception of friends’ use of alcohol, cigarettes, and marijuana among urban schoolchildren: a longitudinal analysis. Addictive Behaviors, 21(5), 615–632.
Institute of Medicine (2004). Reducing underage drinking: A collective responsibility. Washington, DC: Institute of Medicine, National Research Council. The National Academies Press.
Jackson, C., Henriksen, L., & Dickinson, D. (1999). Alcohol-specific socialization, parenting behaviors and alcohol use by children. Journal of Studies on Alcohol, 60(3), 362–367.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2005). Monitoring the Future national survey results on drug use, 1975–2004. Vol 1: Secondary school students. Bethesda, MD: National Institute on Drug Abuse.
Joreskog, K., & Sorbom, D. (2005). LISREL 8.72. Lincolnwood, IL: Scientific Software International, Inc.
Kaplow, J. B., Curran, P. J., & Dodge, K. A. (2002). Child, parent, and peer predictors of early-onset substance use: A multisite longitudinal study. Journal of Abnormal Child Psychology, 30(3), 199–216.
Komro, K. A., Perry, C. L., Veblen-Mortenson, S., Williams, C. L., & Roel, J. P. (1999). Peer leadership in school and community alcohol use prevention activities. Journal of Health Education, 30(4), 202–208.
Komro, K. A., Perry, C. L., Williams, C. L., Stigler, M. H., Farbakhsh, K., & Veblen-Mortenson, S. (2001). How did Project Northland reduce alcohol use among young adolescents? Analysis of mediating variables. Health Education Research, 16(1), 59–70.
Kosterman, R., Hawkins, J. D., Guo, J., Catalano, R. F., & Abbott, R. D. (2000). The dynamics of alcohol and marijuana initiation: patterns and predictors of first use in adolescence. American Journal of Public Health, 90(3), 360–366.
Li, X., Stanton, B., & Feigelman, S. (2000). Impact of perceived parental monitoring on adolescent risk behavior over 4 years. Journal of Adolescent Health, 27(1), 49–56.
Liddle, H. A., Dakof, G. A., Parker, K., Diamond, G. S., Barrett, K., & Tejeda, M. (2001). Multidimensional family therapy for adolescent drug abuse: results of a randomized clinical trial. American Journal of Drug & Alcohol Abuse, 27(4), 651–688.
Marshal, M. P., & Chassin, L. (2000). Peer influence on adolescent alcohol use: The moderating role of parental support and discipline. Applied Developmental Science, 4(2), 8–88.
Micucci, J. A. (2002). Accuracy of MMPI-A scales ACK, MAC-R, and PRO in detecting comorbid substance abuse among psychiatric inpatients. Assessment, 9(2), 111–122.
Murray, R. P., Connett, J. E., Tyas, S. L., Bond, R., Ekuma, O., Silversides, C. K., et al. (2002). Alcohol volume, drinking pattern, and cardiovascular disease morbidity and mortality: is there a U-shaped function?. American Journal of Epidemiol, 155(3), 242–248.
Perry, C. L., Williams, C. L., Forster, J. L., Wolfson, M., Wagenaar, A. C., Finnegan, J. R., et al. (1993). Background, conceptualization and design of a community-wide research program on adolescent alcohol use: Project Northland. Health Education Research, 8(1), 125–136.
Perry, C. L., Williams, C. L., Komro, K. A., Veblen-Mortenson, S., Forster, J. L., Bernstein-Lachter, R., et al. (2000). Project Northland high school interventions: Community action to reduce adolescent alcohol use. Health Education & Behavior, 27(1), 29–49.
Perry, C. L., Williams, C. L., Komro, K. A., Veblen-Mortenson, S., Stigler, M. H., Munson, K. A., et al. (2002). Project Northland: long-term outcomes of community action to reduce adolescent alcohol use. Health Education Research, 17(1), 117–132.
Perry, C. L., Williams, C. L., Veblen-Mortenson, S., Toomey, T. L., Komro, K. A., Anstine, P. S., et al. (1996). Project Northland: outcomes of a communitywide alcohol use prevention program during early adolescence. American Journal of Public Health, 86(7), 956–965.
Raudenbush, S. W., & Bryk, A. S. (2002). Hierarchical linear models: Applications and data analysis methods. (2nd ed.). Thousand Oaks: Sage Publications.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., et al. (1997). Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. Journal of American Medical Association, 278(10), 823–832.
Rinaldo, J. C., & Baer, R. A. (2003). Incremental validity of the MMPI-A content scales in the prediction of self-reported symptoms. Journal of Personality Assessment, 80(3), 309–318.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis: Modeling change and event occurrence. New York: Oxford University Press.
Spoth, R., Redmond, C., & Lepper, H. (1999) Alcohol initiation outcomes of a universal family-focused preventive interventions: one- and two-year follow-ups of a controlled study. Journal of Studies on Alcohol Supplement, 13, 103–111.
Sroufe, L. A., & Rutter, M. (1984). The domain of developmental psychopathology. Child Development, 55(1), 17–29.
Stein, L. A., & Graham, J. R. (2001). Use of the MMPI-A to detect substance abuse in a juvenile correctional setting. Journal of Personality Assessment, 77(3), 508–523.
Stein, L. A. R., & Graham, J.R. (2005). Ability of substance abusers to escape detection on the Minnesota Multiphasic Personality Inventory-Adolescent (MMPI-A) in a juvenile correctional facility. Assessment, 12(1), 28–39.
Stigler, M. H., Perry, C. L., Komro, K. A., Cudeck, R., & Williams, C. L. (2006). Teasing apart a multiple component approach to adolescent alcohol prevention: What worked in Project Northland?. Prevention Science, 7, 269–280.
Substance Abuse and Mental Health Services Administration. (2004). Alcohol dependence or abuse and age at first use. The NSDUH report. Retrieved March 22, 2007, from http://oas.samhsa.gov/2k4/ageDependence/ageDependence.cfm.
Weed, N. C., Butcher, J. N., & Williams, C. L. (1994). Development of MMPI-A alcohol/drug problem scales. Journal of Studies on Alcohol, 55(3), 296–302.
Williams, C. A., Butcher, J. N., Ben-Porath, Y. S., & Graham, J. R. (1992). MMPI-A content scales: Assessing psychopathology in adolescents. Minneapolis, Minnesota: University of Minnesota Press.
Williams, C. L., Perry, C. L., Dudovitz, B., Veblen-Mortenson, S., Anstine, P. S., Komro, K. A., et al. (1995a). A home-based prevention program for sixth grade alcohol use: Results from Project Northland. Journal of Primary Prevention, 16(2), 125–147.
Williams, C. L., Perry, C. L., Farbakhsh, K., & Veblen-Mortenson, S. (1999). Project Northland: comprehensive alcohol use prevention for young adolescents, their parents, schools, peers and communities. Journal of Studies on Alcohol Supplement, 13, 112–124.
Williams, C. L., Toomey, T. L., McGovern, P., Wagenaar, A. C., & Perry, C. L. (1995b). Development, reliability, and validity of self-report alcohol-use measures with young adolescents. The Journal of Child and Adolescent Substance Abuse, 4(3), 17–40.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Perry, C.L., Lee, S., Stigler, M.H. et al. The Impact of Project Northland on Selected MMPI-A Problem Behavior Scales. J Primary Prevent 28, 449–465 (2007). https://doi.org/10.1007/s10935-007-0105-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10935-007-0105-9