
Abstract
A picture archiving and communication system (PACS) is a medical imaging technology which provides economical storage of and convenient access to images from multiple modalities (source machine types). PACS have been widely introduced as a credible alternative to the traditional film-based radiological service. This study was planned and conducted to determine the physicians’ views and assessments on PACS in two public hospitals in Turkey. A questionnaire was prepared by viewing the literature related to PACS. The questionnaires were distributed several times to a total of 150 physicians two public hospitals in Ankara, Turkey. The overall response rate is 46%. Some questions required a graduated score in response and others an open ended response. The majority of physicians judged PACS to be a major advance for their hospitals with less frustration than using film high quality images and an improvement in their working lives and patient care. They reported that PACS gave them to radiology reports in short time. Also physicians believed that PACS has improved their consultations. Open ended questions were prepared with concerning the benefits and disadvantages of PACS. The assessments of the physicians demonstrated many more benefits than disadvantages of PACS in their hospitals. PACS has been accepted well by a wide percentage of hospital physicians. PACS evolves over time components are frequently replaced and so the users must expect continuous learning about new updates and improved functionality. The implementation of the PACS clearly contributes to an increase in the productivity of health professionals and physicians
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Healthcare providers and governments around the world are facing an unprecedented challenge to improve the quality of healthcare while simultaneously reducing costs. Medical information technology plays an important role in meeting this challenge. Today, we have more and better medical information technologies than ever before [1]. However, medical information and records are usually maintained separately by various healthcare providers often in paper format preventing their optimal use for the treatment and care of patients. In an effort to both improve healthcare quality and reduce costs of healthcare professionals in all specialty areas are moving from paperbased medical records to integrated electronic health records (EHRs). In addition, clinical departments using imaging equipment are moving to picture archiving and communication systems (PACS) for the management of image data [2]. PACS is being seen as an indispensable part of the drive towards a full Electronic Patient Record [3].
PACS is widely used in hospitals and is considered a mission critical system for around-the-clock daily clinical operation [4]. A Picture Archiving and Communication System (PACS) is one of the most valuable tools supporting the medical profession both in decision-making and during treatment procedures. Healthcare organizations and hospitals are increasingly turning to digital medical imaging systems to promote better diagnosis and treatment of their patients. The implementation of the PACS clearly contributes to an increase in the productivity of health professionals and physicians [5, 6].
PACS based on digital communication display and information technologies has revolutionized the practice of radiology, and in a sense of medicine during the past 15 years [7, 8]. The radiology component of this revolution is often called PACS [9]. Although the concept of PACS was developed in Europe during the latter part of the 1970s no working system was completed at that time. The first PACS implementations took place in the United States in the early 1980s. Some more or less successful PACS developments also took place in Europe in the 1980s particularly in the Netherlands, Belgium, Austria, the United Kingdom, France, Italy, Scandinavia, and Germany [10, 11].
A PACS is a medical imaging technology which provides economical storage of and convenient access to images from multiple modalities (source machine types) (Choplin, 1992). Electronic images and reports are transmitted digitally via PACS; this eliminates the need to manually file retrieve or transport film jackets The universal format for PACS image storage and transfer is DICOM (Digital Imaging and Communications in Medicine) [12, 13]. Non-image data, such as scanned documents, may be incorporated using consumer industry standard formats like PDF (Portable Document Format), once encapsulated in DICOM, A PACS consists of four major components: The imaging modalities such as X-ray computed tomography (CT) and magnetic resonance imaging (MRI) a secured network for the transmission of patient information, workstations for interpreting and reviewing images, and archives for the storage and retrieval of images and reports. Combined with available and emerging web technology. PACS has the ability to deliver timely and efficient access to images, interpretations, and related data. PACS breaks down the physical and time barriers associated with traditional film-based image retrieval, distribution, and display [2, 13].
PACS are becoming recognised as the most appropriate means of acquiring, archiving and communicating all forms of radiology imaging because of the some benefits listed in below [3].
Image manipulation, Reduced radiation dose with computed radiography and direct radiography, Reduction in repeat radiographs, Instant image availability, Previous image availability and comparison, No lost images, Images available in many places simultaneously, Improved medical staff efficiency, Reports available with images etc.
There have been several studies which have attempted to demonstrate the benefits and disadvantages of PACS to users and physicians, but many of these have concentrated on particular groups of users such as radiology trainees [14], users in a particular clinical units [15] or have been more focused in their approach and physicians’ experiences [16, 17]. A limited study was conducted and planned views and assessments of clinicians on PACS in Turkey. This study was planned and conducted to determine the physicians’ views and assessments on PACS in two public hospitals in Turkey.
Method
This study is descriptive and based on questionnaire survey. A questionnaire was prepared by viewing the literature related to PACS [3, 18]. This questionnaire was used by JR Pilling in 2002. It used a combination of responses to statements and questions, graduated from 1 to 6 and some opportunities for open ended questions. Respondents were invited to allocate a score from 1, if they thought they could not agree with the question or statement at all to 6, if they were in complete agreement with the statement or question. The statements/questions are documented in Table 1 with an indication of the values of a score of 1 and 6 in relation to each question. The questionnaire has some statements/questions about use of PACS, facilities available, the perceived quality of images, reporting, image availability, image accessibility, training, ease of use of PACS, benefits and disadvantages of PACS. Any sampling method was not used this study. The questionnaires were distributed several times to a total of 150 physicians who used PACS in two public hospitals in Ankara, Turkey. The universe of this study is 150 physicians who used PACS for 2 years. The overall response rate is 46% (69 physicians). The survey was conducted from the beginning of November to mid-December 2008. All questionnaires were taken anonymously.
The hospitals where this study was conducted and planned have gotten PACS for 2 years. Two public hospitals in Ankara were chosen for his study. Because these hospitals had PACS in 2008. These are education hospitals serving a population of approximately 500,000 people. These hospitals build a fully filmless PACS in 2005. As part of the PACS Project all CT and MRI scans and 80% of plain radiographs were archived on to PACS starting in March 2007. Physicians at these hospitals were trained in the use of the PACS before moving to a fully filmless operation.
Results
This section explains the main results according to tables. The full results for 69 physicians are listed in Table 1.
The results were very encouraging with 94% agreeing strongly or very strongly that PACS had been a useful advance for their hospitals. Responses about the quality of the images on the Image Review Workstations/their PCs scored between 2 and 6. Physicians had been consulted about their requirements for viewing images and their choice of 17 in. flat screen LCDs proved to be very good. The availability of radiology reports alongside the images was considered useful by the majority with 74% scoring 5 or 6 for this response. For physicians PACS had improved their consultations with the majority scoring 3 to 6 on all four sections of question about “improving your consultation”. The ability to easily demonstrate images to patients. the improved efficiency in finding images and reports. and the overall improved efficiency of the consultation all showed a favourable response. Question 5 was worded to explore how much PACS had impacted the conduct of ward rounds. It can be seen that this impact was widespread and that most clinicians had altered the conduct of their ward rounds. Four physicians found image review more difficult but a few found it very easier with the majority (36%) of physicians. Overall physicians (56%) preferred PACS to film and found it much less frustrating. One of the benefits of PACS is the reduction in frustration afforded by the instant availability of images and the need no longer to handle films and film packets physically. 66% of respondents scored 5 to 6 on this question shows that the impact of PACS on improving the physicians’ working life. PACS improve especially working life of radiographs and radiology personnel. For the majority of physicians PACS has resulted in a significant change in working practice with 88% scoring 4 to 6 for question about the impact of PACS on working practice. 69% of respondents scored between 5 and 6 in favour of PACS meeting their expectations. The majority of physicians believed that PACS reduce costs, improve patient satisfaction and quality.
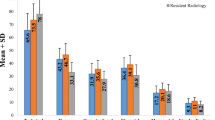
Table 2 shows views and assessments about PACS of physicians according to study hospitals. In this study it is found that there are significant differences between views and assessments about PACS of physicians according to A and B education hospital. There are significant in terms of “The quality of the images on the Image Review Workstation/your PCs”, “Usefulness of radiology reports on PACS”, “Improving your consultation of PACS by reducing the time spent finding images for review”, “Improving your consultation of PACS by reducing the time spent finding radiology reports”, “Changing the conduct of ward round by making it more difficult to review images during a ward round”, “Changing the conduct of ward round by making changes in the way images are reviewed at the beginning of a ward round, the ward round itself is conducted more efficiently”, “Causing you more or less frustrations than using film”, “Meting your expectations for PACS”, “Improving patient care”, “Improving patient satisfaction and quality”. Reason of these significant differences between two hospitals may be that different PACS software is used, and respondents have varying levels of training and experience.
Table 3 shows the perceived benefits of PACS. The perceived benefits of PACS match well the proclaimed benefits which have been trumpeted by PACS suppliers and PACS enthusiasts alike in literature. In this study more perceived benefits of PACS are “Improving the quality and validity of image and adjusting the image sizes”, “Immediate access to reports and availability of images”, “No film packet handling/no lost images”, “Evaluation the films/images with patients (Showing images to patients/patients better informed)”, “Economical and effective”, “Reducing the costs of personnel and materials”.
Table 4 shows the perceived disadvantages of PACS. The perceived benefits of PACS match well the proclaimed benefits which have been trumpeted by PACS suppliers and PACS enthusiasts alike in literature. In this study more perceived disadvantages of PACS are “System failures/can’t log on”, “High maintenance and repair costs”, “Log on problems/moving between systems”.
Discussion and Conclusion
PACS based on digital, communication, display, and information technologies (IT) has revolutionized the practice of radiology, and in a sense, of medicine during the past 30 years. There are many advantages of introducing digital, communications, display and IT to the conventional paper- and film-based operation in radiology and medicine. For example, through digital imaging plate and detector technology and various energy source digital imaging modalities it is possible to improve the modality diagnostic value while at the same time reducing the radiation exposure to the patient, and through the computer and display, it is possible to manipulate a digital image for value-added diagnosis. Also, digital, communication, and IT technologies can be used to understand the health care delivery workflow resulting in speeding up health care delivery and reducing operation costs [7].
The results and findings of this study are consist with the results of previous studies in literature [3, 14, 17, 19–22].
There are some studies are explained in summery in below. PACS are being implemented within radiology departments, and many facilities are entering the next stage of PACS use by deploying PACS to departments outside of radiology and to other facilities located at a distance. Many PACS vendors and department administrators have based cost-justification analyses on the anticipated savings from expanding PACS to these areas. However, many of these cost-savings analyses can be highly suspect in their assumptions and findings. Technology assessment (TA) at the hospital/health system level is an organized, systematic approach to examining the efficacy of a technology in relation to the health system’s mission and clinical needs [20].
A multicentre study conducted and planned by SL. Tan and RA. Lewis was undertaken to assess user’s impressions of picture archiving and communication systems (PACS). In their study 83% felt PACS benefited their work, 79% felt PACS was better than hard copies and 83% would recommend it. Several potential problems were highlighted. Half of responders had no training to use PACS. Of those, 50% stated that no training had been offered. A second concern was unreliability, with 20% feeling that the system was unable to be used at least 1 week every year. Third was the poor quality of images, due to the poor quality of the monitors. All these problems will need to be addressed by any trust intending to implement a reliable and useful system [17]. Mackinnon et al. (2008) had a study to evaluate the impact of picture archiving and communications systems (PACS) on reporting times and productivity in a large teaching hospital. In their study they found out that between 2002 and 2006 the number of radiological patient episodes increased by 30% from 11,531/month to 15,057/month. This was accompanied by a smaller increase in WTE reporting radiologists, from 32 to 37 (15%). Mean reporting times have improved substantially post-PACS, plain radiograph reporting time decreased by 26% (from 6.8 to 5 days; p = 0.002) and specialty modalities by 24% (4.1 to 3.1 days; p < 0.001). Radiologist productivity has increased by 18% (337 films to 407 films/WTE radiologist/month). Unreported films have decreased from 5% to 4% for plain radiographs and are steady for specialty modalities (<1%). In most areas improvements have been sustained over a 3-year period. Since the introduction of PACS, reporting times have decreased by 25% and the productivity improved by 18%. Sustained improvements are felt to reflect the efficiencies and cultural change that accompanied the introduction of PACS and digital dictation [21]. Interviews were carried out with 34 key users and providers of the radiological service at Hammersmith Hospital. Overall, staff were very satisfied with PACS particularly in terms of image availability. All staff said that they preferred PACS to the previous, conventional radiology service [19]. Bryan et al. (1999) planned a study to establish the net costs to the hospital and the broad range of benefits associated with a hospital-wide picture archiving and communication system (PACS) that comprised digital acquisition, storage and transmission of radiological images via a hospital-wide network to 150 workstations. Bryan et al. revealed that PACS was associated with some improvements in the performance of the radiology department: improved image availability (97.7% versus 86.9%), lower repeat imaging rate (7.3% versus 9.9%) and 20% lower total radiation doses for examinations of the lateral lumbar spine. No improvements were identified in the quality of the radiology reporting service. Benefits outside radiology included shorter time from examination to image availability for routine uses in intensive care (19 versus 37 min), and a lower rate of diagnostic ‘errors’ in casualty (0.65% versus 1.51%). High levels of satisfaction with PACS were found amongst both providers and clinical users [23]. PACS was almost universally preferred by users and brought many operational and clinical benefits. However, these advantages came at a significant personnel and material, capital and net eunning costs. Maass et al. (2001) analysed the costs of a halfway implemented PACS in Turku University Central Hospital (TUCH) during 1998. Manual and digital archiving in 1998 continued parallel so that only 10% reduction of film usage was achieved. A 21% increase in image manipulation and storage expenses occurred. A calculation based on potential 90% reduction of film usage and changes in the amount of personnel suggest some direct savings. Also, indirect savings due to more efficient patient treatment and the reduction of time spent in the hospital, and overhead costs of information handling are expected to lead to savings. When full-scale PACS is installed, equipment investments, network and digital ware maintenance costs will drop from 121% to 116% compared with traditional film archiving activity costs [22]. There is a common belief that the introduction of electronic health information systems, such as PACS, will reduce the need for duplicate testing [16, 23]. For instance, You et al. (2008) [24] revealed that the majority (58%) of PACS users believe that the introduction of PACS at their institution was associated with a reduction in the number of unnecessary duplicate imaging tests. This study is the first to report objective data regarding the impact of PACS on the frequency of duplicate testing.
The responses of the physicians to the implementation of two whole hospitals PACS in Turkey indicated that it had been a useful advance for the hospital, with images of good quality available alongside reports, improving consultation services, patient satisfaction, saving in costs and personnel time. PACS has enabled some improvement in outpatient and inpatients health care [25]. For most respondents PACS had more quality of images, lessened frustration, improved their working lives and met their expectations. The perceived benefits of PACS outnumbered the disadvantages and reflected the widely documented benefits of PACS in the literature [3].
Mullins et al. (2001) analyzed impact of PACS on the education of radiology residents. The majority believed that PACS improved patient care (15 of 20, 75%) and their educational experience (15 of 20, 75%). A minority believed that increased patient throughput was harmful to the educational experience (five of 20, 25%) because it permitted attending radiologists to review cases too quickly (four of 20, 20%). Residents favored PACS over hard-copy images for ease of manipulation, resolution, and ability to see pathologic conditions and normal anatomic characteristics [14]. Sacco et al. (2002) [26] analysed: operator costs, paper costs, film costs, chemical costs, costs of optical disks and location rent for hardware and software of RIS/PACS. The results show that advantages provided by PACS implementation derive from a workflow optimization and saving of human resources rather than from a reduction in films and chemicals. Better management of radiological unit and PACS provides improved handling of clinical information, resulting in reduced time to initiate clinical action, with reduction in average length of patient stay and improvements in overall health outcomes [18, 26].
This small study has a number of limitations and direct comparisons between hospitals are inappropriate due to the fact that different PACS software was used, and respondents had varying levels of training and experience. However, a number of important points are raised. The technology clearly has enormous potential, and undisputable theoretical advantages over a hard film system. A number of studies of users’ perceptions report high levels of satisfaction with PACS [3, 16, 27]. The main problems that this study identified concerned the retrieval of images and usability, which have implications for risk management and clinical governance. The usability of a system is affected by a number of factors, including training and the type of software used. The study does not deal with the impacts belonging to multihospital PACS sharing. The future strategies of multihospital PACS projects in Turkey suggesting are some of the main interesting directions for further research. We consider that some of the problems identified may have been alleviated by improved communication and teamwork between radiology, information technology, hospital management and non-radiology clinicians, particularly at the time of implementation in Turkish health care industry.
The main limitation of this study pertains to the relatively low number of respondents, necessarily associated with the relatively small population in this setting. Fortunately, the response rate (45–50%) was comparable to or higher than in other studies involving hospital physicians [28–30], so that we may be confident about the validity of results in this study. A larger number of respondents in more hospitals would also have benefited scale reliability.
The patient-focused evaluation of large scale systems and the hospital-focused evaluation of all PACS systems could feasibly be conducted as contemporaneous experimental comparisons between hospitals in Turkey and other countries but the large research costs implied by such a design almost certainly mean that non-contemporaneous, non-experimental comparisons within hospitals are more realistic. The current situation for the PACS technology is that it has potential, but as yet unproven, benefits and a large capital cost. Thus, the primary purpose of funding additional PACS implementations must be to add to the currently small body of evaluation evidence in Turkey.
More research should be performed in private hospitals, university hospitals, military hospitals and public hospitals or preferably even comparing both types of settings in Turkish health system. Also more research should be conducted and planned on all health professions for PACS in Turkey.
References
Faggioni, L., Neri, E., Castellana, C., Caramella, D., and Bartolozzi, C., The future of PACS in healthcare enterprises. Eur. J. Radiol. 78:253–258, 2011.
Liu, Y., and Wang, J. PACS and digital medicine: essential principles and practical guidance. CRC Press, Taylor & Francis Group, 2011.
Pilling, J. R., Picture archiving and communication systems: users’ view. Br. J. Radiol. 79:519–524, 2003.
Liu, B. J., Cao, F., Zhou, M. Z., Mogel, G., and Documet, L., Trends in PACS image storage and archive. Comput. Med Imaging and Graph. 27:165–174, 2003.
Costa, C., Oliveira, J. L., Silva, A., Ribeiro, V. G., and Ribeiro, J., Design, development, exploitation and assessment of a Cardiology Web PACS. Comput. Methods Prog. Biomed. 93:273–282, 2009.
Pynoo, B., Devoldera, P., Duyck, W., VanBraak, J., Sijnave, B., and Duyck, P., Do hospital physicians’ attitudes change during PACS implementation? A cross-sectional acceptance study. Int. J. Med. Inform. 81:88–97, 2012.
Huang, H. K. PACS and imaging informatics basic principles and applications. Wiley, 2010.
Nagy, P., George, B., Reiner, B. I., and Siegel, E. L., Defining the PACS profession: an initial survey of skills, training, and capabilities for pacs administrators. J. Digit. Imaging 18(4):252–259, 2005.
Gamsu, G., and Perez, E. Picture archiving and communication systems (PACS). 18(3):165–168, 2003.
Lemke, H. U., PACS developments in Europe. Comput. Med. Imaging Graph. 27(2–3):111–120, 2003.
Lemke, H. U., Short history of PACS (Part II: Europe). Eur. J. Radiol. 78:177–183, 2011.
Choplin, R., Picture archiving and communication systems: an overview. Radiographics 12:127–129, 1992.
Toms, A. P., Kasmai, B., Williams, S., and Wilson, P., Building an anonymized catalogued radiology museum in PACS: a feasibility study. Br. J. Radiol. 79:666–671, 2006.
Mullins, M. E., Mehta, A., Patel, H., McLoud, T. C., and Novelline, R. A., Impact of PACS on the education of radiology residents: the residents’ perspective. Acad. Radiol. 8:67–73, 2001.
Reiner, B. I., Siegel, E. L., Hooper, F., Pomerantz, S. M., Protopapas, Z., Pickar, E., et al., Picture archiving and communication systems and vascular surgery: clinical impressions and suggestions for improvement. J. Digit Imaging 9:167–171, 1996.
Bryan, S., Weatherburn, G. C., Watkins, J. R., and Buxton, M. J., The benefits of hospital-wide picture archiving and communication systems: a survey of clinical users of radiology services. Br. J. Radiol. 72:469–478, 1999.
Tan, S., and Lewis, R. A., Picture archiving and communication systems: a multicentre survey of users experience and satisfaction. Eur. J. Radiol. 75(3):406–410, 2010.
MacDonald, D. M. Evaluating the implementation of picture archiving and communication systems in Newfoundland and Labrador. Dissertation, Memorial University of Newfoundland, 2008.
Watkins, J., A hospital-wide picture archiving and communication system (PACS): the views of users and providers of the radiology service at Hammersmith Hospital. Eur. J. Radiol. 32(2):106–112, 1999.
Maliff, R. P., and Launders, J., Using technology assessment as the picture archiving and communication system spreads outside radiology to the enterprise. J. Digit Imaging. 13(2):114–116, 2000.
Mackinnon, A. D., Billington, R. A., Adam, E. J., Dundas, D. D., and Patel, U., Picture archiving and communication systems lead to sustained improvements in reporting times and productivity: results of a 5-year audit. Clin. Radiol. 63(7):796–804, 2008.
Maass, M., Kosonen, M., and Kormano, M., Cost analysis of Turku University Central Hospital PACS in 1998. Comput. Methods Programs Biomed 66(1):41–45, 2001.
Bryan, S., Weatherburn, G., Buxton, M., Watkins, J., Keen, J., and Muris, N., Evaluation of a hospital picture archiving and communication system. J. Health Serv. Res. Pol. 4(4):204–209, 1999.
You, J. Y., Yun, L., and Tu, J. V., Impact of picture archiving communication systems on rates of duplicate imaging: a before-after study. BMC Heal. Serv. Res. 8:234, 2008. doi:10.1186/1472-6963-8-234.
Watkins, J., Weatherburn, G., and Bryan, S., The impact of a picture archiving and communication system (PACS) upon an intensive care unit. Eur. J. Radiol. 34(1):3–8, 2000.
Sacco, P., Mazzei, M., Pozzebon, E., and Stefani, P., PACS implementation in a university hospital in Tuscany. J Digit Imaging. 15(Suppl 1):250–251, 2002.
Hendy, J., Reeves, B. C., Hutchings, A., et al., Challenges to implementing the national programme for information technology: a qualitative study. Br. Med. J. 331:331–336, 2005.
Bhattacherjee, A., and Hikmet, N., Physicians’ resistance toward healthcare information technology: a theoretical model and empirical test. Eur. J. Inform. Syst 16:725–737, 2007.
Ilie, V., VanSlyke, C., Parikh, M. A., and Courtney, J. F., Paper versus electronic medical records: the effects of access on physicians’ decisions to use complex information technologies. Decis. Sci. 40:213–241, 2009.
Duyck, P., Pynoo, B., Devolder, P., Voet, T., Adang, L., and Vercruysse, J., Do hospital physicians really want to go digital? Acceptance of a picture archiving and communication system in a university hospital. Fortschr. Röntg 180(7):631–638, 2008.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Top, M. Physicians’ Views and Assessments on Picture Archiving and Communication Systems (PACS) in Two Turkish Public Hospitals. J Med Syst 36, 3555–3562 (2012). https://doi.org/10.1007/s10916-012-9831-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10916-012-9831-5