
Abstract
Background: Supervisors’ attitudes and measures have been pointed out by employees to influence the return to work process. The purpose of this study was to explore supervisors’ views on employer responsibility in the return to work process and factors influencing the support of sick-listed employees. Method: The focus group method was used. Six groups were conducted and each group met on one occasion. Twenty-three supervisors experienced in managing sick-listed employees participated. Result: Two different themes emerged; In “The Supervisor is the Key Person” the participants found themselves as being key persons, carrying the main responsibility for the rehabilitation of the sick-listed employees and for creating a good working environment, thus preventing ill health and sick-listing among the employees. In the second theme “Influential Factors in Rehabilitation Work” the participants described the rehabilitation work as a part of a greater whole influenced by society, demands and resources of the workplace and the interplay between all parties involved. Conclusion: The study gives us the supervisors’ perspective on the complexity of the return to work rehabilitation. This knowledge could be invaluable and be used to improve the possibilities for developing successful collaboration in occupational rehabilitation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
According to employees, the return to work process is greatly influenced by employers’ attitudes and measures, and the supervisors’ role has been described as significant [1–3]. Women on sick leave due to work-related strain have stressed the importance of communication with the supervisor and the employer’s representative, and how both positive and negative feedback from them affect the women’s possibilities for returning to work. A positive interactive communication between the individual and the supervisor was described as essential [1]. Creating a positive attitude and a “welcome back” atmosphere gives the employees a sense of being valued and facilitates a return to work. Hostility and harassment at the workplaces can be prevented by adequate information provided by the supervisor or the employer’s representative to workmates [1–3]. These findings are all from the employees’ perspective, so finding out the supervisors’ point of view regarding possibilities for returning to work is of great interest.
In the early nineties, legislation in Sweden increased employers’ responsibility regarding rehabilitation back to work for employees on sick leave. The employers have to, within four weeks, initiate an investigation to facilitate rehabilitation back to work for employees on long-term sick leave. The employee’s immediate supervisor is generally responsible for initiating the investigation and, together with the employee, has to assess the required measures for promoting rehabilitation. The investigation has to be sent to the local Social Insurance Office within eight weeks [4]. Studies have shown that approximately 30 to 50 percent of the sick-listed employees have been subjects of rehabilitation investigation by their employer, and that these individuals gained access to vocational training and rehabilitation to a larger extent than others [5, 6]. Early intervention at the workplace including early collaboration between all the parties involved significantly decreases the risk of long-term sickness absence and thus lessens public expenditures [6]. Employer accommodation has also been shown to decrease the risk for job exit for disabled workers [7].
To find successful measures for preventing and decreasing the development of long-term sickness absence, it is of great concern to investigate the interaction between the individual and the environment and to capture the views of the parties involved. Evidently, earlier studies made from the perspective of the individual on sick leave point out the significance of employers’ attitude and measures and the role of the supervisors [1–3]. To our knowledge, very few studies have been made from the employers’ perspective. It is therefore interesting to look into matters such as how supervisors look upon their rehabilitation responsibility and the resources available in the return to work process, as well as their demands on employees and other parties involved. Consequently, the aim of this study was to explore the supervisors’ views on employer responsibility in the return to work process and their views on the possibilities for and obstacles to supporting employees on sick leave.
Method
The focus group methodology was used. It has the form of group discussions and is suitable for picking up the views and experiences of a selected group, which will generate a broad knowledge and understanding. The aim of the methodology is to stimulate the interaction between the participants in the target group so that as many opinions and views as possible about the selected research topic will be discussed. The group process encourages the participants to clarify not only what they think, but also how and why they think in a certain way [8–11]. A focus group consisting of up to six persons seems to be preferable to larger groups, since this allows dynamic discussion with enough room for each of the members to express their opinion [8, 9].
The study was approved by the Ethics Committee of the Faculty of Medicine, Göteborg University, Sweden.
Participants
To create group identity and an atmosphere stimulating discussion, it was essential to consider the homogeneity of the participants in the target group when composing the focus groups [8–10]. The target group comprised supervisors and staff responsible for and experienced in managing employees on sick leave. In this study immediate supervisors and staff with rehabilitation responsibility for employees on sick leave and with experience of making rehabilitation investigations were asked to participate. Homogeneity was primarily represented by the participants’ shared experience in managing employees on sick leave. To obtain a broad representation of the target group between and within the focus groups, researchers considered heterogeneity concerning age, professional and supervisor experience, size of represented companies and work places in the participant selection.
In order to find supervisors experienced in managing employees on sick leave, rehabilitation professionals working in primary health care and case managers at the local Social Insurance Office were asked to suggest employers with such experience. The researchers also searched the telephone directory and specific websites for suitable participants. A total of 30 persons were eventually asked to participate, of which three declined on the grounds of lack of time. Of the 27 who accepted, four found the time of the focus groups unsuitable. The final number of participants was 23. Six groups were carried through; two groups consisting of five participants, two groups of four, one group of three and one group of two participants. The educational and professional levels were similar within each group, and most participants were in public employment. Participants’ age ranged from 31 to 65 years (mean age 48). Professional experience ranged from three to 43 years and supervisor experience from three to 39 years. The workforce of the companies ranged from 14 to 16,990 employees, and that of the workplaces ranged from 14 to 170. The study group consisted of both women and men, with women in the majority. The mean sick leave rate of the workplaces was 6%. The rate varied between the workplaces and at the time of the study ranged from 0 to 14%. The employees of the workplaces were predominantly female. However, the group consisting solely of male supervisors represented male-dominated workplaces. Demographic data of the participants are presented in Table 1.
Procedure
A letter was sent to the supervisors informing them of the aim and procedure of the study. A phone call with further information of the study and an inquiry to participate was made. Both the written and oral information stressed that participation was voluntary and that the participants could withdraw at any time. The project leader (first author) met the participants individually once before the group session. The participants were given the opportunity to present themselves and to ask more about the study. The project leader obtained information about the participants and the workplaces represented, and was able to compose the groups with respect to the homogeneity of the participants. The study took place during the spring of 2004 at the Sahlgrenska Academy, Göteborg University, Sweden. Each group met on one occasion and the session lasted for one to one and a half hours. The discussions were audio taped. All groups had the same moderator (second author) and assistant moderator (first author). The moderator guided the discussion and encouraged all the group members to participate and express their own views on the topic as freely as possible. The participants presented themselves briefly and the moderator introduced the topic by asking some general questions about the participants’ experiences of managing employees on sick leave. The discussions then concentrated on the following key questions:
-
How do you view your responsibility in the return to work process?
-
How do you view the possibilities for supporting an employee on sick leave to return to work?
-
How do you view the obstacles to supporting an employee on sick leave to return to work?
-
What kind of demands do you make on the employee on sick leave and on others?
Analysis
The audio taped group sessions were transcribed verbatim, and the transcripts from the groups were analyzed by the first author with the assistance of the second author. The method used to analyze the material is described by Krueger [12]. To become familiar with and to understand the content of the material in its context the first step in the analysis procedure was to listen through the tapes several times. All the transcripts were then read and analyzed. Sections relevant to the research topic were identified and sorted out according to the research questions. The next step was to create themes and categories that corresponded to the meaning of the material. At this stage, the working material was still in the form of raw data in order to comprehend the contextual meaning of the material. Based on the raw data, descriptive statements were made and illustrative quotations were selected. Finally, the descriptive statements constituted the foundation of synthesizing, abstracting and conceptualizing the data.
Result
Two different themes emerged from the focus group discussions. The first theme, “The Supervisor is the Key Person,” contains the categories describing the meaning of the participants’ views of their role as supervisors. The second theme, “Influential Factors in Rehabilitation Work,” contains the participants’ views on which factors influence rehabilitation work and return to work possibilities for the sick-listed.
The supervisor is the key person
This theme contains the participants’ view of themselves as key persons in preventive and rehabilitation work concerning sick-listed employees. The participants describe how they carry the main rehabilitation responsibility and how they see themselves as tools in the rehabilitation work. The participants also describe making high demands on themselves and at the same time being conscious of the difficulties these demands entail. They find that their responsibility is to create a good working environment, thus preventing ill health and sick-listing among the employees. Still, there is uncertainty about how far the rehabilitation responsibility reaches, i.e. where to draw the line between the responsibility of the employer and that of the employee.
Creating confidence
One important issue that emerges in the discussions is that of creating confidence between the supervisor and the sick-listed employee. A prerequisite for this is showing respect and having trust in the sick-listed person. In order to create confidence, regular contact between the sick-listed employee and the supervisor is essential, as is contact with the workplace. The latter is maintained by inviting the sick-listed employee to meetings, training courses and other social activities. Workmates are encouraged to keep contact with the sick-listed employee. Creating confidence is, however, found to be difficult when the person declines contact with the supervisor or the workplace. Establishing confidence at an early stage when an employee does not feel well and trying to find a solution in collaboration with the employee are seen as preventive actions to avoid long-time sickness absence. An excerpt from discussion,
-
P4
As a boss you have a tremendous, how shall I put it, influence on the individual. And I feel, I really do feel … One feels rather humble at times, like. So, one really, well, think twice about things, so as one … or, well, “I” feel strongly that you influence the actual person really quite a lot.
-
P3
Yeah, especially if that person has confidence in you. That’s the way it is.
-
P4
Yeah, I think it affects the results as well, I believe. That you have both … have good contact, but also that you have a fairly good climate in your workplace.
-
P5
That really means a lot.
-
P4
That is really important.
-
P5
Yes it is.
Being a support
The participants describe it as essential that the supervisor is a support to the sick-listed person during the entire return to work process. One part of the supportive work is to show understanding for the sick-listed employee’s total situation, in working as well as private life. Another part is to be flexible, forthcoming and bent on problem-solving to create prerequisites for a return to work. However, the participants find support in the form of encouraging or checking achievements, like walking a tightrope. It is also considered important to be of support to the individual in relation to the workmates and to create a welcoming atmosphere in the workplace. It is, however, considered essential not to take a counseling role trying to solve the employee’s personal problems.
Making demands
It is considered important by the participants to make demands on the sick-listed employees, which includes these following regulations, as well as taking responsibility for their own rehabilitation. When making demands, the participants describe it as important that the information coming from the supervisor to the sick-listed is clear and communicated both orally and in writing. Regulations concerning the employer’s rehabilitation responsibility and the demands on the employees should be explicit. The participants find the rehabilitation plan to be an important tool for making demands. It is an agreement between the employer and the employee and is described as being straight-forward.
Acknowledging every employee
The participants discuss the value of acknowledging each and every employee and giving positive feedback on their efforts. They consider this sort of attention to be a way of preventing ill health and sick-listing. They also find it important to keep contact and socialize regularly with the employees as a way of acknowledging every employee.
Encouraging participation
The participants considered employees’ participation when creating a good work environment as a prioritized goal. The participants describe how they engage the whole work-team to develop a common value-system where everybody learns how to handle conflicts and take responsibility at work. The views are that when the employees feel secure and are getting on and having fun together, they can concentrate on doing a good job, and so prevent sick-listing.
Uncertainty about rehabilitation responsibility
The participants express uncertainty as to how far their responsibility for rehabilitation should go. When the cause of the sick-listing is not work-related, but is related to private problems, the participants experience a difficulty in knowing if, how and in what way measures should be taken. They receive support and guidance from colleagues in difficult rehabilitation matters.
Influential factors in rehabilitation work
This theme contains the participants’ views on the factors that influence rehabilitation work and the return to work possibilities for those on sick leave. The participants describe how these factors influence positively or negatively and some even both ways. The factors are found on an individual, organizational and social level.
Employee motivation
The sick-listed employee’s own motivation for returning to work is described as essential. The participants express that the sick-listed might have a variety of motives for being sick-listed. These could be related to work, such as not being happy with the work situation, workmates or hours; or matters of a private nature, such as ongoing insurance matter, economy and time-consuming recreational activities. To prevent the motivation from deteriorating, it is advisable to initiate rehabilitation at an early stage. Return to work is made difficult when the sick-listed employee denies having any personal responsibility for the rehabilitation and is prone to shift all responsibility onto the employer. The participants discuss the possibility of the employer being able to demand an answer from the employee whether she wants to return to work or not. If “not” is the case, the discussion revealed that the person should resign from work on her own initiative.
Co-worker support
Workmates engaging themselves in supporting the sick-listed is found to facilitate a return to work. The participants perceive that when rehabilitation succeeds, it is not only the sick-listed employee and the supervisor that come out strengthened, but the whole working team. However, hierarchies in a working group are described as obstructing the return to work for a person disliked by the group.
Employer policies and practices
The participants relate that the employers have developed routines for how preventive as well as rehabilitation work should be carried out. Routines are viewed as a support in rehabilitation work, are well-structured and are solution-orientated. They are based on legislation referring to employers’ rehabilitation responsibility. The participants find staff specialized in rehabilitation matters supportive and describe a regular use of their services.
Work demands
The participants experience that the nature of the job and the work organization make demands on the employees both physically and mentally. Competence requirements are described as generally having risen in recent years, and people with a university education are considered better qualified to meet these raised requirements. To meet the high demands and to create a good psychosocial work environment, employees are given the opportunity to take part in guidance, lectures and training courses. Furthermore, the participants talk about how the employers invest in good physical environments by use of job rotation, ergonomic working tools, as well as ergonomic training.
Economic factors
The participants point out that the economy controls the conditions to a very high extent, and that the supervisor is responsible for keeping the budget balanced, which entails severe rationalization of work. The participants describe a conflict between keeping the budget balanced and finding suitable tasks for a sick-listed person who gradually increases work capacity in order to return to work. The participants discuss the difficulty that they as supervisors find in adapting tasks for a person with a limited work capacity when it is necessary to economize.
Incentives to keep fit
The participants describe how the employer deliberately pursues active keep-fit measures with the purpose of preventing ill health and sick-listing among the employees. Keep-fit measures are stimulated through subsidized fitness centre memberships, time for exercise and information campaigns on lifestyle matters. Still, the participants think that keeping fit should mainly be the personal responsibility of the individual employee.
Collaboration and communication
The participants consider it important that the parties involved, i.e. employers, case manager at the local Social Insurance Office and health care professionals should have a mutual approach to rehabilitation work. A common outlook, common planning and collaboration are essential. Regular meetings with all parties, including the sick-listed, facilitate rehabilitation. The participants particularly appreciate regular contact with the case manager at the Social Insurance Office and the case manager putting pressure on the sick-listed person to take an active part in the rehabilitation work. The participants experience that lack of common outlook affects the work negatively and that this is largely due to the sick-listing doctor’s lack of knowledge of the actual workplace. An excerpt from discussion,
-
P2:
But I think that’s positive, the contact we’ve established with Social Insurance thanks to the attention rehabilitation has received the last few years. It’s really much better. We speak the same language more than we did before. In those days I felt that we didn’t understand the Social Insurance regulations and they didn’t understand the individual’s conditions at work. That’s how I feel it has turned out – we’re collaborating fine.
-
P3:
Yeah, things have changed.
-
P2:
Yeah things really have changed …
-
P3:
… is more valued … than before. Rehab-legislation and all that has been around for quite some time, now, and all.
-
P2:
Yes, but you didn’t see them.
-
P3:
No.
-
P2:
And you heard – most often it was the individual herself that carried messages from Social Insurance and what we said. And there was, like no comprehensive or mutual view. So that’s actually very good.
-
P1:
Yes, they’ve been pressurized by …
-
P3:
Yeah. Yeah, and they’ve got to get started with rehab. They had rehab-money left, wasn’t that so?
-
P1:
That’s right.
-
P3:
Like, loads of sick-listing and stuff – it’s obvious that they had to share in the work, otherwise …
-
P4:
It’s a positive thing, this with the rehab meetings with Social Insurance at the workplaces, so as they get to know the reality of the sick-listed. I think that, I really must say, that I think it has been a positive thing with Social Insurance, and there hasn’t been any fuss. The person we’ve been working with has really done a good job.
-
P3:
Yeah, that goes for us, too.
Societal norms
The participants find that society’s attitude towards sick-listed employees has changed in recent years. The prevailing standpoint makes greater demands on people on sick leave to take responsibility and an active part in the rehabilitation. They discuss that demands are also made on these to be trained back into the regular job rather than to adapted tasks or easier work. Society’s regulations and legislation can, however, be rather stiff and formal and render flexible solutions in the workplace difficult.
Summary of results
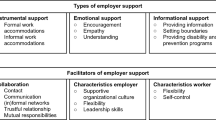
The results can be illustrated in a figure (Fig. 1). From the discussions it emerged that the supervisors see themselves as key persons, carrying the main responsibility for the rehabilitation of the sick-listed employees and continuously interacting with both the sick-listed person and her workmates. The supervisor’s interplay with the parties involved, inside and outside the workplace, is described as essential to the rehabilitation work, as is the interplay between the sick-listed and the workmates. The employer’s and supervisor’s rehabilitation work is seen as a part of a greater whole influenced by the prevailing social climate and the demands and resources of the workplace.

The supervisor is described as the key person in the rehabilitation work, interacting in a greater whole influenced by the prevailing social climate and the demands and resources of the workplace
Discussion
The aim of this study was to find out how supervisors look upon employer responsibility in the return to work process and how they view the possibilities for supporting employees on sick leave. It can be stated that the supervisors describe a thorough commitment to their rehabilitation responsibility and to their work with employees on sick leave. They see themselves as key persons carrying the main responsibility for initiating all collaboration and necessary measures. The supervisors also seek to establish a mutual confidence between themselves and those on the sick list, and stress the importance of being supportive throughout the whole process of returning to work. They also have an ambition to engage workmates in creating a welcome back atmosphere in the workplace and a good work environment. All these findings correspond well with aspects described as significant in studies carried out from the employee’s perspective [1–3] where supervisor contact, encouragement and information are described as central factors for returning to work. Additionally, substantial supervisor support has been found to be a predictive factor for returning to work and to promote the individual’s rehabilitation back to work [13, 14]. Supervisor behavior such as frequent communication between the supervisor and the sick-listed individual was shown to hasten the return to work [13]. The supervisors in this study are aware of the value building up confidence between them and the sick-listed employee and being supportive in the process of returning to work. The supervisors’ great commitment, engagement and sense of responsibility were unexpected but gratifying. It shows that their key position could be used in preventive work aiming to decrease long-term sickness absence in the workplaces and can be central in a return to work program designed in collaboration with the social insurance office and rehabilitation professionals.
In earlier research [1] sick-listed women also emphasized the importance of having supervisors sympathizing with them and helping them to alter their work situation. On the other hand, the sick-listed women stressed that an unchanged work situation was the determining obstacle to returning to work [1]. Despite the supervisors’ serious ambition to be supportive, they do not have enough resources to carry out their intentions to facilitate their employees’ return to work. The supervisors have to recognize several other interests and they have to acknowledge not only the ones on the sick list, but workmates, other parties involved, and the demands of society and the business organization. They experience a conflict between on one hand high work demands and a balanced economy and on the other the need for modified work duties. This concern was also found in a study where the majority of employers had difficulty in providing suitable duties for injured workers. The main reasons given were that the nature of the work made it impossible to modify the activities and that suitable duties were not productive [15]. However, reviews of the effectiveness of modified work program stated that the program facilitate return to work. Modified work enables not only the disabled workers to return to work twice as often but also economic advantages as it lessens the number of lost work days [16, 17]. In the present study, the supervisors describe that keeping the budget balanced entails high work rationalization leading to high work demands on the employees. In Sweden large cuts in public services were made during the nineties and may have resulted in an increased workload for the remaining workforce [18, 19]. Downsizing has, in fact, been shown to be associated with an increased sickness absence among the remaining employees [20, 21]. In this study, the supervisors describe keeping the economy in balance as a matter resting on the individual supervisor, and although they have every intention to support their sick-listed employees back to work, they lack sufficient recourses for carrying it through. It seems that this issue cannot be solved by the individual supervisor but ought to be a matter for the company as a whole. In order to decrease or prevent sickness absence, society should work together with employers in these matters and try to find policies promoting modified workplaces, suitable tasks and less rationalization.
The supervisors consider that engaging all co-workers in creating a good work environment aiming to prevent ill health and sickness absence is a valuable task. They also stress the importance of workmates being supportive and keeping in contact with the sick-listed individual. The interplay between the sick-listed individual and the workmates is described as improving the possibility of returning to work. Research has shown that social support at work is associated with decreased sickness absence and return to work [22–24]. Sick-listed women [1] have also described the importance of workmates keeping contact and how this encouraged them, made them feel welcome back and increased their self-confidence. The supervisors in this study are, however, also aware of the effect of a more hostile climate among co-workers towards sick-listed employees, and how this renders a return to work difficult. Women who reported being bullied in the workplace [24–26] had a double risk of high incidence of sickness absence. Furthermore, several studies have revealed that poor social support at work from supervisors and/or workmates has been associated with prolonged sickness absence [22, 23,25]. The supervisors in this study are fully conscious of this problem and do express that supporting the sick-listed employee in relation to workmates is an essential part of rehabilitation work.
In this study, the motivation of the sick-listed was expressed as a decisive factor in successful rehabilitation. The supervisors experienced that both work-related and private factors were reasons for individuals not wanting to return to work. Research has also shown that sickness absence is complex, being not only work-related but also influenced by several different factors and aspects [1, 25, 27–30]. Socioeconomic factors, life-style and adverse life events are found to affect the rehabilitation process and sickness absence in both women and men [25, 27]. Sick-listed women [1] have described how personal characteristics such as having high demands of capacity, a high sense of responsibility and difficulty in setting limits influence the work situation, sickness absence and rehabilitation. Likewise, the domestic sphere seems to affect women to a higher extent than men. Domestic workload and responsibilities are shown to be connected with obstacles to rehabilitation and increased sickness absence especially in women with children at home [25, 28, 29] as is domestic harassment experienced by women [28, 30]. Although the supervisors state that they understand that the sick-listed person’s total life situation has to be considered and that it has an influence on the return to work possibilities, they find it difficult to draw the line regarding the employer’s rehabilitation responsibility and to find suitable measures. This is especially true when the reason for sick-listing is perceived by the supervisors not to be work-related.
The supervisors believe that it is important to co-operate with other parties involved in the rehabilitation process and to establish a mutual outlook. The collaboration with case managers at the Social Insurance Office is described as working out especially well. In an intervention study, it appeared that giving case managers a more active role in the rehabilitation process back to work resulted in a higher proportion of sick-listed individuals returning to work [6]. It was also shown that sick-listed employees who had received a rehabilitation investigation gained access to rehabilitation program and vocational rehabilitation more often than others [5, 6]. However, the supervisors occasionally describe a lack of understanding, particularly from health professionals, resulting in a negative affect on the rehabilitation process. Professionals in rehabilitation usually have a client-centered perspective putting forward the interests of the client. This is a vital part in all rehabilitation and necessary for a successful outcome [31, 32]. Yet, it is an essential assignment as professionals in rehabilitation to comprehend not only the sick-listed persons but also the conditions at their workplace. Therefore, it is important that professionals also acknowledge the perspectives of the supervisors and seek a mutual outlook in order to promote the return to work process. The perspective given by the supervisors in this study is valuable knowledge and can provide an understanding enabling fruitful collaboration between rehabilitation professionals and responsible supervisors.
The focus group methodology was used. To achieve a satisfying result it is essential to create an atmosphere stimulating an open discussion. This is depending on both the composition of the groups and on the role of the group leader [8–11]. When the focus groups were formed, homogeneity was considered, and was mainly represented by the shared experience of managing employees on sick-leave. Having something in common such as sharing experiences has been shown to be enough to create group identity and to provide interactive discussions wherein a variety of views about the research topic will be discussed [1, 8, 10]. The role of the group leader is crucial for the outcome of the discussions as well. In this study, the group leader was well experienced in guiding focus group discussions and had the ability to create an open climate encouraging discussion. This, together with the compositions of the groups, resulted in the discussions being lively and interactive. Face validity was reached by the participants confirming and opposing each other’s views throughout the discussion. It is essential in the analytical process to stick to the raw data as long as possible and to analyze the data in its context [12]. The themes and categories presented in this study were significant throughout all the different discussions.
However, the focus group discussion is a qualitative method and the results of this study cannot be generalized and have to be interpreted with caution. As mentioned above, to create group identity homogeneity had to be considered while composing the groups. The majority of the participants was representing public employers. This can be explained by the fact that the majority of the sick-listed employees in Sweden are women [33]. Given the gender segregation, with women in the public and men in the private sector [19], the chances of recruiting supervisors representing public employers were high. As the target group comprised supervisors with experience in managing employees on sick leave, we can assume that the members of the focus groups were interested in rehabilitation matters, were well experienced in making rehabilitation investigations and represented employers with policies and routines for rehabilitation. The supervisors in this study also describe having experience of structured rehabilitation routines and collaboration with case managers. Studies have pointed out that less than half of the employers conduct and send a rehabilitation investigation to the Social Insurance Office. The investigation constitutes a starting point for the case manager coordinating rehabilitation [5, 6]. Thus, we could perhaps conclude that supervisors participating in this study represent employers conducting investigations and being used to collaboration. Further research is needed to understand the perspectives of all those employers with less or no experience of rehabilitation of sick-listed employees and also of representatives of private employers, since the majority of the participants represent public employers.
The supervisors in this study describe a situation where many aspects have to be taken into account, and they see rehabilitation work as a part of a greater whole influenced by the prevailing social climate, the demands and resources of the workplace and the interplay between all parties involved. To be engaged in activity such as being able to work can be described as the dynamic relationship between the individual, in her occupations and roles, and the environment. The individual and the environment are dependent on each other, and changes in either one influence the possibilities of performance. An individual’s context is unique, and the individual both affects and is affected by her context, which results in continually changing prerequisites for performing activities and occupations [34, 35]. In this study, the supervisors give us their perspective on managing employees on sick leave back to work, and we learn how they perceive and view the complexity of this process. The supervisors have to consider many different aspects and illustrate how all the different factors are interwoven and dependent of each other. They tell us about how possibilities and obstacles in both the environment and in the individuals interact and have an impact on the rehabilitation process. These perspectives and experiences described by the supervisors could be of great value to all parties involved in the return to work process.
Conclusion
In this study the supervisors find themselves to be key persons and express a thorough commitment to the rehabilitation responsibility. They describe the rehabilitation work as a part of a greater whole influenced by society, demands and resources of the workplace and the interplay between all parties involved. Despite the supervisors’ serious ambition to be supportive, they see a conflict between keeping the budget balanced and finding suitable tasks for the sick-listed employees returning to work. This study gives us the supervisors’ perspective on the complexity of the return to work rehabilitation and shows how the interaction between individuals and the environment seen in its context influences the process. This knowledge could be invaluable for rehabilitation professionals and other parties involved when comprehending workplace conditions and could be used to improve the possibilities for developing successful collaboration in occupational rehabilitation.
References
Holmgren K, Dahlin Ivanoff S. Women on sickness absence–views of possibilities and obstacles for returning to work. A focus group study. Disabil Rehabil 2004;26(4):213–222.
Nordqvist C, Holmqvist C, Alexanderson K. Views of laypersons on the role employers play in return to work when sick-listed. J Occup Rehabil 2003;13(1):11–20.
Strunin L, Boden LI. Paths of reentry: Employment experiences of injured workers. Am J Ind Med 2000;38(4):373–384.
Riksförsäkringsverket. Socialförsäkring. Lagen om allmän försäkran och andra författningar (Social Insurance. The law of general insurance and other constitutions.): Riksförsäkringsverket, 2001. Report No.: AFL 22:3. (In Swedish.)
Heijbel B, Josephson M, Jensen I, Vingard E. Employer, insurance, and health system response to long-term sick leave in the public sector: Policy implications. J Occup Rehabil 2005;15(2):167–176.
Arnetz BB, Sjogren B, Rydehn B, Meisel R. Early workplace intervention for employees with musculoskeletal-related absenteeism: A prospective controlled intervention study. J Occup Environ Med 2003;45(5):499–506.
Burkhauser RV, Butler JS, Yang WK. The importance of employer accommodation on the job duration of workers with disabilities: A hazard model approach. Labour Economics 1995;2:109–130.
Dahlin Ivanoff S. Focus group discussions as a tool for developing a health education programme for elderly persons with visual impairment. Scan J Occup Ther 2002;9:3–9.
Kitzinger J. The methodology of focus groups: The importance of interaction between research participants. Sociology of Health and Illness 1994;16:103–121.
Krueger RA. Quality control in focus group research. In: Morgan DL, ed. Successful focus groups. Advancing the state of the art. California: Sage Publication; 1993, pp. 65–85.
Kitzinger J, Barbour R. Introduction: The challenge and promise of focus groups. In: Barbour R, Kitzinger J, ed. Developing focus group research. Politics, theory and practice. London: Sage Publications; 1999, pp 1–20.
Krueger RA. Focus group. A practical guide for applied research. California: Sage Publications; 1988.
Nieuwenhuijsen K, Verbeek JH, de Boer AG, Blonk RW, van Dijk FJ. Supervisory behaviour as a predictor of return to work in employees absent from work due to mental health problems. Occup Environ Med 2004;61(10):817–823.
Janssen N, van den Heuvel WP, Beurskens AJ, Nijhuis FJ, Schroer CA, van Eijk JT. The Demand-Control-Support model as a predictor of return to work. Int J Rehabil Res 2003;26(1):1–9.
Kenny DT. Employers’ perspectives on the provision of suitable duties in occupational rehabilitation. J Occup Rehabil 1999;9(4):267–276.
Krause N, Dasinger LK, Neuhauser F. Modified work and return to work: A review of the literature. J Occup Rehabil 1998;8(2):113–139.
Franche RL, Cullen K, Clarke J, Irvin E, Sinclair S, Frank J. Workplace-based return-to-work interventions: A systematic review of the quantitative literature. J Occup Rehabil 2005;15(4):607–631.
Navarro V, Shi L. The political context of social inequalities and health. Soc Sci Med 2001;52(3):481–491.
Östlin P. Gender inequalities in health: The significance of work. In: Wamala SP, Lynch J, ed. Gender and social inequities in health. Lund: Studentlitteratur, 2002, pp. 43–65.
Vahtera J, Kivimäki M, Pentti J, Theorell T. Effect of change in the psychosocial work environment on sickness absence: A seven year follow up of initially healthy employees. J Epidemiol Community Health 2000;54(7):484–493.
Vahtera J, Kivimaki M, Pentti J. Effect of organisational downsizing on health of employees. Lancet 1997;350(9085):1124–1128.
Bourbonnais R, Mondor M. Job strain and sickness absence among nurses in the province of Quebec. Am J Ind Med 2001;39(2):194–202.
North FM, Syme SL, Feeney A, Shipley M, Marmot M. Psychosocial work environment and sickness absence among British civil servants: The Whitehall II study. Am J Public Health 1996;86(3):332–340.
Voss M, Floderus B, Diderichsen F. Physical, psychosocial, and organisational factors relative to sickness absence: A study based on Sweden Post. Occup Environ Med 2001;58(3):178–184.
Voss M, Floderus B, Diderichsen F. How do job characteristics, family situation, domestic work, and lifestyle factors relate to sickness absence? A study based on Sweden Post. J Occup Environ Med 2004;46(11):1134–1143.
Vingard E, Lindberg P, Josephson M, Voss M, Heijbel B, Alfredsson L, et al. Long-term sick-listing among women in the public sector and its associations with age, social situation, lifestyle, and work factors: A three-year follow-up study. Scand J Public Health 2005;33(5):370–375.
North F, Syme SL, Feeney A, Head J, Shipley MJ, Marmot MG. Explaining socioeconomic differences in sickness absence: The Whitehall II Study. BMJ 1993;306(6874):361–366.
Ostlund G, Cedersund E, Hensing G, Alexanderson K. Domestic strain: A hindrance in rehabilitation? Scand J Caring Sci 2004;18(1):49–56.
Lundberg U, Mårdberg B, Frankenhaeuser M. The total workload of male and female white collar workers as related to age, occupational level, and number of children. Scand J Psychol 1994;35(4):315–327.
Hensing G, Alexanderson K. The relation of adult experience of domestic harassment, violence and sexual abuse to health and sickness absence. Int J Behav Med 2000;7:1–18.
Pollock N. Client-centered assessment. Am J Occup Ther 1993;47(4):298–301.
Wressle E, Eeg-Olofsson AM, Marcusson J, Henriksson C. Improved client participation in the rehabilitation process using a client-centred goal formulation structure. J Rehabil Med 2002;34(1):5–11.
Riksförsäkringsverket. Långtidssjukskrivna – diagnos, yrke, partiell sjukskrivning och återgång i arbete (Long-term sick-listed – diagnoses, occupation, partial sick-listing and return to work). Stockholm: Riksförsäkringsverket, 2004. Report No.: 2004:7. (In Swedish.)
Dunn W, Brown C, McGuigan A. The ecology of human performance: A framework for considering the effect of context. Am J Occup Ther 1994;48(7):595–607.
Law M, Cooper BA, Strong S, Stewart D, Rigby P, Letts L. The Person-Environment-Occupational Model: A transactive approach to occupational performance. Can J Occup Ther 1996;63(1):9–23.
Acknowledgments
This study was supported by the Primary Health Care in Gothenburg and by grants from the local Research and Development Council of Gothenburg and Southern Bohuslän. We thank Thorbjörn Jonsson for linguistic advice and illustration.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s10926-007-9080-5.
Rights and permissions
About this article
Cite this article
Holmgren, K., Ivanoff, S.D. Supervisors’ views on employer responsibility in the return to work process. A focus group study. J Occup Rehabil 17, 93–106 (2007). https://doi.org/10.1007/s10926-006-9041-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-006-9041-4