
Abstract
Low back pain (LBP) is one of the common problems encountered in medical applications. This paper proposes two expert systems (artificial neural network and adaptive neuro-fuzzy inference system) for the assessment of the LBP level objectively. The skin resistance and visual analog scale (VAS) values have been accepted as the input variables for the developed systems. The results showed that the expert systems behave very similar to real data and that use of the expert systems can be used to successfully diagnose the back pain intensity. The suggested systems were found to be advantageous approaches in addition to existing unbiased approaches. So far as the authors are aware, this is the first attempt of using the two expert systems achieving very good performance in a real application. In light of some of the limitations of this study, we also identify and discuss several areas that need continued investigation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Low back pain (LBP) creating dysfunction in muscular-skeletal system is one of the most common chronic pain syndromes. Forcing of muscles, connective and soft tissues, deformation of vertebrae, disc lesion or the inflammatory mediators associated with disc’s nucleus pulposus cause pain [1]. There are many ways to diagnose type, duration, location and intensity of a patient’s LBP. One of them is to diagnose in terms of the patient’s own statement. This approach is known to be visual analog scale (VAS). The patients are directed to indicate the level of pain on this scale. Thus, the pain is determined subjectively [2]. Although the VAS was reported to be reliable and to be a valuable method in the literature, the determination of the effect level of pain remains inadequate [3]. Skin resistance has been used since 1930s to determine sites of pathological conditions and is defined as the resistance offered to the passage of an electrical current (direct current) through the skin [4, 5]. Skin resistance is related to skin conductance, which changes in the presence of sweat, a fluid composed of water and ions.
There are many benefits in using the expert systems (artificial neural network-ANN and adaptive neuro-fuzzy inference system-ANFIS). By using the expert systems, more complex tasks can be learned from examples than by using conventional statistical techniques. Another benefit is that both qualitative and quantitative data can easily be included in the same model. The expert systems perform well in analysis of nonlinear multivariate data. Yet, a fully trained neural network can be used for further analysis of new data. That is why the expert systems are preferred in dealing with the current problems related to the LBP. The disadvantages related to the use of the expert systems include difficulties of expressing their function in a simple approach. For more details, the interested readers are referred to the work of Liszka-Hackzell and Martin [6].
There are also various studies in recent years to diagnose the LBP based on skin conductivity as a replacement method for the VAS [7–9]. Although there have been a great deal of research coping with the LBP in the literature, in terms of the VAS scale and the resistance, the prediction of the LBP using the ANN and ANFIS has not been investigated yet. There are limited number of studies in the literature [6, 10–13] using the current expert systems. However two of those works [10, 11] are mainly based on questionnaire and therefore they are subjective. It is also noticeable that the rest of those studies are devoted to categorize the patients with low back pain. At the same time, in the literature, there are other attempts concerning LBP and various expert systems [14, 15]. Therefore the main aim of this study is to predict the intensity of LBP using the ANN and ANFIS in terms of the VAS value obtained subjectively and the skin resistance measured objectively, in the receiver-operating characteristic analysis carried out, since the skin resistance values showed to be statistically significant in determining the VAS (P < 0.001).
Material, methods and study design
One hundred and sixty-nine subjects (110 LBP patients, 59 healthy subjects) from the Dumlupinar University Hospital, Physical Therapy and Rehabilitation Department, in 2008. The study had local department committee approval and all the subjects were taken verbal consents.
The skin resistance was recorded with two surface electrodes by the Digital Multimeter (DT-9923B) tool from the lumbar paravertabral area (from both left and right sides) while the subjects are in prone position. Two carbon electrodes were placed over paravertabral musculature of lumbar vertabra (L5) and 15 cm above it and direct current (5.5 V) was applied between the two silver-silver chloride electrodes.
Statistical analysis
SPSS 15.0 for Windows statistical program was used for all statistical analyses. Results were presented as mean ± SD. Statistical evaluation of the data was performed with Independent-Samples t-test for comparison between the two groups. Findings with an error probability value of less than 0.05 were considered as statistically significant.
Artificial Neural Network (ANN)
In this approach, the VAS and the skin resistance values are taken to be the input variables. Hence, pain intensity is the output variable as shown in Fig. 1. The VAS values, the left side skin resistance and pain intensity of totally 169 subjects are used for training data. Similarly, the VAS value and the right side skin resistance of totally 169 subjects are considered for testing data. The input and output variables are normalized between 0.1 and 1.0.

The ANN block diagram
The system diagnosed the pain intensity has been designed using MATLAB 2009 Toolbox. The designed ANN consisted of feed-forward back propagation, two hidden layers, training function (Levenberg-Marquardt), adaptation learning function (learngdm) and performance function (MSE-mean squared error). The neurons used in the system are 10 and 1, in the first and the second layers, respectively.
The data used in this research referred to 169 patients with back pain. The data consisted of 169 patients were used to form the ANN training set. Performance of the ANN training set and R value are 6.98 × 10−4 and 0.998, respectively. After training, the ability of the neural network to classify test patterns not in the training set was investigated.
Adaptive Neuro-Fuzzy Inference System (ANFIS)
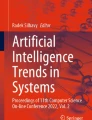
The system is used for prediction of the pain intensity. Similar to the ANN approach, testing and training data are utilized to evaluate the ANFIS methodology. The system diagnosing the pain intensity has been developed using MATLAB 2009 Toolbox, Sugeno type, with two inputs and one output. Each input variable has three triangular membership functions (Fig. 2). The designed ANFIS has been composed of two hidden layers as is the case in the ANN structure. The first and second hidden layers have got 9 and 1 neurons, respectively. In those neurons of the first hidden layer, the rule bases are connected with ‘and’ conjunction. The rule bases are as follows:

The membership functions of input variables
-
if VAS = VAS1 and Sr = Sr1 then O = O1
-
if VAS = VAS1 and Sr = Sr2 then O = O2
-
if VAS = VAS1 and Sr = Sr3 then O = O3
-
if VAS = VAS2 and Sr = Sr1 then O = O4
-
if VAS = VAS2 and Sr = Sr2 then O = O5
-
if VAS = VAS2 and Sr = Sr3 then O = O6
-
if VAS = VAS3 and Sr = Sr1 then O = O7
-
if VAS = VAS3 and Sr = Sr2 then O = O8
-
if VAS = VAS3 and Sr = Sr3 then O = O9
The data consisted of 169 patients were used to form the ANFIS training set. Epoch and performance of the ANFIS training set are 150 and 4.30 × 10−2, respectively. After training the data, the ability of the ANFIS to categorize testing set not in the training set was investigated.
Results
Demographic data of the subjects are presented in Table 1. Demographic and physical features of the LBP and control groups are similar. The intensity level of the LBP measured from the left/right paravertabral sides (real data) and the intensity of the LBP predicted using the ANN and ANFIS values (computed with expert systems) have been compared as seen in Table 2. There is no statistically significant difference between the real data and the computed results with the expert systems (the ANN and ANFIS) in terms of the pain intensity level (P > 0.05). The expert systems behave very similar to real data as seen in Figs. 3 and 4 (R 2 = 0.934 for both the ANN and ANFIS). To make rich this study, the ANN and ANFIS results are compared with a nonlinear regression method (a second-order polynomial). At the end of the comparison, R 2 has been found be 0.935 for the nonlinear regression model. The model used is
where Sr and O stand for the skin resistance value and output, respectively. As can be seen from the corresponding results, the ANN and ANFIS are in very agreement with the result of the above nonlinear model.

A comparision between the ANN results and normalized data

A comparision between the ANFIS results and normalized data
As pointed out by Forsstrom [16], ANNs have been shown to be superior to both conventional statistical methods and manual/specialist-based analysis in many studies. There are many benefits in using neural networks compared to conventional statistical methods. For the details of the discussion interested readers are referred to the corresponding reference.
By using neural networks, more complex tasks can be learned from examples than by using conventional statistical techniques. Another benefit is that both qualitative and quantitative data can easily be included in the same model. Neural networks perform well in analysis of nonlinear multivariate data. The disadvantages related to the use of neural networks include difficulties of expressing their function in a simple way.
As a result of these findings, use of the developed expert systems can be used to successfully diagnose the back pain intensity.
Discussion
In this study, two expert systems evaluating the intensity level of LBP objectively have been developed. In addition, the developed systems have been justified to predict the intensity level of the LBP by using subjective VAS value and objective data of skin resistance. Correlation of the results delivered by the designed algorithms has been found to be excellent. The developed systems have also been found to be consistent between each other. At the same time, since the expert systems are noninvasive, there is no requirement for any surgical operation to diagnose the patients. Thus instead of the VAS method which is a subjective method, the presented objective methods may be used for the scaling the intensity level of the pain.
An attempt was done to diagnose the LBP by Bounds et al. [10] even though their networks did not perform very well. Their data for each patient was collected on a tick sheet which listed symptoms and other relevant previous medical history.
Lin et al. [11] implemented and evaluated a web-based decision support system that employs an intuitive and easy-to-use framework to assess the patient’s information and recommend a diagnosis consisting of one or multiple parts. Their study both contributed to decision support systems research and advanced clinical support for LBP diagnosis.
Carregal et al. [17] designed a system consisting of a perfusion pump guided by a fuzzy logic computer interface to regulate the perfusion of alfentanil in accordance with the patient’s pain response. Their system was also equipped with a safety device that halted perfusion in case of desideration, bradypnea or heart rate or blood pressure variations greater than 25%.
For 255 patients, a novel fuzzy pain demand (FPD) index derived from the interval of each bolus of patient-controlled analgesia was used by Shieh et al. [18]. They found the FPD index modeled from a fuzzy modeling algorithm to interpret the self-titration of the drug delivery can show the patients’ dynamic demand and past efforts to overcome the postoperative pain.
Shamim et al. [19] utilized fuzzy logic-based fuzzy inference system (FIS) for identifying patients unlikely to improve after disk surgery and explored FIS as a tool for surgical outcome prediction. They reported that the FIS has a sensitivity of 88% and specificity of 86% in the prediction of patients most likely to have poor outcome after lumbosacral miscrodiskectomy.
Our designed systems are effectively to predict the pain intensity level objectively. As the studies carried out in the literature, the current developed systems can be used in clinical fields. The computed results indeed demonstrate the effectiveness of the proposed approaches. On the other hand, the suggested systems can be extended to other musculoskeletal pathologies and visceral disorders for prediction of the pain intensity level. Thus, future consideration can be paid on this factor for further research.
References
Langevin, H. M., and Sherman, K. J., Pathophysiological model for chronic low back pain integrating connective tissue and nervous system mechanisms. Med. Hypotheses 68(1):74–80, 2007.
Gould, D., Kelly, D., Goldstone, L., and Gammon, J., Examining the validity of pressure ulcer risk assessment scales: developing and using illustrated patient simulations to collect data. J. Clin. Nurs. 10:697–706, 2001.
Stener-Victorin, E., Lundeberg, T., Kowalski, J., Opdal, L., Sjöström, J., and Lundeberg, L., Perceptual matching for assessment of itch; reliability and responsiveness analyzed by a rank-invariant statistical method. J. Invest. Dermatol. 121:1301–1305, 2003.
Richter, C. P., and Katz, D. T., Peripheral nerve injuries determined by the skin resistance method. JAMA 122:648, 1943.
Riley, L. H., and Richter, C. P., Use of electrical skin resistance method in the study of patients with neck and upper extremity pain. Johns Hopkins Med. J. 137:69–74, 1975.
Liszka-Hackzell, J. J., and Martin, D. P., Categorization and analysis of pain and activity in patients with low back pain using a neural network technique. J. Med. Syst. 26(4):337–347, 2002.
Shankar, K., Bharathi, V. S., and Daniel, J., An empirical approach for objective pain measurement using dermal and cardiac parameters. ICBME 2008(23):678–681, 2009.
Weng, C. S., Tsai, Y. S., Shu, S. H., Chen, C. C., and Sun, M. F., The treatment of upper back pain by two modulated frequency modes of acupuncture-like tens. J. Med. Biol. Eng. 25(1):21–25, 2005.
Weng, C. S., Tsai, Y. S., and Yang, C. Y., Using electrical conductance as the evaluation parameter of pain in patients with low back pain treated by acupuncture like tens. Biomed. Eng. Appl. Basis Commun. 16:205–212, 2004.
Bounds, D. G., Lloyd, P. J., Mathew, B., and Waddell, G., A multi layer perceptron network for the diagnosis of low back pain. IEEE Int. Conf. Neural Netw. 2:481–489, 1988.
Lin, L., Hu, P. J. H., and Sheng, O. R. L., A decision support system for lower back pain diagnosis: uncertainty management and clinical evaluations. Decis. Support Syst. 42:1152–1169, 2006.
Gioftsos, G., and Grieve, D. W., The use of artificial neural networks to identify patients with chronic low-back pain conditions from patterns of sit-to-stand manoeuvres. Clin. Biomech. 11(5):275–280, 1996.
Vaughn, M. L., Cavill, S. J., Taylor, S. J., Foy, M. A., and Fogg, A. J. B. Direct explanations and knowledge extraction from a multilayer perceptron network that performs low back pain classification. In: Wermter, S., and Sun, R. (Eds.), Hybrid Neural Systems. Lecture Notes in Artificial Intelligence. Springer, 2000.
Mathew, B., Morris, D., David, H., and Gordon, W., Artificial intelligence in the diagnosis of low-back pain and sciatica. Spine 13(2):168–172, 1988.
Li, B., Yan, C., and Xu, Y. Designing and implementing of an expert system for the differential diagnosis and treatment of lumbago. Proceedings of the 3rd International Conference on Young Computer Scientists. Beijing, 1027–1028, 1993.
Forsstrom, J. J., Artificial neural networks for decision support in clinical medicine. Ann. Med. 27:509–517, 1995.
Carregal, A., Figueira, A., Núñez, M., Carollo, A., Lorenzo, A., Rey, M., and González, G., Fuzzy logic and postoperative pain. Rev. Esp. Anestesiol. Reanim. 44(6):215–217, 1997.
Shieh, J. S., Dai, C. Y., Wen, Y. R., and Sun, W. Z., A novel fuzzy pain demand index derived from patient-controlled analgesia for postoperative pain. IEEE Trans. Biomed. Eng. 54(12):2123–2132, 2007.
Shamim, M. S., Enam, S. A., and Qidwai, U., Fuzzy Logic in neurosurgery: predicting poor outcomes after lumbar disk surgery in 501 consecutive patients. Surg. Neurol. 72(6):565–572, 2009.
Acknowledgement
For their generous contribution to the conducted study, the employees at the Dumlupinar University, Medical Faculty, Department of Physical Therapy and Rehabilitation outpatient clinic are appreciated.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sari, M., Gulbandilar, E. & Cimbiz, A. Prediction of Low Back Pain with Two Expert Systems. J Med Syst 36, 1523–1527 (2012). https://doi.org/10.1007/s10916-010-9613-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10916-010-9613-x