
Abstract
Physical activity promotes health and is important for preventing chronic conditions, such as obesity and cardiovascular disease. Little is known about factors associated with different types of PA among Latina women, particularly Dominicans, who now constitute the fifth largest group of Latinos in the United States. The purpose of this study was to examine whether occupational physical activity, acculturation, familism, and norms held by family and friends are associated with three types of PA: vigorous and moderate leisure-time physical activity (LTPA), and resistance training. Interviews were conducted with 418 Dominican women. We assessed self-reported PA using standardized measures. Data were collected between July 2010 and July 2012 in New York City. Most women reported no vigorous LTPA or resistance training (74.5 and 73.1 %, respectively); about half (52.1 %) reported no moderate LTPA. After adjusting for sociodemographic factors, occupational physical activities were associated with greater LTPA. Acculturation was not associated with any outcome. Positive family norms about exercise were associated with increased LTPA and resistance training. Family norms may play a critical role in PA and should be included in programs to increase PA among Latina women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical activity (PA) is key to promoting health and preventing a variety of chronic diseases, including obesity and cardiovascular disease. Low engagement in PA is a major public health concern, particularly among Latina women. Recent data from the National Health Interview Survey (2014) indicate that only 38.9 % of Latina women engage in sufficient levels of aerobic PA, and only about one of ten (11.5 %) Latinas fully meet the recommended guidelines for PA, which include both aerobic and muscle-strengthening activities [1].
There is growing recognition of differing health patterns and profiles among the various Latino groups [2]. Although there are currently 50.5 million Latinos in the United States, comprising 16 % of the U.S. population, the “Latino” category combines very diverse populations. Numbering over one million persons, Dominicans are the fifth largest Latino group in the nation [3], but there is very little research on the health or health behaviors of this group. There is some evidence that Dominicans show a mixed health profile of disparities and advantages. For example, relative to other Latino groups, Dominicans report poorer subjective health ratings; but lower levels of overweight [2]. Dominicans have the lowest rates of leisure-time physical activity (LTPA) among Hispanics [4, 5] and non-Hispanic whites [4]. However, there is very little research on PA among Dominicans [6], and there is a relatively small body of research on other Latino groups [4–6].
Research on PA among Latinos (of any nationality) is further hampered by the focus of most studies on leisure-time activities, which do not take into account exertion related to physically demanding occupations or unpaid work (e.g., housework). More Latinos than whites report engaging in five or more hours per day of physically demanding work activities, and some research suggests that increases in levels of arduous labor are associated with decreases in leisure-time physical activities [7]. A recent analysis of NHANES data showed that relative to non-Latino whites, Mexican Americans have higher total PA levels due to occupational activity, but analyses did not directly compare Mexican Americans to other groups within similar occupational strata [8]. Moreover, gender differences may be present. Latinas who work outside the home have high levels of PA, especially those in occupations that require intensive labor [9]. Latinas engage in more household activities than Latino men, and Latino men report more occupational and overall activity [10].
There is growing evidence that PA increases with greater acculturation, an effect that has been most consistently observed among Latina women [11–13]. The higher rate of PA with greater acculturation may be due to the adoption of health beliefs about the benefits of exercise, greater knowledge about or ability to exercise, or other factors, including more supportive social norms regarding PA. However, most studies of acculturation and PA among Latinos focus on LTPA. Few examine the association between acculturation and different types of PA. Latinos at low levels of acculturation may engage in non-leisure PA. Marquez and McAuley [10] found that greater acculturation was associated with less occupational physical activity (OPA), but that lower acculturation was associated with greater overall activity. They proposed that greater acculturation can lead to occupations that do not require manual labor and that if PA is assessed solely as LTPA, low-acculturated Latinos, who may hold more manual labor positions, may be incorrectly classified as sedentary.
Much of the literature on acculturation and health behaviors assumes that beliefs or norms concerning particular behaviors change with greater acculturation. For example, greater acculturation may lead to changes in beliefs about PA, or in specific values or norms. Familism, in particular, is a core feature of Latino value systems and is defined as a general orientation towards family (i.e., strong family ties, view of the family as a source of support, strength and inspiration) [14]. Familism may create time demands that pose barriers to engaging in LTPA [15, 16]. Whether this cultural value is associated with various types of PA—and whether PA declines with greater acculturation—remain questions for further research.
There is a need for more integrative research that considers social norms and cultural values (e.g., familism), as well as acculturation, as determinants of PA. However, few studies explore acculturation and norms, and no published study that we have been able to locate explores all of these factors among Dominican women (or any other Latino group). Therefore, the primary purpose of this study was to examine cultural values and norms as predictors of three types of PA among Dominican women: moderate PA, vigorous PA, and resistance training. After adjusting for potential confounders (sociodemographic characteristics, marital status, and health status), the main questions driving this study were: (1) Is occupational physical activity (OPA) associated with LTPA? (2) To what extent do acculturation and familism correlate with different types of LTPA? (3) What is the role of norms in predicting LTPA? Specifically, are norms about LTPA or being overweight associated with LTPA?, and (4) do norms held by friends and family differentially predict LTPA?
Methods
Procedures
The data presented in this report are from a larger study of health promoting behaviors (and breast cancer screening practices) among Dominican women living in two New York City neighborhoods that are predominantly Dominican. New York is home to 674,787 Dominicans—the largest number in the U.S.—constituting almost half (48 %) of all Dominicans in the country [3].
Participants were recruited using several methods. We recruited from a range of culturally-relevant community sites including a university-based center that provides services to the community (e.g., free use of computers, access to health information in Spanish). We also posted flyers in designated areas in the target communities, including apartment buildings and community-based agencies and service facilities (e.g., senior centers).
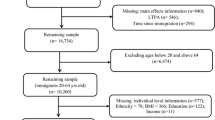
Approximately 54 % of the sample was recruited from community sites, 10 % from respondent referrals, and the remainder by other methods. Eligibility criteria were: (1) Dominican female aged 40 years or older and (2) no prior diagnosis of any form of cancer. All participants gave their informed consent prior to their inclusion in the study, and the research was approved by the university’s medical center Institutional Review Board. A total of 418 Dominican women participated in the study and all interviews occurred between July 2010 and July 2012.
Data were collected by a structured in-person interview conducted in Spanish in the respondent’s site of choice (e.g., home or community-based site). Interviews lasted an average of 55 min. Respondents were paid $20 cash for their participation.
Measures
We used a back-translation technique with two iterations to create Spanish versions of measures. Scales were translated by independent, native Spanish-speaking translators with extensive previous experience translating research instruments for Dominican populations.
Sociodemographic and Health Status Variables
Variables assessed as potential confounders were: age (years); education (highest grade completed in years); employment (1 = employed, 0 = not employed); and marital status (1 = married, 0 = unmarried). Health Status was assessed with a standardized question used in various national surveys: “In general, would you say your health is excellent (5), very good (4), good (3), fair (2), or poor (1)?”.
Acculturation
We used the 12-item short form of the Acculturation Rating Scale for Mexican Americans (Brief ARSMA-II) [17], which is one of the most widely-used measures of acculturation, and can be adapted for use with several Latino populations [18]. Items include English- and Spanish-language ability and preference (speaking, writing and reading) and extent of embeddedness with Anglo American friends. Higher scores indicate greater acculturation.
Familism
Familism is one of the most prominent cultural values identified among Latinos [14, 19]. We measured familism with Sabogal and colleagues 15-item scale [20], which has good reliability, and is associated with acculturation among various Latinos groups [20]. Using a five-point scale, respondents rated their level of agreement with items that tap family as referents (e.g., “The family should consult close relatives concerning its important decisions”), and beliefs about familial obligations (e.g., “I would help within my means if a relative told me that she/he is in financial difficulty”). We calculated scores by averaging across items, with greater values representing a higher level of familism.
Body Mass Index
For descriptive purposes, we assessed BMI. Interviewers weighed and measured the height of study participants using a portable scale and tape measure. We calculated BMI from these measurements using the standard BMI formula.
Social Norms About Overweight and Physical Activity
To assess social norms, we borrowed questions from the New York Social Environment Study [21]. We assessed descriptive norms, that is, having family members who are overweight and who engage in PA, by asking “How many of your family members are overweight [exercise]?” with response options of: 1 = none of them, 2 = a few, 3 = some, 4 = many, 5 = all of them. We refer to these variables as family overweight and family exercise, respectively. We assessed injunctive norms of family and friends, that is, family and friends’ attitudes about overweight and exercise, by asking, ‘‘What do most of your family members [close friends] think about being overweight [exercise]?” Response options were: they think it is acceptable, unacceptable, they don’t care, or I don’t know; dichotomized to reflect positive norms about overweight and exercise: 1 = acceptable and 0 = all other responses. These items were used as separate indices of family and friends norms about being overweight and exercise.
Physical Activity Variables
Occupational Physical Activity
Moderate and vigorous PA at work were assessed with two items: “Does your work require vigorous/moderate PA that lasts at least 10 min?” Both were coded dichotomously to create vigorous and moderate occupational physical activity (OPA) variables: 0 = no occupational physical activity, 1 = occupational physical activity.
Vigorous, Moderate, and Resistance Training Leisure Time Physical Activity
LTPA was assessed with standardized questions from the National Health Interview Survey to measure self-reported frequency of activities. Each type of LTPA was assessed by asking “How often during the week do you do vigorous [moderate] activities for at least 10 min continuously for recreation, fun, exercise, or sports?” Resistance training activities were assessed by asking, “How often during the week do you do physical activities specifically for strengthening muscles, such as lifting weights or gymnastics?” The outcome measures of vigorous, moderate, and resistance training LTPA were assessed as the actual number of times the respondent indicated that she engaged in at least 10 min each type of LTPA per week.
Statistical Analyses
We conducted one set of models for each outcome variable, vigorous LTPA, moderate LTPA, and resistance training as Poisson Generalized Linear Models (GLM) to account for the skewed nature of the variables because we were fitting count data. In model 1, the predictors were demographics: age, education, employment status, marital status, and health status. In model 2, we added OPA variables: moderate work activities and vigorous work activities. Model 3 added acculturation variables: ARSMA and familism scales. Finally, model 4 added social norms variables regarding overweight and exercise: family overweight, family’s norms on overweight, friends’ norms on overweight, family exercise, family’s norms on exercise, and friends’ norms on exercise. All analyses were conducted using SPSS v. 22.
Results
Descriptive Statistics
There were 418 Dominican women included in this study. Table 1 provides data on demographic, physical activity and social norms. The sample can be characterized as older (mean age = 60.5 years), mostly unemployed, and as having low education and acculturation. The sample was generally physically inactive. Many women reported engaging in LTPA zero times per week: most women (74.5 %) engaged in no vigorous LTPA per week, about half (52.1 %) in no weekly moderate LTPA; and most women (73.1 %) reported no weekly resistance training. With regard to occupational activity, 19.0 % reported having work that requires vigorous activity. Almost half (48.0 %) reported that work requires moderate activity. The mean BMI of the sample was 29.4 (SD = 5.6; median = 28.5; range = 17.3, 52.0).
Women reported negative injunctive norms about overweight, indicating that most family (81.2 %) and friends (77.4 %) believed that being overweight was not acceptable. Conversely, they reported positive norms about exercise, indicating that most family (91.0 %) and friends (86.4 %) found exercise to be acceptable. With regard to descriptive norms, approximately one-third (33.1 %) of women said that none of their family members were overweight. The majority of women (65.4 %) reported that some, many or all family members engaged in exercise.
Results for Main Research Questions
Research question 1: Are occupational activities associated with LTPA? We tested the effect of vigorous and moderate OPA on LTPA outcomes, adjusting for demographic variables, in model 2 in Tables 2, 3 and 4. The LTPA outcomes represent the number of times per week that a respondent reported engaging in vigorous, moderate, and resistance training physical activities.
Those who engaged in vigorous OPA had 2.68 (95 % CI 2.06, 3.47) times the number of vigorous LTPA sessions than women who did not engage vigorous OPA (Table 2, model 2). Those who engaged in moderate OPA had 1.48 times (95 % CI 1.12, 1.96) more vigorous LTPA per week than those reporting no moderate OPA. After adjusting for all acculturation and social norm variables, associations for both vigorous and moderate OPA remained significant, with little attenuation of effect (RR vigorous OPA = 2.60 and RR moderate OPA = 1.42).
In models for moderate LTPA (Table 3), only moderate OPA was significantly associated. In the final model, those who reported moderate OPA engaged in 2.01 (95 % CI 1.67, 2.41) times more moderate LTPA per week than those without moderate OPA, after adjusting for covariates.
Resistance training was associated with both vigorous and moderate OPA (Table 4). After all adjustments in the final model, those who reported vigorous OPA engaged in 1.52 (95 % CI 1.17, 2.00) times more regular resistance training per week than those with no vigorous OPA. Those who reported moderate OPA engaged in 1.31 (95 % CI 1.03, 1.67) times more resistance training sessions than those without moderate OPA.
Research question 2: To what extent do acculturation and familism correlate with different types of PA? Acculturation was not significantly associated with any of the outcomes in the final models. Familism was positively associated with moderate LTPA in the final model, RR = 1.33(95 % CI 1.10, 1.61), controlling for sociodemographic variables and acculturation.
Research questions 3 and 4: What is the role of norms in LTPA? Are norms about LTPA or being overweight associated with LTPA? Are norms held by friends and family differentially associated with LTPA behaviors? Family’s opinions on exercise were associated with engagement in all LTPA outcomes. Relative to those without positive family norms, women with positive family norms on exercise, on average, engaged in 3.6 times (95 % CI 1.29, 10.07) more vigorous LTPA per week, 2.29 times (95 % CI 1.35, 3.90) more moderate LTPA per week, and 2.21 (95 %CI 1.05, 4.63) more resistance training sessions per week. Family members being overweight and family’s norms on being overweight were negatively associated with moderate LTPA and resistance training. Women with overweight family members engaged in 14 % less moderate LTPA than women with no overweight family members. Women with overweight family members engaged in 15 % less resistance training than women with no overweight family members. Friends’ norms on exercise were negatively associated with engagement in moderate LTPA (RR = 0.76, 95 % CI 0.59, 0.98); this was the only outcome for which friends’ norms were significant.
Discussion
This study focused on both LTPA and OPA among Dominican women living in New York City. Overall, we found low rates of LTPA in our sample, with nearly three-quarters of women engaging in no LTPA. Women who engaged in moderate or vigorous OPA were more likely to engage in vigorous LTPA, and those who engaged in vigorous OPA were also more likely to engage in resistance training. Marquez and McAuley [10] examined OPA and LTPA among a diverse sample of 155 Latino men and women and found that non-LTPA accounted for nearly 80 % of the sample’s self-reported overall PA. Although they found no differences in recreational activity levels, OPA and overall PA was more common among Latino men than Latina women, and household/domestic PA was more common among Latina women than Latino men. They also found that Latina women with higher overall levels of PA were less likely to engage in domestic activity. These results compliment other findings that LTPA is particularly low among Latina women in comparison to Latino men, and suggest that increasing LTPA among Latinas is a priority area [22]. Moreover, given evidence that, relative to non-Latino whites, Latinos are more likely to engage in non-LTPA [23] and that Latino immigrants report greater work demands to meet their financial obligations in the U.S., leaving less time for leisure-time activities that include PA [24], it is critical to understand the determinants of PA using broader measures that do not focus exclusively on LTPA. More work is needed to understand how participation in OPA influences LTPA, and how determinants of both types of PA may differ by gender.
We did not find an association between acculturation and LTPA, but these null findings may relate to low variability in acculturation among this sample. Although women had been living in the United States for an average of 25 years, they had relatively low levels of acculturation as measured by the Brief ARSMSA-II scale. In some studies, acculturation is associated with greater LTPA among Latinos [11–13]. Marquez and McAuley’s data [10], however, reveal complexities in the association between acculturation and different types of PA: more acculturated Latinos engaged in less OPA and overall PA than less acculturated Latinos, but no association was found between acculturation and household metabolic equivalents (MET) hour per week, recreational MET, or average daily activity counts. Given these complex findings, it will be important to more closely understand how acculturation shapes activity patterns, measuring both LTPA and non-LTPA among Latinos.
In examining cultural norms, we found that greater familism was associated with higher levels of moderate LTPA. Women with strong familial attachments may have more opportunities to be physically active as a family or may perceive their family members to be supportive of PA. Future research among Latinas should further explore how familism and other cultural norms may influence PA, including perceptions of ideal body size and weight [15, 25–27].
We found that positive family opinions on exercise were significantly and independently associated with greater engagement in moderate and vigorous LTPA and resistance training. In contrast, friends’ opinions about exercise were negatively associated with moderate LTPA. Descriptive and injunctive family norms on being overweight were associated with decreased moderate LTPA and perceiving one’s family to be overweight was associated with decreased resistance training. A few prior studies assessed measures related to social norms about exercise, as was explored here. For example, knowing people who exercise [28], and seeing people exercise in the neighborhood [29] is associated with PA among Latinas. However, little research explicitly examines normative differences between friends and family that may influence PA among Latinos. Some studies [30] report that Latinos with higher levels of PA have more support from friends, but not family, though other studies find no association [31]. Husbands or partners, in particular, are cited as a negative influence on exercise for Latinas [32, 33]. Our findings suggest that Latinas may be influenced by the experiences and opinions of family members with respect to weight and PA. Future research should continue to disentangle which family members are most critical in influencing PA. If confirmed, these data suggest that PA interventions might be most effective if they target the entire family unit, and that for maximal impact, social network interventions should address the attitudes and behaviors of both Latinas and their family members.
Limitations
It is important to consider our findings in light of study limitations. First, the study was cross-sectional, therefore, conclusions cannot be drawn about causality. Second, all measures were collected by self-report. Estimates of LTPA may be subject to recall bias and may overestimate actual PA levels. However, the LTPA measures employed in this study are standardized instruments used in several iterations of the National Health Interview Survey. Moreover, women reported very low levels of PA. Therefore, if there is a self-report bias towards overestimating PA, the tendency to over-report may not have been great in this sample, given that reported levels of PA were so low. Moreover, LTPA questions asked in a similar way show satisfactory levels of reliability and validity among Latinos [34]. Finally, our findings are likely generalizable only to urban Latinas, given our recruitment from the New York City area.
New Contribution to Literature
Despite some limitations, there are several notable strengths of the study that contribute to the literature. First, unlike much existing research, our study assessed multiple forms of PA, including LTPA, OPA and resistance training. This is critical as our approach provides a comprehensive assessment of PA, and taps into aspects of PA that may be more common among Latinas (e.g., domestic or household PA). Second, with over 400 respondents, our sample size is robust, and constitutes one of the largest community-based studies of PA among Latinas. Third, our study contributes to scientific knowledge on Dominicans, who—despite their prominence as the fifth largest group of Latinos in the United States—are vastly underrepresented in the public health literature. Finally, our study enhances understanding of the role of family and friend social norms in shaping PA behaviors among Latinas. Results suggest that family may be a particularly critical influence that should be included or addressed in health promotion programs to enhance PA among this population.
References
National Health Interview Survey. Data Table A-14a: Summary Health Statistics: National Health Interview Survey, 2014. http://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2014_SHS_Table_A-14.pdf (2014).
Zsembik BA, Fennell D. Ethnic variation in health and the determinants of health among Latinos. Social Sci Med. 2005;61:53–63.
The Hispanic population 2010. U.S. Department of Commerce Economics and Statistics Administration. http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdf (2011). Accessed 25 Jan, 2014.
Neighbors CJ, Marquez DX, Marcus BH. Leisure-time physical activity disparities among Hispanic subgroups in the United States. Am J Public Health. 2008;98:1460.
Vermeesch AL, Stommel M. Physical activity and acculturation among US Latinas of childbearing age. West J Nurs Res. 2013. doi:10.1177/0193945913507341.
Jurkowski JM, Mosquera M, Ramos B. Selected cultural factors associated with physical activity among Latino women. Women’s Health Issues. 2010;20:219–26.
Centers for Disease Control and Prevention. Prevalence of leisure-time and occupational physical activity among employed adults–United States, 1990. Morb Mortal Wkly Rep. 2000;49:420.
Gay JL, Buchner DM. Ethnic disparities in objectively measured physical activity may be due to occupational activity. Prev Med. 2014;63:58–62.
López IA, Bryant CA, McDermott RJ. Influences on physical activity participation among latinas: an ecological perspective. Am J Health Behav. 2008;32:627–39.
Marquez DX, McAuley E. Gender and acculturation influences on physical activity in Latino adults. Ann Behav Med. 2006;31:138–44.
Cantero PJ, Richardson JL, Baezconde-Garbanati L, Marks G. The association between acculturation and health practices among middle-aged and elderly Latinas. Ethn Dis. 1998;9:166–80.
Abraído-Lanza AF, Chao MT, Flórez KR. Do healthy behaviors decline with greater acculturation?: implications for the Latino mortality paradox. Soc Sci Med. 2005;61:1243–55.
Crespo CJ, Smit E, Carter-Pokras O, Andersen R. Acculturation and leisure-time physical inactivity in Mexican American adults: results from NHANES III, 1988–1994. Am J Public Health. 2001;91:1254–7.
Marín G, Gamba RJ. Acculturation and changes in cultural values. In: Chun KM, Balls Organista P, Marín G, editors. Acculturation: Advances in theory, measurement and applied research. Washington, DC: American Psychological Association; 2003. p. 83–93.
Juarbe T, Turok XP, Pérez-Stable EJ. Perceived benefits and barriers to physical activity among older Latina women. West J Nurs Res. 2002;24:868–86.
Evenson KR, Sarmiento OL, Ayala GX. Acculturation and physical activity among North Carolina Latina immigrants. Soc Sci Med. 2004;59:2509–22.
Cuellar I, Bastida E, Braccio SM. Residency in the United States, subjective well-being, and depression in an older Mexican-origin sample. J Aging Health. 2004;16:447–66.
Chun KM, Balls Organista PE, Marín GE, editors. Acculturation: advances in theory, measurement and applied research. Washington, DC: American Psychological Association; 2003.
Cuéllar I, Arnold B, González G. Cognitive referents of acculturation: assessment of cultural constructs in Mexican Americans. J Commun Psychol. 1995;23:339–56.
Sabogal F, Marín G, Otero-Sabogal R, Marín BV, Perez-Stable EJ. Hispanic familism and acculturation: what changes and what doesn’t? Hispanic J Behav Sci. 1987;9:397–412.
Stuber J, Galea S, Link BG. Smoking and the emergence of a stigmatized social status. Soc Sci Med. 2008;67:420–30.
Marquez B, Elder JP, Arredondo EM, Madanat H, Ji M, Ayala GX. Social network characteristics associated with health promoting behaviors among Latinos. Health Psychol. 2014;33:544–53.
Brownson RC, Eyler AA, King AC, Brown DR, Shyu YL, Sallis JF. Patterns and correlates of physical activity among US women 40 years and older. Am J Public Health. 2000;90:264–70.
Juniu S. The impact of immigration: leisure experience in the lives of South American immigrants. J Leisure Res. 2000;32:358–81.
Martinez SM, Arredondo EM, Perez G, Baquero B. Individual, social, and environmental barriers to and facilitators of physical activity among Latinas living in San Diego County: focus group results. Fam Commun Health. 2009;32:22–33.
Keller C, Fleury J. Factors related to physical activity in Hispanic women. J Cardiovasc Nurs. 2006;21:142–5.
Day K. Active living and social justice: planning for physical activity in low-income, black, and Latino communities. J Am Plan Assoc. 2006;72:88–99.
Evenson KR, Sarmiento OL, Tawney KW, Macon ML, Ammerman AS. Personal, social, and environmental correlates of physical activity in North Carolina Latina immigrants. Am J Prev Med. 2003;25:77–85.
Wilbur J, Chandler PJ, Dancy B, Lee H. Correlates of physical activity in urban Midwestern Latinas. Am J Prev Med. 2003;25:69–76.
Marquez DX, McAuley E. Social cognitive correlates of leisure time physical activity among Latinos. J Behav Med. 2006;29:281–9.
Eyler AA, Brownson RC, Donatelle RJ, King AC, Brown D, Sallis JF. Physical activity social support and middle- and older-aged minority women: results from a US survey. Soc Sci Med (1982). 1999;49:781–9.
Bautista L, Reininger B, Gay JL, Barroso CS, McCormick JB. Perceived barriers to exercise in Hispanic adults by level of activity. J Phys Act Health. 2011;8:916–25.
Ramirez AG, Chalela P, Gallion K, Velez LF. Energy balance feasibility study for Latinas in Texas: a qualitative assessment. Prev Chronic Dis. 2007;4:A98.
Rauh MJ, Hovell MF, Hofstetter CR, Sallis JF, Gleghorn A. Reliability and validity of self-reported physical activity in Latinos. Int J Epidemiol. 1992;21:966–71.
Acknowledgments
Thanks to Raziel D. Valiño, Emily Vasquez, Elisa Gonzalez, Evianna Cruz, Milagros Ventura, and Karen R. Flórez for their research assistance.
Funding
This work was supported by Grant R21CA134247 from the National Cancer Institute of the National Institutes of Health. The work was also supported, in part by Grants R25GM062454, and UL1TR000040 from the National Institutes of Health; and the American Cancer Society (124793-MRSG-13-152-01-CPPB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
All the authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in this study, which involved human participants, were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Abraído-Lanza, A.F., Shelton, R.C., Martins, M.C. et al. Social Norms, Acculturation, and Physical Activity Among Latina Women. J Immigrant Minority Health 19, 285–293 (2017). https://doi.org/10.1007/s10903-016-0519-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-016-0519-7