
Abstract
The purpose of this study was to develop the Health and Work Survey (INSAT) and examine the validity of the discomfort rating scale. Data were collected from 706 Portuguese workers from six economic sectors with the support of the Health and Work Survey (INSAT - Inquérito Saúde e Trabalho). The INSAT is a self-administered questionnaire to assessing working conditions, health and wellbeing, and to provide information to the occupational health systems in the organisations. For the survey instrument validation, the Rasch Partial Credit Model (PCM) was used to analyse item fit statistics. From the application of PCM, Person Separation Reliability was obtained (0.8761) and the value can be considered very good (>0.8). From the statistical analysis, the Overall Model fit information, given by Outfit Mean square/Infit Mean square, is between 0.5 and 1.5, meaning “Productive for measurement” and “acceptable fit overall”. The INSAT items can generate predictable response patterns. We recommend that the INSAT discomfort rating scale and some other items should be reviewed in future works. In any event, this tool proves to be useful in assessing the relationship between work and health and in evaluating key main risk factors, helping to prevent problems and improving occupational health systems.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the past few years, a growing body of systems /instruments to evaluate occupational health has been observed, with the main goal to improve working conditions and to promote health and wellbeing at the workplace. This concern reflects the idea that if work-related risks are better known, work contexts can be managed more effectively and hence improvements in workers’ health and wellbeing can be achieved.
To better evaluate the impact of working conditions on workers’ health and wellbeing, it is important to analyse a set of different variables such as work characteristics and conditions, health and safety, work organisation, opportunities for the development of work, and balance between work and life outside work, as mentioned by Eurofound [1–3].
In the following sections, the theoretical-methodological principles of the instrument will be explained and its dimensions described. The structure of the instrument and all validation procedures are also described. The article ends with an evaluation of the potential of this instrument in measuring work and health relations and with some recommendations for further research.
Occupational health assessment
Several studies have been completed in the domain of occupational health and work psychology [4–11]. These reinforce the importance of a complete assessment of all work factors that interact with health dimensions, including other health problems caused by working conditions. Some of these lie beyond officially-recognised occupational diseases.
Efforts to improve health and wellbeing are recognised as a multi-dimensional phenomenon comprising the interaction of physical, psychological and social dimensions. It can affect workers at cognitive and behavioural level as well as in their physical and psychological health [8, 12–15]. Thus, it is assumed that a health-work study must adopt a person-centred approach, expressing new and subtle relationships between health and work. It is important to consider workers’ statements, their perceptions, complaints and feelings. The personal and interpersonal dimensions of work activity [16] reveal less visible effects of work on health state (feeling exploited, impossible to express oneself, fear, anxiety, irritability or apathy). This supports the importance of a more individual-centred perspective based on the worker’s subjective experience [16–18].
At this point, it is fundamental to assume a more global, multidimensional, and integrated approach to occupational health assessment and recognise the multifactorial status of health problems [18–26]. The development of an instrument that meets these requirements has two main goals. The first is to support research about health and wellbeing at work, providing evaluation of causes (three dimensions for work conditions: environment and physical constraints; organisational and relational constraints; and work characteristics) and effects (three dimensions for health and wellbeing: occupational disease; health problems; and subjective wellbeing). The second goal is to help workers and organisations to develop diagnoses and to design intervention plans in a work context.
INSAT development
The Inquérito Saúde e Trabalho (INSAT) was developed to analyse the relationship between work conditions and health and wellbeing. It consists of a self-administered questionnaire that allows the identification, description and evaluation of a set of questions related with work characteristics and conditions, the individual’s physical and psychological health problems, and their wellbeing. It also enables analysis of the interactions between physical, cognitive, organisational and psychosocial dimensions related with work activity as well as their effects on physical and social health and psychological wellbeing [27].
The development of this survey had contributions from different European surveys, such as the SUMER, the EVREST, and European Working Conditions Survey conducted by Eurofound since 1990 [19, 28] .
The first published version of INSAT was presented in 2007, reviewed in 2010, 2013, and consolidated in 2016, through several studies developed in different business sectors in Portugal such as: a) Health and Social Support; (b) Education; (c) Wholesale and Retail; (d) Manufacturing Industry; (e) Public Administration and Defence, and (f) other service activities [27, 29–33].
The INSAT survey was validated by the ethical commission of the University of Porto and University Fernando Pessoa since 2015.
Underlying objectives to INSAT application
The following related objectives can be identified: 1) characterise work conditions in different business sectors; 2) Identify the main risk factors and their interactions; 3) support the organisations, work physicians, and health and safety technicians in defining risk maps; 4) promote individual and group awareness related of the effects of work conditions on health and safety.
Material and methods
Instrument structure and variables
The INSAT focuses on the diverse and variable questions related to different work situations. It has a logical and integrated structure – from the causes to their effects – to promote increased worker awareness about the effects of work in health and wellbeing.
The INSAT includes different sets of questions organised into seven sections.
First section: The Work. A set of questions focuses on job description in terms of the nature of work, type of contract, working hours and shifts.
Second Section: Work Characteristics and Conditions. Questions about worker exposure conditions are grouped in three categories: 1 – Physical and Environmental Constraints such as noise, vibrations, temperature, radiation, biological and chemical agents, and physical constraints such as repetitive movements, intense physical efforts, painful postures, and workplace ergonomic issues; 2 – Organisational and Relational Constraints such as pace of work, autonomy and initiative, and relational constraints, work relations and relations with the public; 3 – Work Characteristics. Statements about my work that lead to a lack of satisfaction (e.g. facing high demands; being exploited in my work; working conditions that undermine my personal dignity) or pleasure and personal achievement (e.g. learning new things; my work is useful to society).
Third Section: Conditions of one’s life outside work. Questions about conciliation between work and family, time spent travelling to and from work, and on housework and childcare.
Fourth Section: Training and Work. Questions about training hours and contents.
Fifth Section: Health and Work. Questions about work accidents and occupational diseases; and information provided by the organisation about professional risks and their prevention.
Sixth Section: My health and my work. A list of common health problems such us back pain, headaches, respiratory, heart and vision problems, and musculoskeletal disorders, among others. If the answer is affirmative, the respondent is invited to present his perception about the relationship between the health problem identified and his work. There is also some information about specific pathologies and medication consumption.
Seventh Section: My health and wellbeing. A set of questions about health and wellbeing, using the Portuguese version of the Nottingham Health Profile (NHP) [31].
This instrument includes 154 items that cover all sections. All sections present a dichotomous scale (yes or no) and for Work Characteristics and Conditions (second section) the participants are also invited to indicate the degree of discomfort for each situation, using a Likert rating scale 1 to 5, where 1 represents “absence of discomfort” and 5 represents “maximum discomfort”. For example, if the answer to noise exposure is “yes”, the participant must indicate the level of discomfort that causes that exposure in an ordinal scale, 1 to 5 (discomfort scale).
Data collection
Data were collected in several companies using a self-administered paper and pencil questionnaire, followed by the researchers’ guidance, and conducted between 2010 and 2014. Participants received all materials consisting of the INSAT, a covering letter explaining the purpose of the survey, and the guidelines to complete it. All of the participants gave their informed consent to participate, and their confidentiality was guaranteed.
Sample
For the validation process of the INSAT survey a sample with 706 Portuguese workers was selected with the following characterisation: 37% were male and 63% were female; the mean age was 37.65 years with a standard deviation of 9.05; for the highest level of education, the levels more commonly reported were basic education (22%), high education (43%) and graduate (23%).
The sample included workers from six economic sectors: (a) Health and Social Support (hospital front offices and pharmacists); (b) Education (high school and university teachers); (c) Wholesale and Retail (salespeople, store managers and market cashiers); (d) Manufacturing Industry (highly-qualified and technical staff, middle managers, back office workers, warehouse and logistics workers, and assembly line workers); (e) Public Administration and Defence (directors, middle managers, case-workers, human resources technicians, front and back office workers), and (f) Other service activities (hairdressers, psychologists). An exclusion criterion was defined for those workers who did not answer a third or more of the questions.
Statistical analysis
The statistical analysis applied to this survey was divided into two parts: A descriptive analysis was applied to all sections; and a validation process using Rasch Partial Credit Model (PCM) was applied only to section II – Conditions and characteristics of work within the categories: 1 – Physical and Environmental Constraints; 2 – Organisational and Relational Constraints; 3 – Work Characteristics.
Using Rasch model for validation
In the first version of INSAT concerns regarding the content validity were discussed with a multidisciplinary team including psychology, ergonomics, and medical researchers as well as a sample of workers from several business sectors. The team also analysed the format in which the issues were presented and the rating scales [34, 35]. The collected comments contributed to the reformulation of some items and the review of some response scales to ensure their suitability to participants.
The Rasch Partial Credit Model (PCM) was used to validate the process of the discomfort rating scale. Although exploratory factor analysis (EFA) and Cronbach’s alpha are the classical statistical methods used to assess psychometric validity, these methods have been criticised by several authors as being insufficient to assess validity in psychological research instruments [36–38].
The selection of this psychometric validation model is supported by the following factors: it is a model with a strong tradition in the field of health [39, 40] and was originally developed for binary data (most INSAT variables are precisely dichotomous or ordinal type); the validation model is “sample-free” (it is not necessary to calibrate the model for each sample of workers who answered the survey) [41, 50, 51]; it has a probabilistic and not deterministic character and, therefore, is consistent with the type of statistical analysis commonly-used in the treatment of INSAT results (nonparametric and logistic regression tests) [29–31]; and the Rasch model allows for invariance test items, which is of particular importance considering the cross-cultural use of instruments of this type.
This model specifies that each item has its own rating scale structure. It is derived from multiple-choice tests where responses that are incorrect, but indicate some knowledge, are given partial credit towards a correct response. The amount of partial correctness varies across items. This is considered by some authors to be one of the simplest and most useful Item Response Theory (IRT) models [42, 43].
The PCM was applied to all 76 items from the second section and the rating scale was “reorganised” to align with this application. This section has two types of scales for each item, a first with a nominal scale for exposure risk factor (yes / no) followed by an ordinal scale for measuring discomfort (e.g., from 1 to 5, where 1 represents the absence of discomfort and 5 represents the maximum discomfort). To apply PCM the scales were transformed and codified in only one scale: 0 – Not exposed and no discomfort; 1 – Exposed and no discomfort; 2 – Exposed and minor discomfort; 3 – Exposed and discomfort; 4 – Exposed and quite discomfort; 5 – Exposed and too much discomfort.
The software used was R version 3.2.0, with package eRm, and IBM SPSS statistics, version 22.
Results
Descriptive analysis
Relevant INSAT descriptive results are expressed in terms of frequency of exposure to different risk factors (for higher frequencies: > 50% in our sample) – environmental risk factors (e.g. 58.1% for harmful noise and 67.3% for temperature variations – heat/cold), physical constraints (e.g. 62.0% repetitive gestures, 56.0% for standing up in the same position for a long period of time, and 58.1% for standing up with displacements), and work intensification constraints (e.g. 52.3% for high pace of work, 67.7% for standard production or restricted deadlines, 63.5% for having constantly to adapt to method changes or work tools, 57.8% for working for long periods at the computer, 64.4% for frequent interruptions, 69.0% for hyper-requests, and 65.5% for having to continue working beyond my assigned timetable).
Rasch Partial Credit Model (PCM)
As previously noted, the PCM was applied to 76 items from the second section of INSAT (work conditions and characteristics: environment, physical constraints and work characteristics). Item 57 (sexual orientation discrimination) was excluded because all the participants answered 0 (not exposed and no discomfort).
The Person Separation Reliability obtained was 0.8761 and the statistical information obtained for the Overall Model fit, given by Outfit Mean square /Infit Mean square is presented in Table 1.
The statistical results of the item fit (an index of whether items function logically and provide a continuum useful for all responses) were obtained and presented in Table 2 (Physical and Environmental Constraints such as noise, vibrations, temperature, radiation, biological and chemical agents, and physical constraints such as repetitive movements, intense physical efforts, painful postures, and workplace ergonomic issues), Table 3 (Organizational and Relational Constraints such as pace of work, autonomy and initiative, and relational constraints, work relationships and relations with the public), and Table 4 (Work Characteristics such as workers’ dissatisfaction and difficulties - e.g. working to high demands; the feeling of being exploited; working conditions which diminish personal dignity, − or pleasure and personal achievement feelings - e.g. learning new things; being useful to society).
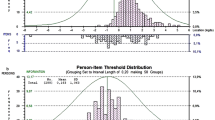
Figures 1, 2 and 3 show the location of item (and threshold) parameters as well as the distribution of person parameters along the latent dimension. Person-item maps are useful in comparing the range and position of the item measure distribution (lower panel) to the range and position of the person measure distribution (upper panel).

Person-item map for physical and environmental constraints

Person-item map for organisational and relational constraints

Person-item map for work characteristics
Discussion
The INSAT, by adopting an approach that takes a more focused perspective on the person and oriented to a subjective dimension [17, 44] helps to identify new, more discret relationships between health and work (including those of a psychosocial nature, such as fear, anxiety, irritability or apathy). In fact, a health and wellbeing orientation places the centre of the analysis on different dimensions. It is not just the use of physical and mental dimensions and even the affective dimension, but a full use of itself [45, 46].
The descriptive analysis revealed a large exposure either to environmental, physical, organisational or psychosocial risks in a sample that contemplates six business sectors and different professions. This reinforces the importance of INSAT in assessing the relationship between the work and health of individuals, and evaluating the main risk factors which can be used to prevent problems and improve health at work.
From the PCM the Person Separation Reliability obtained, which indicates the proportion of person variance that is not due to error, is considered very good (>0.8) (The concept is similar to Cronbach’s α in definition and value) [47]. The results obtained for Overall Model Fit, based on the criteria defined by Linacre, which should be between 0.5 and 1.5 [48], mean “Productive for measurement” and “acceptable fit overall”. As result, it is expected that these items from the INSAT Survey generate predictable response patterns.
From the analysis of the Item Fit statistics only a few items fail to fulfil the same criteria defined by Linacre [48] (bold in Tables 3 and 4). From the analysis of outfit measure (since the Infit measure – information weighted fit statistics – is less sensitive than Outfit measure – outlier sensitive statistics), it was possible to determine that some items from category Organisational and Relational Constraints (i27 – Take work home; i50 - sexual harassment; i58 – Direct contact with the public; and i62 - Physical aggression from the public) (Table 3), as well as some items from the category Work Characteristics (i65 – monotonous work; i68 – Complex work; i70 – lack of career evolution; and i72 – lack of resources to do my work) (Table 4), under fit the data, meaning that they contain unusual and /or inappropriate response patterns [42, 49]. All of these items, which reveal inappropriate wording (that means not completely understood by the participants), will be rewritten or further clarified to make them more obvious and easier to understand.
Some items from the category Organisational and Relational Constraints (i42 – no help from colleagues; i43 - rare exchange experiences; and i55 – nationality discrimination) over fit the data, which means small variations in the response pattern suggest redundant items (Table 3) [42, 49]. Independently of the statistical results, these items will be maintained due to their importance in the occupational health evaluation, namely inasmuch as they concern psychosocial risks.
From Figs. 1, 2, and 3 it is possible to observe that the distribution of a person’s ability is well shaped, with the mode located on the “more ability” range to deal with discomfort. Regarding the item map, all of them are in the middle of the “discomfort” range, meaning they are not too high disturb / too low disturb impact factor.
Conclusions
The statistical results obtained using PCM for INSAT validation reveal generally very good results. From the statistical analysis the Overall Model fit information, given by Outfit Mean square /Infit Mean square, it is possible to conclude that most of the items can generate predictable response patterns. However, some of them did not fulfil the referred-to criteria and must be analysed more carefully to ensure the improvement of the instrument in the next INSAT revision. The improvement of INSAT rating scale for the Work Characteristics and Conditions items (second section) is also important, and the transformed scale used in this work is a good suggestion.
These results corroborate the idea that INSAT is a valid multidimensional evaluation instrument, considering the fact that it integrates the analysis of different risk factors with good predictive indicators. In fact, the complexity that characterizes the relationship between health and work requires the understanding of a set of factors that interact with each other, and at different levels of functioning.
As such, the integration of a diverse set of issues related with work context (even those that appeal to a more subjective dimension of work activity analysis) is one of the central concerns of this instrument and an anchor point of the methodological approach proposed.
Due to the complexity that characterizes the relationship between health and work an instrument such as INSAT, which integrates a set of factors that interact with each other and at different levels of functioning, is fundamental for a comprehensive and multifaceted approach to the evaluation of health and work, and in promoting more effective interventions in occupational health issues.
References
Eurofound, Health and well-being at work - Q2 2014, Brussels: European Observatory for Working Life. 2015.
Eurofound, Developments in working life in Europe. EurWORK annual review 2014, 2015.
Eurofound and EU-OHSA, Psychosocial risks in Europe: Prevalence and strategies for prevention, Publications Office of the European Union: Luxembourg. 2014.
André, J.-C., Complexity and occupational safety and health prevention research. Theoretical Issues in Ergonomics Science. 6(6):483–507, 2005. doi:10.1080/14639220500071570.
Daubas-Letourneux, V., and Thébaud-Mony, A., Organisation du travail et santé dans l’Union Européenne. Office des Publications Officielles des Communautés Européennes, Luxembourg, 2002.
Derriennic, F., Touranchet, A., and Volkoff, S., Âge, travail, santé. Les Éditions INSERM, Paris, 1996.
Gollac, M., and Volkoff, S., Les Conditions de Travail. Éditions La Découverte, Paris, 2000.
Ilmarien, J., Work ability – A comprehensive concept for occupational health research and prevention. Scand J Work Environ Health. 35(1):1–5, 2009. doi:10.5271/sjweh.1304.
Nielsen, K., et al., Conducting organizational-level occupational health interventions: What works? Work & Stress. 24(3):234–259, 2010. doi:10.1080/02678373.2010.515393.
Stansfeld, S.A., and Candy, B., Psychosocial work environment and mental health – A meta-analytic review. Scandinavian Journal of Work and Environmental Health. 32:443–462, 2006.
Teiger, C., Le vieillissement différentiel par et dans le travail: un vieux problème dans un contexte récent. Le Travail Humain. 52(1):21–56, 1989.
Molinié, A. and A. Leroyer Suivre les évolutions du travail et de la santé: EVREST, un dispositif commun pour des usages diversifiés. PISTES. 3, 2011.
Taris, T., et al., Inequity, burnout and psychological withdrawal among teachers: A dynamic exchange model. Anxiety, Stress and Coping. 11(1):103–122, 2004.
Kortum, E., Leka, S., and Cox, T., Psychococial risks and work-realted stress in developing countries: Health impact, priorities, barriers and solutions. Int J Occup Med Environ Health. 23(3):225–238, 2010. doi:10.2478/v10001-010-0024-5.
Farzanfar, R., et al., Design and development of a mental health assessment and intervention system. J Med Syst. 31:49–62, 2007. doi:10.1007/s10916-006-9042-z.
Clot, Y. and J. Leplat La méthode clinique en ergonomie et en psychologie du travail. Le Travail Humain, 4(68): p. 289–316, 2005.
Ilies, R., Aw, S., and Pluut, H., Intraindividual models of employee well-being: What have we learned and where do we go from here? European Journal of Work and Organizational Psychology. 24(6):827–838, 2015. doi:10.1080/1359432X.2015.1071422.
Barros-Duarte, C. and M. Lacomblez Santé au travail et discrétion des rapports sociaux. . Revue électronique PISTES - Perspectives interdisciplinaires sur le travail et la santé. 2006.
Coutrot, T., and Wolff, L., L’impact des conditions de travail sur la santé: une expérience méthodologique. Centre d’études de l’emploi, Paris, 2005.
Härenstam, A., et al., Multilevel analyses of organizational change and working conditions in public and private sector. European Journal of Work and Organizational Psychology. 13(3):305–343, 2004. doi:10.1080/13594320444000119.
Cunha, L., S. Nogueira, and M. Lacomblez, Beyond a man's world: Methodological contributions of considering gender when studying bus drivers' activity. . Work, 2014, DOI: 10.3233/WOR-131611.
Mergler, D., Combining quantitative and qualitative approaches in occupational health for a better understanding of the impact of work-related disorders. Scandinavian Journal of Work, Environment & Health. 15(4):54–60, 1999.
Arandjelovic, M., A need of holistic approach to the occupational health developing (in Serbia). Int J Occup Med Environ Health. 24(3):229–240, 2011. doi:10.2478/s13382-011-0033-z.
Janssens, H., et al., Association between psychosocial characterisitcs of work and presenteeism: A cross-sectional study. Int J Occup Med Environ Health, 29(2): p. 331–344, 2016, DOI: 10.13075/ijomeh.1896.00588.
Carvalho, J., A. Rocha, and A. Abreu, Maturity Models of Healthcare Information Systems and Technologies: a Literature Review. J Med Syst 40(131), 2016, DOI: 10.1007/s10916-016-0486-5.
Rocha, A. and J. Freixo, Information Architecture for Quality Management Support in Hospitals. J Med Syst 39(125), 2015, DOI: 10.1007/s10916-015-0326-z.
Barros-Duarte, C., Cunha, L., and Lacomblez, M., INSAT: uma proposta metodológica para análise dos efeitos das condições de trabalho sobre a saúde. Laboreal. 3(2):54–62, 2007.
Niedhammer, I., Chastang, J., and David, S., Importance of psychosocial workfactors on general health outcomes in the national French SUMER survey. Occup. Med. 58(1):15–24, 2008.
Barros-Duarte, C., et al., Occupational risks behind teaching activity (223–228) in Occupational Safety and Hygiene II, P.A.e. al., Editor, Taylor & Francis Group, CRC Press. p. 803pp, 2014.
Barros, C., et al., Will I be able to do my work at 60? An analysis of working conditions that hinder active ageing. WORK: A Journal of Prevention. Assessment & Rehabilitation. 51:579–590, 2015. doi:10.3233/WOR-152011.
Silva, C., et al., Prevalence of back pain problems in relation to occupational group. International Journal of Industrial Ergonomics. 52:52–58, 2016. doi:10.1016/j.ergon.2015.08.005.
Barros-Duarte, C., and Cunha, L., INSAT2010 – Inquérito Saúde e Trabalho: outras questões, novas relações. LABOREAL. 6:19–26, 2010.
Barros-Duarte, C. and L. Cunha, Avaliação dos fatores psicossociais de risco: contributos do Inquérito INSAT (333–346) in Manual sobre Riscos Psicossociais no Trabalho, H.V.Neto, J.Areosa, and P.A. (Org), Editors, Vila do Conde: Civeri Publishing, 2014.
Haynes, S., Richard, D., and Kubany, E., Content validity in psychological assessment: A functional approach to concepts and methods. Psychol Assess. 7:238–247, 1995.
Kline, P., Handbook of Psychological Testing Routledge; 2 edition. 752. 2000.
Waugh, R., and Chapman, E., Attitude to mathematics for primary-aged students: A comparison of true score and Rasch measurement in Frontiers in Educational Psychology, Nova science publishers, New York. USA. p. 89-105, 2005.
Sijtsma, K., On the use, the misuse and the very limited usefulness of Cronabch’s alpha. Psychometrika. 74(1):107–120, 2009. doi:10.1007/s11336-008-9101-0.
Rocha, N., and Fleck, M., Validity of the Brazilian version of WHOQOL-BREF in depressed patients using Rasch modelling. Rev Saúde Pública. 43(1):147–153, 2009.
Tennant, A., and Conaghan, P., The Rasch measurement model in rheumatology: What is it and why use it? When should it be applied, and what should one look for in a Rasch paper? Arthritis Care & Research. 57(8):1358–1362, 2007. doi:10.1002/art.23108.
Shea, T., A. Tennant, and J. Pallant Rasch model analysis of the Depression, Anxiety and Stress Scales (DASS). BMC Psychiatry. 9, 2009. DOI: 10.1186/1471-244X-9-21.
Wright, B. and M. Stone, Measurement essentials. Wilmington: Wide Range Inc. 221. 1999.
Green, C. and C. Frantom, Survey development and validation with Rasch Model: International Conference on Questionnaire Development Evaluation, and Testing, Charleston, SC, November, 14–17. p. 30. 2002.
Mair, P., R. Hatzinger, And M.J. Maier, Extended Rasch Modeling: The R Package eRm. PDF-Dateianhang zum Programmpaket eRm, 2009.
Dejours, C., Insatisfaction au travail et souffrance mentale. in Problèmes politiques et sociaux, Thébaud-Mony, A. & Robatel N. (orgs.). p. 35–49, 2009.
Schwartz, Y., Le paradigme ergologique ou un métier de philosophe. Octarès, Toulouse, 2000.
Thébaud-Mony, A., Riscos. Laboreal. 6:72–73, 2010.
Wright, B.D., and Stone, M.H., Measurement essentials. Wilmington. Wide Range Inc: p. 221, 1999.
Linacre, J.M., What do Infit and outfit, mean-square and standardized mean? Rasch Measurement Transactions. 16(2):878, 2002.
Joan Stelmack, O., et al., Use of Rasch person-item map in exploratory data analysis: A clinical perspective. Journal of Rehabilitation Research & Development, 2004.
Gonçalves, J.J., and Rocha, Á., A decision support system for quality of life in head and neck oncology patients. Head & Neck Oncology. 4(1):3, 2012.
Faria, B.M., Gonçalves, J.J., Reis, L.P., and Rocha, Á., A clinical support system based on quality of life estimation. Journal of Medical Systems. 39(10):114, 2015.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Patient Facing Systems
Rights and permissions
About this article

Cite this article
Barros, C., Cunha, L., Baylina, P. et al. Development and Validation of a Health and Work Survey Based on the Rasch Model among Portuguese Workers. J Med Syst 41, 79 (2017). https://doi.org/10.1007/s10916-017-0727-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-017-0727-2