
Abstract
Objectives Knowledge regarding the working mechanism of an intervention is essential for obtaining a better understanding of the intervention and contributes to optimize its outcome. This study aimed at investigating whether changes in cognitive-behavioral factors and muscle activation patterns after myofeedback training and ergonomic counseling were associated with outcome, in subjects with work-related musculoskeletal neck-shoulder complaints. Methods Seventy-nine symptomatic subjects received either myofeedback with ergonomic counseling (Mfb/EC) or ergonomic counseling alone (EC). Outcome measures discomfort and disability, and process factors catastrophizing, pain control, fear-avoidance beliefs, and muscle activation patterns were assessed at baseline, after the interventions (T0), and at 3 months follow-up (T3). Mixed modeling techniques were used for analysis. Results Outcome in terms of discomfort and disability was generally comparable between both interventions. Catastrophizing was significantly reduced and fear-avoidance beliefs about work slightly increased after the interventions, but no consistent changes in muscle activation patterns were observed. Changes in discomfort were especially associated with changes in catastrophizing at T0 and T3, but R2 was low (<0.14). Reduced catastrophizing at T0 and T3, and also reduced fear-avoidance beliefs about work at T3, were related to reduced disability (R2 between 0.30 and 0.40). No differences between the two intervention groups were observed. Conclusions Intervention effects were generally non-specific and findings suggested that cognitive-behavioral factors underlie the outcome of these interventions rather than changes in muscle activation patterns. Emphasizing these factors during therapy may increase the beneficial outcome of occupational interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Musculoskeletal neck-shoulder complaints related to work are multifactorial in nature involving both physiological factors, psychosocial factors, and cognitions [31]. A variety of interventions addressing these complaints have been applied, most often focusing on the adjustment of the physical work environment and/or education about working posture according to ergonomic principles [21, 28]. In spite of such attention to ergonomics, the prevalence of work-related musculoskeletal complaints is still high [5, 10, 61]. Interventions to reduce these complaints might benefit from expanding their current focus from a purely ergonomic approach to including also knowledge on the underlying physiological abnormalities in work-related neck-shoulder complaints. A number of studies indicate that lack of muscle relaxation is related to work-related musculoskeletal complaints [15, 40] according to the Cinderella hypothesis [23]. This hypothesis comprises the idea of a fixed order of motor unit recruitment in muscle activation and subsequent sustained activation of the low threshold motor units that are activated first. This fixed order is assumed to contribute to insufficient relaxation and recovery of the motor units that are activated first, which at long term can result in discomfort. Based on these findings Hermens and Hutten developed an ambulant myofeedback device [18], which provides feedback by means of vibration and a soft sound when the trapezius muscle relaxation is insufficient. Two aspects distinguish this approach from traditional biofeedback: (1) It is provided when muscle relaxation is insufficient rather than when muscle activation exceeds a certain threshold, and (2) being ambulant, it enables continuous monitoring, e.g. at the workplace, over days and weeks instead of weekly sessions of up to 60 min at the clinic.
Two feasibility studies have shown beneficial effects in about half of the subjects with neck-shoulder complaints taking part in an intervention based on this myofeedback approach. The first focused on neck-shoulder pain related to work [18], the second on Whiplash Associated Disorder grade II [56]. A randomised controlled trial (RCT) was subsequently set up in order to compare the myofeedback intervention as defined in these feasibility studies (i.e. 4 weeks of myofeedback training and coaching by a therapist), to a control group: Ergonomic counselling (EC) was compared to ergonomic counselling in combination with the myofeedback intervention (Mfb/EC). This way, the ergonomic counselling not only assured the ergonomic standard of the participants’ workplaces in both intervention groups, but also provided therapist attention to both intervention groups on a comparable level.
The main results of the RCT study have been presented in Voerman et al. [54]. In short, it was found that both intervention groups significantly improved from baseline to follow-ups in terms of discomfort and disability. There was no specific effect for type of intervention although a slightly higher percentage of subjects in the Mfb/EC group showed clinically relevant improvements compared to the EC group.
Besides investigating the overall result of an intervention in terms of pre- and post-intervention measures it is also of great value to describe outcome by its underlying working mechanism, as it increases our understanding and facilitates improvement of the intervention. Knowledge of working mechanisms is however scarce, especially for effects of occupational interventions [26]. For the ambulant myofeedback training, it can be hypothesized that changes in muscle relaxation underlie changes in outcome measures discomfort and disability. Vollenbroek-Hutten and colleagues [57] found first empirical support for this hypothesis by showing significant associations between increased muscle relaxation and decreased discomfort levels after four weeks of ambulant myofeedback training. The maximum percentage explained variance in discomfort was however 36%, leaving a considerable part of variance unexplained. This remaining variance might be attributed to cognitive changes induced by the myofeedback training [20] especially with regard to perceived control [8, 38]. Sarnoch et al. [41] for instance found an association between an increased sense of control and a reduction in pain intensity after traditional myofeedback training in patients with fibromyalgia and suggested that cognitive-behavioural factors are probably more relevant for outcome after the myofeedback training compared to physiological factors. The nature of the myofeedback intervention, providing the subject insight into normally invisible physiological responses and the sense of internal control over these responses, might thus positively affect maladaptive cognitions. More generic, when looking at working mechanisms of intervention programs for chronic pain, whether or not including myofeedback, changes in coping strategies like catastrophizing and fear-avoidance beliefs appear related to outcome (also called process factors) [e.g. 6, 7, 25, 32, 44, 58]. There is a need of empirical studies investigating whether these factors are also involved in outcome after occupational interventions, like Mfb/EC and EC, as such knowledge contributes to our understanding of exactly how these interventions work.
This study further explores the findings reported in Voerman et al. [54], and aims at investigating:
-
1.
whether cognitive-behavioural factors and muscle activation patterns (entitled process factors) change; and
-
2.
whether these factors are related to outcome (discomfort and disability) both immediately after Mfb/EC and EC as well as at follow up
in subjects with work-related neck-shoulder complaints. For both EC and Mfb/EC it was hypothesised that providing the subject information about the benign character of their pain and a tool to deal with this pain, catastrophizing and fears would be reduced, and this would contribute to reduced discomfort and disability levels. It was anticipated that especially Mfb/EC induces an increased sense of control over pain and enhances muscle rest in subjects with work-related neck-shoulder complaints because of the nature of the myofeedback intervention and that changes in these factors are related to reduced discomfort and disability.
Methods and Materials
Design and Subjects
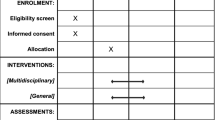
This study further explores the results of the randomized controlled trial evaluating the effects of 4 weeks ambulant myofeedback training combined with ergonomic counselling (Mfb/EC) and ergonomic counselling alone (EC). Participants were randomly assigned to either the Mfb/EC or the EC group (considered the control intervention group), based on a randomisation schedule that was adopted from Pocock [36]. A block randomisation procedure was used: Each new group of subjects starting with the study was considered a block, and half of the subjects in each block were assigned to the Mfb/EC group. Measurements were performed at baseline (B) prior to the intervention but before randomization, immediately after four weeks of intervention (T0), and at the three (T3) months follow-up.
Participants were elderly (predominantly over the age of 45) female computer workers who were recruited in Sweden (area of Göteborg) and the Netherlands (area of Enschede) between April 2003 and June 2005. Only females were included because of the high prevalence of complaints in this group [2, 29, 35]. They were approached at their work place, by telephone, and announcements, and ultimately selected based on the findings in a screening questionnaire [39]. This questionnaire contains general questions as well as detailed questions related to the musculoskeletal status and (work) factors that are believed to affect musculoskeletal health. In addition, subjects were asked about their expectancies with regard to the benefits of participation in this study for their musculoskeletal complaints, and at T0 subjects were asked whether their expectancies had been fulfilled. Subjects eligible for participation were working for at least 20 h a week and reported persistent musculoskeletal complaints in the neck and/or shoulder region for at least 30 days during the last year.
The study was approved by the medical ethics committee and all participants gave their informed consent prior to participation.
Interventions
The interventions were provided by three different therapists who were trained together to ensure that they would provide as identical interventions as possible. The character of the intervention made blinding of the therapists and participants to the interventions impossible. For full specifications of the interventions and procedures the reader is referred to Voerman et al. [54].
Ergonomic Counselling (EC)
Subjects received 4 weeks of intervention during which they kept a diary of activities and discomfort scores. During this period they were visited weekly by their therapist. The first visit comprised an ergonomic workplace investigation by means of the risk inventory ‘RSI in computer related work: Prevention and integration’ of Huppes et al. [22]. Based on the results of the checklist, possible improvements were discussed with the subject. The remaining visits were used to further discuss ergonomics according to a manual which was specifically developed for this study and contains standard instructions for beginning and ending of the visits, structured questions regarding the ergonomic changes that were performed during or after previous visits, the consequences of these changes in terms of discomfort, individual goals, and appointments for the next week.
Myofeedback Training (Mfb/EC)
Subjects assigned to the Mfb/EC group received myofeedback training on top of EC. A two-channel ambulant feedback system combined with a garment incorporating dry sEMG (surface ElectroMyoGraphy) electrodes to enable recording of upper trapezius muscle activity was used [18]. The harness was connected with a sEMG processing and storage system. The sEMG signal was amplified (15×), band pass filtered between 30 and 250 Hz, sampled at 512 Hz, digitized (22 bits ADC), and smooth rectified with removal of the low frequency components. Embedded software provided the detection and calculation of muscle rest, expressed as the sEMG parameter Relative Rest Time (RRT). RRT was defined as the percentage of time of complete muscle rest (Root Mean Square (RMS) < 10 μV for at least 0.12 s) during a 10 s interval. The parameters RRT and RMS were stored on the device. Sensory feedback by means of vibration and a soft sound was provided after each 10 s interval when the relative duration of muscle relaxation in that particular interval was below 20% (i.e. when RMS was below 10 μV during less than 2 s for that interval) [15, 53].
Immediately after baseline subjects assigned to the Mfb/EC group received the myofeedback system, they were explained the principles of feedback. Subjects were instructed that relaxation could be reached by slightly depressing the shoulders, or by sitting down quietly with the eyes closed, the hands in the lap while breathing deeply. Another relaxation strategy was to maximally elevate the shoulders for 3 s to build up muscle tension and then to let loose this tension.
Subjects used the system for 4 weeks, for at least 8 hours a week (distributed over 2 h a day and 2 days a week as a minimum) during occupational activities. During the weekly visits, the sEMG data from the previous week were scrutinized and discussed, and it was verified whether subjects complied with the eight hours requirement as mentioned above. This procedure was facilitated by means of the diary.
Measurements
Measurements were performed at B, T0, and T3, and comprised outcome, i.e. discomfort and disability, and process factors, i.e. coping strategies, fear-avoidance beliefs, and muscle activation patterns.
Outcome Measures
The effect of the interventions on work-related neck-shoulder complaints was assessed with outcome measures discomfort and disability.
Discomfort in the neck, shoulders, and upper back was assessed by means of Visual Analogue Scales (VAS) [14], a 10 cm horizontal line with ‘no discomfort at all’ at the left and ‘as much discomfort as possible’ at the right extremity of the line. Subjects were asked to rate their subjectively experienced level of discomfort at that particular moment. Psychometric properties of the VAS have proven to be sufficient [50].
The level of experienced disability was assessed with the Pain Disability Index (PDI), a self-rating scale that measures the impact of pain on the abilities to participate in life activities [37]. The PDI contains seven items, one for each domain, i.e. (1) family and home responsibilities, (2) recreation, (3) social activity, (4) occupation, (5) sexual behaviour, (6) self care, and (7) life-support activity. Answers are provided on a categorical 11-points scale with ‘not disabled’ and ‘fully disabled’ at the extremes. Psychometric properties of the PDI are sufficient [48]. In the current study, Cronbachs’ alpha was .89.
Process Factors
Cognitive-behavioural factors included in this study were catastrophizing, control, and fear-avoidance beliefs, selected based on literature. The first factor was assessed using the subscale of the Swedish [24] and Dutch [46] versions of the Coping Strategies Questionnaire (CSQ). Observed pain control was assessed with the Dutch version of the CSQ. The Swedish CSQ consists of 7-point numerical rating scales, while for the Dutch version questions are answered by means of a mark at a VAS scale with ‘never’ and ‘always’ as extremes. The CSQ is known to have good psychometric properties [46] and alphas for the subscales catastrophizing and observed control were sufficiently high in the current sample (.75 and .91 respectively).
Fear-avoidance beliefs were assessed using the Swedish and Dutch language versions of the Fear-Avoidance Beliefs Questionnaire (FABQ) [51, 59], a 16-item 7-point measure that aims at identifying beliefs concerning the influence of work (subscale W) and physical activity (subscale PA) on bodily damage and on whether activities should be avoided. High scores represent high fear-avoidance beliefs. The FABQ has proven to be psychometrically sound [47] with alpha .82 for FABQ_W and .83 for FABQ_PA for the current sample.
Muscle activation patterns of both upper trapezius muscles were assessed using surface Electromyography (sEMG). Electrodes were placed according to the international guidelines of SENIAM [17]. The electrodes were connected to the EMG unit by means of cables that were attached to the skin with tape to minimise noise. The sEMG signal was sampled (1,024 Hz), band pass filtered (20–500 Hz), and stored on a computer for off line analysis.
Four reference contractions of the upper trapezius muscles were performed according to the guidelines of Mathiassen et al. [30]. Subjects were sitting and held the arms straight and horizontal in 90° abduction with no additional weight, with the hands relaxed and the palms pointing downwards. Each measurement lasted for 15 s with 30 s rest in between. Subsequently subjects performed three computer-related tasks in random order: A bilateral typing task and two unilateral mouse tasks, i.e. a stress task and a precision task. For these tasks, the table and chair of the computer work station were adjusted to the anthropometric properties of the subject. Each task was preceded and followed by a few minutes rest for recovery. During the typing task, subjects were instructed to copy a text that was situated in a document holder at the left side of the subject, adjustable in height and distance. The stress task was a modified Stroop task that required subjects to use the mouse to click at the name of the colour of the print of each colour-word. The appearance of this word varied in time and appeared at random location at the screen. An incorrect or late answer was followed by a beep [27] which was assumed to increase the stress level [4]. For the precision task [3], subjects were shown a graph of 7 circular targets of 7 mm diameter connected by means of lines on the right half of the computer screen. Subjects were instructed to duplicate this graph on the left half of their screen on which the circular targets were shown. Lines could be drawn by means of clicking on the targets in the correct order. As soon as a drawing was completed another drawing popped up.
These tasks were chosen as they were assumed to give a valid representation of activities performed at the (computer) workplace, encompassing both unilateral as well as bilateral movements in a static posture, including also the stress component which is often associated with neck-shoulder complaints.
Analysis
Data from the questionnaires and the sEMG recordings performed in the laboratory were used to investigate whether cognitive-behavioural factors and muscle activation patterns changed during the interventions and whether these changes were related to outcome after the interventions in terms of discomfort and disability.
Data Reduction
VAS scores for the neck, shoulders, and upper back were summed and averaged resulting in one total VAS score for the neck-shoulder region. PDI and FABQ (subscale) scores were calculated for each subject for each measurement. CSQ scoring methodology varied between the Swedish and the Dutch questionnaire. Therefore, relative scores were calculated by expressing the score of the subscale as a percentage of the maximum subscale score.
Two sEMG parameters were calculated: Root Mean Square (RMS) and Relative Rest Time (RRT). RRT was defined as the percentage of time in which RMS was below threshold (6 μV) [19] for at least 0.125 s. RMS and RRT values during the computer tasks were calculated for 4 epochs about 60 s duration each. The values were subsequently averaged per task for each subject. For the reference contraction, RMS values were calculated for the middle 10 s of each contraction [30], resulting in four RMS values that were averaged and used for normalisation. This means that RMS values during the typing, stress, and precision tasks were expressed as percentages of this mean reference value.
Statistical Analysis
Factors that were not normally distributed were log transformed to obtain a distribution close to normal. Statistical analysis consisted of two parts. First, it was investigated whether outcome and process factors changed after the intervention. For the normally distributed factors Mixed Linear Modelling was used to identify significant changes over time. Time (B, T0, and T3), intervention type (i.e. Mfb/EC and EC), and study group (Sweden and the Netherlands) were considered fixed factors, as well as the interaction terms intervention × time and intervention × study group. The factor study group comprises variance due to possible sociodemographic differences as well as variance caused by the different therapists, organizations, and job characteristics in the two countries. The factor subject was included in the model as a random factor. When a significant effect was observed for the factor time, post hoc Mixed Models were run to explore whether these changes occurred between B and T0 or between B and T3. For RRT variables, bimodal in origin, log transformation does not result in closer to normal distributions, so for this factor non-parametric methods (Friedman tests) were used to identify changes over time. Wilcoxon Signed Ranks Tests were performed post hoc to identify whether the factors changed between B and T0 or between B and T3.
Secondly, the factors that significantly changed over time were entered in a Mixed Linear Model as fixed factors to study their associations with outcome (discomfort and disability, dependent factors) after the interventions for that specific time interval (i.e. B–T0 or B–T3). Intervention type was additionally entered as a fixed factor, including its interactions with the process factors in order to investigate whether these factors were differently relevant for the Mfb/EC and the EC group. In other words, it was investigated whether the process factors for the outcome were different between the two interventions. Again, the models were corrected for study group and its interactions. Percentages explained variance (first level R2) were calculated for these models by comparing variance in the model including fixed factors and the model without fixed factors, by using the following formula according to Snijders and Bosker [45]:
wherein σ2 corresponds to the within-subject variance (residual) and τ2 is the between-subject variance (intercept), I refers to the summed variance of the model without fixed factors, and II refers to the variance of the model with the fixed factors.
Traditionally, analyses aimed at identifying process factors are performed by calculating delta (Δ) scores of the process variables, for instance between B and T0, and to enter these scores into a regression model with delta scores of outcome as dependent variable. However, there is a major concern using this approach. The Δ scores of both outcome and process factors itself are dependent on the baseline value. Thus, for a proper model baseline values should be corrected for. The problem with this approach is that the model is at risk of containing too many variables (>1 per 10 observations) [34] which makes it instable and invalid. To overcome these problems Mixed Linear Modelling was used to study the association between factors, and Δ scores were only used to provide insight in the direction of the correlations (Spearmans’ rho) between changes in outcome and changes in process factors.
Statistical Package for Social Sciences (SPSS) 11.5 was used for statistical testing and alpha was set at .05 for statistical significance.
Results
Detailed descriptions of the subject population as well as the course of VAS and PDI over time are provided in Voerman et al. [54]. Here, these data are presented in short.
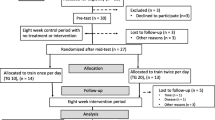
Seventy-nine subjects with work-related neck-shoulder complaints were included in this study, 38 from the Netherlands and 41 from Sweden. Forty-two subjects were assigned to the Mfb/EC group and 37 to the EC group. Between B and T0, 5 subjects in the Mfb/EC and 2 subjects in the EC group dropped out, and between T0 and T3 another 4 subjects in the Mfb/EC and 2 in the EC group ended participation.
Before randomisation was performed, 79% and 73% of the subjects in the Mfb/EC and the EC group respectively, subjectively reported to expect that participation in this study would be beneficial. At T0, 73% of the subjects in the Mbf/EC group reported that participation indeed has been beneficial, while 58% reported this in the EC group. Subject characteristics at baseline are presented in Table 1.
Outcome factors VAS (discomfort) and PDI (disability) significantly changed over time (F = 50.21, P < .01 and F = 35.30, P < .01 respectively), generally without a specific effect for interventions. VAS was significantly reduced between B and T0 (F = 31.06, P < .01) and between B and T3 (F = 41.4, P = <.01), without additional effects for intervention type, study group, or interactions (P > .07). For PDI, besides significant reductions between B and T0 (F = 27.77, P < .01) and between B and T3 (F = 26.41, P < .01), values were additionally significantly higher in the Dutch compared to the Swedish subject sample (F = 5.45, P = .02). Finally, an interaction effect was found for intervention*time between B and T3 (F = 5.54, P = .02), indicating that subjects assigned to the Mfb/EC group showed a continued decrease in disability at T3 compared to B, while subjects in the EC group did not (see also Table 2).
Changes in Process Factors
Median (inter-quartile range) values of the cognitive-behavioural factors observed at B, T0, and T3 in Mfb/EC and EC are presented in Table 2. A main effect was found for the factor time for CSQ subscale catastrophizing (F = 7.07, P = .01), with significant decreases between B and T0 (F = 8.94, P < .01) and between B and T3 (F = 5.18, P = .03). Generally, higher scores were observed in the Dutch compared to the Swedish sample (P ≤ .02), but no other (interaction) effects were found (P > .36).
A significant effect for the factor time was also observed for FABW_W (F = 18.20, P < .01). Fear-avoidance beliefs were slightly, but significantly, increased between B and T0 (F = 6.27, P = .01) and between B and T3 (F = 13.37, P < .01), with an additional interaction effect between B and T0 for intervention × time (F = 5.98, P = .02) which indicates that the increase in FABQ_W was significantly larger in the Mfb/EC compared to the EC group. No other main or interaction effects were found significant for FABQ_W (P > .13). CSQ subscale Observed control and FABQ_PA did not change over time and no other (interaction) effects were found significant (P > .06).
Normalised RMS values during typing, stress, and precision in Mfb/EC and EC are presented in box plots in Fig. 1 and Fig. 2, without extremes. Generally, these figures show no clear pattern of change, although a significant effect was observed for the factor time during the precision task (left side) and the stress task (right side) (F = 4.12, P = .04). Post hoc analysis revealed that small, but significant, increased RMS values were found during the precision task at the left side (F = 5.74, P = .01) at T0 compared to B. RMS values during the stress task were significantly reduced at the right side at T3 compared to B (F = 4.05, P = .05) but no other main effects or interactions were observed (P > .08).

Box plots for normalised RMS values of the right upper trapezius muscle over time during typing, stress, and precision tasks for Mfb/EC and EC group

Box plots for normalised RMS values of the left upper trapezius muscle over time during typing, stress, and precision tasks for Mfb/EC and EC group
Table 2 presents the median value and inter-quartile ranges of RRT values. RRT values did not change after the intervention (T0 and T3) compared to B (0 ≥ Z ≥ −1.71 with P ≥ .09).
Associations between Process and Outcome Factors
Bivariate correlation coefficients between ΔVAS (changes in discomfort) and ΔPDI (changes in disability) and Δ scores of the cognitive-behavioural factors and muscle activation patterns that significantly changed between B and T0 and/or between B and T3, are presented in Table 3. Significant relations were only observed between reductions in catastrophizing and reductions in disability.
Mixed linear modelling indicated that changes in catastrophizing were consistently related to changes in VAS at T0 (F = 10.93, P < .01) and T3 (F = 14.16, P < .01) without other significant main or interaction effects (P > .09). Catastrophizing was also significantly associated with PDI at T0 (F = 34.86, P < .01) and T3 (F = 59.67, P < .01). Furthermore, FABQ_W was positively associated with PDI at T3 (F = 6.46, P = .01) but no other main or interaction effects (P > .09) were observed.
R2 was relatively low for VAS (i.e. 0.09 for B–T0 and 0.14 for B–T3) and considerable for PDI (i.e. 0.30 for B–T0 and 0.40 for B–T3).
Discussion
Knowledge regarding process factors of an intervention is essential for obtaining a better understanding of the underlying working mechanism and provides input for improvement of the intervention itself. The present study aimed at identifying changes in cognitive-behavioural factors and muscle activation patterns after either ambulant myofeedback training combined with ergonomic counselling (Mfb/EC) or ergonomic counselling alone (EC), in subjects with work-related neck-shoulder complaints. Furthermore it was explored whether these changes were related to outcome after the interventions. The results of this study indicate that rather than muscle activation patterns, cognitive-behavioural factors were likely to change and are associated with changes in discomfort and disability.
Cognitive-Behavioural Factors
Catastrophizing appeared to be the main process factor: Baseline catastrophizing levels were low in both intervention groups but despite this, further reduction occurred and these reductions were related to reduced discomfort and disability levels after the interventions. These findings correspond to literature reporting on the relevance of catastrophizing in the development and chronification of pain [16, 42, 52] as well as its relevance for outcome after treatment of (chronic) low back pain patients [44], fibromyalgia patients [32] and chronic pain patients in general [6, 7, 25]. The present findings do not justify statements with regard to causality, but it seems reasonable to hypothesize that the changes in catastrophizing were brought about by the interventions. Burns and colleagues [6, 7] used a cross-lagged correlation approach to explore the effects of multidisciplinary treatment on outcome in chronic pain patients. In addition to pre- and post-treatment observations they added a midterm observation that was applied to study whether early changes in cognitive factors preceded late-term changes in outcome. They showed that an early change in cognitions indeed predicted outcome at the end of the treatment and that catastrophizing is thus likely a mediating factor for outcome. Exactly how reduced catastrophizing contributes to reduced discomfort from a psychophysiological perspective is not clear, but Geisser et al. [12] suggested that catastrophizing is related to decreased pain thresholds in patients with fibromyalgia. Information on the benign nature of complaints and the provision of a possible tool for handling these complaints by providing the patients an intervention, might have contributed to reduced catastrophizing.
Contrary to literature [e.g. 13, 58, 62, 63], fear-avoidance beliefs about work slightly, but significantly, increased rather than decreased after the intervention, with a larger increase in subjects receiving Mfb/EC compared to subjects receiving EC. One possible explanation for the small increase in these beliefs is enclosed in the focus of the intervention. The relation between work and complaints is stipulated during the interventions and this may have sensitized ‘fear’ resulting in increased fear-avoidance beliefs about work. The larger increase in the Mfb/EC group may be attributed to the experience of feedback as stressing the risks of work. In most studies usually the focus of treatment is on other aspects than work, and therefore these studies [13, 58, 63] may report decreased fear-avoidance beliefs. The level of fear-avoidance beliefs about work remained however low (<30, which is the cut-off point for low and high scores [11]) and did not significantly contribute to explaining variance in outcome after the interventions, except for at the 3 months follow-up. It needs to be explored whether this finding is also valid for populations in which fear-avoidance belief values are within the entire range of values, rather than within the small range of low values as reported in this study.
Changing cognitions was not one of the initial targets of the two interventions in this study and this might more likely be expected in multidisciplinary treatments focusing on cognitive-behavioural aspects. It has however more often been reported in literature that treatments which do not deliberately focus on cognitive factors but aim at changing behaviour are responsible for a cognitive change. Generally, it is assumed that cognitions can very well be altered by changing motor behaviour [1]. From this perspective, both the Mfb/EC and the EC interventions may have induced changed motor behaviour at the workplace and this may have reduced the negative perception towards pain (catastrophizing). The actual change in work related risk factors has not objectively been quantified in this study, and this should be considered a limitation because it remains unclear whether the interventions worked as intended like changing work postures for instance. Although exact numbers can not be provided, there is no doubt that workplaces changed: The therapists subjectively noted alterations in the height of the chair and desk, together with the positioning of the computer screen on almost each occasion, suggesting a reduced risk for complaints.
Besides the relevance of catastrophizing and fear-avoidance beliefs, several authors [8, 38, 41, 62] reported that observed control over pain or health is one of the principal process factors for outcome after myofeedback interventions. Although these studies concern traditional myofeedback approaches with other subject populations, it was hypothesized that the findings would also apply to the current study, but no effects were observed. One explanation might be that a few subjects in the Mfb/EC group had difficulties in responding to the feedback: They reported that they were on several occasions unable to relax and switch off the feedback this way. As a result they may not have experienced an increased control over their pain, explaining the absence of changes on a group level. It should also be considered that this CSQ subscale consisting of only two items has the lowest test-retest reliability of all subscales (r = 0.45) [46]. In addition, it should be acknowledged that the pain control subscale data is only available for half of the subjects as it was no part of the Swedish version of the SCQ. This small number of observations might have resulted in an inability to demonstrate changes. Further research, preferably combined with other methods to assess control is needed.
Muscle Activation Patterns
The myofeedback training in the current study aimed at increasing the time the trapezius is relaxed rather than reducing muscle activation. Accordingly, it was expected that muscle relaxation would be a key process factor in changing discomfort and disability after myofeedback training, in line with Vollenbroek-Hutten et al. [57] and that these changes would be more prominent for Mfb/EC than for the EC group as the latter group was not specifically trained to increase relaxation. However, no consistent change in muscle relaxation was found, neither a consistent relation between changed muscle activation and changed outcome. Rokicki et al. [38] studied the relation between tension headache and myofeedback-induced changes in muscle activation, and also found no association between change in muscle activation and change in outcome, and Sarnoch et al. [41] reported comparable findings. One explanatory concept is provided by Cram [9] who suggested that ‘temporal dislocation’ accounts for the discrepancy between changes in pain and changes in muscle activity. The initial changes in discomfort are hypothesized to be more likely brought about by cognitive changes rather than by muscle activation pattern changes. This might account for the absent relation. When looking at the baseline data muscle relaxation was already quite high (>50%) and muscle activation was low for the unilateral mouse tasks indicating a likely ceiling respectively floor effect for these parameters during these tasks. This finding might question the relevance of abnormal muscle activation patterns in persisting musculoskeletal complaints, at least in this specific subject sample. Although low amount of muscle rest during work has been associated with neck/shoulder symptoms [33], there are also studies not finding this association [33, 43, 49, 60]. Additional research needs to be done to further clarify the relation between muscle activation patterns and neck-shoulder pain, preferably specified into subgroups of subjects [55] with more severe complaints than those in the present study. Another explanation for absent changes in muscle activation patterns after myofeedback training may be that the continuous training provided at the work place may not necessarily result in changes in muscle activation patterns in a laboratory setting. It is therefore recommended to incorporate field studies in the evaluation of interventions for work-related neck-shoulder complaints, as this may provide insight in the course of changes in muscle activation patterns during training at work.
Concluding Remarks and Clinical Implications
The results of the present study indicate that the interventions for work-related neck-shoulder complaints show comparable beneficial effects for discomfort and disability, but there is no mean specific effect on muscle activation. Changes in the cognitive-behavioural factors, catastrophizing and fear-avoidance beliefs about work, were more prominent and appeared to be related to changes in discomfort and disability. Despite being inconclusive about the exact working mechanism, reducing catastrophic thoughts and fear-avoidance beliefs about work is probably playing a role in the mechanism of reducing discomfort and disability levels, and as such it is recommended to focus occupational interventions on at least these two factors. Whether this is best achieved with the currently investigated interventions needs to be studied further.
Although subjects might have changed their motor behaviour in response to the interventions this cannot be stated based on the results presented in the current study. Furthermore this study concerns a rather specific subject population, being only mildly affected, additional research is needed to investigate whether the findings can be generalised to subjects with more severe neck-shoulder complaints or with a different aetiology given the results of myofeedback training in a whiplash associated disorders (WAD) population.
Other factors than currently addressed may be related to changes in behaviour and perpetuation of this behaviour after the intervention, as is reflected in the low level of explained variance of the models. The number, relevance, or quality of the ergonomic changes performed during the intervention period might be such factors. Additional research needs to provide more insight into the relative contribution of different ergonomic adjustments to improvement after the intervention.
References
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Bingefors K, Isacson D. Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain–a gender perspective. Eur J Pain. 2004;8(5):435–50.
Birch L, Juul-Kristensen B, Jensen C, Finsen L, Christensen H. Acute response to precision, time pressure and mental demand during simulated computer work. Scand J Work Environ Health. 2000;26(4):299–305.
Bongers PM, Kremer AM, ter Laak J. Are psychosocial factors, risk factors for symptoms and signs of the shoulder, elbow, or hand/wrist?: A review of the epidemiological literature. Am J Ind Med. 2002;41(5):315–42.
Brandt LP, Andersen JH, Lassen CF et al Neck and shoulder symptoms and disorders among Danish computer workers. Scand J Work Environ Health. 2004;30(5):399–409.
Burns JW, Glenn B, Bruehl S, Harden RN, Lofland K. Cognitive factors influence outcome following multidisciplinary chronic pain treatment: a replication and extension of a cross-lagged panel analysis. Behav Res Ther. 2003;41(10):1163–82.
Burns JW, Kubilus A, Bruehl S, Harden RN, Lofland K. Do changes in cognitive factors influence outcome following multidisciplinary treatment for chronic pain? A cross-lagged panel analysis. J Consult Clin Psychol. 2003;71(1):81–91.
Chen WW. Enhancement of health locus of control through biofeedback training. Percept Mot Skills. 1995;80(2):395–8.
Cram JR. Surface EMG recordings and pain-related disorders: a diagnostic framework. Biofeedback Self Regul. 1988;13(2):123–38.
Ekman A, Andersson A, Hagberg M, Hjelm EW. Gender differences in musculoskeletal health of computer and mouse users in the Swedish workforce. Occup Med (Lond). 2000;50(8):608–13.
Fritz JM, George SZ. Identifying psychosocial variables in patients with acute work-related low back pain: the importance of fear-avoidance beliefs. Phys Ther. 2002;82(10):973–83.
Geisser ME, Casey KL, Brucksch CB, Ribbens CM, Appleton BB, Crofford LJ. Perception of noxious and innocuous heat stimulation among healthy women and women with fibromyalgia: association with mood, somatic focus, and catastrophizing. Pain. 2003;102(3):243–50.
George SZ, Fritz JM, McNeil DW. Fear-avoidance beliefs as measured by the fear-avoidance beliefs questionnaire: change in fear-avoidance beliefs questionnaire is predictive of change in self-report of disability and pain intensity for patients with acute low back pain. Clin J Pain. 2006;22(2):197–203.
Gift AG. Visual Analogue Scales: Measurement of a subjective phenomena. Nursing Research. 1989;30:268–88.
Hägg GM, Åström A. Load pattern and pressure pain threshold in the upper trapezius muscle and psychosocial factors in medical secretaries with and without shoulder/neck disorders. Int Arch Occup Environ Health. 1997;69(6):423–32.
Hasenbring M, Hallner D, Klasen B. Psychologische mechanismen im prozess der schmerzchronifizierung_unter- oder ueberbewertet. Schmerz. 2001;15:442–7.
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10(5):361–74.
Hermens HJ, Hutten MMR. Muscle activation in chronic pain: its treatment using a new approach of myofeedback. Int J Indust Ergon. 2002;30:325–36.
Hermens HJ, Vollenbroek-Hutten MM. Effects of electrode dislocation on electromyographic activity and relative rest time: effectiveness of compensation by a normalisation procedure. Med Biol Eng Comput. 2004;42(4):502–8.
Holroyd KA, Penzien DB, Hursey KG, et al. Change mechanisms in EMG biofeedback training: cognitive changes underlying improvements in tension headache. J Consult Clin Psychol. 1984;52(6):1039–53.
Horgen G, Aaras A, Dainoff MJ, Konarska M, Thoresen M, Cohen BG. A cross-country comparison of short- and long-term effects of an ergonomic intervention on musculoskeletal discomfort, eyestrain and psychosocial stress in VDT operators: selected aspects of the international project. Int J Occup Saf Ergon. 2005;11(1):77–92.
Huppes G, Peereboom KJ, Schreibers KBJ. (1997). Checklist RSI bij beeldschermwerk: preventie en reintegratie [Checklist RSI in computer work: prevention and rehabilitation]. Zeist: Kerckebosch.
Hägg GM. Static work loads and occupational myalgia- a new explanation model. Anderson PA, Hobart DJ, Danoff JVe. Electromyographical Electromyography. Elsevier Science Publishers B.V. (Biomedical Division), 1991:141–3.
Jensen IB LSJ. Coping Strategies Questionnaire (CSQ): Reliability of the Swedish version of the CSQ 1993:139–45.
Jensen MP, Turner JA, Romano JM. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J Consult Clin Psychol. 2001;69(4):655–62.
Karsh B-T, Moro FBP, Smith MJ. The efficacy of workplace interventions to control musculoskeletal disorders: a critical analysis of the peer-reviewed literature. Theor Issues Ergon Sci. 2001;2(1):23–96.
Laursen B, Jensen BR, Garde AH, Jorgensen AH. Effect of mental and physical demands on muscular activity during the use of a computer mouse and a keyboard. Scand J Work Environ Health. 2002;28(4):215–21.
Linton SJ, van Tulder MW. Preventive interventions for back and neck pain problems: what is the evidence? Spine. 2001;26(7):778–87.
Makela M, Heliovaara M, Sievers K, Impivaara O, Knekt P, Aromaa A. Prevalence, determinants, and consequences of chronic neck pain in Finland. Am J Epidemiol. 1991;134(11):1356–67.
Mathiassen SE, Winkel J, Hägg GM. Normalization of surface EMG amplitude from the upper trapezius muscle in ergonomic studies—a review. J Electromyogr Kinesiol. 1995;5(4):197–226.
Merskey H, Bogduk N. Classification of chronic pain, second edition, IASP Task Force on Taxonomy. Seattle: IASP Press; 1994.
Nielson WR, Jensen MP. Relationship between changes in coping and treatment outcome in patients with Fibromyalgia Syndrome. Pain. 2004;109(3):233–41.
Nordander C, Hansson GA, Rylander L, et al. Muscular rest and gap frequency as EMG measures of physical exposure: the impact of work tasks and individual related factors. Ergonomics. 2000;43(11):1904–19.
Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48(12):1503–10.
Pernold G, Mortimer M, Wiktorin C, Tornqvist EW, Vingard E. Neck/shoulder disorders in a general population. Natural course and influence of physical exercise: a 5-year follow-up. Spine. 2005;30(13):E363–8.
Pocock SJ. Clinical trials; a practical approach. Chicester: Joh Wiley and Sons; 1997.
Pollard CA. Preliminary validity study of the pain disability index. Percept Mot Skills. 1984;59(3):974.
Rokicki LA, Holroyd KA, France CR, Lipchik GL, France JL, Kvaal SA. Change mechanisms associated with combined relaxation/EMG biofeedback training for chronic tension headache. Appl Psychophysiol Biofeedback. 1997;22(1):21–41.
Sandsjö L, Larsman P, Vollenbroek-Hutten MM, et al. Comparative assessment of study groups of elderly female computer users from four European countries: questionnaires used in the NEW study. Eur J Appl Physiol. 2006;96(2):122–6.
Sandsjö L, Melin B, Rissen D, Dohns I, Lundberg U. Trapezius muscle activity, neck and shoulder pain, and subjective experiences during monotonous work in women. Eur J Appl Physiol. 2000;83(2–3):235–8.
Sarnoch H, Adler F, Scholz OB. Relevance of muscular sensitivity, muscular activity, and cognitive variables for pain reduction associated with EMG biofeedback in fibromyalgia. Percept Mot Skills. 1997;84(3 Pt 1):1043–50.
Severeijns R, Vlaeyen JW, van den Hout MA, Weber WE. Pain catastrophizing predicts pain intensity, disability, and psychological distress independent of the level of physical impairment. Clin J Pain. 2001;17(2):165–72.
Sjogaard G, Sogaard K, Hermens HJ, et al. Neuromuscular assessment in elderly workers with and without work related shoulder/neck trouble: the NEW-study design and physiological findings. Eur J Appl Physiol. 2006;96(2):110–21.
Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7(4):261–71.
Snijders T, Bosker R. Multilevel analysis. An introduction to basic and advanced multilevel modeling. London: Sage; 1999.
Spinhoven Ph, ter Kuile MM, Linssen ACG. CPV Coping met Pijn Vragenlijst [Dutch version of tthe Coping Strategies Questionnaire]. Lisse: Swets & Zeitlinger B.V.; 1994.
Swinkels-Meewisse EJ, Swinkels RA, Verbeek AL, Vlaeyen JW, Oostendorp RA. Psychometric properties of the Tampa Scale for kinesiophobia and the fear-avoidance beliefs questionnaire in acute low back pain. Man Ther. 2003;8(1):29–36.
Tait RC, Chibnall JT, Krause S. The Pain Disability Index: psychometric properties. Pain. 1990;40(2):171–82.
Thorn S, Sogaard K, Kallenberg LA, et al. Trapezius muscle rest time during standardised computer work - A comparison of female computer users with and without self-reported neck/shoulder complaints. J Electromyogr Kinesiol. 2007;17(4):420–7.
Todd KH, Funk KG, Funk JP, Bonacci R. Clinical significance of reported changes in pain severity. Ann Emerg Med. 1996;27(4):485–9.
Vendrig A, Duetz P, Vink I. Nederlandse vertaling en bewerking van de fear-avoiance beliefs questionnaire. Nederlands Tijdschrift Voor Pijn En Pijnbestrijding. 1998;18:11–4.
Vlaeyen JW, Kole-Snijders AM, Boeren RG, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain. 1995;62(3):363–72.
Voerman GE, Sandsjö L, Vollenbroek-Hutten MM, Groothuis-Oudshoorn CG, Hermens HJ. The influence of different intermittent myofeedback training schedules on learning relaxation of the trapezius muscle while performing a gross-motor task. Eur J Appl Physiol. 2004;93(1–2):57–64.
Voerman GE, Sandsjö L, Vollenbroek-Hutten MMR, Larsman P, Kadefors R, Hermens HJ. Effects of ambulant myofeedback training in female computer workers with work-related neck-shoulder complaints: a randomized controlled trial. J Occup Rehabil. 2007;17(1):137–52.
Voerman GE, Vollenbroek-Hutten MM, Hermens HJ. Upper trapezius muscle activation patterns in neck-shoulder pain patients and healthy controls. Eur J Appl Physiol. 2006.
Voerman GE, Vollenbroek-Hutten MM, Hermens HJ. Changes in pain, disability, and muscle activation patterns in chronic whiplash patients after ambulant myofeedback training. Clin J Pain. 2006;22(7):656–63.
Vollenbroek-Hutten M, Hermens H, Voerman G, Sandsjö L, Kadefors R. Are changes in pain induced by myofeedback training related to changes in muscle activation patterns in patients with work-related myalgia? Eur J Appl Physiol. 2006;96(2):209–15.
Vowles KE, Gross RT. Work-related beliefs about injury and physical capability for work in individuals with chronic pain. Pain. 2003;101(3):291–8.
Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–68.
Westgaard RH, Vasseljen O, Holte KA. Trapezius muscle activity as a risk indicator for shoulder and neck pain in female service workers with low biomechanical exposure. Ergonomics. 2001;44(3):339–53.
Westgaard RH, Winkel J. Ergonomic intervention research for improved musculoskeletal health: a critical review. Int J Indust Ergon. 1997;20:463–500.
Woby SR, Watson PJ, Roach NK, Urmston M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? Eur J Pain. 2004;8(3):201–10.
Woby SR, Watson PJ, Roach NK, Urmston M. Adjustment to chronic low back pain–the relative influence of fear-avoidance beliefs, catastrophizing, and appraisals of control. Behav Res Ther. 2004;42(7):761–74.
Acknowledgement
This work was undertaken within the project Neuromuscular Assessment of the Elderly Worker (NEW) with partial financial support from the EC within the RTD action DRLT 2000 00139, AFA Insurance (Sweden), and by funding of the exchange visits by NWO-NL and the Swedish Research Council. The authors would like to thank Lena Grundell, Richel Lousberg, Karin Groothuis, and Linda Oostendorp for their valuable contribution to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Voerman, G.E., Sandsjö, L., Vollenbroek-Hutten, M.M.R. et al. Changes in Cognitive-Behavioral Factors and Muscle Activation Patterns after Interventions for Work-Related Neck-Shoulder Complaints: Relations with Discomfort and Disability. J Occup Rehabil 17, 593–609 (2007). https://doi.org/10.1007/s10926-007-9109-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-007-9109-9