
Abstract
The use of conventional immobilization splints can cause a lot of mishaps and discomfort in patients. In addition, it is common the generation of muscle, joint and vascular complications arising from the application of classic restraint devices in this phase of treatment. Currently, it is being observed that these problems could be solved with the use of Advanced Manufacturing techniques based on Additive Manufacturing (AM), industrial digitalization and reverse engineering for the realization of individualized immobilization splints. The present study proposes to give these splints a functional character in their design adapting them to a specific pathology, in this case to the partial rupture of Achilles tendon. It also provides a comparison against the use of conventional plaster splints as an improvement factor for their definitive implementation considering the initial sanitary use for which they were designed. In this way, there have been created therapeutic windows that allow the application of rehabilitation techniques, being the treatment that would be carried out developed in parallel. The designed splint has been made in FilaFlex and Polycarbonate, materials that guarantee comfort and resistance at the same time. In addition, an optimization in terms of material has been executed, lightening the splint and reducing environmental impact and manufacturing costs. As a result of this preliminary study, a prototype on scale printed in PLA has been generated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Industry 4.0 is living and promoting the use of new techniques that allow to provide new applications and methodologies with concepts such as Advanced Manufacturing (AM) and Industrial Design. Significant results are being achieved in aspects such as the optimization of the design process [1, 2], reduction of manufacturing costs, materials’ development [3,4,5] and decrease of the environmental impact [6]. These advances are not simply limited to the industrial area, but also they are being transferred to areas such as Medicine with applications in Bioengineering [7].
Advanced Manufacturing, thanks to the use of different methods of Three-Dimensional Industrial Digitalization and Reverse Engineering has allowed a recent emergence of solutions based on additive manufacturing in the field of Medicine [8]. In fact, additive manufacturing is booming. It can be seen, for example, in the case of its substitute or complementary use to bones of cadavers for the study of anatomy because printed bones significantly meet the pedagogical objectives [9]. Given their interest, even within this same field there are very diverse utilities, such as the manufacture of oral appliance (OA) devices due to the need of making them customizable and adjustable to optimize their effects [10].
Orthopaedics and Rehabilitation are among this large number of Medicine specialties that may be conducive to technological developments in the field of R + D + i. In recent years there has been great progress in mass-use products such as splints, orthoses, prostheses or assistive devices combining efforts with other technical disciplines. At the same time, the applications of exoskeletons have been revolutionized by combining knowledge with robotic. These cases demonstrate the need for information to flow transversally. Orthopaedics and Rehabilitation are two highly demanded specialties that present a very significant turnover in developed countries because they belong to the Health sector [11]. However, the implementation and viability of all the novelties that arise in these fields also require a possible demand, to reach a minimum level of maturity and technological development, and a profitability that justifies both economically and technically the change of the proposed production model [12]. Products, such as splints, made by additive manufacturing offer great advantages over classic methods of assistance and permanent immobilization (plaster splints) or commercial methods (orthoses, corsets, etc.). These advantages can be resumed as follow: adaptation, customization, hygiene, materials or the environmental impact, among others. However, sometimes there are certain disturbances in the fused deposition that can affect the final quality of the product [13] and have drawbacks such as the initial investment and training or its manufacturing time [14]. At present, the technological development achieved allows to quickly overcome the aforementioned drawbacks. However, the definitive implantation of these splints requires other arguments of additional improvement, such as providing the splints with a functionality that considers the initial sanitary use for which they were conceived. This functionality was unthinkable to date because it is impossible its integration into traditional manufacturing methods and requires cooperation between different areas of knowledge such as engineering and medicine. Integration in the design of functional aspects represents a step forward in the provision of key decision factors in the implementation of this type of product. For all these reasons, this work has been oriented to the development of a functional splint that allows to begin the rehabilitation of partial rupture of Achilles tendon in the period of immobilization using Advanced Manufacturing methods.
The Achilles tendon is the common terminal tendon of three muscle heads that form the triceps surae (gastrocnemius or calf muscle and soleus) that attaches to the posterior part of the calcaneus. Of these three muscles, the soleus is the deepest, monoarticular and is originated simultaneously in the tibia and the fibula. The other two muscle heads are biarticular; the external calf muscle is originated above the external condyle of the femur and in the external condylar shell and the internal calf muscle does so in the internal femoral condyle and external condylar shell. These two origins form the lower “V” of the popliteal rhombus [15] (Fig. 1). At the origin, the tendinous tissue of the Achilles tendon is mixed with the muscle fibres and inserted into the posterior part of the calcaneus distal and medial third. It has the important function of elevating the heel, which is done by applying a tensile force to the calcaneus that is transmitted through an aponeurosis (plantar fascia) to the metatarsal heads of each of the fingers, giving the arrangement of the plantar arch. [16].

Anatomy of Achilles tendon
The Achilles tendon has a recognizable paratendon, an additional sheath called epitendon, which is a layer of lubricating synovial tissue. In addition, it has a cellular portion composed of fibroblasts that maintains the fibres and extracellular matrix, facilitating the metabolism of tissues, providing hydration, firmness, cushioning, flexibility and reducing friction [17, 18]. Some of the most frequent injuries in the Achilles tendon are: thickening of the peritoneum, periaquilian bursitis and partial intrasubstance ruptures or complete ruptures in the myotendinous junction with the triceps surae [19]. The Achilles tendon with gastrocnemius and soleus belong to the posterior muscle chain [20], perform the foot plantar flexion, elevate the heel in the standing position on the floor and participate in the stages of walking, jumping and running [21].
The rupture of the Achilles tendon is usually caused by a sudden distention of the tendon, when the triceps surae is contracted, by forced plantar flexion or in violent and sudden dorsiflexion of the foot [22] [23]. The triggering mechanisms are usually while practicing running and jumping sports and displacements with changes of direction. The incidence rate is greater in males from the 3rd and 4th decade of life, with excess weight or those who practice sports occasionally because the lack of physical activity favours tissue degeneration of the tendon [24].
The clinic is accompanied by the sign of whiplash, sharp pain of rapid progression, eventually with an audible clicking at the time of the rupture. It is also being noticed a loss of plantar flexion, the presence of the tendon gap at the rupture level (Fig. 2a) and foot drop when the patient lies prone with the ankles out of the stretcher (Fig. 2b). Thomson test: exerted pressure on the triceps muscle does not cause plantar flexion [25].

Thompson test, thickening of the tendon and “tennis leg” injury. Own image
Due to the reasons above described, the present study proposes to provide a splint with functional features in its initial design for rehabilitation of partial Achilles tendon. The objectives proposed to carry out the design of the functional splint are the following:
-
Programming of conservative treatment of rehabilitation of intrasubstance rupture of the Achilles tendon by immobilization, integrated in a functional splint designed by Advanced Manufacturing (AM) methods and comparison with the programming of the same case resolved by immobilization with a plaster splint.
-
Design of an individualized immobilization splint for lower limb (leg) with functional characteristics, as a decision factor for the implementation of the use of Advanced Manufacturing compared to conventional or 3D printed splints.
Methodology
The methodology followed for the 3D modelling of the splint is analogous to the immobilization of articulations of the upper limb such as the wrist [6]. However, in this case the splint has two materials instead of one: a flexible inner layer, FilaFlex, and a rigid outer, Polycarbonate. The goal pursued using FilaFlex is to improve user comfort. In addition, it will optimize the conformability to the leg, both in a first moment when the leg has a greater volume produced by the swelling, and once the swelling decreases. Polycarbonate on the outside guarantees the rigidity and resistance necessary for the immobilization. Below, the necessary steps for its creation are explained.
The process starts with a scan of the leg in order to achieve a design tailored to the user. The 3D Systems Sense® scanner is used to perform vertical sweeps 360 degrees around the leg (Fig. 3). The scan should be done keeping the leg in suspense because the detailed surface of the lower part of the leg and the foot is required. The digitization of the member is a fast step, but is one of the keys of the process.

3D scan with 3D Systems Sense®.
Once the file has been generated, it is imported from the 3D Systems Geomatic Design X® CAD (Computer Aided Design) program (Fig. 4). This program allows the transformation of the points cloud into a surface, the basis for the creation of the solid that constitutes the splint.

3D Systems Geomagic Design X® interface.
The surface is exported to Rhinoceros 5 CAD program, specialized in 3D object modelling. The surface is offset 1 mm (Fig. 5) to ensure a slight clearance and that the member is not pressed, ensuring greater comfort. Next, the surface is divided into two sections: upper, covering the leg and upper part of the foot, and lower, corresponding to the sole of the foot. This separation is motivated due to the sections will be manipulated differently. The upper section already presents its definitive structure. On the other hand, the lower section will be modified so as not to mould itself specifically to each of the fingers but to the sole of the foot as a whole.

Offset surface to allow clearance
With the separation made, the upper surface is offset 1.5 mm, this time as a solid. This solid will be the flexible material (FilaFlex). It is cut by using planes until the desired final shape is obtained (Fig. 6). Subsequently, the upper surface is offset again, in this case 2.5 mm as solid. This solid will be the rigid material (Polycarbonate). A similar procedure to the one made with the flexible solid is followed: the unnecessary area is trimmed (in this case the fingers part, because the will remain uncovered).

Upper flexible surface trimmed
Then, it is time to return to the lower surface (which is the support of the sole). In it, the part of the fingers is cut out and replaced by a curved surface that covers all of them at once and not individually (Fig. 7). The same process of offsets that was followed with the upper part is executed to create the sole as flexible and rigid solid.

Lower surface covering the fingers as a whole
Once the solid have been completed, it can be proceeded to the realization of the therapeutic windows. These windows allow to begin the rehabilitation techniques while the immobilization lasts (Fig. 19). They have the shape, position and dimensions that are specified in Fig. 8, which are those required by the proportions of the tissues to be treated and the devices with which the different treatments will be made. The electro medical devices used and considered for the design of the splint are from the Fisioline® brand (Mobile Module, OPAF, Fisiofield middle and laser LUMIX 3 Ultra).

Therapeutic windows to be made in the splint. Dimensions in mm [26]
A cover for the largest therapeutic window (60 × 120 mm) is created, which is the one that covers the wound (Fig. 9). Finally, the solid is divided into two halves and the closing buttons are placed.

Therapeutic window for the Achilles tendon area
Once the splint design is finished, it can be exported to Solid Thinking Inspire program for optimization. To generate the model, boundary conditions are established, design space is selected, forces are established and the load cases are generated (Fig. 10). The determination of these parameters is reinforced thanks to the study of different articles on leg orthoses:

Splint prepared for optimization
The first study covers the design of a KAFO (knee-ankle-foot orthosis) that helps to hold the leg supporting its weight [27]. From the second publication it is possible to obtain the maximum value that the leg must support in normal gait: 1.5 times the weight of the user [28]. Finally, the most extensive article and also the one of greater interest is the one of Ilzarbe [29]. In this study it is argued that for normal gait only forces occurring in the sagittal plane are considered and provide a more in-depth study of the phases of gait.
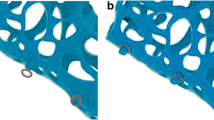
By means of the optimization process, it is obtained with precision where it is necessary to have material to support the efforts to which the splint can be exposed and in which parts it is dispensable (Fig. 11). This reduction of material causes a lightening of the splint and a decrease not only in the cost of the material but also in the printing process by reducing time and in the rehabilitation by losing a smaller amount of muscle mass linked to this lightening.

Result of the optimization
Knowing the areas where material is not required, it can be proceeding to make the different apertures that allow to continue identifying the rehabilitation windows while removing material (Fig. 12).

Creation of optimization apertures
With the optimization completed, the model can be prepared for printing, by selecting aspects such as position, temperature depending on the material, density or thickness (Table 1). After this step it can be proceeding to the manufacture. For this study, a prototype in PLA has been made in order to verify the feasibility and strength of the design (Fig. 13). The leg has also been printed to check its adjustment.

Part of the splint ready for printing
Results
Design of the functional splint
A splint that consists of 4 pieces is obtained (Fig. 14): an interior one of FilaFlex and three externals of Polycarbonate. Two of the externals constitute the body of the splint and the other one is a removable cover of one of the treatment windows.

Parts of the splint: a) flexible solid b) rigid solid part 1 c) rigid solid part 2 d) cover
For attaching the cover, the splint has buttons divided between the two pieces that are joined by an elastic band (Fig. 15). The join, between the two rigid parts of the body, is carried out through rails fitting one part of the splint in the other. To ensure its attachment, it is secured with two buttons, like those on the cover, on the upper part. The result of the assembled splint is shown in Fig. 16.

Closing button

Design of the splint for individual leg immobilization: a) top-side view b) rear view c) side view d) top view e) bottom view
Figure 17 shows images of the prototype printing on scale.

Prototype 3D printed in PLA
Discussions
The change of the proposed production model for the lower limb immobilization splints based on Advanced Manufacturing (AM) technique requires a study of establishment and feasibility based on a possible demand, at a minimum level of technological development and maturation, and in a profitability that justifies it economically and technically. Once the technological feasibility described in the previously developed methodology has been solved, and to highlight the improvements made in terms of adaptation, personalization, hygiene, materials used or environmental impact, among others, it is interesting to provide a comparative case study between the two systems of manufacturing that takes into account the initial sanitary use for which they were designed, as a key decision factor in the implementation of this type of product. Consecutively, is a comparison between the programming of conservative rehabilitation treatment by immobilization of intrasubstance rupture of the Achilles tendon, integrated in a functional splint designed by Advanced Manufacturing (AM) methods, and the programming of the same case solved by classical immobilization by a plaster splint.
The programming of a conventional rehabilitation treatment for intrasubstance rupture of the Achilles tendon by a plaster immobilization consists initially in the immobilization with plaster of the foot and leg up to the knee. The programming of this treatment is shown in the scheme of Fig. 18 and is divided into three stages: keeping the cast for at least a month, two weeks of partial standing with crutches while rehabilitation begins and from week 7 the patient begins to walk, continuing with treatment until week 12. This method has the disadvantage that it does not allow performing physiotherapy techniques until the immobilization is removed.

Chronogram of the conservative rehabilitation program with immobilization by plaster splint
The programming of the same treatment by immobilization with functional splint is shown in Fig. 19 and consists of the same three stages. In it, the physiotherapeutic treatment begins as soon as the injury is caused by applying cold, magnetic and compression bandages during the first week while the splint is designed and manufactured. Since the second week, the patient will wear it until the first month is reached, but still wearing immobilization it will be proceed to continue with all rehabilitation techniques: drainage techniques, US (with and without contact), laser, iontophoresis and electrostimulation. This is possible through the therapeutic window system that has the splint and that are designed to apply the treatment without removing it. Both the second period of partial standing with crutches and the third in which the patient can already walk continues with other therapies such as kinesitherapy, proprioception and massage until week 8.

Chronogram of the conservative rehabilitation program with immobilization by functional splint
The most notable characteristics are the following:
-
The treatment estimates a duration of 8 weeks including functional readjustment. Weeks 1 to 4 will be without standing, week 5 with assisted support with crutches, and week 6 through 8 with autonomous support.
-
The first week of the treatment, the convenient diagnostic tests will be effected, an immobilization by a compressive bandage will be conducted, and the design and manufacture of the functional splint will be proceeded, adapted to the requirements of the rehabilitation techniques used.
-
A frequency of 5 rehabilitation sessions is scheduled in the weeks in which physiotherapy or retraining treatment is applied (weeks 2 to 8).
Through this system, the duration of the injury is markedly reduced due to the immediate application of all the therapy necessary while the ankle remains immobilized.
The proposed rehabilitation techniques are described below:
-
Cryotherapy: Anti-inflammatory effect of cold. Application in the splint windows.
-
Lymphatic drainage. Device: Module Mobile de Fisioline [30]. A drain is performed with a balanced symmetric square wave with 7 channels or sectors operating with Vodder sequence (program 16). The incidence in the designed splint will be the one shown in the drainage sectors 2 and 3, while the drainage area 1 is located above the splint (Fig. 20).
-
Sonotherapy (US). Improves the elasticity of tissues, mechanical, antalgic and circulatory effect. Device: OPAF of Fisioline [31].
Treatment: applied underwater by introducing the area to be treated in the water, sliding the head at 1 or 2 cm from the skin, producing a less concentrated massage in the area of the injury. Dosage: Continuous, 100%, 2 W/cm2, 1200 J/cm2, 10 min. The splint requires the design of a therapeutic window in the area affected by the injury. The evacuation of the water and apertures for drying by dryer will be carried out through the whole set of apertures made.
-
Magnetotherapy. Improvement of tissue permeability enhancing the effect of other combined techniques. Fisiofield middle device by Fisioline [32]. Treatment: Prog. 4 on muscle 2 weeks (antalgic), 30 min. In the successive sessions, Prog. 48 on tendon, 30 min. It does not require therapeutic windows on the splint.
-
Laser therapy: accelerates energy metabolism and tissue synthesis [33]. LUMIX 3 Ultra device of Fisioline class I type B [34], head of 9 collimated diodes (6 pulsed and super pulsed, 2 continuous and 1 guide light) and diameter of 30 mm. Infrared sources of Laser GaAs between 780 and 905 nm. Treatment: weeks 2 to 5.
-
Iontophoresis: Improvement of tissue permeability and application of anti-inflammatory and antalgic drugs. Device: Physioline Mobile Module. Treatment: Drug: Indomethacin (−) application on the cathode, dose: 1 cm3 for 5 cm2 of chamois, time: 10–15 min according to skin tolerance [35]. The cathode is applied in the window of the affected area and the anode requires a specific hole in the anterior part of the splint as shown in Fig. 8.

Areas to perform drainage treatment using electrodes. Manual Fisioline
Muscular electrostimulation electrotherapy
TENS in gastrocnemius muscle (antalgic and anti-inflammatory effect), low frequency analgesic currents and faradic currents (retardation of muscle atrophy in calf muscle) and stimulating currents in gastrocnemius and intrinsic muscles of the sole (motor responses, avoiding Sudeck processes) [35]. It is applied with 50 × 50 mm electrodes on therapeutic windows made on the splint according to Fig. 8.
In the comparison between the two programs shown, a shortening of 4 weeks can be observed in the rehabilitation period due to the advancement of the application of physiotherapy techniques applicable in the immobilization stage. This shortening involves at least 30% of the treatment period.
On the other hand, the application of physiotherapy techniques since the immobilization phase contributes to the prevention of muscular, joint and vascular complications derived from the application of retention devices in this phase of treatment:
The results obtained from the functional immobilization splint for partial rupture of the Achilles tendon have integrated the necessary apertures and accesses for the application of the different physiotherapy techniques proposed and described previously. Fig. 15 schematically shows the size, shape and position of the apertures required (Fig. 8) and realized.
The use of functional splints provides both the advantages of the use of classic splints of immobilization by additive manufacturing to the initial sanitary use for which they were designed. Among others, it can be highlighted the hygienic, skin, visual control of the evolution of the lesion or environmental problems [6].
The integration of various types of functionality to a splint created by Advanced Manufacturing methods contributes to provide an added value that can be a key decision factor for its implementation.
There is the possibility of designing functional splints for home use for the application of some ambulatory rehabilitation techniques applicable in the immobilization phase that avoid the frequent journey of the patient to hospital centres. This requires a design of the own splint by the specialists, and a specific development of medical devices adapted to a user-patient.
Conclusions
The objective of this work is the study, design and manufacture of a functional splint for partial rupture of the Achilles tendon. The state of the technology allows the realization of individualized immobilization splints by Advanced Manufacturing techniques based on additive manufacturing, industrial digitalization and reverse engineering.
The treatment of conservative rehabilitation of intrasubstance rupture of the Achilles tendon by functional splint of individualized immobilization made by additive manufacturing, allows the integration of the necessary elements and accessories to allow the application of physiotherapy techniques in this stage.
The application of physiotherapeutic techniques in the immobilization stage allows the prevention of possible muscular, articular, cutaneous and vascular complications derived from the application of the classic retention devices in this phase of the treatment.
The advantages or improvements applied in the immobilization stage thanks to the use of functional splints made by Advanced Manufacturing techniques can be summarized in two groups: the control measures and continuous monitoring and the active techniques of the field of physiotherapy.
As control and monitoring measures, it is necessary to emphasize the visual control of the state of the injured area, the control of appearance of inflammatory, vascular and neurological alterations (effusions, Sudeck’s disease), or dermatological control of the area affected by the immobilization (pruritus, eschar).
The applicable physiotherapeutic techniques thanks to their integration in the design of the functional splints are aimed at the substantial reduction of the deterioration associated with the period of immobilization of the lesion. In this way problems such as inflammation, pain, problems of the venous and lymphatic circulatory system or loss and atrophy of muscle mass are prevented, mitigated or avoided.
The use of functional immobilization splints in the immobilization process under study allows a shortening of at least 30% of the treatment period compared to the use of plaster splints.
Consequently, the improvements brought about using individualized immobilization splints by Advanced Manufacturing techniques based on additive manufacturing in the treatment of conservative rehabilitation of intrasubstance rupture of the Achilles tendon should allow the beginning of a functional readjustment phase with favourable muscular and articulations conditions and achieve the shortening of the rehabilitation period and the total duration of the treatment.
References
D’Amato, R., Calvo, R., and Gómez, E., Sensitivity study of the morphometric fitting on the pressure field inside ankle joints. Case Stud Mech Syst Signal Process 1:8–14, 2015. https://doi.org/10.1016/j.csmssp.2015.04.001.
D’Amato, R., Calvo, R., Ruggiero, A., and Gómez, E., Measurement capabilities for ball bearing wear assessment. Procedia Manuf 13:647–654, 2017. https://doi.org/10.1016/j.promfg.2017.09.136.
Ruggiero, A., D’Amato, R., and Gómez, E., Experimental analysis of tribological behavior of UHMWPE against AISI420C and against TiAl6V4 alloy under dry and lubricated conditions. Tribol Int 92:154–161, 2015. https://doi.org/10.1016/j.triboint.2015.06.005.
Ruggiero, A., D’Amato, R., Gómez, E., and Merola, M., Experimental comparison on tribological pairs UHMWPE/TIAL6V4 alloy, UHMWPE/AISI316L austenitic stainless and UHMWPE/AL2O3ceramic, under dry and lubricated conditions. Tribol Int 96:349–360, 2016. https://doi.org/10.1016/j.triboint.2015.12.041.
Valášek, P., D’Amato, R., Müller, M., and Ruggiero, A., Musa textilis cellulose Fibres in biocomposites – An investigation of mechanical properties and microstructure. BioResources 13:3177–3194, 2018.
Blaya, F., Pedro, P. S., Silva, J. L., D’Amato, R., Heras, E. S., and Juanes, J. A., Design of an Orthopedic Product by using additive manufacturing technology: The arm splint. J Med Syst:42, 2018. https://doi.org/10.1007/s10916-018-0909-6.
Affatato, S., Ruggiero, A., De Mattia, J. S., and Taddei, P., Does metal transfer affect the tribological behaviour of femoral heads? Roughness and phase transformation analyses on retrieved zirconia and biolox® Delta composites. Compos Part B Eng 92:290–298, 2016. https://doi.org/10.1016/j.compositesb.2016.02.020.
Kelly S, Paterson A, Bibb RJ (2015) A review of wrist splint designs for additive manufacture. Rapid Des Prototyp Manuf Conf
Lozano, M. T. U, D’Amato, R., Ruggiero, A., Manzoor, S., Haro, F. B., Méndez, J. A. J,. A study evaluating the level of satisfaction of the students of health sciences about the use of 3D printed bone models. In: Proceedings of the Sixth International Conference on Technological Ecosystems for Enhancing Multiculturality - TEEM’18. ACM Press, New York, New York, USA, pp 368–372, 2018
García, N. M., Blaya, F., Urquijo, E. L., Haro, F. B., Soriano Heras, E., D’Amato, R., García, N. M., Blaya, F., Urquijo, E. L., Soriano Heras, E., D’Amato, R.,Study, Design and Prototyping of Oral Appliances to Treat Obstructive Sleep Apnea. Proc Sixth Int Conf Technol Ecosyst Enhancing Multicult - TEEM’18 416–421, 2018. doi: https://doi.org/10.1145/3284179.3284250.
Evill, J. Cortex. http://www.evilldesign.com/cortex. Accessed 13 Jun 2018
Emelogu, A., Marufuzzaman, M., Thompson, S. M., Shamsaei, N., and Bian, L., Additive manufacturing of biomedical implants: A feasibility assessment via supply-chain cost analysis. Addit Manuf 11:97–113, 2016. https://doi.org/10.1016/J.ADDMA.2016.04.006.
Haro, F. B., de Agustín del Burgo, J. M., D’Amato, R., Marcos, M. I., Heras, E. S., Alonso, J. M. G., Monitoring of the additive manufacturing process for the use of biomaterials in medical field. In: Proceedings of the Sixth International Conference on Technological Ecosystems for Enhancing Multiculturality - TEEM’18. ACM Press, New York, New York, USA, pp 428–432, 2018.
Paterson, A. M., Bibb, R., Campbell, R. I., and Bingham, G., Comparing additive manufacturing technologies for customised wrist splints. Rapid Prototyp J 21:230–243, 2015. https://doi.org/10.1108/RPJ-10-2013-0099.
Viel, E., La marcha humana, la carrera y el salto: Biomecánica, exploraciones, normas y alteraciones. 59–60, 2002.
Kapandji, A., Fisiología Articular, Tomo 2: Miembro Inferior, 6a Edición. Editorial Medica Panamericana S.A., 2012.
Wren, T. A., Yerby, S. A., Beaupré, G. S., and Carter, D. R., Mechanical properties of the human achilles tendon. Clin Biomech 16:245–251, 2001. https://doi.org/10.1016/S0268-0033(00)00089-9.
Kannus, P., Structure of the tendon connective tissue. Scand J Med Sci Sport 10:312–320, 2000. https://doi.org/10.1034/j.1600-0838.2000.010006312.x.
Claudia Astudillo, A., Indicaciones del ultrasonido musculoesquelético diagnóstico. Rev Médica Clínica Las Condes 24:88–97, 2013. https://doi.org/10.1016/S0716-8640(13)70133-0.
Busquet, L., Urrits, C. (1994) Las cadenas musculares. Paidotribo.
Elvira JLL. V-GFJ. MM. GJA. Motricidad : European Journal of Human Movement. Asociación Española de Ciencias del Deporte, 2008.
Zaragoza-Velasco, K., Fernández-Tapia, S. Ligamentos y tendones del tobillo: anatomía y afecciones más frecuentes analizadas mediante resonancia magnética. In: Anales de radiología México. pp 81–94, 2013.
Romero-Barajas, A., Ventura-Ríos, L., Pineda, C., and Hernández-Diaz, C., Tendón de Aquiles y su Estudio Ultrasonográfi-co; Más Allá de sus Alteraciones Inflamatorias. Rev chil Reum 30:122–127, 2014.
Lantto, I., Heikkinen, J., Flinkkilä, T., Ohtonen, P., and Leppilahti, J., Epidemiology of Achilles tendon ruptures: Increasing incidence over a 33-year period. Scand J Med Sci Sports 25:e133–e138, 2015. https://doi.org/10.1111/sms.12253.
Heim, U., Baltensweiler, J., Guía de traumatología, Segunda ed. Thieme, Barcelona, 1988..
Anatomy Learning - 3D Atlas.
Muñoz, A., Pelliccioni, O., C M-K Diseño Y Construcción de un Prototipo dE Bitutor Largo de Tipo Kafo Termoconformado.
Jose, O., Monrroy, P., Candal, M. V., Mechanical evaluation of a designed plastic modular system of knee- ankle-foot orthotics for children Congreso Internacional de Métodos Numéricos en Ingeniería y Ciencias Aplicadas CIMENICS 2016 View project Computational Biofluid Dynamic of a mechanical, 2016.
EB Projecte Final d’Estudis Màster en Enginyeria Biomèdica Análisis Dinámico de las Fuerzas de Contacto Ortesis- Pierna Mediante un Modelo Biomecánico Tridimensional, 2014.
Modulo Medical 4. http://www.fisioline.com/es/estimuladores-neuromusculares/modulo-medical-4.html. Accessed 19 Oct 2018
Una Acción Focalizada Profundidad De Alta Potencia PE ONDAS DE PRESIÓN DE ALTA FRECUENCIA.
F I S I O F I E L D M I D D L E.
Heras, E. S., D’Amato, R., Marcos, M. I., de Agustín del Burgo, J. M., Haro, F. B., Alonso, J. M. G,. Monitoring of the additive manufacturing process for the use of biomaterials in medical field. ACM, pp 428–432, 2018.
LUMIX ® Plus y LUMIX ®.
Rodríguez Martín, J. M., Electroterapia en fisioterapia. Editorial Médica Panamericana, 2014.
Acknowledgments
The authors gratefully acknowledge the company Trimédica S.L. (http://www.trimedica.es/) and the manufacturer of electromedical devices fisioline (http://www.fisioline.com/es/home-medical-es.html) for their assignment of all the required electromedical equipment in the present research work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Fernando Blaya Haro declares that he has no conflict of interest. Pilar San Pedro declares that he has no conflict of interest. Alonso Blaya San Pedro declares that he has no conflict of interest. Julia Lopez-Silva declares that he has no conflict of interest. Juan A. Juanes declares that he has no conflict of interest. Roberto D’Amato declares that he has no conflict of interest. Manuel Islán declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. This article does not contain any studies with animals performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Education & Training
Rights and permissions
About this article

Cite this article
Blaya, F., Pedro, P.S., Pedro, A.B.S. et al. Design of a Functional Splint for Rehabilitation of Achilles Tendon Injury Using Advanced Manufacturing (AM) Techniques. Implementation Study. J Med Syst 43, 122 (2019). https://doi.org/10.1007/s10916-019-1247-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-019-1247-z