
Abstract
Slowing down the progression of chronic kidney disease (CKD) and its adverse health outcomes requires the patient’s self-management and attention to treatment recommendations. Information technology (IT)–based interventions are increasingly being used to support self-management in patients with chronic diseases such as CKD. We conducted a systematic review of randomized controlled trials (RCTs) to assess the features and effects of IT-based interventions on self-management outcomes of CKD patients. A comprehensive search was conducted in Medline, Scopus, and the Cochrane Library to identify relevant papers that were published until May 2016. RCT Studies that assessed at least one automated IT tool in patients with CKD stages 1 to 5, and reported at least one self-management outcome were included. Studies were appraised for quality using the Cochrane Risk of Bias assessment tool. Out of 12,215 papers retrieved, eight study met the inclusion criteria. Interventions were delivered via smartphones/personal digital assistants (PDAs) (three studies), wearable devices (three studies), computerized systems (one study), and multiple component (one study). The studies assessed 15 outcomes, including eight clinical outcomes and seven process of care outcomes. In 12 (80%) of the 15 outcomes, the studies had revealed the effects of the interventions as statistically significant positive. These positive effects were observed in 75% of the clinical outcomes and 86% of the process of care outcomes. The evidence indicates the potential of IT-based interventions (i.e. smartphones/PDAs, wearable devices, and computerized systems) in self-management outcomes (clinical and process of care outcomes) of CKD patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic Kidney Disease (CKD) is a prolonged and debilitating disease that currently affects 13.4% of the population worldwide [1]. In most cases, this disease has comorbid chronic conditions or multi-morbidities such as diabetes, hypertension and cardiovascular diseases, which add to the complexity of the treatment process [2, 3]. The poor care of CKD leads to kidney failure, which requires costly treatments such as dialysis or transplant and is known to be one of the expensive contemporary diseases [4].
Slowing down the progression of CKD and its adverse health outcomes requires the patient’s self-management and attention to complex treatment recommendations such as blood sugar and blood pressure (BP) monitoring, maintaining physical activity, changing nutrition patterns, and adherence to medication regimens [5]. Self-management interventions in CKD patients have led to positive outcomes such as improvement in symptoms and complications, enhanced self-care knowledge, ability and behavior, improved health-related quality of life (HRQOL), time to initiation of renal replacement therapy (RRT) and survival after RRT [6,7,8,9,10]. Studies have been indicative of a poor self-management in CKD patients and non-adherence to treatment recommendations, as a result of which adverse clinical outcomes tend to be very common in these patients [11, 12] and which make the successful treatment of CKD patients a rather challenging task.
Recent years have witnessed an increase in the use of information technology (IT) for supporting self-management in patients with chronic diseases [13]. Evidence from a literature review suggests that IT-based interventions help improve self-management outcomes, including clinical outcomes, by improving the access to health information and aiding communication with healthcare providers in patients with chronic diseases [14,15,16,17,18].
Many interventional studies have been conducted to date to assess the use of IT tools to improve self-management in CKD patients and some have found this intervention to be effective [19,20,21] and some have not shown positive results [22]. This disparity of results demonstrates the need for a systematic review study to combine the results of the available studies. To the best of our knowledge so far, only two systematic review studies have assessed the effect of IT-based interventions on self-management in CKD patients [23, 24]. The systematic review study by Campbell and Porter limited itself to interventions based on dietary mobile applications and their lack of effect on nutritional indicators in CKD patients [23]. In a meta-analysis, He et al. argued that IT tools such as short message service (SMS), video conferencing, and telephonic contact have significantly reduced hospital readmissions, emergency room visits and number of days in the hospital and improved the HRQOL in CKD patients [24].
Although IT-based interventions have the potential to improve self-management in patients, the need for the direct involvement of providers in non-automated IT-based interventions, such as telephonic contact, can create new challenges, such as human errors, in the use of these interventions. Due to the lack of direct human involvement, the incidence of error is unlikely in automated IT-based interventions (e.g. automated SMS and automated telephone communication systems (ATCS)). None of the systematic review studies conducted on self-management in CKD patients have focused on automated IT tools. The present study therefore aims to integrate the results of published studies on the effects of automated IT-based interventions with patients as the consumers on the outcomes of self-management in CKD patients. The questions raised on this subjected include: What types of interventions have been evaluated in this field? What were their features? What effects did these interventions have on the outcomes of self-management in CKD patients?
Methods
The present systematic review was conducted and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) proposed by Moher et al. [25].
Data sources and search strategies
A comprehensive search was conducted in Medline (through PubMed), Scopus, and the Cochrane Central Register of Controlled Trials (Cochrane) to identify relevant studies published until May 2016. The search strategy included a combination of keywords and MeSH terms related to IT (such as information technology, internet, and monitoring systems) and also kidney disease (such as kidney disease, dialysis, and kidney transplant). Table 1 presents the complete list of the keywords and phrases used in the search.
Eligibility criteria
The selection criteria were determined according to the population, intervention, comparator, outcomes, and study design (PICOS) format. Automated IT tools are IT tools with automated capabilities and without the direct involvement of the human. The study inclusion criteria were: (1) IT-based interventions in patients with CKD stages 1 to 5; (2) Interventions with all kinds of IT-based tools, such as a smart phone, tablet, smart TV or computer, that support all or part of the intervention consisting of the self-management; (3) The study design being a randomized controlled trial (RCT); (4) Having a control group receiving standard/usual care without IT-based systems.
The study exclusion criteria were: (1) Studies in which healthcare providers were the consumers of the intervention; (2) Studies with the IT-based intervention performed only through the direct involvement of healthcare providers (such as telephonic contact, non-automated SMS and email, and video conferencing systems); (3) Studies focused on the feasibility, validity, acceptability, or description of IT-based tools and systems; (4) Descriptive studies without comparison group, case reports, commentaries, reviews, study protocols, surveys, conference proceedings, and before-after trials. No language limitations were imposed on the studies.
Data extraction
The two reviewers independently screened the titles and abstracts of all the articles identified through the electronic search. The full-text of any articles deemed potentially relevant according to one of the two reviewer was retrieved and assessed for final inclusion. Differences of opinion regarding the relevance of the articles were resolved through discussion. Once the articles were finalized, a specific spreadsheet was prepared for the systematic extraction of data from the studies. The data extracted included the authors’ name, date of the study, country and number of participants, technology type, technology functionality, technology description, duration of the intervention, outcomes, and findings. Data were extracted by the first reviewer and then the second reviewer checked and verified them in terms of accuracy and identified any missing information.
Risk of bias in the included studies
To assess the risk of bias in the included studies, Cochrane Collaboration’s assessment tool, which recommends the assessment of six specific domains, was used [26]. Of these domains, sequence generation and allocation concealment are meant to prevent selection bias, blinding of participants and personnel to prevent performance bias, blinding of outcome assessment to prevent detection bias, incomplete outcome data to prevent attrition bias and selective outcome reporting to prevent reporting bias.
Data synthesis and analyses
No meta-analysis was performed because of the variability and heterogeneity of the outcomes and interventions. A narrative synthesis was carried out based on the classification of the outcomes and the intervention type and effect. Outcomes were classified into two categories: clinical outcomes and process of care outcomes. Clinical outcomes indicate the severity of the disease, such as BP [27]. Process of care outcomes affect the patient by improving the provision of healthcare or the patient-healthcare provider interactions [27]. According to a study conducted by Vegesna et al. [28], the interventions were classified as follows:
-
Smartphones or personal digital assistant devices (PDAs) (software/application/SMS) used to transfer data to the healthcare providers/researchers.
-
Wearable devices: devices worn or placed to part of the body to record specific physiological changes (such as monitoring BP).
-
Computerized systems: systems in which data are entered by the patient through the internet or are given to the patient by this means.
-
Multiple components: containing more than one technology category above (for example, wearable devices and smartphones)
The IT functionalities were classified based on the technology functionality framework [29, 30] shown in Table 2.
The effect of the intervention was classified according to one of the following cases: statistically significant positive, positive without statistical argument, no effect (not statistically significant), and mixed effect (both positive and without an effect).
Results
Study selection
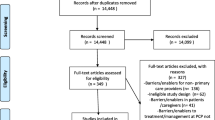
As shown in Fig.1, 15,504 records were identified from the search conducted in Medline, Scopus and Cochrane databases. After the elimination of the repetitive records, 12,215 single records remained. After assessing the titles and abstracts according to the inclusion and exclusion criteria, 30 papers were selected for full text assessment, 22 of which were later excluded based on the exclusion criteria, leaving eight papers that matched the specified criteria of the study.

Flow diagram of the literature search and study selection
General characteristics of the included studies
Table 3 presents the general characteristics of the included studies. The eight papers included in the review reported on eight separate studies and were published in English. The oldest article had been published in 2012 and the latest in 2016. The studies included five from the United States [22, 31, 32, 34, 35] and one each from Germany [33], Belgium [19] and the the United Kingdom [20]. Three studies were on hemodialysis patients [19, 22, 33], two on kidney transplant patients [31, 34], and the rest on CKD patients with different stages 1 to 5 [20, 32, 35]. The median number of participants in the studies was 150 (range, 22–488 participants), and the median duration of the studies was 10 months (range, three weeks to 12 months). The majority of the studies (5/8, 62.5%) had examined more than one outcome.
Risk of bias assessment
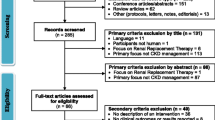
The results of the quality assessment of the studies are shown in Fig. 2. Half of the studies (50%) had specifically reported on their allocation sequence generation and allocation sequence concealment. Only 12.5% of the studies had reported adequate information about the blinding of the participants and the personnel and the outcome assessment. The amount and causes of attrition were reported in all the studies, considering that sample loss was less than 20% in all of them. The reviewed studies had little bias in terms of incomplete outcome data. In studies with a registration number, selective reporting was assessed based on the match between the predetermined outcomes and the reported outcomes, and 62.5% of the studies had a low selective reporting bias.

Risk of bias assessment of the included studies
Effects of the interventions on the outcomes
Table 4 shows the effects of the interventions on the outcomes in the included studies. The studies assessed 15 outcomes overall, including eight clinical outcomes and seven process of care outcomes. In 12 (80%) of the 15 outcomes, the studies had revealed the effects of the interventions as statistically significant positive. In one study (6.7%), no significant differences were reported between the intervention and control groups, and in two studies (13.3%), there was a mixed effect (both positive and without an effect).
Clinical outcomes
The clinical outcomes associated with CKD assessed in these studies were BP (four studies), average daily interdialytic weight gain [IDWGA] (two studies), intact parathyroid hormone [iPTH] (one study), and ultrafiltration rate (one study). Overall, the effect of IT-based interventions was reported as statistically significant positive in six (75%) of the clinical outcomes, while in one case (12.5%), no significant difference was reported between the intervention and control groups, and in one case (12.5%), a mixed effect was reported.
Four of the included studies had assessed the effects of IT-based interventions on BP, which had the highest frequency compared to the other clinical outcomes. Two studies found a statistically significant positive effect for wearable devices on BP [32, 35] and one study found a statistically significant positive effect of multicomponent interventions (BP monitoring device, electronic medication tray and text messages [34]) on BP. In another study, wearable devices had a mixed effect on BP [33].
Two studies examined the effect of IT-based interventions on IDWGA; one was conducted on hemodialysis patients and found that wearable devices had a statistically significant positive effect on IDWGA [33]. In contrast, the other study using PDA to provide nutrition guideline had no statistically significant effects on IDWGA [22].
As for the other clinical outcomes, electronic medication event monitoring systems were found to have a positive effect on iPTH control in hemodialysis patients [19]. In another study, wearable devices had a positive effect on ultrafiltration rate in hemodialysis patients [33].
Process of care outcomes
The process of care outcomes that assessed in the reviewed studies were medication adherence (two studies), patients’ knowledge (one study), medication dose (one study), medication usage (one study), BP reading (one study) and dietary sodium intake (one study). Overall, the effects of IT-based interventions on process of care outcomes were reported as statistically significant positive in six cases (86%) and a mixed effect was reported in one case (14%).
Two of the included studies reported the effect of IT-based interventions on medication adherence as statistically significant positive, including one study on the positive effects of multicomponent interventions (BP monitoring device, electronic medication tray and text messages) in kidney transplant patients [34] and another on the positive effects of electronic medication event monitoring system on adherence to cinacalcet in hemodialysis patients [19].
Regarding the other process of care outcomes, one study showed that access to website had a statistically significant positive effect on the knowledge score in kidney transplant candidates and their family members in the intervention group compared to the controls [31]. Another study showed that electronic medication event monitoring systems had a statistically significant positive effect on reducing the dose of cinacalcet in hemodialysis patients [19]. Another study showed that SMS have a positive effect on BP reading and medication usage in CKD patients in stages 3–5 [20]. Another study conducted on hemodialysis patients reported a mixed effect for PDA on dietary sodium intake [22].
Classification of the interventions according to technology type and features (Table 5)
Three studies evaluated the effect of smartphone/PDA interventions using software programs [22], SMSs [20], and electronic medication event monitoring systems [19]. Smartphone/PDA functionalities included inform, record, display, communicate, remind/alert and guide. The effect of smartphones/PDAs was positive on five out of the seven outcomes assessed.
Three studies assessed the effects of wearable devices and their functionalities, including record, display, communicate and alert. These studies found wearable devices to positively affect four of the five outcomes assessed.
Another study assessed the effect of the inform functionality of a health information website [31] in kidney transplant candidates and their family members and reported positive effects on the one outcome assessed.
Only one study had evaluated the effect of multicomponent interventions [34], which used wearable devices in combination with SMS and offered functionalities including remind/alert and communicate. The effect of using this multicomponent intervention was reported as positive on both outcomes.
None of the reviewed studies had evaluated effects of personal health record (PHR) on self- management of CKD patients.
Discussion
This systematic review combined the results of RCTs that evaluated the effect of IT-based interventions on self-management outcomes in CKD patients. The results (eight studies, 1637 patients) showed that IT-based interventions had improved self-management outcomes in CKD patients in the majority of the studies. The self-management outcomes investigated were statistically significant positive in 80% of the studies. This positive effect was observed in 75% of the clinical outcomes and 86% of the process of care outcomes. The included studies had evaluated the effect of smartphones/PDAs, wearable devices, computerized systems, and multicomponent interventions.
The present findings revealed the positive effect of IT-based interventions on clinical outcomes in CKD patients, which agrees with the results of several other systematic reviews conducted on the effect of IT-based interventions on clinical outcomes in chronic diseases [14,15,16,17,18, 36, 37]. It can therefore be concluded that IT-based tools provide appropriate interventions for controlling clinical outcomes in chronic patients. In the present study, BP was the clinical outcome most frequently assessed in CKD patients, which showed improvements in most cases. This result suggests that BP is a key outcome in self-management in these patients and that IT-based interventions can help control BP in CKD patients. In the included studies, IT-based interventions had increased the frequency of BP reading by the patient, led to more timely adjustment with the antihypertensive medication regimens and increased the patients’ awareness about the value of BP and their sense of control and had thus led to an improvement in BP through advices such as instructing to change the nutritional regimen [20, 32, 34, 35].
Although process of care outcomes such as medication adherence have no direct effects on clinical outcomes, their mediated improvement can help improve the patient’s clinical conditions as well [38]. The present findings showed that IT-based interventions improve adherence to medication in CKD patients. In line with these findings, a systematic review study by Vervloet et al. showed that automated IT-based interventions have the potential to increase adherence to medication by sending electronic reminders to patients with chronic disease [39]. Considering the importance of timely medication use in CKD patients and their likelihood of non-adherence to medication [11, 12, 40,41,42,43,44,45,46,47,48], IT-based tools are recommended to be used to improve adherence to medication in these patients.
In some of the included studies, wearable devices had been used for the intervention. In most of these studies, the provider received the patient data from a distance and provided any necessary guidance accordingly. The direct and wireless transmission of patient data from the device to the central system reduces human errors caused by manual data entry and transmission to the central system; in addition, the reduced data entry by the patient helps increase the success rate of these systems, since the consumers do not require any computer skills or internet access in this system [32, 49, 50].
With the global growth in mobile technology, facilitating the access to smartphone applications seems like the logical approach for improving patients’ self-management skills. The capacities of these applications include increased access to educational sources and self-management strategies and tracking physical and psychological symptoms. Among the included studies, one conducted by Sevick assessed the effect of mobile applications and found that they had a mixed effect on IDWGA and no effects on sodium intake [22]. A recent systematic review focused on dietary mobile applications and their effects on nutritional indicators in CKD patients reviewed two RCTs and three case studies and showed that using dietary mobile apps in CKD patients causes no significant changes in IDWGA, liquid intake or sodium and potassium intake and only causes a negligible reduction in them [23]. It appears that assessing the actual effectiveness of this technology in improving nutritional indicators in CKD patients requires further clinical trials.
The importance of using PHR in empowering chronic patients has been demonstrated in recent years [51,52,53,54]; for instance, using ePHR in diabetic patients led to an improvement in BP and A1C hemoglobin [52], and this system was further associated with an improved patient satisfaction and increased communication with healthcare providers in patients with prostate cancer [53]. Nonetheless, the researchers did not find any studies on the empowering effects of PHR in kidney patients and future studies are recommended to investigate the effects of using PHR in CKD patients.
Strengths and limitations
This study had several strengths and limitations. The strengths include the extensive search strategy used, which led to the extraction of a large number of studies, and therefore made the likelihood of missing relevant studies very small. Moreover, only RCTs were included in the study (due to the confidence in the high quality of these studies) and other types of studies were not included. The limitations include the exclusion of studies presented in conferences (due to the unavailability of their full text), which means the potential loss of some relevant studies. Moreover, due to the great diversity of outcomes, performing a meta-analysis was not possible.
Implications for practice
In patients in early stages of CKD, preventing progress to the end stages of renal disease (ESRD) is very important. It is therefore necessary for them to gain disease management skills. Disease management is also important for patients who have already reached ESRD. This study showed that IT-based interventions can lead to the empowerment of kidney patients (for example, through BP control and increased adherence to medication intake). Such interventions are therefore recommended to be used in clinical settings to further empower the patients.
Implications for further research
Considering that all these studies have been conducted in developed countries, the effect of the proposed interventions should also be studied in developing countries. The majority of the studies had examined ESRD patients and those undergoing hemodialysis and kidney transplant, and none had examined patients undergoing peritoneal dialysis and only a few were on patients in early stages of CKD. Future studies should evaluate the effects of these interventions on patients undergoing peritoneal dialysis and patients in early stages of CKD.
Conclusion
IT-based interventions such as smartphones/PDAs, wearable devices, and computerized systems could improve self-management in CKD patients (clinical and process outcomes) by removing the gap between them and healthcare providers. Further research is needed on the effects of IT-based interventions on self-management outcomes in CKD patients living in developing countries, patients undergoing peritoneal dialysis, and those in early stages of CKD.
References
Hill, N.R., Fatoba, S.T., Oke, J.L., Hirst, J.A., O’Callaghan, C.A., Lasserson, D.S., and Hobbs, F.R., Global prevalence of chronic kidney disease–a systematic review and meta-analysis. PLoS One. 11(7):e0158765, 2016.
Fraser, S.D., Roderick, P.J., May, C.R., McIntyre, N., McIntyre, C., Fluck, R.J., Shardlow, A., and Taal, M.W., The burden of comorbidity in people with chronic kidney disease stage 3: A cohort study. BMC Nephrol. 16(1):193, 2015.
Ronksley, P.E., and Hemmelgarn, B.R., Optimizing care for patients with CKD. Am. J. Kidney Dis. 60(1):133–138, 2012.
Bethesda, M., US renal data system, USRDS 2011 annual data report: Atlas of chronic kidney disease and end-stage renal disease in the United States. National Institute of Diabetes and Digestive and Kidney Diseases. 10, 2011.
Tuot, D.S., Plantinga, L.C., Judd, S.E., Muntner, P., Hsu, C.-y., Warnock, D.G., Gutiérrez, O.M., Safford, M., Powe, N.R., and McClellan, W.M., Healthy behaviors, risk factor control and awareness of chronic kidney disease. Am. J. Nephrol. 37(2):135–143, 2013.
Wang, L.-M., and Chiou, C.-P., Effectiveness of interactive multimedia CD on self-care and powerlessness in hemodialysis patients. J. Nurs. Res. 19(2):102–111, 2011.
Moattari, M., Ebrahimi, M., Sharifi, N., and Rouzbeh, J., The effect of empowerment on the self-efficacy, quality of life and clinical and laboratory indicators of patients treated with hemodialysis: A randomized controlled trial. Health Qual. Life Outcomes. 10(1):115, 2012.
Yıldız, A.U., and Kurcer, M.A., Life style education and counseling improved quality of life and renal function in patients with chronic kidney disease. TAF Prev. Med. Bull. 11(6):667–672, 2012.
Devins, G.M., Mendelssohn, D.C., Barré, P.E., Taub, K., and Binik, Y.M., Predialysis psychoeducational intervention extends survival in CKD: A 20-year follow-up. Am. J. Kidney Dis. 46(6):1088–1098, 2005.
Devins, G.M., Mendelssohn, D.C., Barré, P.E., and Binik, Y.M., Predialysis psychoeducational intervention and coping styles influence time to dialysis in chronic kidney disease. Am. J. Kidney Dis. 42(4):693–703, 2003.
Karamanidou, C., Clatworthy, J., Weinman, J., and Horne, R., A systematic review of the prevalence and determinants of nonadherence to phosphate binding medication in patients with end-stage renal disease. BMC Nephrol. 9(1):2, 2008.
Ghimire, S., Castelino, R.L., Lioufas, N.M., Peterson, G.M., and Zaidi, S.T.R., Nonadherence to medication therapy in haemodialysis patients: A systematic review. PloS one. 10(12):e0144119, 2015.
Heapy, A.A., Higgins, D.M., Cervone, D., Wandner, L., Fenton, B.T., and Kerns, R.D., A systematic review of technology-assisted self-management interventions for chronic pain. Clin. J. Pain. 31(6):470–492, 2015.
Hamine, S., Gerth-Guyette, E., Faulx, D., Green, B.B., and Ginsburg, A.S., Impact of mHealth chronic disease management on treatment adherence and patient outcomes: A systematic review. J. Med. Internet Res. 17(2), 2015.
Tao, D., and Or, C.K., Effects of self-management health information technology on glycaemic control for patients with diabetes: A meta-analysis of randomized controlled trials. J. Telemed. Telecare. 19(3):133–143, 2013.
Hall, A.K., Cole-Lewis, H., and Bernhardt, J.M., Mobile text messaging for health: A systematic review of reviews. Annu. Rev. Public Health. 36:393–415, 2015.
Heitkemper, E. M., Mamykina, L., Travers, J., and Smaldone, A., Do health information technology self-management interventions improve glycemic control in medically underserved adults with diabetes? A systematic review and meta-analysis. J. Am. Med. Inform. Assoc., 2017.
Tao, D., Wang, T., Wang, T., Liu, S., and Qu, X., Effects of consumer-oriented health information technologies in diabetes management over time: A systematic review and meta-analysis of randomized controlled trials. J. Am. Med. Inform. Assoc., 2017.
Forni Ogna, V., Pruijm, M., Zweiacker, C., Wuerzner, G., Tousset, E., and Burnier, M., Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study. Biomed. Res. Int. 2013:104892, 2013. https://doi.org/10.1155/2013/104892.
Cottrell, E., Chambers, R., and O'Connell, P., Using simple telehealth in primary care to reduce blood pressure: A service evaluation. BMJ Open. 2(6), 2012. https://doi.org/10.1136/bmjopen-2012-001391.
Gallar, P., Vigil, A., Rodriguez, I., Ortega, O., Gutierrez, M., Hurtado, J., Oliet, A., Ortiz, M., Mon, C., Herrero, J.C., and Lentisco, C., Two-year experience with telemedicine in the follow-up of patients in home peritoneal dialysis. J. Telemed. Telecare. 13(6):288–292, 2007. https://doi.org/10.1258/135763307781644906.
Sevick, M.A., Piraino, B.M., St-Jules, D.E., Hough, L.J., Hanlon, J.T., Marcum, Z.A., Zickmund, S.L., Snetselaar, L.G., Steenkiste, A.R., and Stone, R.A., No difference in average interdialytic weight gain observed in a randomized trial with a technology-supported behavioral intervention to reduce dietary sodium intake in adults undergoing maintenance hemodialysis in the united states: primary outcomes of the balancewise study. J. Ren. Nutr. 26(3):149–158, 2015. https://doi.org/10.1053/j.jrn.2015.11.006.
Campbell, J., and Porter, J., Dietary mobile apps and their effect on nutritional indicators in chronic renal disease: A systematic review. Nephrology. 20(10):744–751, 2015.
He, T., Liu, X., Li, Y., Wu, Q., Liu, M., and Yuan, H., Remote home management for chronic kidney disease: A systematic review. J. Telemed. Telecare. 1357633X15626855, 2016.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., and Group, P, Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6(7):e1000097, 2009.
Higgins, J.P.T., Green, S. (Eds.). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Beratarrechea, A., Lee, A.G., Willner, J.M., Jahangir, E., Ciapponi, A., and Rubinstein, A., The impact of mobile health interventions on chronic disease outcomes in developing countries: A systematic review. Telemed. E Health. 20(1):75–82, 2014.
Vegesna, A., Tran, M., Angelaccio, M., and Arcona, S., Remote patient monitoring via non-invasive digital technologies: A systematic review. Telemed. E Health, 2016.
Aitken, M., and Gauntlett, C., Patient apps for improved healthcare: From novelty to mainstream. Parsippany, NJ, IMS Institute for Healthcare Informatics, 2013.
Chaet, A.V., Morshedi, B., Wells, K.J., Barnes, L.E., and Valdez, R., Spanish-Language Consumer Health Information Technology Interventions: A Systematic Review. J. Med. Internet Res. 18(8), 2016.
Gordon, E.J., Feinglass, J., Carney, P., Vera, K., Olivero, M., Black, A., O'Connor, K., MacLean, J., Nichols, S., Sageshima, J., Preczewski, L., and Caicedo, J.C., A culturally targeted website for hispanics/latinos about living kidney donation and transplantation: A randomized controlled trial of increased knowledge. Transplantation. 100(5):1149–1160, 2016. https://doi.org/10.1097/TP.0000000000000932.
Rifkin, D.E., Abdelmalek, J.A., Miracle, C.M., Low, C., Barsotti, R., Rios, P., Stepnowsky, C., and Agha, Z., Linking clinic and home: A randomized, controlled clinical effectiveness trial of real-time, wireless blood pressure monitoring for older patients with kidney disease and hypertension. Blood Press. Monit. 18(1):8–15, 2013. https://doi.org/10.1097/MBP.0b013e32835d126c.
Neumann, C.L., Wagner, F., Menne, J., Brockes, C., Schmidt-Weitmann, S., Rieken, E.M., Schettler, V., Hagenah, G.C., Matzath, S., Zimmerli, L., Haller, H., and Schulz, E.G., Body weight telemetry is useful to reduce interdialytic weight gain in patients with end-stage renal failure on hemodialysis. Telemed. J. E Health. 19(6):480–486, 2013. https://doi.org/10.1089/tmj.2012.0188.
McGillicuddy, J.W., Gregoski, M.J., Weiland, A.K., Rock, R.A., Brunner-Jackson, B.M., Patel, S.K., Thomas, B.S., Taber, D.J., Chavin, K.D., Baliga, P.K., and Treiber, F.A., Mobile health medication adherence and blood pressure control in renal transplant recipients: A proof-of-Concept randomized controlled trial. J. Med. Internet Res. 15(9), 2013. https://doi.org/10.2196/resprot.2633.
Margolis, K.L., Asche, S.E., Bergdall, A.R., Dehmer, S.P., Groen, S.E., Kadrmas, H.M., Kerby, T.J., Klotzle, K.J., Maciosek, M.V., Michels, R.D., O'Connor, P.J., Pritchard, R.A., Sekenski, J.L., Sperl-Hillen, J.M., and Trower, N.K., Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control: A cluster randomized clinical trial. JAMA. 310(1):46–56, 2013. https://doi.org/10.1001/jama.2013.6549.
Jackson, C.L., Bolen, S., Brancati, F.L., Batts-Turner, M.L., and Gary, T.L., A systematic review of interactive computer-assisted technology in diabetes care. J. Gen. Intern. Med. 21(2):105–110, 2006.
Wu, Y., Yao, X., Vespasiani, G., Nicolucci, A., Dong, Y., Kwong, J., Li, L., Sun, X., Tian, H., and Li, S., Mobile app-based interventions to support diabetes self-management: A systematic review of randomized controlled trials to identify functions associated with glycemic efficacy. JMIR mHealth uHealth. 5(3), 2017.
Kaushal, R., Shojania, K.G., and Bates, D.W., Effects of computerized physician order entry and clinical decision support systems on medication safety: A systematic review. Arch. Intern. Med. 163(12):1409–1416, 2003.
Vervloet, M., Linn, A.J., van Weert, J.C., De Bakker, D.H., Bouvy, M.L., and Van Dijk, L., The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: A systematic review of the literature. J. Am. Med. Inform. Assoc. 19(5):696–704, 2012.
Weng, F.L., Chandwani, S., Kurtyka, K.M., Zacker, C., Chisholm-Burns, M.A., and Demissie, K., Prevalence and correlates of medication non-adherence among kidney transplant recipients more than 6 months post-transplant: A cross-sectional study. BMC Nephrol. 14(1):261, 2013.
Magacho, E., Ribeiro, L., Chaoubah, A., and Bastos, M., Adherence to drug therapy in kidney disease. Braz. J. Med. Biol. Res. 44(3):258–262, 2011.
Gerbino, G., Dimonte, V., Albasi, C., Lasorsa, C., Vitale, C., and Marangella, M., Adherence to therapy in patients on hemodialysis. Giornale italiano di nefrologia: organo ufficiale della Societa italiana di nefrologia. 28(4):416–424, 2010.
Chiu, Y.-W., Teitelbaum, I., Misra, M., De Leon, E.M., Adzize, T., and Mehrotra, R., Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients. Clin. J. Am. Soc. Nephrol. 4(6):1089–1096, 2009.
Muntner, P., Judd, S.E., Krousel-Wood, M., McClellan, W.M., and Safford, M.M., Low medication adherence and hypertension control among adults with CKD: Data from the REGARDS (reasons for geographic and racial differences in stroke) study. Am. J. Kidney Dis. 56(3):447–457, 2010.
Sontakke, S., Budania, R., Bajait, C., Jaiswal, K., and Pimpalkhute, S., Evaluation of adherence to therapy in patients of chronic kidney disease. Indian J. Pharm. 47(6):668, 2015.
Blydt-Hansen, T.D., Pierce, C.B., Cai, Y., Samsonov, D., Massengill, S., Moxey-Mims, M., Warady, B.A., and Furth, S.L., Medication treatment complexity and adherence in children with CKD. Clin. J. Am. Soc. Nephrol. 05750513, 2013.
Schmid, H., Hartmann, B., and Schiffl, H., Adherence to prescribed oral medication in adult patients undergoing chronic hemodialysis: A critical review of the literature. Eur. J. Med. Res. 14(5):185, 2009.
Silva, A.N., Moratelli, L., Tavares, P.L., Marsicano, E.D.O., Pinhati, R.R., Colugnati, F.A.B., Lucchetti, G., and Sanders-Pinheiro, H., Self-efficacy beliefs, locus of control, religiosity and non-adherence to immunosuppressive medications in kidney transplant patients. Nephrology. 21(11):938–943, 2016.
Yang, Z., Zhou, Q., Lei, L., Zheng, K., and Xiang, W., An IoT-cloud based wearable ECG monitoring system for smart healthcare. J. Med. Syst. 40(12):286, 2016. https://doi.org/10.1007/s10916-016-0644-9.
Rajanna, V., Vo, P., Barth, J., Mjelde, M., Grey, T., Oduola, C., and Hammond, T., KinoHaptics: An automated, wearable, haptic assisted, physio-therapeutic system for post-surgery rehabilitation and self-care. J. Med. Syst. 40(3):60, 2016. https://doi.org/10.1007/s10916-015-0391-3.
Azizi, A., Aboutorabi, R., Mazloum-Khorasani, Z., Afzal-Aghaea, M., Tabesh, H., and Tara, M., Evaluating the effect of web-based Iranian diabetic personal health record app on self-care status and clinical indicators: Randomized controlled trial. JMIR Med. Inform. 4(4), 2016.
Tenforde, M., Nowacki, A., Jain, A., and Hickner, J., The association between personal health record use and diabetes quality measures. J. Gen. Intern. Med. 27(4):420–424, 2012.
Pai, H., Lau, F., Barnett, J., and Jones, S., Meeting the health information needs of prostate cancer patients using personal health records. Curr. Oncol. 20(6):561–569, 2013.
Crouch, P.-C.B., Rose, C.D., Johnson, M., and Janson, S.L., A pilot study to evaluate the magnitude of association of the use of electronic personal health records with patient activation and empowerment in HIV-infected veterans. PeerJ. 3:e852, 2015.
Funding
This study was supported by a grant from Kashan University of Medical Sciences Research Council (Number: 95,031).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
This article is part of the Topical Collection on Patient Facing Systems
Rights and permissions
About this article

Cite this article
Jeddi, F.R., Nabovati, E. & Amirazodi, S. Features and Effects of Information Technology-Based Interventions to Improve Self-Management in Chronic Kidney Disease Patients: a Systematic Review of the Literature. J Med Syst 41, 170 (2017). https://doi.org/10.1007/s10916-017-0820-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-017-0820-6